





 , Lidia Febrianti 2, Ekorini Listiowati 3, Husnan Nurjuman 4, Endang Lukitosari 5, Nurhalina Afriana 5
, Lidia Febrianti 2, Ekorini Listiowati 3, Husnan Nurjuman 4, Endang Lukitosari 5, Nurhalina Afriana 51 Department of Obstetrics and Gynecology, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta, 55183 Yogyakarta, Indonesia
2 Department of Midwifery, Sekolah Tinggi Ilmu Kesehatan Guna Bangsa Yogyakarta, 55283 Yogyakarta, Indonesia
3 Department of Family Medicine and Public Health, School of Medicine, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta, 55183 Yogyakarta, Indonesia
4 Department of Communication Sciences, Faculty of Social and Political Sciences, Universitas Sultan Ageng Tirtayasa, 42163 Serang, Indonesia
5 Ministry of Health of the Republic of Indonesia, 12950 Jakarta, Indonesia
Abstract
Globally, the World Health Organization (WHO) estimates that 7 per 1000 pregnant women have maternal syphilis infection. This study aims to investigate the expansion of dual Human Immunodeficiency Virus (HIV) and syphilis screening among pregnant women in Indonesia, with a focus on East Java and Central Java.
This study used a mixed method design. Primary data from questionnaire and interview guides. The study was conducted in two provinces and four districts, including Semarang City, Pekalongan District, Surabaya City, and Ponorogo District. The sample included 40 health facilities, of which 24 were public and 16 private. Univariate and bivariate analyses used IBM SPSS 25.0. All surveyed public health facilities (100%, 24/24) offered HIV testing services.
Among the surveyed private facilities, 18.8% (3/16) reported that they offered HIV testing, whereas 12.5% (2/16) reported that they offered syphilis (Treponema pallidum) testing. The availability of treatment services remains very limited. A large gap also exists between HIV and syphilis testing. Among pregnant women visiting the maternal and child health (MCH) services, 3.95% were tested for HIV but did not receive syphilis testing.
Overall, Indonesia has made progress in closing the gap between HIV and syphilis testing through the introduction of dual testing. Data on the use of dual test are encouraging, with many health workers reporting that the test is easy to use and considering it as an effective approach to achieve the Triple Elimination goal by the WHO.
Keywords
- syphilis screening
- pregnant women
- dual test
According to estimates from the World Health Organization (WHO), 7 out of 1000 pregnant women worldwide are infected with maternal syphilis [1]. In 2023, this condition led to over 200,000 neonatal fatalities and 1.5 million cases of infected neonates globally, with more than two-thirds of all cases reported in Africa [2, 3]. Up to 40% of pregnant women with syphilis may deliver stillborn neonates, and 33% may have infants with low birth weight if the infection is not diagnosed and treated promptly [4]. The annual cost associated with untreated congenital and maternal syphilis is close to $310 million. Between 2011 and 2020, the global incidence of congenital syphilis rose by 500% [3, 4]. In 2020, there were 661,000 cases of congenital syphilis worldwide, equivalent to 473 cases per 100,000 live births [5]. These comprise 355,000 adverse birth outcomes, such as clinical or symptomatic congenital syphilis, low birth weight, early fetal death, neonatal mortality, preterm birth, or stillbirth [3, 4, 5, 6]. Some countries, such as Cuba, Malaysia, Maldives, Sri Lanka, and Thailand, have virtually eradicated congenital syphilis despite its rising global incidence [7]. Indonesia has one of the highest burdens of untreated congenital syphilis worldwide [4, 5, 6, 7, 8].
According to the most recent study on Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) estimates and projections in Indonesia from 2019 to 2024, the prevalence of syphilis in adults is projected to be 3.0% among Papuans and 0.8% among non-Papuans [9]. A subsequent study reported a 0.46% prevalence of active syphilis infection among pregnant women, based on the Sexually Transmitted Infections (STI) Spectrum model [6]. Finally, according to Syphilis Information and Health Assessment (SIHA), 0.5% of pregnant women in health facilities tested positive for syphilis in 2022 [5, 10]. According to demographic and prevalence estimates, at least 23,000 pregnant women who test positive for Treponema pallidum each year are at risk of giving birth to infants who have congenital syphilis [4]. In 2017, Indonesia adopted the Triple Elimination Plan, which aims to eliminate of HIV, syphilis, and hepatitis B in pregnant women by 2030 [11, 12].
In 2017, only about 1.6% of pregnant women were screened for syphilis, compared with 25.4% for HIV, representing a 23.8% disparity [12]. In 2021, Indonesia implemented the WHO’s recommendation to replace individual HIV and syphilis tests with a combined test as the initial screening for pregnant women receiving prenatal care, initially on a small scale, in an attempt to address this disparity [10, 12]. As a result, in 2022, syphilis screening increased to 24.5%, while HIV screening increased to 57.2%, resulting in a new gap of 32.7% [13]. Similar disparities persist in syphilis treatment coverage, as nearly 40% of pregnant women with syphilis did not receive treatment in 2022. By the third quarter of 2024, the syphilis screening coverage rate in Central Java was 63.2%. This coverage remains below the national target of 95%. In 2023, the Republic of Indonesia’s Ministry of Health officially introduced the HIV/syphilis combination test nationwide to reduce the screening gap and accelerate the Triple Elimination process [11]. This study aims to investigate the expansion of dual-test screening among pregnant women in Indonesia, especially in East Java and Central Java.
This study used a mixed-methods design. Qualitative data were obtained from focus group discussions (FGDs) and in-depth interviews, while quantitative data were obtained through surveys. The primary data sources consisted of responses to questionnaires and information gathered using an interview guide. The study was conducted at two provinces (four districts), including Semarang City, Pekalongan District, Surabaya City, and Ponorogo District. The sample included 40 health facilities (24 public and 16 private institutions). The criteria for selecting research sites included health service facilities that provide dual test services and willingness to participate in the study. The dual test (HIV/Syphilis) or dual test is rapid test commonly used in Indonesian. The rapid test was carried out at all health service facilities across Indonesia.
The questionnaire and interview guide were tested for validity and reliability through expert review by experts in the field of maternal and child health from the Ministry of Health of the Republic of Indonesia. The questionnaire consisted:
1. Role of Private Health Facilities.
2. Planning and Budgeting for Triple Elimination.
3. Procurement Processes.
4. Tracking Health Indicators.
5. Special Allocation Fund Management.
6. Achievements Following HIV/Syphilis Combination Testing.
Interview guide consists of:
1. Service Availability.
2. Combo Test Adoption Status.
3. Referral System.
Inclusion criteria:
1. Health facilities located in the study area, covering of two provinces (four districts), including Semarang City, Pekalongan District, Surabaya City, and Ponorogo District.
2. Facilities providing Triple Elimination services.
3. Voluntarily participating in research stages.
Exclusion criteria:
1. Health facilities that do not provide the Triple Elimination program.
2. Health facilities that refused to participate in this study.
3. Health facilities that did not complete all stages of data collection.
Data analysis was performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). Univariate and bivariate analysis were performed, using Pearson chi-square test. This study involved human participants and received ethical approval from Gadjah Mada University (KE/FK/1445/EC).
Fig. 1 shows a comparison of the proportions of HIV and syphilis testing, as
well as related medical services available between public and private health
facilities. All surveyed public health facilities (100%, 24/24) offered HIV
testing services, according to SIHA data. However, only 18.8% (3/16) of surveyed
private facilities reported offering HIV testing, while 12.5% (2/16) reported
offering syphilis testing. Among the public facilities, 62.5% (15/24) provided HIV
treatment, while 54.2% (13/24) reported offering syphilis treatment, specifically,
first-line benzathine penicillin. In private facilities, only 6.3% (1/16)
reported offering HIV treatment, while none offered syphilis treatment. Public
health facilities were approximately 5.33 times more likely to provide HIV
testing (relative risk [RR] = 5.33; 95% CI: 1.92–14.79, p
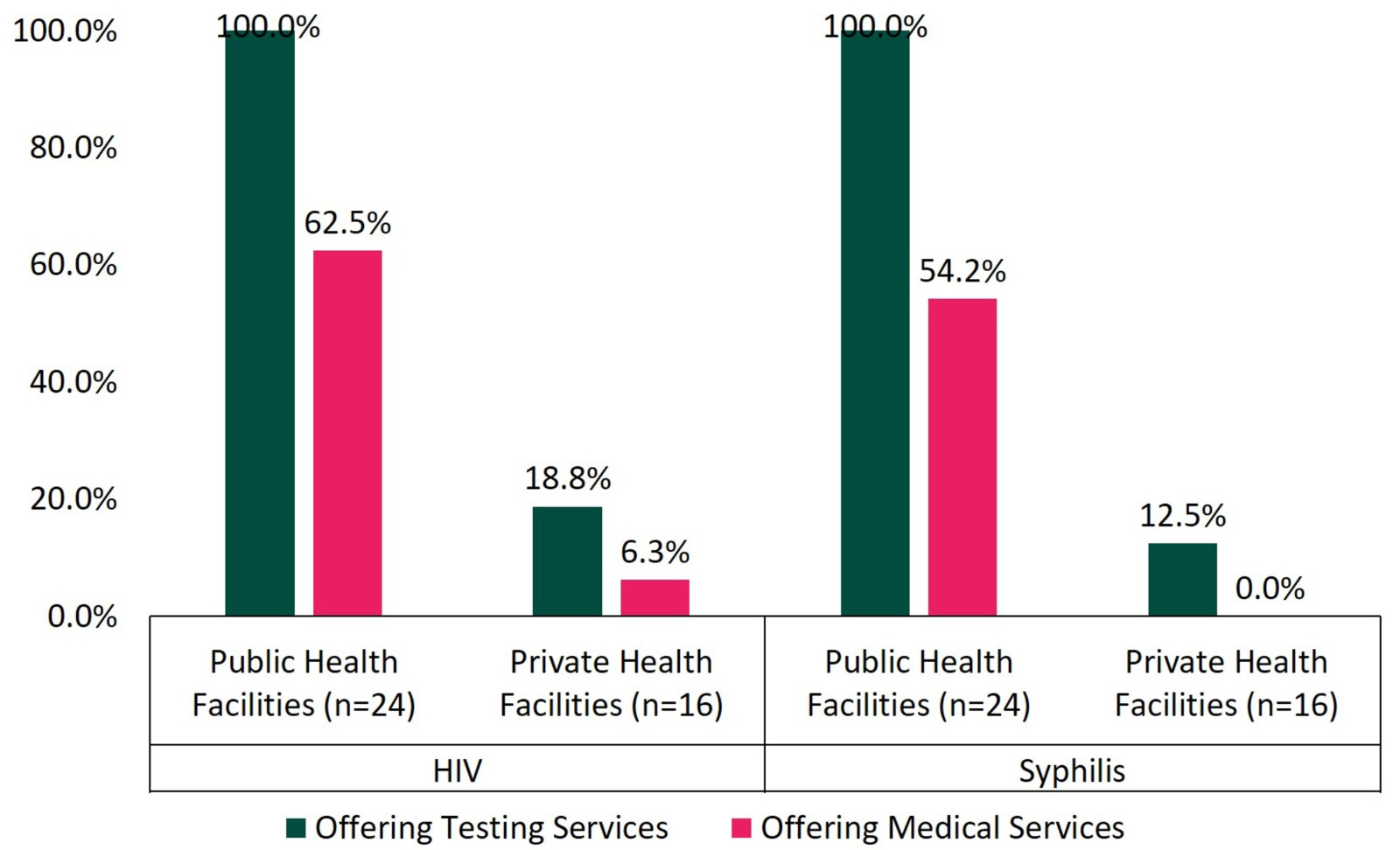 Fig. 1.
Fig. 1.
Proportion of HIV and syphilis testing and related medical services in public and private health facilities. HIV, Human Immunodeficiency Virus.
Fig. 2 presents a comparison of the proportions of HIV and syphilis testing
among pregnant women between public and private health facilities. In private
health facilities, there is a larger disparity between HIV and syphilis testing.
According to SIHA data, 3.95% of pregnant women accessing maternal and child
health (MCH) services underwent HIV testing but did not undergo syphilis testing.
This disparity can be explained by the fact that fewer private health facilities
offer syphilis testing compared to HIV testing: 31.2% provide HIV testing, while
25.0% provide syphilis testing. Public health facilities are significantly more
likely to offer HIV testing to pregnant women (RR = 2.933; 95% CI: 1.404–6.128;
p
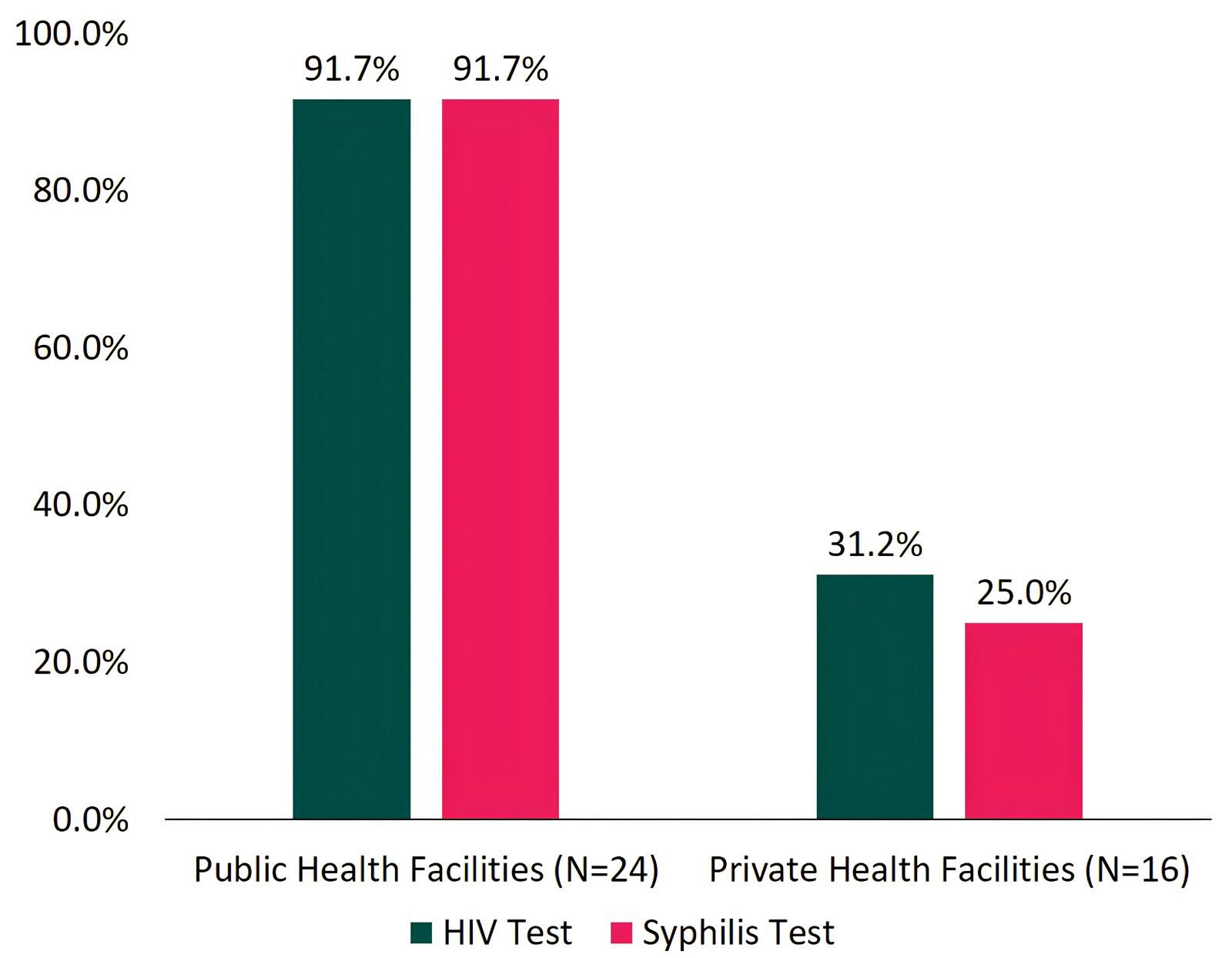 Fig. 2.
Fig. 2.
Proportion of HIV and syphilis testing among pregnant women in public and private health facilities.
Fig. 3 shows a comparison of the proportions of public and private health
facilities that had combination tests in stock and were using them on the
assessment day. Although all public health facilities (100.0%) had a stock of
combination tests on the assessment day, only 52.6% (10/19) reported having used
the tests, with most facilities receiving their stock in July 2023, while the
assessment questions explored test usage from January through July 2023. In
private healthcare facilities, only 12.5% (2/16) had a stock of combination
tests on the assessment day. Aside from these two healthcare facilities, no other
facilities reported having previously stocked these tests. Of the two healthcare
facilities that had a stock, both reported having used the combination tests.
Public healthcare facilities were 8 times more likely to have a stock of
combination tests (RR: 8.000; 95% CI: 2.188–29.249; p
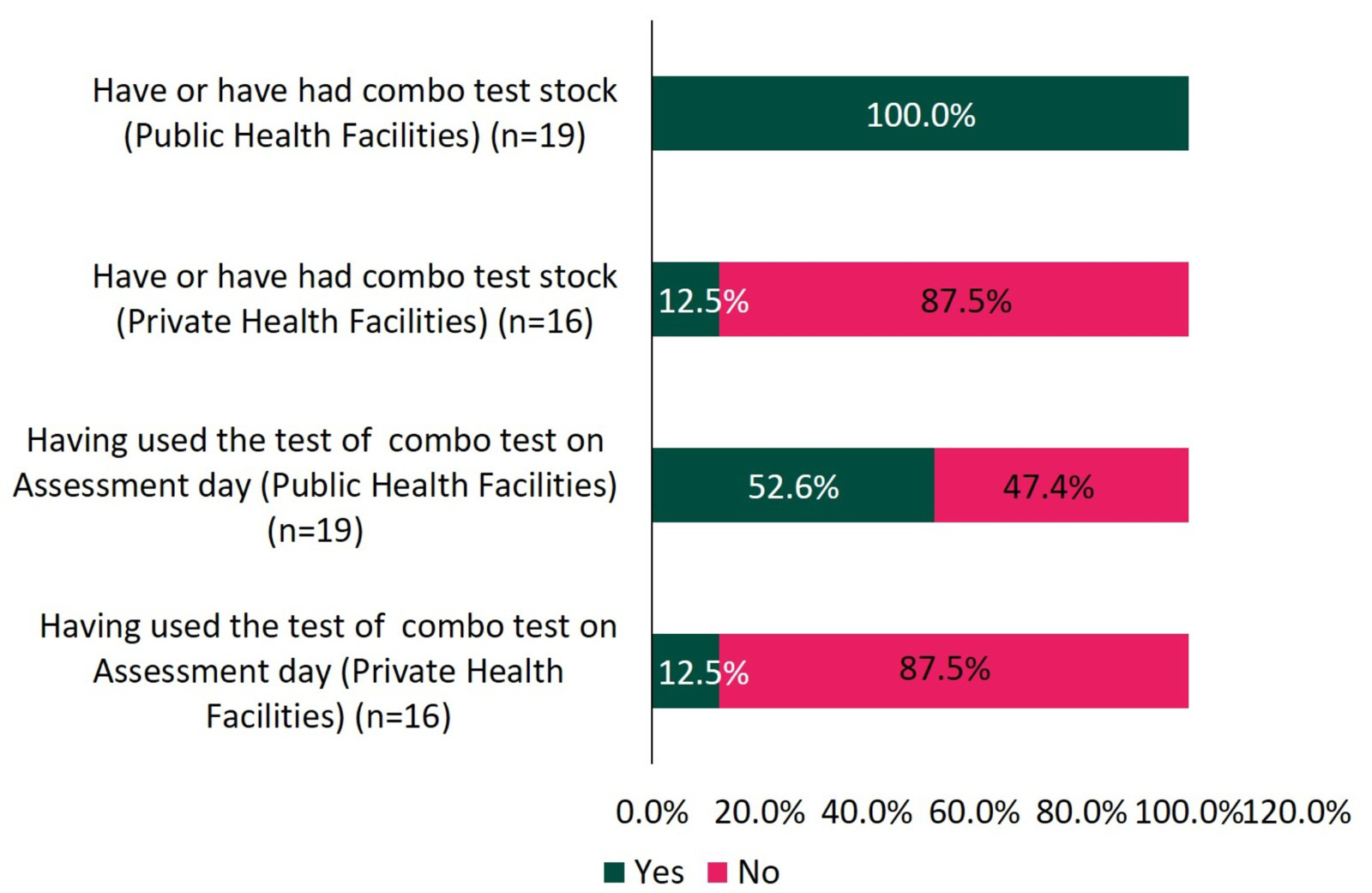 Fig. 3.
Fig. 3.
Proportion of ownership and use of combination test stock on the day of assessment in public and private health facilities.
Fig. 4 shows that, across both public and private sectors, 21 health facilities had providers who reported using the combination test. Of these, the majority reported ease of use, although only 19.0% (4/21 health facilities using the combination test) reported receiving any formal training or outreach on its use.
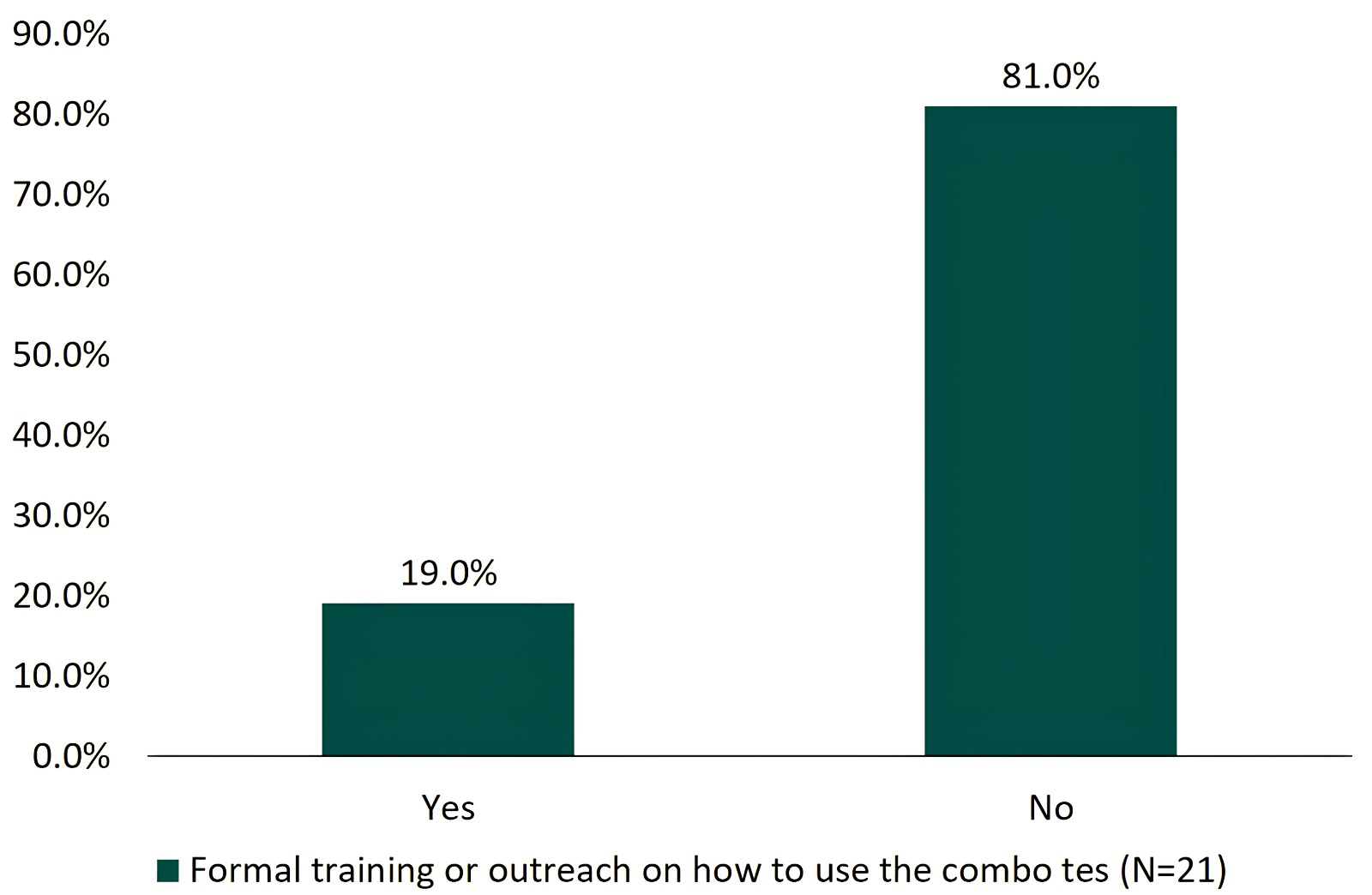 Fig. 4.
Fig. 4.
Report of health facilities receiving formal training on the use of the combination test.
Mother-to-child transmission of HIV, hepatitis B, and syphilis is preventable using similar interventions [2]. These interventions are broadly categorized as: (1) early antenatal testing and retesting in high prevalence settings, for HIV, hepatitis B and syphilis; and (2) timely treatment and management during pregnancy and postpartum [4, 7, 12]. The prevalence of HIV, syphilis, and hepatitis B among pregnant women has decreased [14]. However, these rates remain below the targets set by the Ministry of Health [10, 14]. This aligns with the WHO’s Southeast Asia regional goals, which aim to reduce the incidence and prevalence of these infections among pregnant women [7]. WHO also evaluated impact targets for HIV, syphilis, and hepatitis B; however, these impacts could not be assessed due to the lack of follow-up data on exposed infants [15]. Therefore, strengthening the health system to provide sustainable syphilis management services and to meet WHO’s established validation standards is essential [15, 16]. The Indonesian government has designated the HIV and syphilis test as a dual, or combination test, rapid screening test for pregnant women. This test offers the advantage of easy administration in healthcare facilities.
Three main digital health information systems are used in public health facilities for Triple Elimination: SIHA, Indonesia’s Hepatitis and Gastrointestinal Infectious Diseases Information System, and e-MCH cohort. The Family Health Unit of the Ministry of Health tracks MCH maternal and child health data through e-MCH, while HIV and syphilis data are collected through SIHA. Indonesia’s Hepatitis and Gastrointestinal Infectious Diseases Information System, the system used to track hepatitis and gastrointestinal infections, also tracks the number of MCH visits. There is no consistent standard for how these systems track key indicators or determine progress toward Triple Elimination [16]. At the time of the assessment, several health facilities reported the number of MCH visits based on the number of HIV and syphilis tests performed according to SIHA, while others relied on e- MCH or on manual records maintained at the health facility. Comparison MCH data across the three systems at each health facility revealed discrepancies in the number of K1 visits, indicating that the MCH data were not reliable [17].
To achieve Triple Elimination, increased syphilis testing coverage needs to be accompanied by expanded treatment of positive cases [10]. Health workers in both public and private facilities require training on the appropriate syphilis treatment protocol for pregnant women [9, 13]. This training should also be accompanied by some refresher materials on the Triple Elimination testing protocol [18]. In Indonesia, benzathine penicillin may only be administered by a doctor, although in rare cases, doctors can train health cadres to administer it. However, considering that many pregnant women seek care at midwife clinics that may not have doctors, task shifting syphilis treatment from doctors to nurses or midwives, a common practice in many other countries, may be appropriate [6, 9, 18]. During the assessment, several health workers reported concerns about adverse reactions to benzathine penicillin as a reason for not treating pregnant women who tested positive for syphilis [19].
Barriers to syphilis screening and treatment in Indonesia include limited availability of benzathine penicillin and fear of its side effects. Additionally, healthcare professionals are not always available at healthcare facilities. If a doctor is unavailable on the day a pregnant woman tests positive, healthcare professionals may offer alternative treatments (e.g., erythromycin), refer the pregnant woman to another healthcare facility, or ask her to return on a later day—all of which contribute to low syphilis treatment coverage.
The involvement of non-governmental organizations (NGOs) in monitoring the treatment of pregnant women with syphilis and hepatitis is required [20, 21]. Currently, NGO support has focused predominantly on pregnant women with HIV; however, extending this assistance to women with syphilis and hepatitis is required to enhance outcomes [20, 21]. NGOs providing guidance and support to these women can improve health outcomes and promote safer pregnancies. In addition, successful elimination of transmission of infectious diseases also requires the intersection of scientific feasibility, coordinated interventions, and political will [22]. Excellence in antenatal care and screening, the use of antiretroviral therapy and penicillin for syphilis, and appropriate follow-up of mothers and infants have yielded notable success, although overall infection control remains challenging [23].
A limitation of this study was the interviewing skills of the enumerators. Some responses to the assessment were misinterpreted by enumerators due to lack of probing skills or limited understanding of the topic. For example, when asked about the process for reporting HIV or syphilis positive cases through SIHA, respondents often replied “never been a case”. This response recurred for specific questions on the management of HIV or syphilis positive cases. The quality of these responses also suggests that the health workers participating in the Needs Assessment may not have been the most appropriate individuals to answer these questions.
The study included a limited number of samples drawn from 2 regions, despite Indonesia having 34 provinces. Only a few health service facilities were included, and their selection system was based on the Ministry of Health’s and the Provincial Health Office’s assessment of which facilities had greater knowledge regarding the conditions in the study area. The migration of SIHA also limited the data quality, as some health facilities were unable to access the platform and were therefore unable to enter data during or before the Needs Assessment. As a result, some health facilities lacked complete data for the collected indicators. As a solution, health workers provided data taken from other recording systems, such as e-MCH cohort and Indonesia’s Hepatitis and Gastrointestinal Infectious Diseases Information System, to the data collectors. This created challenges for data interpretation, as data analysis showed discrepancies and inconsistencies between SIHA and the alternative records.
Overall, Indonesia has made progress in closing the gap between HIV and syphilis testing through the introduction of combination testing. Data on the use of dual testing are encouraging, as many health workers report that the test is easy to use and consider it an effective approach to support the Triple Elimination goal. However, unless testing and treatment are available at all health facilities that provide maternal and child health services, especially private health facilities, some pregnant women who attend MCH services may not receive HIV and syphilis testing and treatment. In addition, efforts to simplify the recording and reporting system and reduce the burden on health workers will likely improve data quality and encourage private health facilities to offer HIV and syphilis services.
The datasets used and analyzed during the current study are available from the authors upon reasonable request.
SW: conceptualization, funding acquisition, resources, data curation, formal analysis, supervision, investigation, writing—original draft, writing—review & editing. LF: formal analysis, software, visualization, writing—original draft, writing—review & editing. ELis: funding acquisition, methodology, supervision, investigation, project administration. HN: investigation, supervision, project administration, data curation. ELuk: conceptualization, Validation. NA: conceptualization, validation. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Gadjah Mada University: KE/FK/1445/EC.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.