




1 Department of Medical Genetics, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, 610041 Chengdu, Sichuan, China
3 Department of Obstetrics and Gynecology, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
Abstract
Stillbirth is among the most severe adverse pregnancy outcomes. Over the past three decades, the global number of stillbirths has steadily declined. Despite this progress, the overall burden remains high, with rates ranging from 2.9 to 22.8 per 1000 births. This underscores the need for improved clinical care to further lower stillbirth rates. Identifying risk factors and implementing etiology-based clinical management remain challenging.
This review summarizes recent evidence on risk factors, causes, and active intervention measures for stillbirth. This narrative review is based on a search of Ovid MEDLINE and EMBASE (Excerpta Medica Database) databases conducted in October 2025.
Most stillbirths (~77.4%) occur in low-resource regions such as South Asia and sub-Saharan Africa. Strong associations link stillbirth to modifiable factors in these regions, including lower maternal education, out-of-hospital delivery, limited access to antenatal care, vaginal instrumental delivery, and cesarean section. Nonmodifiable or potentially modifiable risk factors, such as pre-existing hypertension, obesity, excessive gestational weight gain, smoking, and alcohol consumption, are more commonly associated with stillbirth in high-income countries. More than 80 classification systems are currently in use worldwide to categorize the causes of stillbirth, yet many cases remain unclassified. Pathological evaluation of the placenta, umbilical cord, and fetal membranes is one of the most valuable tools for investigating the etiology of stillbirth in all settings. Genetic testing also plays an essential role in identification of underlying causes when accessible. A stratified framework for risk identification and etiological classification, along with an individualized preventive approach tailored to specific circumstances and available resources, should be implemented to address modifiable risk factors before conception or throughout pregnancy. Genetic counseling and reproductive planning should be provided for cases of fetal genetic abnormalities.
Active identification of potential risk factors for stillbirth and management of modifiable factors are essential in all pregnancies. A multidimensional evaluation can help determine the underlying cause of stillbirth, including detailed review of obstetric records, gross and pathological examination of the fetus, placenta, associated tissues, and genetic testing when available. Therefore, a tailored, tiered approach based on local etiological classifications could be implemented to reduce the risk of recurrent stillbirth.
Keywords
- stillbirth
- risk factor
- placenta
- fetus
- preterm prelabor rupture of membranes
Stillbirth is a severe pregnancy outcome, affecting approximately two million third-trimester fetuses in 2019 [1, 2]. Definitions of stillbirth vary. The American College of Obstetricians and Gynecologists (ACOG) and Society for Maternal-Fetal Medicine (SMFM) define it as fetal death occurring at or after 20 weeks of gestation, or a birth weight above 350 grams if gestational age is unknown [3]. The World Health Organization (WHO) defines stillbirth as fetal death occurring at 28 weeks of gestation or later [4]. The French College of Obstetricians and Gynecologists (CNGOF) defines stillbirth as the spontaneous cessation of cardiac activity beyond 14 weeks of gestation [5]. These differing definitions lead to variations in reported incidence and complicate regional comparisons. This narrative review searched Ovid MEDLINE, https://www.ovid.com/ (MEDLINE accessed via the Ovid platform) and EMBASE, https://www.embase.com/ (Excerpta Medica Database) databases using terms such as “stillbirth”, “fetal death”, “risk factor”, “etiology”, “cause”, “prevention”, and “prenatal care”. The final search was completed in October 2025. Relevant literature on epidemiology, risk factors, cause classification, and preventive measures for stillbirth was reviewed and summarized.
The global stillbirth rate at or after 28 weeks of gestation is estimated at 13.9 per 1000 total births. This rate ranges from 2.9 per 1000 in Western Europe to 22.8 per 1000 in West and Central Africa. This estimate is based on a systematic review of 195 countries from 2000 to 2019 [2]. Another study reported a global stillbirth rate of 16.1 per 1000 births in 2021 for cases occurring at or after 28 weeks of gestation [6]. The global stillbirth rate at or after 20 weeks of gestation in 2021 was 23.0 per 1000 births. Based on these estimates, about 0.926 million stillbirths— representing 30.5% of the global total—occurred between 20 and 28 weeks of gestation [6]. Intrapartum stillbirth rates are about 1 per 1000 births in high-resource countries but can reach 20–25 per 1000 births in some low-resource regions [7]. Despite a steady decline in global stillbirth numbers over the past three decades, the rate decreased by 39.8%, from 5.08 million in 1990 to 3.04 million in 2021. Nevertheless, the overall burden remains alarmingly high, especially in South Asia and sub-Saharan Africa. These regions accounted for 77.4% of global stillbirths in 2021, an increase from 60.3% in 1990 [6, 8]. Ending preventable stillbirth has become a central long-term priority in global maternal and child health initiatives [9]. Strengthening the identification of risk factors and applying clinical management based on etiology are critical but challenging strategies for reducing stillbirth incidence.
Factors that are rarely observed in live births but frequently present in stillbirth cases are considered potential causes. Conversely, factors commonly found in live births and even more prevalent in stillbirths are more likely risk factors [7]. Nevertheless, distinguishing between risk factors and causes of stillbirth remains a significant challenge. For clarity, risk factors are defined as conditions associated with an elevated likelihood of stillbirth, whereas “causes” refers to the direct pathological mechanisms leading to fetal death.
Current evidence identifies non-Hispanic Black race, extremes of maternal age (very young or advanced), and elevated prepregnancy body mass index (BMI) as prepregnancy risk factors for stillbirth [1, 3, 10, 11]. Women with a history of stillbirth, preterm birth, or small-for-gestational-age (SGA) infant face an increased risk of stillbirth in subsequent pregnancies. The smaller and more preterm the prior infant, the greater the risk in the subsequent pregnancy [12, 13]. Additional risk factors include assisted reproductive technology, multiple gestations, excessive gestational weight gain, and post-term pregnancies beyond 41 weeks. Medical conditions during pregnancy, such as antiphospholipid syndrome (APS), fetal growth restriction (FGR), placental abruption, genetic abnormalities, thyroid disorders, thrombophilia, malaria, intrahepatic cholestasis of pregnancy, systemic lupus erythematosus, renal disease, and intrauterine infections, are also associated with stillbirth [1, 3, 10, 11, 14, 15, 16].
Risk factors for stillbirth are closely associated with regional health and economic conditions. Specifically, in low- and middle-income countries (LMICs), stillbirth is strongly associated with lower education, limited access to antenatal care, out-of-hospital births, delivery by less-skilled providers, lack of availability of assisted vaginal delivery, and low cesarean section rates [17, 18, 19]. In contrast, stillbirths in high-income countries are more often associated with non-modifiable or potentially modifiable factors. These include pre-existing hypertension, obesity, excessive gestational weight gain, smoking more than 10 cigarettes per day, alcohol consumption, illicit drug use, and sleeping in a supine position during pregnancy [15]. Emerging evidence also indicates positive associations between stillbirth and environmental exposures, including annual average PM2.5 concentration [20], high heat exposure [21], and pesticide exposure [22]. These findings suggest that regional context is critical in understanding and addressing stillbirth risk factors.
The “causes” of stillbirth are conditions with a direct causal relationship to the outcome. Establishing such definitive conclusions remains challenging. For instance, evaluating maternal and fetal infections is crucial in identifying causes of stillbirth. However, infections may trigger a prolonged pathological cascade, making it difficult to determine their primary causative role [23]. Assigning causes of death in stillbirths has clear clinical value, which has led to the development of over 80 classification systems worldwide. Among the most widely used systems are the Perinatal Society of Australia and New Zealand Perinatal Death Classification (PSANZ-PDC), Causes of Death and Associated Conditions (CODAC), the WHO application of the International Classification Of Diseases (ICD), 10th revision, to deaths during the perinatal period (ICD-PM), classification system according to Relevant Condition at Death (ReCoDe), and Stillbirth Collaborative Research Network (SCRN), as summarized in Table 1 (Ref. [24, 25, 26, 27, 28, 29, 30, 31, 32]). In high-resource settings, complex systems offer greater nuance, precision, and specificity. However, the required data may be unavailable or unaffordable in low-resource settings. For example, a prospective observational study in South Africa reported that obstetricians used a modified version of the SCRN classification system to determine and classify the causes of stillbirth. A likely or probable underlying cause was identified in 82% of cases. Specifically, maternal medical conditions accounted for 21% (64/298) of cases, predominantly hypertensive disorders. Placental or fetal infections accounted for 19% (58/298) of cases and included histopathological evidence of inflammation in fetal membranes and the placenta, as well as circulatory abnormalities [33].
| Origin | Core features | Data/diagnostic requirements | Strengths/limitations | Typical proportion of unexplained stillbirths |
| PSANZ-PDC [24] | Uses obstetric antecedent factors to identify the primary contributor initiating the cascade of events leading to fetal death, following a predominantly hierarchical structure arranged in descending order, with specific criteria clearly defined in the accompanying Guidelines for Use. | Clinical data and autopsy findings, including placental histology. | Classified independently according to PSANZ-PDC and PSANZ-NDC using standardized and systematic processes, demonstrating a high level of consistency and a high rate of information retention [25]. | Approximately 20%~30% [24, 26] |
| Relies on trained physicians to perform the classification. | ||||
| CODAC [27] | Includes ten main categories and 94 subcategories, designed to record both the underlying cause of death and up to two contributing conditions. | Comprehensive investigation, placental pathological examination, and fetal autopsy. | Offers strong practicability; however, the presence of multiple levels and coding options may complicate usability and increase user training requirements. | Approximately 17% [28] |
| ICD-PM [29] | A globally applicable system classifies perinatal mortality by integrating the timing of death and associated maternal factors. By recognizing the mother–infant dyad, the system facilitates the identification of key areas for targeted programmatic interventions. | Clinical history, laboratory examinations, and placental pathological examination. | Promote a unified system to enhance global data comparability and improve usability, while emphasizing the maternal-infant relationship. | Over half of antepartum fetal deaths [30] |
| Exhibits relatively low specificity and is highly sensitive to the completeness of available information. | ||||
| ReCoDe [31] | Identifies the clinically relevant conditions present at the time of intrauterine death and aims to determine what went wrong, without necessarily establishing the underlying etiology, using a hierarchical classification structure that emphasizes FGR. | Clinical data, placental pathological examination, and fetal autopsy. | Focuses on directly relevant clinical scenarios with strong practical applicability, emphasizing modifiable factors. | Approximately 15.2% [31] |
| Category specificity should be enhanced, and placental examination should be conducted independently. | ||||
| SCRN [32] | Aims to identify the causes of stillbirth in a racially and geographically diverse population across the United States. | Clinical history review, autopsy, placental pathology, and karyotype or chromosomal microarray analysis. | Features high data quality and multidisciplinary collaboration. | Approximately 24% [32] |
| The workflow is complex, and the focus remains predominantly on research-oriented tools. |
Note: PSANZ-PDC, Perinatal Society of Australia and New Zealand Perinatal Death Classification; PSANZ-NDC, Perinatal Society of Australia and New Zealand Neonatal Death Classification; CODAC, Causes of Death and Associated Conditions; ICD-PM, ICD-10 to deaths during the perinatal period; ReCoDe, Relevant Condition at Death; FGR, fetal growth restriction; SCRN, Stillbirth Collaborative Research Network.
Overall, stillbirth causes can be classified into maternal, fetal, placental, and umbilical factors. Maternal conditions include diabetes, thrombophilia, hypertension, renal disease, thyroid dysfunction, and uterine defects [34]. In a study of 75,132 births, including 949 stillbirths, preeclampsia and eclampsia were associated with an 11.7% increase in antepartum stillbirths [35]. An individual-level data analysis in middle- and high-income countries reported that about three-quarters of stillbirths occurred before term [36]. Most preterm stillbirths result from spontaneous preterm birth associated with preterm labor, cervical insufficiency, preterm prelabor rupture of membranes (PPROM), chorioamnionitis, and placental abruption, which lead to delivery at a previable or periviable gestational week [32]. Approximately one-fifth of post-term stillbirths involved SGA infants, with a strong, graded association observed between stillbirth risk and fetal growth patterns [36]. Fetal congenital anomalies, including structural malformations and genetic abnormalities such as aneuploidy and monogenic disorders, represent another major cause of stillbirth. Major structural abnormalities include hydrops fetalis, cystic hygromas, heart failure, thoracic and craniofacial defects, and multiple congenital anomalies [37]. Placental and umbilical cord complications represent another significant cause of intrauterine fetal death. The main placental abnormalities include placenta previa, vasa previa, placental abruption, and placental insufficiency. Umbilical cord abnormalities include entrapment, knots, excessive torsion, narrowing, cord prolapse, vasa previa, and compromised fetal microcirculation. A prospective study using robust data and comprehensive cause-of-death analysis reported that these abnormalities accounted for 19% of all stillbirths and 28% of those occurring at or after 32 weeks of gestation [38].
Notable differences exist in the etiologies underlying antepartum stillbirth and intrapartum stillbirth. Major causes of antepartum stillbirth include maternal medical conditions during pregnancy, clinical obstetric complications, intrauterine infection, pathological placental conditions, and congenital malformations [7, 33, 34]. Antepartum hemorrhage, obstructed or prolonged labor, birth asphyxia, preterm birth, and neonatal infections are primary contributors to intrapartum fetal death [32, 33].
Accurately determining the cause of stillbirth requires a comprehensive obstetric record, including documentation of vaginal bleeding, fetal heart rate, maternal blood pressure, as well as gross and histological examination of the placenta and fetus. Omission of any one of these core diagnostic components often leads to an inconclusive determination of cause in a substantial proportion of stillbirth cases. A thorough medical, obstetric, and genetic history should always be obtained. In a study by the SCRN, which included 80 of 512 stillbirths undergoing complete evaluation, placental pathology (64.6%) was the most informative test, followed by fetal autopsy (42.4%) and genetic testing (11.9%) [39].
A stepwise evaluation, beginning with the obstetric record and laboratory findings, followed by placental pathological examination and, subsequently, fetal autopsy was applied in a cohort of 144 stillbirth cases. Clinical and laboratory data alone identified the cause of fetal death in 24% of cases. After integrating placental pathological assessment, the proportion of cases with an identified cause increased to 61% and further rose to 74% with the addition of autopsy findings [40]. Accordingly, placental pathological examination is expected to guide clinical management in 36% of cases, while fetal autopsy contributed to additional management modifications in 6%.
A comprehensive analysis of family, maternal, and obstetric histories, followed
by a thorough review of the current pregnancy, provides essential information.
The family history should include congenital anomalies, hereditary disorders, and
consanguinity. Maternal history encompasses prior diabetes mellitus, chronic
hypertension, thrombophilia, autoimmune diseases, heart disease, and the use of
potentially teratogenic medications. Obstetric history includes recurrent
miscarriages, previous offspring with congenital anomalies, hereditary
conditions, FGR, or fetal demise, as well as prior gestational hypertension or
preeclampsia, gestational diabetes mellitus, or placental abruption. Key factors
for the current pregnancy include maternal age, gestational age, preexisting or
newly developed medical conditions, pregnancy weight gain and BMI, complications
associated with multifetal gestation, placental abruption, abdominal trauma,
preterm labor or premature rupture of membranes, gestational age at onset of
prenatal care, ultrasound-detected abnormalities, vaginal bleeding, fetal heart
rate, maternal blood pressure, and evidence of infections or chorioamnionitis
[3]. Maternal laboratory testing should be tailored to clinical indications, such
as complete blood count, Kleihauer-Betke test, screening for thrombophilias
(lupus anticoagulant, anticardiolipin, and anti-
Consequently, evaluations of the placenta, umbilical cord, and fetal membranes—both gross, histologic, and, when indicated, microbiological—are considered among the most effective diagnostic tests for confirming or excluding potential causes of death through standardized, comprehensive evaluation [39, 41, 42]. In all cases involving fetal anomalies, external physical examination, medical photography, and standard radiographic or computed tomography imaging should be performed [43]. Parents should be offered counseling on options for full, limited, or stepwise postmortem examination in both high-income and LMICs.
The Amsterdam Placental Workshop Group established standardized criteria for placental sampling, gross examination descriptions, pathological terminology, and diagnostic definitions. Consensus was achieved on the nomenclature and histological features of maternal and fetal vascular malperfusion, delayed villous maturation, patterns of ascending intrauterine infection, and villitis of unknown etiology [44]. The standard procedure included an initial assessment; external and internal macroscopic examination, including fetal measurements and imaging; dissection and inspection of the organ block; collection of tissue samples; and microscopic examination [45]. When parents remain reluctant to consent to a complete autopsy, alternative approaches may be offered, including partial autopsy, imaging via ultrasound or magnetic resonance imaging (MRI), gross examination by a trained pathologist, and minimally invasive tissue sampling [46, 47]. Timely communication before and after autopsy among the primary healthcare provider, the perinatal pathologist, and the parents is essential. The primary healthcare provider should meet with the family during follow-up to discuss autopsy findings, plan management strategies for future pregnancies, obtain consent for additional testing, and provide genetic counseling to other family members when indicated [43].
With the expanded understanding of the genetic basis of stillbirth and advances in genetic testing technologies, genetic testing has become particularly important for identifying the underlying genetic causes of stillbirth in high-income countries. It supports key Information to guide decision-making in subsequent pregnancies.
Karyotype analysis is a foundational method for detecting aneuploidies, large chromosomal deletions or duplications (exceeding 7–10 Mb), and structural rearrangements [48, 49]. Studies report that a successful karyotype identifies chromosomal abnormalities in 6–13% cases of stillbirth. The diagnostic yield increases significantly, exceeding 20%, when fetal structural anomalies or growth restriction are present. The most prevalent aneuploidies associated with stillbirth are Trisomy 21, Trisomy 18, Trisomy 13, and Monosomy X [49, 50]. Chromosomal microarray analysis (CMA) is another core genetic test that improves both the success rate and sensitivity for detecting genetic abnormalities in stillbirth compared with conventional karyotyping. In a population-based study, postmortem examinations and genetic testing were performed on 532 stillbirths. CMA demonstrated improved detection of genetic abnormalities (8.3% vs. 5.8%) and a higher success rate than karyotyping (87.4% vs. 70.5%). Among the subgroup of antepartum stillbirths (443 cases), CMA identified a greater proportion of cases with genetic defects (8.8% vs. 6.5%), as it did in the subgroup with congenital anomalies (67 cases; 29.9% vs. 19.4%). Compared with karyotyping, CMA increased the diagnostic yield for genetic abnormalities by 41.9% across all stillbirths, 34.5% in antepartum cases, and 53.8% in cases with structural anomalies [50]. Therefore, CMA is recommended when further cytogenetic investigation is indicated in intrauterine fetal demise or stillbirth [51, 52].
In addition, molecular diagnoses were established in 6.1% of stillbirth cases (15/246) through exome sequencing (ES). A significant enrichment of loss-of-function variants was observed in genes highly intolerant to such mutations in the human population (odds ratio [OR]: 2.15; 95% confidence interval [CI]: 1.46 to 3.06). Notably, these variants in mutation-intolerant genes were predominantly identified in genes not previously associated with known human diseases (OR: 2.22; 95% CI: 1.41 to 3.34) [53]. For fetuses presenting with structural anomalies, particularly those with presumed lethal phenotypes, a comprehensive autopsy followed by trio-based ES is strongly recommended [54]. A definitive molecular diagnosis has been reported in 35.5% (93/262) of fetuses with structural anomalies, and nearly two-thirds of stillbirth cases receiving a genetic diagnosis involve those with multiple anomalies [55]. A retrospective study evaluating perinatal multidisciplinary assessment, postmortem examination, and at least CMA testing in perinatal death cases with structural anomalies reported that the diagnostic yield increased from 24% (29/123) to 45% (29/64) in stillbirth cases with a suspected genetic etiology. Postmortem examination revealed phenotypic findings in 79% of cases. Genomic testing provided a valuable complement to postmortem evaluation in structurally abnormal perinatal deaths, improving diagnostic accuracy without substituting for pathological examination [56].
Genome sequencing (GS) is not currently part of standard clinical practice but may become available in the future. Another study evaluated genomic autopsy, using either GS or ES, as an adjunct to conventional autopsy in 200 families who had experienced fetal or neonatal death, with phenotypes ranging from severe congenital malformations to unexplained fetal demise. This study established a definitive or candidate genetic diagnosis in 52.5% of families, providing robust evidence that genomic autopsy offers significant advantages over current diagnostic approaches for investigating perinatal death [57].
For pregnancies presenting with modifiable risk factors for stillbirth, particularly those in low-income settings, targeted interventions should be implemented to reduce risks. Over three-quarters of perinatal deaths are associated with identifiable delays in accessing or receiving healthcare services, nearly half of which are considered preventable— primarily due to modifiable factors including inadequate maternal health-seeking behaviors and substandard intrapartum care. In previous stillbirths attributed to maternal conditions, management focuses on preconception intervention and continuous monitoring throughout pregnancy. Actively recognizing and addressing modifiable risk factors, including—but not limited to—hypertension, obesity, diabetes, and chronic infections, is strongly recommended when preparing for pregnancy. Thus, lifestyle modifications and pharmacological therapy are essential for achieving optimal control of underlying risk factors. Multidisciplinary assessment should be initiated to facilitate early detection and monitoring of obstetric complications once pregnancy is confirmed [3, 15, 58].
For previous stillbirths attributed to fetal genetic abnormalities, precise recurrence risk assessment and targeted reproductive interventions should be arranged. Evidence-based genetic counseling should be provided to couples with positive molecular findings, and preimplantation genetic testing (PGT) or prenatal diagnosis following natural conception should be offered when indicated to prevent the transmission of pathogenic variants and reduce the risk of stillbirth recurrence in subsequent pregnancies [55, 57]. In cases of previous stillbirth due to impaired placental perfusion or thrombophilia, early monitoring of placental function and prophylactic anticoagulation, when indicated, should be considered in subsequent pregnancies [59]. Although conventional ultrasound techniques, such as serial fetal biometry and Doppler assessment of the umbilical and uterine arteries, are routinely employed in the management of high-risk pregnancies, additional parameters—including placental dimensions and structural characteristics—remain underexplored [60]. Integrating etiology-specific strategies, from post-stillbirth diagnostic findings to precision-guided care, would provide more effective management in subsequent pregnancies. A simplified flowchart outlining the process of stillbirth evaluation is presented in Fig. 1.
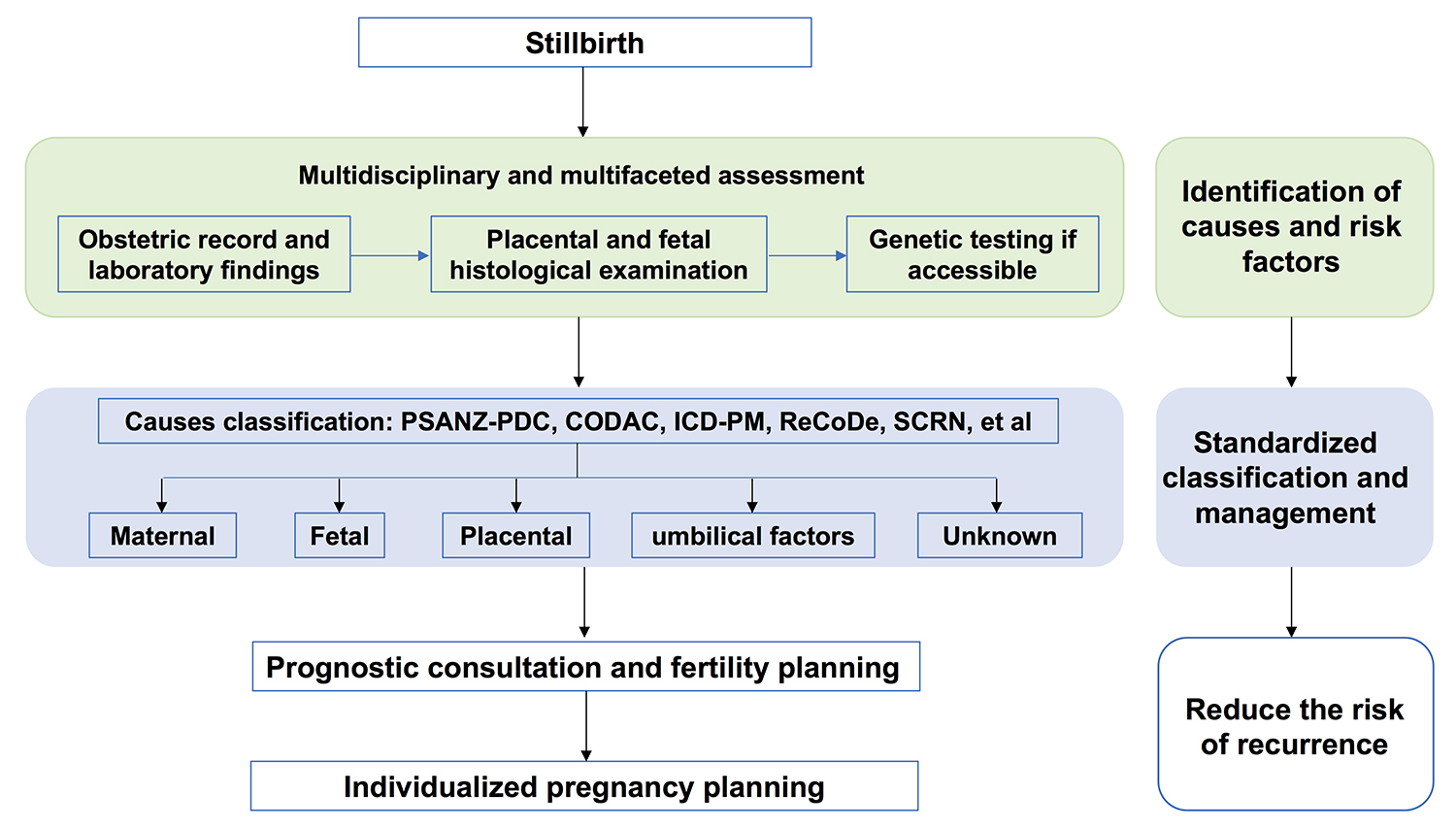 Fig. 1.
Fig. 1.
Flowchart illustrating the stillbirth evaluation process.
This review has several limitations. As a narrative review, it does not provide formal clinical recommendations, nor does it assess the strength of the evidence. Instead, it focuses on synthesizing the existing literature relevant to risk factor identification, cause classification, and etiology-based clinical considerations. Although several assessment methods are recognized as diagnostic approaches for stillbirth, further research is needed to generate robust evidence on scalable strategies in LMICs, the global standardization of placental pathology reporting, the cost-effectiveness of molecular autopsy in accessible settings, and interventions that can be widely implemented to reduce intrapartum stillbirth.
In summary, although global stillbirth rates have steadily declined over the last thirty years, stillbirth remains one of the most devastating adverse pregnancy outcomes and continues to pose a significant public health challenge. Achieving further reductions in stillbirth incidence remains a substantial and ongoing challenge. Based on existing evidence, in resource-limited areas, a detailed medical history review and a gross pathological examination are fundamental and highly recommended. In high-income countries, a comprehensive assessment involving detailed obstetric histories, pathological evaluation, and genetic testing, can help determine the underlying causes of stillbirth to the greatest extent possible. In addition to identifying the most likely causes, an individualized management strategy should be implemented to actively address modifiable preconception risk factors, provide reproductive guidance when indicated, and monitor maternal health during pregnancy. These strategies, applied to both previous stillbirths and subsequent pregnancies, are critical for accelerating reductions in stillbirth.
FZ and XW conceptualized and designed the study. FZ, YL, and JZ conducted a comprehensive review of the relevant literature and analysis of the literature. FZ drafted the initial manuscript. All authors contributed to subsequent revisions and provided critical feedback during the revision process. All authors read and approved the final version of the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work, the authors used Grammarly to check spelling and grammar. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.