


 , Kaiming Li 1, Xiangao Lei 1, Bo Zhang 2, Fumin Zhao 1
, Kaiming Li 1, Xiangao Lei 1, Bo Zhang 2, Fumin Zhao 11 Department of Radiology, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Department of Ultrasound, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
Abstract
Fetal growth restriction (FGR) and placental insufficiency (PI) are major contributors to adverse perinatal outcomes, and early identification remains clinically challenging. This study aimed to evaluate the utility of artificial intelligence (AI)-based fetal magnetic resonance imaging (MRI) for early screening of FGR and PI.
A retrospective analysis was conducted on 120 pregnant women with a gestational age of 24–36 weeks who underwent fetal MRI examinations at the Second Hospital of West China, Sichuan University, from September 2024 to May 2025. Participants were divided into an FGR group, defined by an estimated fetal weight (EFW) below the 10th percentile for gestational age based on the Hadlock growth chart (n = 60), and a non-FGR group, defined by an EFW at or above the 10th percentile for gestational age (n = 60). MRI examinations were performed using a 3.0-T MRI Premier scanner with a 32-channel Head GE AIR™ Coil body coil, acquiring T2-weighted single-shot fast spin-echo (SSFSE) sequences of the fetal abdomen and placenta. Accelerated protocol images were reconstructed using the AIR™ Recon Deep Learning (DL) algorithm. FGR assessment relied on EFW, calculated from U-Net-segmented fetal abdominal volume combined with ultrasound-measured fetal femur length (FL) using the Hadlock formula, and compared with birth weight. EFW below the 10th percentile for gestational age served as the criterion for FGR. Segmentation performance was evaluated using the Dice similarity coefficient (target >0.85), diagnostic accuracy via the area under the receiver operating characteristic (ROC) curve (AUROC), and EFW error via mean absolute error (MAE, target <150 g). Ultrasound FL measurements were performed using a GE Voluson E10 system by certified sonographers, following the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) guidelines, within 3 days of MRI to ensure consistency.
AIR™ Recon DL-reconstructed images achieved a signal-to-noise ratio (SNR) of 59.5 ± 7.1 and a contrast-to-noise ratio (CNR) of 26.9 ± 4.8, significantly higher than non-reconstructed images (p < 0.05). The Dice coefficient for placental and fetal structure segmentation was 0.892 ± 0.021, the EFW MAE was 148.2 g, and FGR diagnostic accuracy was 91.7% (AUROC = 0.938), outperforming manual assessment (84.5%, AUROC = 0.864; p = 0.032). In the FGR with PI subgroup, diagnostic accuracy reached 93.4%, with an MAE of 135.6 g (p = 0.016).
Fetal MRI combined with the AIR™ Recon DL algorithm shows significant clinical value in assessing FGR and PI. This system enhances image quality, accelerates scanning, and reduces artifacts, thus improving the accuracy of FGR and PI diagnosis in early screening. This technique also offers reliable support for early screening and the development of individualized treatment plans in the context of high-risk pregnancy.
Keywords
- deep learning
- fetal growth retardation
- placental insufficiency
- magnetic resonance imaging
- image enhancement
- artificial intelligence
Fetal growth restriction (FGR) and placental insufficiency (PI), two common complications during gestation, are closely linked to fetal health and prognostic outcomes [1, 2]. FGR refers to a fetal weight below the 10th percentile for gestational age, whereas FGR denotes growth restriction triggered by PI or other pathological factors [3]. The occurrence of FGR is often correlated with preterm delivery, low birth weight (LBW), neonatal asphyxia, neurodevelopmental disorders, and other adverse outcomes, standing as a high-risk factor during pregnancy [4]. PI, a leading pathogenic factor for FGR, severely disrupts normal fetal growth and development by impairing oxygen delivery and nutrient exchange.
Accurate early diagnosis of FGR and PI is crucial for reducing fetal complications and enhancing pregnancy outcomes. Early identification and intervention allow clinicians to develop individualized treatment regimens, hence effectively preventing or mitigating adverse pregnancy outcomes. However, conventional assessment methods, like ultrasound, computed tomography (CT), and routine magnetic resonance imaging (MRI), have certain limitations in specific contexts [5, 6]. Ultrasound is widely used for FGR and PI screening; however, it has limited accuracy for assessing placental function and early symptoms of FGR in certain situations due to operator dependence, equipment performance, fetal position, amniotic fluid volume (AFV), and other technical factors [7]. CT is accompanied by ionizing radiation risks, making it generally unsuitable for pregnant women and fetuses [8]. Moreover, while conventional MRI provides excellent soft tissue contrast, it remains susceptible to fetal motion artifacts and requires prolonged acquisition times, limiting its utility for detailed visualization of the placenta and fetal structures [9].
Traditional imaging methods have long served as the primary approaches for the assessment of FGR and PI, among which ultrasound is the most prevalent. Ultrasound evaluates fetal health by estimating fetal weight and measuring placental blood flow. Nevertheless, image quality of ultrasound images usually fluctuates with operator experience and equipment performance, which limits the accuracy of FGR detection and placental function assessment. For example, fetal weight estimation using ultrasound depends on fetal volume and image clarity, both of which may be influenced by changes in AFV, fetal position, and other factors, hence affecting the accuracy of measurements [10].
As a radiation-free imaging modality, MRI demonstrates distinct advantages for the FGR and PI assessment due to its high-resolution soft tissue images. This technique provides clear visualization of placental and fetal anatomical structures, playing an irreplaceable role in the imaging of vital organs like the brain and heart for fetuses, particularly in complex cases. However, this traditional method also has clear limitations. Conventional MRI, however, remains affected by equipment performance, fetal motion, and prolonged acquisition times, which collectively limit image quality and diagnostic reliability. Therefore, strategies that address these limitations and enhance the clinical value of MRI in evaluating FGR and PI represent important research goals [11].
Over recent years, deep learning (DL) techniques, especially convolutional neural network (CNN), have achieved substantial progress in medical imaging field applications [12, 13]. DL can emulate neural processing in the human brain and efficiently extract image features for further classification, testing, and reconstruction, which supports image quality enhancement, automated diagnosis, and disease prediction [14, 15]. In the field of MRI, DL is mainly adopted for image reconstruction and denoising to improve image quality, shorten scan time, and lessen artifacts [16]. Specifically, this technology enables effective denoising of images with low signal-to-noise ratio (SNR) and enhances image resolution by learning features from large-scale imaging datasets, which improves diagnostic accuracy [17, 18]. In addition to enhancing image details, DL can also improve image contrast, performing particular effectiveness in fetal and placental image reconstruction. Furthermore, DL can automatically identify lesions or abnormalities, assisting clinicians in more accurately assessing fetal and placental health.
Previous studies have also explored DL-based fetal segmentation and estimated fetal weight (EFW) prediction. Specktor-Fadida et al. [14] developed a DL-based whole-body fetal MRI segmentation framework for MRI-based fetal weight estimation, achieving high segmentation performance (Dice = 0.973) and high accuracy with a mean difference between MRI-estimated fetal weight (EFW) and birth weight of –0.39%. Knoll et al. [19] optimized a 3D U-Net model for fetal brain segmentation with high reproducibility, while Sobhaninia et al. [20] proposed a multi-task DL approach for fetal ultrasound biometry. However, most of these studies have focused on single-modality segmentation (MRI or ultrasound), without integrating DL-based image reconstruction or placental function analysis. Therefore, clinically validated frameworks combining DL-enhanced MRI reconstruction with fetal body segmentation and EFW prediction remain limited.
Since the introduction of the AIR™ Recon DL algorithm by General Electric (GE), DL-based reconstruction methods have greatly improved MRI image quality [21]. By optimizing the image reconstruction process, AIR™ Recon DL can effectively denoise images and enhance fine details [22], demonstrating substantial advantages especially in fetal and placental imaging. Studies have shown that AIR™ Recon DL can accelerate scanning, reduce the scanning duration of conventional MRI, and boost the quality of images with low SNR, thereby providing clearer visualization of fetal and placental structure details [16, 22]. Thus, fetal MRI using this algorithm on 3.0-T SIGNA™ Premier equipment can provide higher quality images and more precise information for the early diagnosis of FGR and PI.
The primary aim of this study is to evaluate the diagnostic performance and image quality improvement achieved by the built-in AIR™ Recon DL reconstruction algorithm in fetal MRI using the GE 3.0-T SIGNA™ Premier system. Specifically, this study focuses on validating the algorithm’s impact on image quality, artifact reduction, and diagnostic efficiency for FGR and PI.
This study was designed to evaluate the utility of artificial intelligence
(AI)-based fetal MRI for the early screening of FGR and PI (Fig. 1).
Specifically, the study aimed to validate the diagnostic performance of the
built-in AIR™ Recon DL reconstruction algorithm, rather than to
develop a new CNN model. The study population consisted of pregnant women
undergoing fetal MRI examinations at the Obstetrics Department of West China Second University Hospital from September 2024 to May 2025. All participants carried singleton pregnancies.
Based on the diagnostic criterion for FGR (EFW below the 10th percentile for
gestational age), participants were assigned to an FGR group. This diagnostic
threshold follows the clinical guidelines issued by the International Society
of Ultrasound in Obstetrics and Gynecology (ISUOG), which define FGR as an EFW
below the 10th percentile for gestational age [10]. Although all eligible
participants were consecutively enrolled, to minimize the potential influence of
gestational age on group comparisons and to maintain statistical balance,
frequency matching by gestational age was applied during analysis. This approach
resulted in equal numbers of participants in the FGR and non-FGR groups (n = 60
each), totaling 120 participants. The sample size was determined via power
calculation (
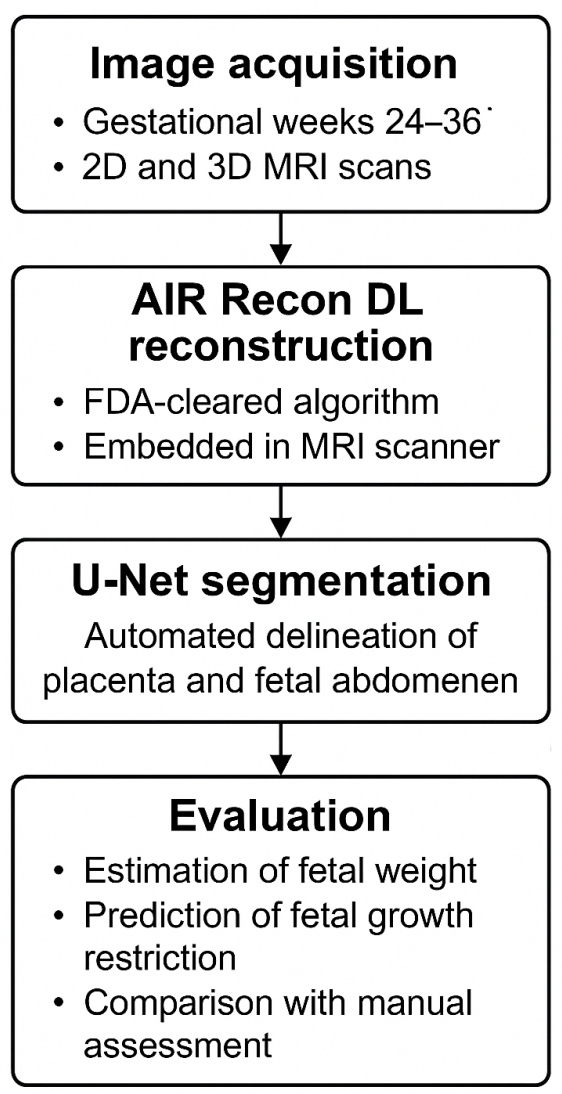 Fig. 1.
Fig. 1.
Flowchart of the study pipeline for AI-based fetal MRI using the AIR™ Recon DL algorithm. AI, artificial intelligence; MRI, magnetic resonance imaging; DL, deep learning.
This retrospective study was reviewed and approved by the Institutional Review Board (IRB) of the Medical Research Ethics Committee of the Second Hospital of West China, Sichuan University (Approval No. 313, 2024). The requirement for written informed consent was formally waived by the IRB due to the retrospective nature of the study. All procedures were conducted in accordance with the Declaration of Helsinki and applicable national regulations.
Inclusion criteria were: (1) gestational age of 24–36 weeks; (2) absence of severe complications (e.g., malignant tumors, or endocrine disorders); and (3) MRI examinations of acceptable diagnostic quality without severe motion artifacts. Only fetuses without major structural or chromosomal abnormalities were included to ensure dataset homogeneity. Exclusion criteria included: (1) severe fetal anomalies; (2) MRI contraindications (e.g., implanted metal devices); and (3) inability to tolerate scanning.
FGR diagnosis was defined as an EFW below the 10th percentile for gestational
age based on the Hadlock growth chart, which was also used to establish
percentile thresholds for postnatal birthweight confirmation [10]. Cases were
retrospectively reviewed, and final FGR classification was supported by
birthweight percentiles and available prenatal Doppler findings, including an
umbilical artery pulsatility index
During the study period, 156 pregnant women underwent fetal MRI examinations. Of these, 132 met the inclusion criteria, and 120 were ultimately analyzed after excluding cases with incomplete data or poor image quality.
All fetal MRI examinations were conducted using a 3.0-T MRI scanner (SIGNA™ Premier, GE Healthcare, Chicago, IL, USA) equipped with a 32-channel GE AIR™ Coil body coil for signal reception. The coil’s high sensitivity and uniform signal coverage optimized the SNR and contrast-to-noise ratio (CNR), while effectively minimizing fetal motion artifacts during imaging of the placenta and fetal abdomen. The standard fetal MRI protocol included axial T2-weighted fat-saturated (FS) single-shot fast spin-echo (SSFSE), axial T1-weighted gradient-echo, sagittal T2-weighted SSFSE, coronal T2-weighted SSFSE, and three-dimensional (3D) T2-weighted sequences to capture images of the placenta and fetal abdomen. Both two-dimensional (2D) and 3D acquisitions were performed to assess volumetric reconstruction and segmentation. FGR assessment relied on MRI-derived fetal abdominal volume combined with fetal femur length (FL) measured via ultrasound to calculate EFW. Ultrasound examinations were performed using a GE Voluson E10 ultrasound system (GE HealthCare, Zipf, Austria) by certified sonographers with at least 5 years of fetal ultrasound experience, following standardized biparietal diameter and FL measurement protocols, as per ISUOG guidelines [10]. MRI and ultrasound examinations were conducted within the same gestational week (24–36 weeks), with a maximum interval of 3 days to ensure data consistency. Doppler ultrasound was performed within three days of MRI acquisition to measure the umbilical artery pulsatility index, middle cerebral artery PI, and to calculate the CPR. All examinations were performed by certified obstetric sonographers following ISUOG standards for fetal Doppler assessment [10].
The standard MRI protocol had an average scanning time of 18 minutes and 45
seconds, while an accelerated protocol averaged 7 minutes and 30 seconds. Raw
accelerated MRI images were transferred to post-processing software (Orchestra
SDK, GE Healthcare) and reconstructed using the AIR™ Recon DL
algorithm, with reconstructed images labeled as DL sequences. The
AIR™ Recon DL pipeline incorporates a deep CNN with approximately
10,000 kernels and 4.4 million trainable parameters. Importantly, this CNN is an
FDA (Food and Drug Administration)-cleared, commercially embedded algorithm
within the GE scanner, rather than a newly developed research model. The CNN
processes raw complex-valued imaging data to generate high-quality output images
by: (1) reducing user-adjustable image noise, (2) minimizing truncation
artifacts, and (3) enhancing edge sharpness. Integration into the scanner’s
native inline reconstruction pipeline ensures access to raw, full-bit-depth data.
The CNN was trained using supervised learning with image pairs consisting of
near-perfect high-resolution images (minimal ringing, low noise) and conventional
images synthesized to include higher noise and truncation artifacts. In our
study, the use of AIR™ Recon DL under the same acquisition
protocol reduced the mean scan time by approximately 60% while maintaining
equivalent spatial resolution. The cohort-specific SNR increased by 92%
This denoising and edge-enhancement capability further improved the diagnostic quality of MRI images that were acceptable but not entirely free of motion artifacts. To assess consistency and reproducibility, two independent radiologists evaluated 30 randomly selected MRI studies twice, separated by a 2-week interval, and inter-observer and intra-observer agreement were calculated using intraclass correlation coefficients (ICCs). Ultrasound data were stored in Digital Imaging and Communications in Medicine (DICOM) format and, together with MRI images, transferred to the Picture Archiving and Communication System (PACS; IMPAX 6, Agfa-Gevaert NV) for further analysis.
MRI image datasets were exported from the PACS and preprocessed using ITK-SNAP
(version 3.8) for registration, denoising, and standardization. Segmentation of
the placenta and fetal abdomen was performed using a 2D U-Net model, trained on
an NVIDIA RTX 3090 GPU for 100 epochs with a cross-entropy loss function and a
learning rate of 0.001. The Adam optimizer (
The training dataset comprised images from 80 pregnant women (67%), with
validation and test sets each including images from 20 pregnant women (16.7%).
To ensure subject-level independence, all images from a single subject were
assigned to only one subset. Segmentation masks were annotated by two
radiologists (Kappa = 0.85). In addition, inter-rater reliability was further
assessed using Dice overlap (mean = 0.87
Fetal FL was measured via ultrasound using standardized ISUOG measurement
protocols [10], and the data were input as numerical values into the subsequent
EFW calculation model. FGR identification was based on EFW calculated from
MRI-segmented fetal abdominal volume and ultrasound-measured FL, using the
Hadlock formula, compared against birth weight, with EFW below the 10th
percentile serving as the criterion for FGR prediction. Segmentation performance
was evaluated using the Dice similarity coefficient (target
For the segmentation model, datasets were divided into training, validation, and test subsets (80, 20, and 20 subjects, respectively), as described in Section 2.3. For the subsequent regression model used for EFW prediction and FGR identification, data from 120 subjects were divided at the subject level into training (80%) and validation (20%) subsets, and five-fold cross-validation was applied to enhance model generalization.
Placental and fetal abdominal segmentation was performed using the 2D U-Net model, while the EFW prediction model integrated MRI-segmented abdominal volume and ultrasound-measured FL data using a regression framework based on the Hadlock formula. No additional CNN or classification networks were trained or fine-tuned in this study; all reconstructions were performed using the manufacturer-implemented AIR™ Recon DL algorithm. The regression model was trained to minimize prediction error between MRI-based EFW and actual birth weight. To prevent potential temporal bias, datasets were randomly partitioned according to acquisition date to ensure chronological independence between training and validation samples. Fold-wise performance metrics were averaged across five folds, and 95% confidence intervals (CIs) were calculated to assess model stability.
Evaluation metrics included the Dice similarity coefficient (target
The FGR identification function of the DL system was based on a comparison between the EFW, calculated by integrating MRI-segmented fetal abdominal volume and ultrasound-measured FL, with the actual birth weight. Using an EFW below the 10th percentile as the criterion for FGR prediction, the accuracy, sensitivity, specificity, and AUROC of the DL system were calculated.
The manual assessment was carried out by 2 senior radiologists separately. The physicians completed fetal weight assessment and placental function analysis as per routine imaging criteria, with the same diagnostic criteria for FGR. Comparisons were made between the assessment results and the diagnostic results from the DL system, and the accuracy, sensitivity, specificity, and AUROC of the manual and system results were calculated.
The reference placental volume used for error analysis was obtained from manual segmentation performed by two experienced radiologists using ITK-SNAP software (version 3.8, www.itksnap.org). Each segmentation was performed independently and subsequently reviewed jointly to reach consensus. The mean of the two measurements was considered the actual placental volume for comparison with the system-estimated volume.
All statistical analyses were performed using SPSS software (version 26.0, IBM, Armonk, NY, USA). Image quality metrics (SNR, CNR, and edge sharpness scores) were compared between AIR™ Recon DL-reconstructed and non-reconstructed images using paired t-tests. For intergroup comparisons of continuous variables (e.g., per-case Dice Dcoefficients), independent-samples t-tests or Mann–Whitney U tests were applied according to the Shapiro–Wilk normality test. The “Consistency of placental volume measurement” reported in Table 3 represents a reliability coefficient (ICC). Because this metric is a statistical coefficient rather than a continuous variable, it was summarized descriptively (0.85 vs. 0.93). The p-value reflects a comparison of these coefficients using Fisher’s z-transformation rather than a t-test.
For Table 4, per-case continuous outcomes, such as placental-volume estimation error, were analyzed using paired t-tests or nonparametric alternatives. Summary performance metrics, such as accuracy and AUROC, were not treated as continuous variables; AUROC values were compared using DeLong’s test.
Placental segmentation performance was assessed via the Dice similarity coefficient, and the diagnostic accuracy for FGR and PI was evaluated using ROC curve analysis with AUROC calculation (AUROC). For each key metric (AUROC, MAE, and Dice coefficient), 95% CIs were computed to assess statistical precision and robustness. Comparisons between the AUROC values of the DL system and manual assessment were performed using DeLong’s test. Multiple comparisons across subgroups were adjusted using the Benjamini–Hochberg false discovery rate (FDR) correction method to control type I error inflation. Correlations between MRI-derived placental parameters (e.g., placental volume, mean T2 value) and Doppler indices (umbilical artery PI, CPR) were assessed using Pearson or Spearman correlation coefficients, depending on data distribution.
EFW prediction error was evaluated using MAE, with a target MAE below 150 g. All
statistical tests were two-sided, with significance thresholds adjusted for
multiple comparisons (adjusted p
A total of 120 pregnant women who underwent fetal MRI were included in the study
and were grouped according to the presence of FGR: the FGR group (n = 60) and the
non-FGR group (n = 60). The two groups showed no significant differences in
baseline characteristics, including gestational age and maternal age (p
| Indicators | FGR group (n = 60) | Non-FGR group (n = 60) | 95% CI (FGR / Non-FGR) | p-value |
| Gestational age (weeks) | 31.2 |
31.6 |
(30.6–31.8) / (31.1–32.1) | 0.296 |
| Maternal age (years) | 29.8 |
30.2 |
(28.9–30.7) / (29.3–31.1) | 0.512 |
| EFW (g) | 1230.6 |
1685.9 |
(1176–1285) / (1624–1748) | |
| Placental volume (cm³) | 310.7 |
391.5 |
(299–322) / (379–404) | |
| Placental T2 value (ms) | 87.4 |
101.2 |
(85.1–89.7) / (98.8–103.6) | |
| Birth weight (g) | 2145.8 |
2923.3 |
(2058–2233) / (2844–3002) |
Note: FGR, fetal growth restriction; CI, confidence interval; EFW, estimated fetal weight; T2, transverse relaxation time; SD, standard deviation.
High-precision segmentation of the placenta and fetal brain structures was
achieved using the fetal MRI image analysis system based on DL. The Dice
coefficient for placental segmentation was 0.892
| Items | Values | 95% CI |
| Dice coefficient of placental segmentation | 0.892 |
0.888–0.896 |
| Intersection over union (IoU) of placental segmentation | 0.821 |
0.814–0.828 |
| EFW MAE (g) | 148.2 | 139.6–156.8 |
| EFW RMSE (g) | 192.6 | 180.2–205.0 |
| Predicted R2 | 0.86 | 0.82–0.90 |
| FGR identification accuracy | 91.70% | 88.5–94.9 |
| AUROC | 0.938 | 0.912–0.964 |
| Sensitivity/specificity | 88%/93% | (82–94) / (89–97) |
Note: Dice, Dice similarity coefficient; IoU, intersection over union; CI, confidence interval; EFW, estimated fetal weight; MAE, mean absolute error; RMSE, root mean square error; R2, coefficient of determination; AUROC, area under the receiver operating characteristic curve.
All MRI images were collected through the GE SIGNA™ Premier 3.0-T system, with the AIR™ Recon DL image reconstruction algorithm applied. This algorithm enhances image SNR and CNR based on raw k-space data and attenuates Gibbs artifacts. Comparison of 20 cases before and after applying AIR™ Recon DL found noticeable enhancement in image quality and subsequent segmentation performance (Table 3).
| Indicators | Without DL reconstruction (n = 20) | With AIR™ Recon DL (n = 20) | p-value | 95% CI (DL vs non-DL) |
| SNR | 46.2 |
59.5 |
(43.5–48.9) / (57.1–61.9) | |
| CNR | 19.7 |
26.9 |
(18.2–21.2) / (25.6–28.2) | |
| Placental border clarity score (1–5 points) | 3.2 |
3.9 |
0.003 | – |
| Consistency of placental volume measurement | 0.85 | 0.93 | 0.018 | – |
| Improvement in segmentation Dice coefficient | 0.871 |
0.908 |
0.018 |
Note: AIR™ Recon DL, Adaptive Image Reconstruction Deep Learning; DL, deep learning; SNR, signal-to-noise ratio; CNR, contrast-to-noise ratio; Dice, Dice similarity coefficient. Edge sharpness and placental border clarity were scored by two blinded radiologists using a validated 5-point scale (1 = poor, 5 = excellent). Placental border clarity score (1–5) was analyzed as a continuous variable due to its quasi-continuous distribution, consistent with common imaging-quality assessment practices. The comparison was performed on a paired subset of 20 cases randomly selected from the overall study cohort (the same subjects scanned before and after AIR™ Recon DL reconstruction).
The MRI system based on deep learning demonstrated significant advantages were observed in the FGR identification task. The system achieved an accuracy of 91.7%, substantially higher than the 84.5% of manual assessment. Additionally, the system showed a superior performance in predicting placental volume and identifying placental perfusion abnormalities compared with manual assessment. Combining the two methods further increased the accuracy to 92.2%. See Table 4.
| Items | Manual (n = 120) | MRI system (n = 120) | Manual + system (n = 120) | p-value (system vs. manual) | 95% CI (Manual/System) |
| FGR identification accuracy (%) | 84.50% | 91.70% | 92.20% | 0.032 | (80.2–88.8) / (88.5–94.9) |
| AUROC | 0.864 | 0.938 | 0.944 | 0.041 | (0.822–0.906) / (0.912–0.964) |
| Placental volume estimation error (cm³) | 42.7 |
39.3 |
38.6 |
0.118 | (38.3–47.1) / (35.0–43.6) |
Note: MRI, magnetic resonance imaging.
We analyzed subgroups with different FGR and PI conditions. The system demonstrated superior performance in the FGR + PI group, showing the lowest EFW error (135.6 g) and an FGR detection accuracy of 93.4%. These results suggest that this system has greater application value in high-risk pregnant populations (Table 5).
| Subgroups | Predicted MAE (g) | R2 | FGR detection accuracy | 95% CI (MAE / Accuracy) | p-value (vs. non-PI group) |
| Non FGR + normal function | 152.4 | 0.84 | 89.20% | (140–165) / (85.0–93.4) | – |
| Non FGR + PI | 158.3 | 0.81 | 85.10% | (145–172) / (80.2–90.0) | 0.229 |
| FGR + normal function | 141.2 | 0.86 | 90.00% | (130–152) / (86.0–94.0) | 0.118 |
| FGR + PI | 135.6 | 0.88 | 93.40% | (125–146) / (89.8–97.0) | 0.016 |
Note: PI, placental insufficiency; MAE, mean absolute error.
This study aimed to evaluate the clinical value of the AIR™ Recon DL algorithm in the assessment of FGR and PI. Our results showed that the AIR™ Recon DL algorithm significantly improved fetal MRI image quality, as evidenced by heightened SNR and CNR. This finding is consistent with preceding study findings, suggesting that DL can effectively reduce motion artifacts and noise generated in traditional imaging methods and enhance image spatial resolution [23, 24, 25]. Previous studies have shown that deep learning-based reconstruction can effectively reduce image noise and improve image clarity, thereby mitigating motion-related artifacts and improving diagnostic image quality [21, 22]. Consistent with their results, our study further validates these advantages in the context of FGR and PI. Moreover, by integrating MRI-based volumetric analysis with ultrasound-derived biometric parameters, our work expands the application of AIR™ Recon DL from image optimization to comprehensive multimodal evaluation of fetal growth and placental function. With regards to placental and fetal structure visualization, the image clarity achieved by this algorithm was superior to that of traditional MRI reconstruction. The AIR™ Recon DL algorithm further enhanced image usability by applying DL to raw k-space data, enabling more accurate assessment of fetal growth and placental function.
Previous studies have investigated DL-based fetal segmentation and EFW prediction using MRI and ultrasound modalities. Specktor-Fadida et al. [14] developed a whole-body fetal MRI segmentation framework that achieved a Dice coefficient of approximately 0.87 and an EFW MAE within 160 g. Knoll et al. [19] optimized a 3D U-Net model for fetal brain segmentation, while Sobhaninia et al. [20] implemented a multi-task DL approach for fetal ultrasound biometry. However, these studies mainly focused on single-modality imaging and did not integrate DL-based MRI reconstruction or placental function analysis. In contrast, our study integrates DL-enhanced MRI with ultrasound-based biometric data and provides a validated clinical evaluation of FGR and PI. This multimodal framework therefore extends previous segmentation and EFW estimation approaches toward a and clinically applicable diagnostic workflow.
Here, the AIR™ Recon DL algorithm enabled efficient segmentation of the placenta, achieving a Dice coefficient of 0.892, markedly higher than that of traditional image reconstruction methods [18, 19]. Placental volume serves as a significant indicator of fetal health, showing substantial clinical significance particularly in examining PI [26]. By using the DL algorithm, placental volume can be measured more accurately, providing strong support for the early diagnosis of FGR and PI.
By integrating high-resolution fetal abdominal MRI with ultrasound-measured
fetal FL, this study overcame the limitation of not acquiring fetal femur MRI
data, significantly enhancing the clinical utility of EFW predictions. MRI,
leveraging its superior soft tissue resolution and the image optimization
capabilities of the AIR™ Recon DL algorithm (SNR 59.5
Moreover, the system demonstrated strong performance in predicting fetal weight. The MAE reached 148.2 in our study. Compared with conventional ultrasound-based fetal weight estimation, our approach showed improved predictive performance [27]. This observation confirms that DL-based MRI image reconstruction performs well in anatomical structure assessment and fetal growth assessment with high accuracy. This high-precision weight prediction method is crucial for early-stage FGR and PI detection and can offer strong and reliable evidence for clinical interventions.
This study unraveled that the AIR™ Recon DL algorithm excelled in identifying FGR, achieving an accuracy of 91.7% and an AUROC of 0.938. Compared with the manual method, the system combined with the DL model showed a better performance, with diagnostic accuracy particularly enhanced in high-risk pregnant populations. Currently, FGR diagnosis primarily depends on clinical experience and traditional imaging methods, but they are confronted with various challenges during early-stage diagnosis, such as quality restriction and fetal motion artifacts [28]. DL technology can automatically analyze fetal MRI images to overcome the shortcomings of these traditional methods and improve the early diagnostic rate for FGR.
Consistent with comparisons to manual assessment, the DL system’s superiority in FGR diagnosis may originate from its ability to automatically identify features in complex situations, especially through image denoising and edge contrast enhancement [12]. In future clinical applications, DL-assisted fetal MRI assessment can significantly improve the accuracy of early diagnosis. It can display huge potential when it comes to regions with limited resources or environments with low technological levels.
Although this study demonstrated the potential of AIR™ Recon DL in placental segmentation and the assessment of FGR and PI, its clinical implementation still faces several challenges. Despite the improvement in image quality, fetal motion artifacts remain a persistent limitation in fetal MRI, especially during active fetal movement. Furthermore, the evaluation of PI relies not only on imaging quality but also on comprehensive integration with other clinical parameters, such as hemodynamic indices and laboratory data. The retrospective, single-center design of this study and the relatively small sample size may also limit the generalizability of the findings. In addition, the results may be influenced by scanner- and vendor-specific characteristics, as all MRI data were acquired on a single 3.0-T GE SIGNA™ Premier system using the AIR™ Recon DL algorithm. Therefore, caution should be exercised when extrapolating the results to other MRI platforms or reconstruction algorithms. Although ultrasound FL measurements followed ISUOG guidelines and were performed by experienced sonographers, operator- and equipment-related variability could not be completely eliminated, potentially affecting the accuracy of EFW. Future studies involving multiple vendors, standardized multicenter ultrasound protocols, and larger patient cohorts are warranted to further validate the robustness and general applicability of our findings.
With ongoing advancements in technology and imaging hardware, DL–based fetal MRI assessment is expected to further reduce manual intervention, improve efficiency, and enhance diagnostic precision. Such AI-assisted systems hold promise as valuable tools for the early detection and individualized management of high-risk pregnancies.
In conclusion, our study shows that fetal MRI combined with AIR™ Recon DL has significant clinical value for the assessment of FGR and PI. This technique enhances image quality and reduces artifacts, with high accuracy in fetal weight prediction, placental segmentation, and FGR detection. Despite remaining challenges, this approach offers strong potential for further refinement and wider clinical application and is likely to become an important tool for the management of high-risk pregnancies.
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
All authors contributed to the study conception and design. YZ and FZ were responsible for material preparation. XL and KL were responsible for data collection. BZ was responsible for data analysis. The first draft of the manuscript was written by YZ, and all authors critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This retrospective study was approved by the Institutional Review Board of the Medical Research Ethics Committee of the Second Hospital of West China, Sichuan University (Approval No. 313, 2024). The requirement for written informed consent was waived due to the retrospective nature of the study. The study was conducted in accordance with the guidelines of the Declaration of Helsinki.
The authors would like to thank the radiology and obstetrics teams of the Second Hospital of West China, Sichuan University for their technical assistance and valuable support during data acquisition and analysis.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work, we used ChatGPT (OpenAI, San Francisco, CA, USA) to assist in checking English grammar and spelling. After using this tool, we carefully reviewed and edited the content to ensure accuracy and appropriateness, and take full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.