






 , Saime Ozbek Sebin 2
, Saime Ozbek Sebin 21 Department of Obstetrics and Gynecology, University of Health Sciences, Erzurum City Hospital, 25240 Erzurum, Türkiye
2 Department of Physiology, Faculty of Medicine, Atatürk University, 25240 Erzurum, Türkiye
Abstract
This case-control study explored circulating endothelial cell-specific molecule-1 (endocan), a marker of vascular impairment, in women diagnosed with missed abortion and compared the findings with those of healthy pregnant controls. In addition, the associations between serum endocan levels and two oxidative stress markers, malondialdehyde (MDA) and nitric oxide (NO), were assessed.
A total of 83 participants were divided into two cohorts: the missed abortion group (n = 44) and the control group (n = 39), each comprising of women with a singleton intrauterine pregnancy. Serum levels of endocan, MDA, and NO were quantified using enzyme-linked immunosorbent assay (ELISA).
Women with missed abortion exhibited significantly elevated serum concentrations of endocan (p = 0.029), NO (p = 0.011), and MDA (p = 0.021) compared with the control group. Endocan levels showed strong positive correlations with NO (r = 0.795, p < 0.001) and MDA (r = 0.685, p < 0.001). A similar positive correlation was observed between NO and MDA (r = 0.685, p < 0.001). In multivariate regression analysis, both MDA (β = 0.26, t = 3.00, p = 0.004) and NO (β = 0.61, t = 6.94, p < 0.001) were significant predictors of serum levels.
Serum levels of endocan, NO, and MDA were higher in women diagnosed with missed abortion than in healthy pregnant controls. These findings support the presence of endothelial dysfunction in missed abortion.
The study has been registered on https://zenodo.org/ (registration number: zenodo. 17910736; registration link: https://zenodo.org/records/17910736).
Keywords
- endocan
- nitric oxide
- malondialdehyde
- missed abortion
- oxidative stress
Missed abortion refers to a condition in which the uterus remains quiescent while retaining an embryo that lacks cardiac activity or a gestational sac that contains no embryo [1]. Between the 4th and 20th gestational weeks, approximately 12%–15% of clinically recognized pregnancies conclude as abortion, a situation that holds significant importance in obstetric practice because of the maternal complications it may cause. Although maternal, fetal, and paternal factors have been implicated, the precise mechanism underlying missed abortion has not been fully clarified. Damage to the vascular endothelium may impair embryo implantation in the endometrium, promote ischemic injury, or disrupt placental function, thereby inhibiting fetal development. Consequently, any condition capable of altering microcirculation may contribute to the occurrence of missed abortion [2].
Endothelial cell-specific molecule-1 (endocan) is a soluble dermatan sulfate proteoglycan produced by endothelial cells and is recognized as a novel inflammatory indicator reflecting endothelial dysfunction. This molecule participates in several biological processes—including cell proliferation, migration, adhesion, and neovascularization—and regulates multiple inflammatory events. Increased endocan expression has been documented in response to inflammatory stimuli, and its serum concentration has been suggested as a marker of both the presence and the intensity of inflammation [3, 4]. Given that endocan reflects vascular endothelial injury, we postulated that it could be associated with the etiopathogenesis of missed abortion.
Malondialdehyde (MDA) is commonly used as a biochemical marker of lipid peroxidation, and elevated plasma MDA concentrations are considered indicative of the extent of cellular injury and various pathological processes [5].
Nitric oxide (NO), due to its free-radical nature, low molecular mass, and strong reactivity, has a very short half-life (2–30 seconds). It is released rapidly and participates in numerous physiological and pathological mechanisms. Its ability to diffuse across biological membranes without requiring receptors makes NO an efficient and versatile signaling molecule [6, 7].
Experiencing a missed abortion can inflict significant physical and psychological distress on pregnant women and their families. Couples who repeatedly seek medical care often encounter substantial emotional and financial strain. Identifying biomarkers that may help predict the likelihood of missed abortion is therefore of great clinical relevance. Although previous studies [8, 9] have indicated an imbalance between oxidants and antioxidants in women diagnosed with missed abortion, serum endocan concentrations in this patient group have not yet been examined.
This case-control study received approval from the Ethics Committee of Atatürk University, Faculty of Medicine (approval no: B.30.2.ATA.0.01.00/414) and was conducted in accordance with the principles of the Declaration of Helsinki. The research was carried out at the University of Health Sciences, Erzurum City Hospital, Clinic of Obstetrics and Gynecology (Türkiye), between April and July 2024. Written informed consent was obtained from all participating women.
A total of 83 pregnant women aged 18–40 years who attended routine antenatal assessment between 7 and 12 gestational weeks were recruited. Women with multiple gestations, thrombophilia, chronic, endocrine, infectious, autoimmune, or inflammatory disorders, vaginal bleeding during pregnancy, medication use (including progesterone, antibiotics, or iron supplementation), alcohol, tobacco, or substance use, or those undergoing medical termination of pregnancy were excluded. Furthermore, pregnancies conceived through in vitro fertilization were not included. All eligible women underwent transvaginal ultrasonography to confirm the presence of a viable intrauterine pregnancy or to diagnose a missed abortion.
Two study groups were created. The control group included women with a confirmed viable singleton intrauterine pregnancy. Gestational dating was performed by measuring the maximal embryonic pole diameter up to 9 weeks of pregnancy or by evaluating crown-rump length and cardiac activity when present [10].
The missed abortion group consisted of women at
Demographic data and obstetric histories were recorded for all participants. For women diagnosed with missed abortion, blood samples were obtained immediately after diagnosis. Under sterile conditions, 5 mL of venous blood was drawn, centrifuged at 3000 rpm for 10 minutes, and the resulting serum was stored at –80 °C until biochemical analyses were performed. Serum concentrations of endocan, NO, and MDA were measured using enzyme-linked immunosorbent assay (ELISA) kits according to the manufacturer’s protocols. The kits used included: Human MDA ELISA (catalogue no: E1371Hu; BT LAB, Shanghai, China), Human NO ELISA (catalogue no: E1510Hu; BT LAB, Shanghai, China), and Human ESM-1 ELISA (catalogue no: E3160Hu; BT LAB, Shanghai, China). All assays were within manufacturer-defined reference intervals. Concentrations of endocan, NO, and MDA were expressed in ng/L, µmol/L, and µmol/L, respectively.
The main outcome variable was the difference in serum endocan levels between the
two groups. Sample size estimation was based on the findings of Yoruk et
al. [12], where endocan levels were reported as 620
All statistical analyses were performed using IBM SPSS Statistics version 20
(SPSS Inc., Chicago, IL, USA). Endocan, NO, and MDA values were summarized as
means, standard deviations, counts, and percentages. The Shapiro-Wilk test was
used to assess the normality of continuous variables. For normally distributed
parameters, comparisons between two independent groups were performed using the
independent-samples t-test, whereas the Mann-Whitney U test was used for
non-normally distributed variables. Pearson’s correlation coefficient was used to
evaluate the linear relationship between endocan and both MDA and NO.
Additionally, a multiple regression analysis was performed to determine whether
MDA and NO levels predicted serum endocan concentrations. A p-value
The study flowchart is presented in Fig. 1. Of the 112 women initially evaluated, 95 (50 controls and 45 with missed abortion) agreed to participate. Eleven women in the control group were later excluded for not meeting the inclusion criteria, and one woman in the missed abortion group was excluded due to progesterone use. Ultimately, 44 women with missed abortion and 39 healthy controls were included in the analysis.
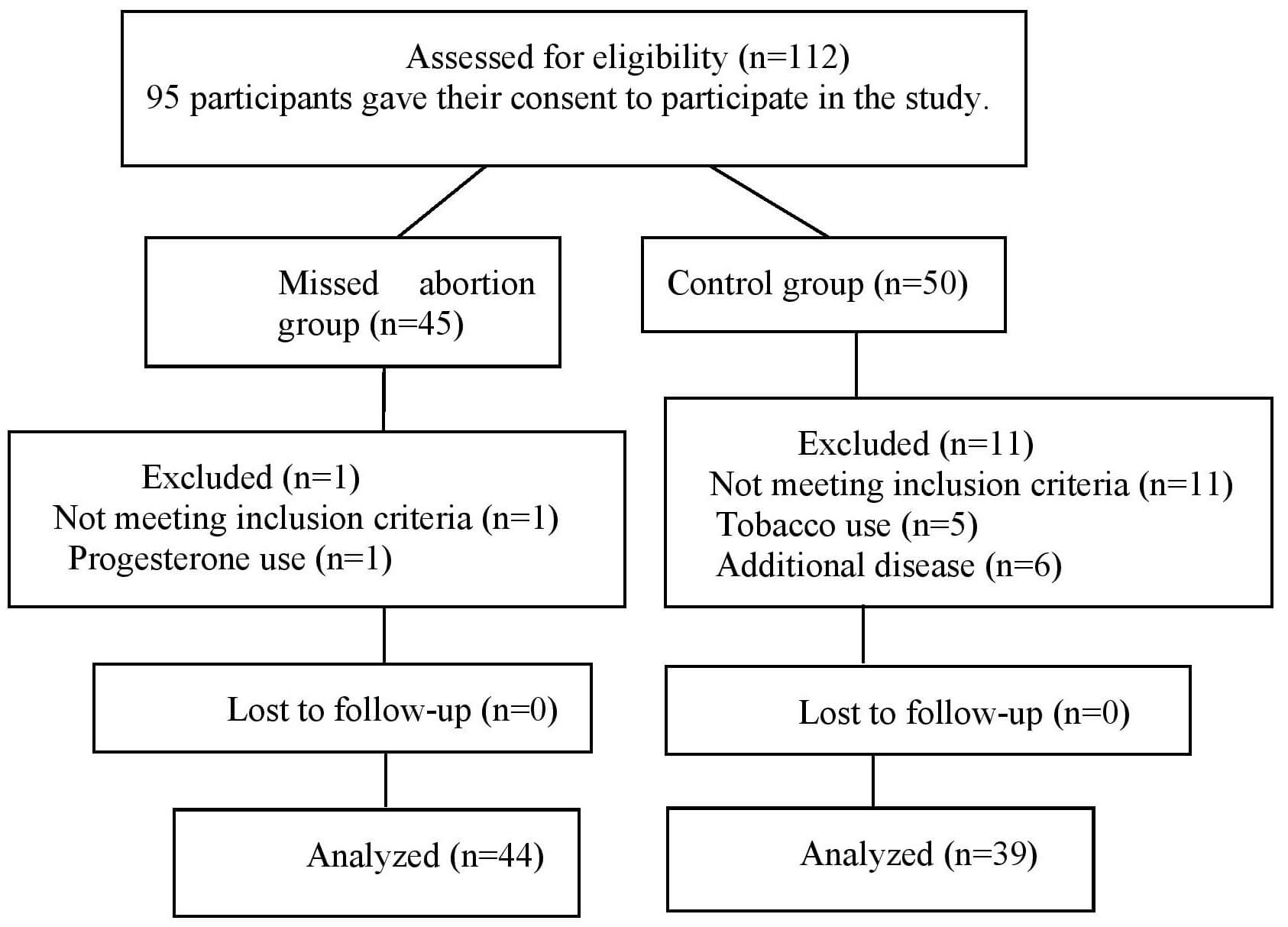 Fig. 1.
Fig. 1.
Study flowchart. n, number of samples.
No statistically significant differences were found between groups regarding
demographic characteristics (Table 1). Serum concentrations of endocan
(p = 0.029), NO (p = 0.011), and MDA (p = 0.021) were
significantly higher in women with missed abortion compared to controls. Positive
correlations were noted between endocan and MDA (r = 0.685, p
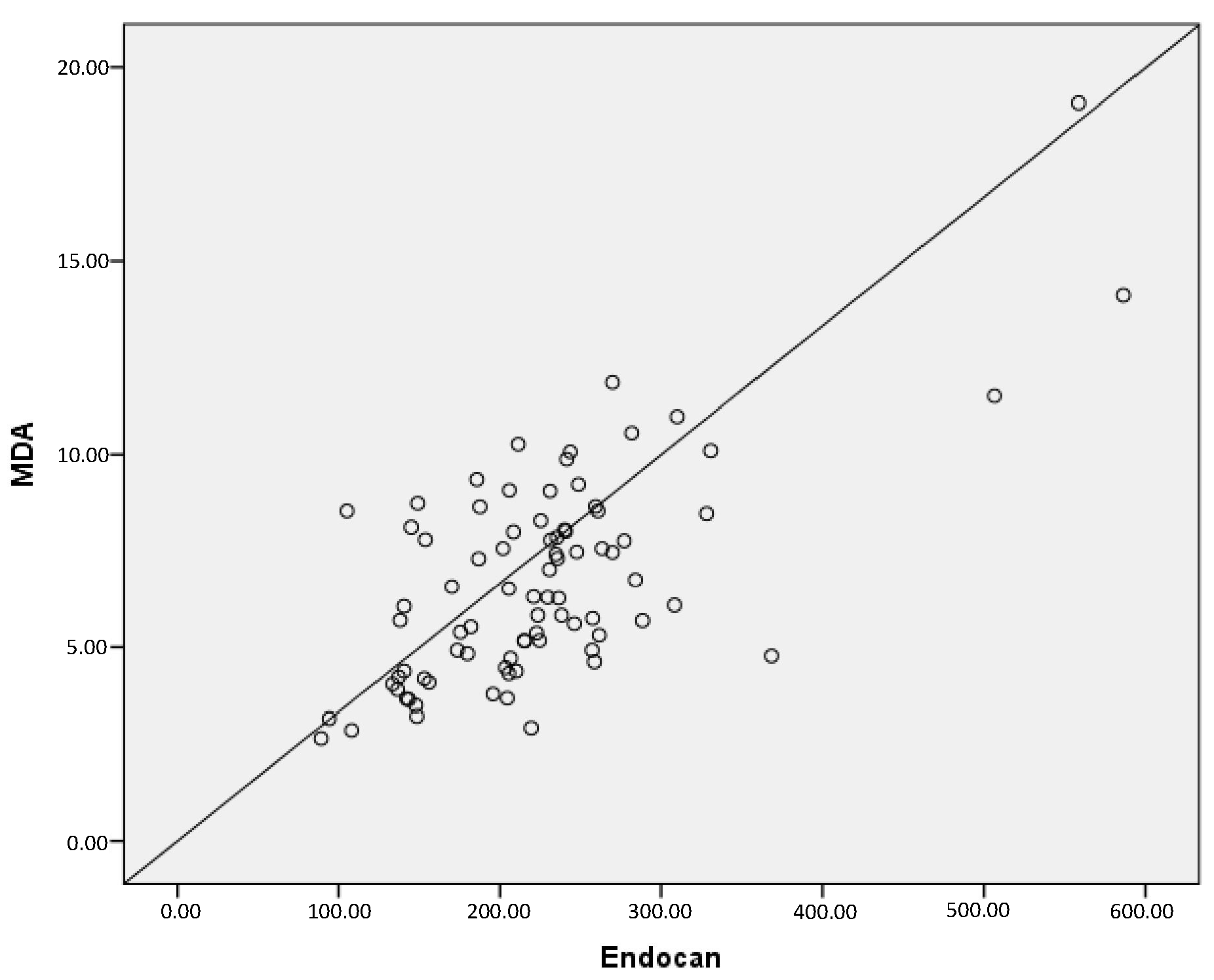 Fig. 2.
Fig. 2.
A positive correlation between serum endocan and MDA levels (r =
0.685, p
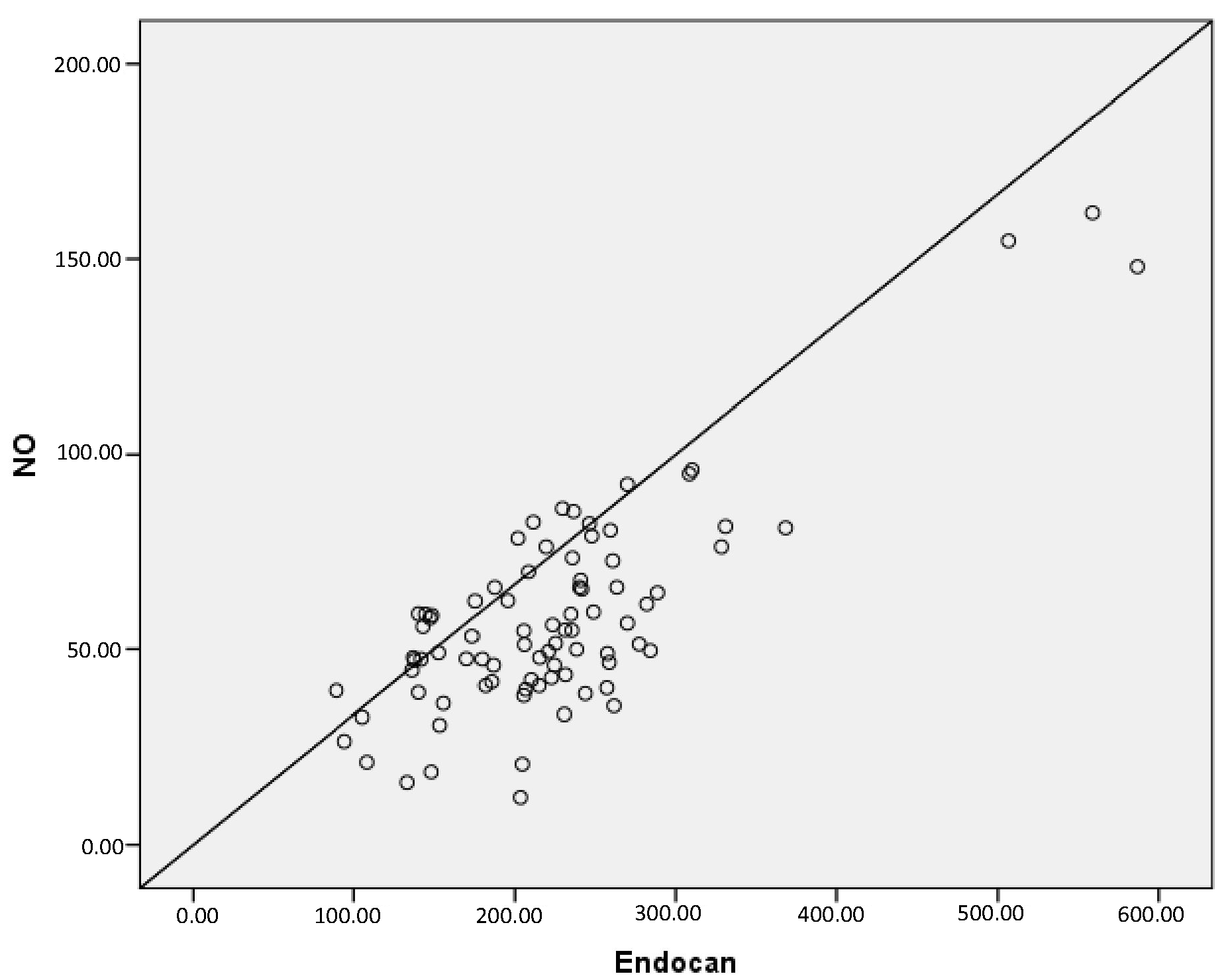 Fig. 3.
Fig. 3.
A positive correlation between serum endocan and NO levels (r =
0.795, p
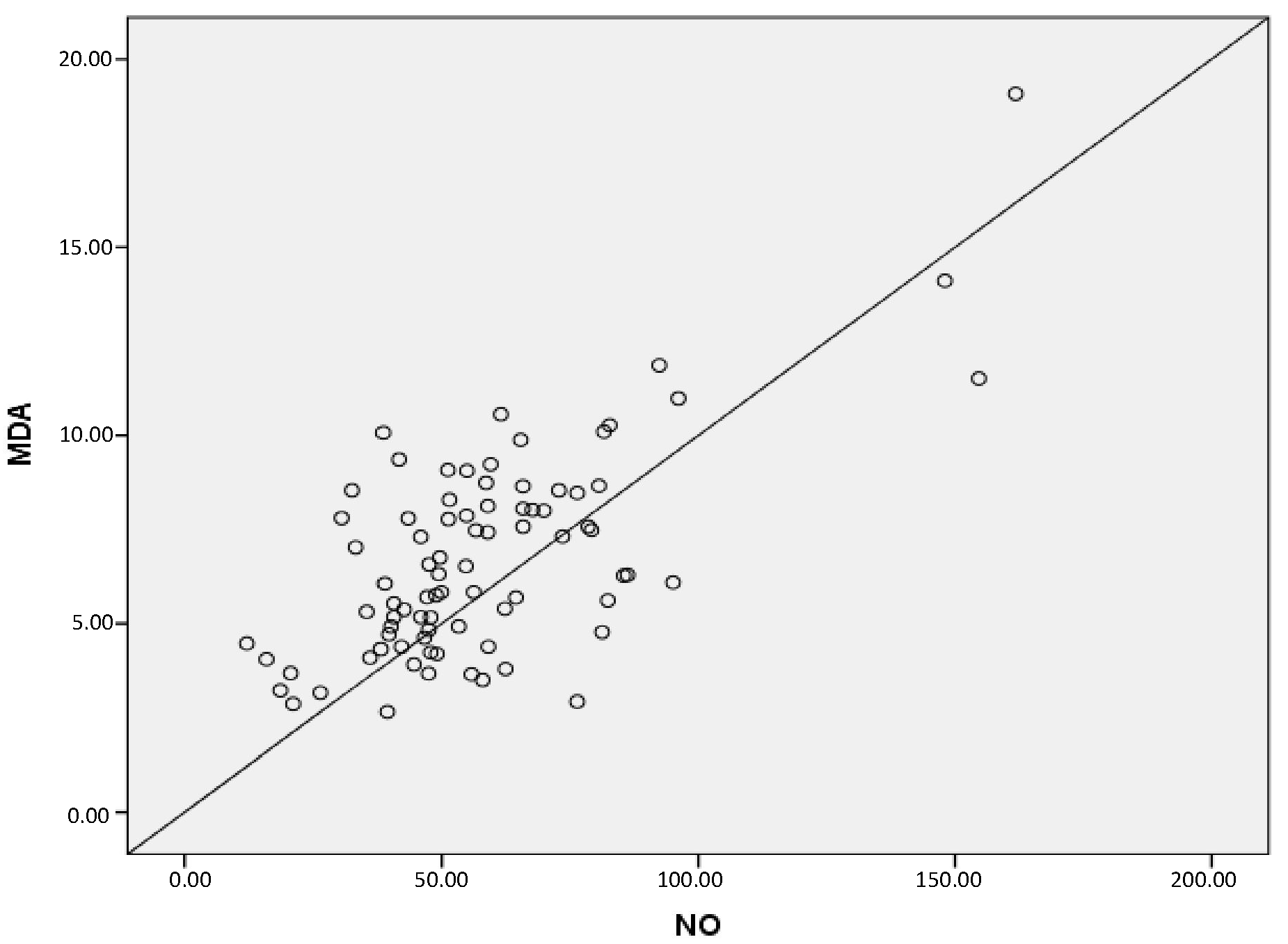 Fig. 4.
Fig. 4.
A positive correlation between serum NO and MDA levels (r =
0.685, p
| Missed abortion group (n = 44) | Control group (n = 39) | p value | |
| Age (years) | 31.80 |
30.69 |
0.390 |
| Gestational week | 10.61 |
11.38 |
0.344 |
| BMI (kg/m2) | 25.39 |
25.26 |
0.862 |
| Hemoglobin (g/dL) | 12.81 |
12.82 |
0.966 |
| Protein S (mmol/L) | 99.94 |
99.57 |
0.875 |
| Protein C (mmol/L) | 96.99 |
100.56 |
0.215 |
| vit D (ng/mL) | 27.16 |
25.55 |
0.196 |
| Vitamin B12 (pg/mL) | 308.64 |
329.64 |
0.366 |
| FT3 (pg/mL) | 3.27 |
3.26 |
0.860 |
| FT4 (pg/mL) | 1.20 |
1.05 |
0.749 |
| TSH (mU/L) | 2.04 |
2.04 |
0.547 |
| Gravidity (n) | 3.77 |
3.26 |
0.927 |
| Parity (n) | 1.93 |
2.26 |
0.117 |
| Abortion (n) | 1.61 |
- | - |
| MDA (µmol/L) | 7.39 |
6.01 |
0.021* |
| Endocan (ng/L) | 243.42 |
202.94 |
0.029* |
| NO (µmol/L) | 64.88 |
50.22 |
0.011* |
| Fibrinogen (mg/dL) | 334.18 |
348.67 |
0.303 |
| D-Dimer (ng/mL FE) | 424.18 |
391.08 |
0.098 |
| INR | 0.98 |
1.00 |
0.607 |
Values were expressed as mean
| Slope | Standard error | rpartial | t | R2 | p value | ||
| Endocan (constant) | 54.331 | ||||||
| NO levelsa | 1.977 | 0.285 | 0.613 | 6.941 | 0.61 | 0.669 | |
| MDA levelsa | 8.215 | 2.735 | 0.265 | 3.003 | 0.26 | 0.669 | 0.004* |
*p
aThere is a significant linear correlation between serum Endocan with MDA
and NO levels F(2,80) = 80.88, R2 = 0.669, p
In the present study, we observed that women diagnosed with missed abortion had significantly elevated serum concentrations of endocan, NO, and MDA compared with healthy pregnant controls. Numerous angiogenic factors have previously been examined as potential serum biomarkers capable of identifying pregnancies at high risk for early failure [3]. Based on this perspective, our aim was to explore the association between circulating endocan levels and oxidative stress markers in missed abortion cases.
Earlier reports indicate that systemic and placental oxidative stress—leading to endothelial injury, disturbed placental vascular development, and immune dysregulation—plays an important role in the mechanisms underlying both spontaneous and recurrent pregnancy loss [9, 12, 13]. There remains limited clarity regarding uterine perfusion dynamics during the implantation of embryonic trophoblasts. As uterine vascular proliferation progresses, the embryo transitions into a progressively hyperoxic environment. During this period of vascular remodeling, cytotrophoblasts differentiate into extravillous trophoblast cells, enabling infiltration into the spiral arteries and facilitating the development of vessels essential for sustaining pregnancy [14, 15]. This shift from relative hypoxia to normoxia creates an ischemia-reperfusion milieu in the developing embryo.
Oxidative cellular damage is primarily mediated by reactive oxygen species (ROS), and excessive ROS accumulation promotes apoptosis and premature cellular aging [16, 17]. To counter ROS-mediated injury, endogenous antioxidant mechanisms are activated within affected tissues. A study has demonstrated that alterations in oxidant and antioxidant levels are strongly linked to various conditions, including spontaneous miscarriage [18]. It has also been documented that the embryo experiences low oxygen tension in early gestation, with partial oxygen pressure measured at approximately 20 mmHg between 7–10 weeks of gestation—a period corresponding to early embryonic developmental stages when growth arrest is often observed in missed abortion cases [19]. Earlier research has shown that although pregnancy is accompanied by increased placental oxidative stress and ROS levels, antioxidants such as superoxide dismutase rise concurrently. As long as the balance between oxidants and antioxidants is maintained, normal pregnancy progression continues [20].
The literature presents conflicting evidence regarding NO concentrations in pregnancy loss. Some researchers have reported elevated NO levels in women with habitual or spontaneous abortion [21, 22, 23], whereas others have reported the opposite [24]. Paradisi et al. [24] described decreased NO levels in missed abortion patients and increased levels in healthy pregnancies. They suggested that reduced NO could induce vasoconstriction in uterine vessels, subsequently triggering decidual platelet aggregation. In contrast to these findings, our results demonstrated significantly higher NO concentrations in those experiencing missed abortion compared with healthy pregnant women. Considering that NO exerts anti-inflammatory, cytoprotective, and antimicrobial effects [7, 9, 25], the increased NO observed in our participants might represent a physiological response to inflammation triggered by a nonviable embryo or potential microbial exposure. Nevertheless, NO’s short biological half-life (2–30 seconds) must be considered.
In a separate study, trophoblast specimens obtained from women with missed abortion exhibited increased ROS levels and reduced superoxide dismutase activity during early pregnancy compared with controls. Such disruptions in redox balance are believed to impair trophoblast proliferation and may contribute to embryonic developmental arrest and missed abortion [26].
Additionally, a study evaluating oxidative stress in pregnancy has identified elevated oxidative markers in both the plasma and placental tissues of women with habitual abortion [27]. In our study, serum MDA levels—which reflect lipid peroxidation—were significantly higher in participants with missed abortion than in the control group. Adequate uteroplacental perfusion is fundamental to the continuation of a normal pregnancy, and impairment of this circulation is known to contribute to pregnancy loss [28].
Endocan, a molecule expressed at low levels in resting endothelial cells, increases during inflammatory activity and angiogenesis and is therefore considered a marker of endothelial activation. It has been proposed that because endocan reflects vascular integrity, this biomarker may be useful in identifying endothelial injury and inflammatory vascular processes [29, 30]. Elevated endocan levels have previously been reported in pre-eclampsia [31], a condition in which early pathological events include impaired trophoblast invasion into maternal spiral arteries, resulting in placental hypoxia and the release of anti-angiogenic and inflammatory mediators. Because endocan is involved in angiogenesis, inflammation, endothelial dysfunction, and cell adhesion, it is plausible that similar biological pathways contribute to the increased endocan levels observed in women with missed abortion in our study.
Transvaginal ultrasonography is a widely accepted diagnostic tool that greatly facilitates the early identification of pregnancy failure. However, in some circumstances, ultrasound findings alone are inconclusive, requiring the use of biochemical markers such as human chorionic gonadotropin or progesterone. Although these biomarkers can confirm pregnancy failure in symptomatic women, they are insufficient for identifying individuals at risk before the onset of symptoms. Currently, widely validated biomarkers capable of predicting miscarriage prior to clinical presentation are lacking.
To our knowledge, this is the first study examining serum endocan levels in missed abortion patients. The main limitation of our study is the inability to determine the exact timing of pregnancy loss, which is inherently difficult to ascertain clinically. Variability in the timing of embryonic demise may have influenced circulating endocan concentrations, suggesting that serum levels may fluctuate with the interval between fetal demise and diagnosis. Therefore, larger and more detailed studies are required to clarify these observations. On the other hand, the current study is a case-control study, and serum samples were collected during pregnancy. If serum samples had been collected after the pregnancy, the results might have been different. Studies could be planned to measure endocan levels in serum samples collected after pregnancy termination in patients with a history of missed abortion.
This study evaluated serum endocan concentrations as a potential marker of maternal endothelial dysfunction in missed abortion. We found significantly higher serum endocan, NO, and MDA levels in the missed abortion group compared with healthy pregnant women, supporting the involvement of oxidative stress and endothelial injury in the condition’s pathophysiology. As the first preliminary investigation on this topic, our findings highlight the need for future research with larger, diverse cohorts and combined biomarker approaches.
The study has been registered on https://zenodo.org/ (registration number: zenodo. 17910736; registration link: https://zenodo.org/records/17910736). Datasets are available from the registration link.
NY and SOS conceptualized and designed the study. NY recruited the participants and collected the clinical data. SOS performed the laboratory analyses and experiments. NY conducted the statistical analysis. Both authors interpreted the data, drafted and critically revised the manuscript for important intellectual content, and approved the final version of the manuscript. Both authors participated sufficiently in the work, and agree to be accountable for all aspects of the study.
This case-control study received approval from the Ethics Committee of Atatürk University, Faculty of Medicine (approval number: B.30.2.ATA.0.01.00/414), and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to participation after a detailed explanation of the study procedures.
We express our gratitude to Prof. Dr. Ayşe Nur Aksoy for her valuable support during manuscript revision. We also thank all peer reviewers for their constructive comments and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.