



 , Menghan Liu 1,2, Ke Yang 1,2, Xiao Duan 3, Haiyan Kuang 1,2, Yingchun Luo 1,2, Yu Long 1,2,*
, Menghan Liu 1,2, Ke Yang 1,2, Xiao Duan 3, Haiyan Kuang 1,2, Yingchun Luo 1,2, Yu Long 1,2,*
1 NHC Key Laboratory of Birth Defect for Research and Prevention, Hunan Provincial Maternal and Child Health Care Hospital, 410008 Changsha, Hunan, China
2 Ultrasound Medical Center, Hunan Provincial Maternal and Child Health Care Hospital, 410008 Changsha, Hunan, China
3 Department of Radiology, 921st Hospital of the Joint Logistic Support Force of the Chinese People’s Liberation Army, 410003 Changsha, Hunan, China
Abstract
This study aimed to analyze the clinical and ultrasonographic features of 6 pathologically confirmed cases of uterine inflammatory myofibroblastic tumors (UIMT) and to enhance clinicians’ ability to achieve timely diagnosis and treatment.
This retrospective case series included 6 patients with pathologically confirmed UIMT who were admitted to our hospital between January 2019 and January 2025. Clinical, ultrasonographic, and pathological data were collected and analyzed retrospectively.
All 6 tumors were solid and originated from the myometrium. 3 were confined to the myometrium, 2 extended toward the submucosa, and 1 toward the subserosa. 5 lesions were hypoechoic and 1 was hyperechoic, all showing heterogeneous internal echoes and a characteristic “blurred halo sign”. The median maximum diameter was 6.9 cm. Color Doppler flow imaging (CDFI) showed an Adler grade ≥2, demonstrating a “colorful mosaic sign”. During follow-up, 2 lesions increased in size by 1 cm and 2 cm, respectively, within 2–4 months. No extrauterine metastasis was observed. All cases were positive for anaplastic lymphoma kinase (ALK), as confirmed by fluorescence in situ hybridization (FISH). All patients underwent surgical treatment, including 1 total hysterectomy and 5 local resections. No recurrence or metastasis was observed during 21–57 months of follow-up.
UIMT exhibits characteristic sonographic features, including solid masses with heterogeneous internal echoes (“blurred halo sign”) and abundant blood flow signals (“colorful mosaic sign”). Recognizing these distinctive imaging patterns is critical for improving diagnostic accuracy and guiding appropriate clinical management.
Keywords
- uterine inflammatory myofibroblastic tumor
- ultrasonography
- blurred halo sign
- colorful mosaic sign
- diagnosis
Inflammatory myofibroblastic tumor (IMT) is a rare neoplasm characterized by the proliferation of myofibroblastic spindle cells accompanied by marked inflammatory infiltration [1]. It mainly occurs in the lungs and soft tissues of the abdomen, while uterine involvement is uncommon. This etiology remains uncertain but may be associated with chronic infection, autoimmune disorders, or trauma [2]. According to the latest World Health Organization (WHO) classification, approximately 5% of IMT cases may recur or metastasize [3]. Because of its morphological similarity to other spindle cell tumors of the female reproductive tract, uterine IMT (UIMT) is often misdiagnosed as a smooth muscle tumor. Studies on the ultrasonographic manifestations of UIMT are limited and mostly confined to isolated case reports. Therefore, this study systematically analyzes UIMT’s clinical and ultrasonographic characteristics to enhance clinicians’ understanding and facilitate timely diagnosis and treatment.
This was a retrospective case analysis including 6 UIMT patients confirmed by
surgery and pathology at our hospital between January 2019 and January 2025.
Inclusion criteria: Postoperative pathological findings consistent with the
diagnostic criteria for UIMT in the [2020 WHO Classification of Soft
Tissue and Bone Tumours] [1], characterized by spindle cell proliferation with
inflammatory cell infiltration and positive anaplastic lymphoma kinase
(ALK) expression; complete preoperative transvaginal three-dimensional
(3D) ultrasonography data and clinical medical records. Exclusion criteria:
Concurrent gynecological malignancies or other soft tissue tumors; incomplete
ultrasonographic data; loss to follow-up. Ultrasonographic examinations were
performed using GE E8, GE E6 (General Electric Company, Waukesha, WI, USA), and
Philips IU22 systems (Philips Healthcare, Best, North Brabant, the Netherlands)
equipped with transvaginal 3D probes (4–9 MHz). All scans were conducted by
obstetric and gynecologic ultrasound physicians with more than 10 years of
experience. Clinical data, including demographic characteristics and
diagnosis/treatment information, were retrieved from the hospital’s electronic
medical records system. Ultrasonographic data were extracted from the imaging
reporting system, documenting lesion mass characteristics such as location, size,
shape, margin, internal echo pattern, and blood flow signals. Blood flow was
assessed using the Adler semi-quantitative grading system [4]: Grade 0 (no
detectable flow); Grade 1 (scant flow, 1–2 punctate/short rod-like signals);
Grade 2 (moderate flow, 3–4 punctate/short rod-like signals or a vessel diameter
Data analysis was performed using SPSS version 26.0 (IBM Corporation, Armonk,
NY, USA). Continuous variables were described as mean
A total of 6 patients with pathologically confirmed UIMT were included, aged
24–49 years (mean 37.8
| Number | Age (years) | Clinical Symptoms | Obstetric History (G/P/A) | CA125 (U/mL) | WBC (×109/L) | Hb (g/L) | Surgical Method | Recurrence/Metastasis | Follow-up Time (months) |
| 1 | 36 | Increased menstrual flow, prolonged menstrual period | 4/2/2 | 15.1 | 9.8 | 91 | Hysteroscopic electroresection of intrauterine neoplasms | no | 57 |
| 2 | 38 | Uterine mass, dysmenorrhea (detected by physical examination) | 1/0/0 | 38.4 | 11.4 | 103 | Laparoscopic resection of uterine lesions | no | 43 |
| 3 | 49 | Increased menstrual flow, prolonged menstrual period | 1/1/1 | 162 | 12.7 | 89 | Laparoscopic total hysterectomy | no | 47 |
| 4 | 39 | Increased menstrual flow, prolonged menstrual period, dysmenorrhea | 3/1/2 | 31.9 | 10.7 | 83 | Laparoscopic resection of uterine lesions | no | 26 |
| 5 | 41 | Prolonged menstrual period | 3/1/2 | 32.7 | 6.4 | 100 | Laparoscopic resection of uterine lesions | no | 33 |
| 6 | 24 | Uterine mass, dysmenorrhea (detected by physical examination) | 0/0/0 | 18.6 | 5.2 | 100 | Laparoscopic resection of uterine lesions | no | 21 |
Note: G, gravidity; P, parity; A, abortion; WBC, white blood cell; Hb, hemoglobin; CA125, cancer antigen 125; UIMT, uterine inflammatory myofibroblastic tumor.
All 6 UIMT cases (100%) underwent ultrasonography, with imaging features summarized in Table 2. All lesions were solid and originated in the myometrium. Three (50%) were confined to the myometrium, 2 (33.3%) protruded toward the submucosa, and 1 (16.7%) extended toward the subserosa. Sonographically, 5 lesions (83.3%) were hypoechoic and 1 was hyperechoic, all demonstrating heterogeneous internal echoes and a characteristic “blurred halo sign”—manifested as scattered strip or patchy slightly hyperechoic areas within a hypoechoic background. Five tumors (83.3%) were oval, and 1 was elongated, with maximum diameters ranging from 4.3 to 9.3 cm (median 6.9 cm). Four (66.7%) had well-defined margins, and 2 (33.3%) had poorly defined boundaries.
| Number | Location | Echogenicity | Echo structure | Shape | Boundary | Solid/cystic | Maximum diameter of the tumor (cm) | Change in tumor size | CDFI (Adler classification) |
| 1 | Submucosal | hypoechoic | Heterogeneous echo | elongated | clear | solid | 4.3 | First detected | 2 |
| 2* | Intramural | hyperechoic | Heterogeneous echo | oval-shaped | clear | solid | 5.7 |
Increased by 1 cm in two months ( |
3 |
| 3* | Submucosal | hypoechoic | Heterogeneous echo | oval-shaped | clear | solid | 3.6 |
Increased by 2 cm in four months ( |
3 |
| 4 | Intramural | hypoechoic | Heterogeneous echo | oval-shaped | poorly defined | solid | 7.3 | No change within one month | 2 |
| 5 | Subserosal | hypoechoic | Heterogeneous echo | oval-shaped | clear | solid | 7.1 | First noted | 2 |
| 6 | Intramural | hypoechoic | Heterogeneous echo | oval-shaped | poorly defined | solid | 9.3 | No change within one month | 2 |
Note: CDFI, color Doppler Flow Imaging; * indicates tumor enlargement.
According to the Adler classification [4] of color Doppler flow, 4 lesions (66.7%) were Grade 2 and 2 (33.3%) were Grade 3, showing a “colorful mosaic sign”. Two patients underwent a single ultrasound examination, while 4 underwent repeat scans. Among the 4 patients who had follow-up ultrasounds, 2 showed no change in tumor size, 1 exhibited a 1 cm increase after 2 months, and another showed a 2 cm increase after 4 months. All lesions were confined to the uterine corpus, with no evidence of extrauterine metastasis.
Grossly, the tumors appeared grayish-white to grayish-red with a moderately firm to slightly soft texture, occasionally showing mucoid changes. Among the 6 cases, 2 had well-circumscribed margins, 2 exhibited infiltrative growth, and 2 had poorly defined boundaries. Histologically, 4 (66.7%) cases were classified as the myxoid type, characterized by sparsely arranged spindle or short spindle cells within a myxoid stroma and moderate inflammatory infiltration under low magnification. The remaining 2 cases (33.3%) were dense spindle cell type, composed of compact bundles or fascicles of spindle cells with mild inflammation and focal myxoid changes. High magnification showed mild cellular atypia with abundant, lightly eosinophilic cytoplasm. Immunohistochemistry: All 6 cases (100%) showed ALK gene rearrangement confirmed by FISH. Three cases showed partial CD10 positivity, and 2 were H Caldesmon-positive. Estrogen receptor (ER), progesterone receptor (PR), Desmin, smooth muscle actin (SMA), and p16 were positive in all cases. p53 displayed a wild-type expression pattern, and the Ki67 proliferation index ranged from 5% to 30%.
All 6 patients underwent surgical treatment. One patient with a submucosal mass received a laparoscopic total hysterectomy. Three patients with intramural masses and 1 patient with a subserosal mass underwent laparoscopic local excision, while 1 patient with a submucosal mass received hysteroscopic electrosurgical resection. The surgical indications included prolonged menorrhagia with anemia, a mass diameter exceeding 5 cm, or rapid mass enlargement within a short period [5]. All patients were preoperatively diagnosed with “uterine space-occupying lesions” based on imaging examinations, and none underwent Tru-cut biopsy before surgery. During the follow-up period of 21–57 months, no cases of recurrence or metastasis were observed.
This study demonstrated that UIMT can arise in various locations within the uterine corpus [6, 7], consistent with previous findings. In addition, Bhardwaj et al. (2025) [8] reported cases involving the cervical region, suggesting that the anatomical distribution of UIMT may be relatively extensive.
In terms of internal echogenicity, UIMT typically presents as hypoechoic, although hyperechoic appearances can also occur. The latter may be associated with increased tumor cell cellularity and pronounced inflammatory cell infiltration (Fig. 1a). Moreover, most UIMT lesions exhibit heterogeneous internal echoes, likely resulting from the irregular interlacing of collagen fibers within the tumor stroma [9].
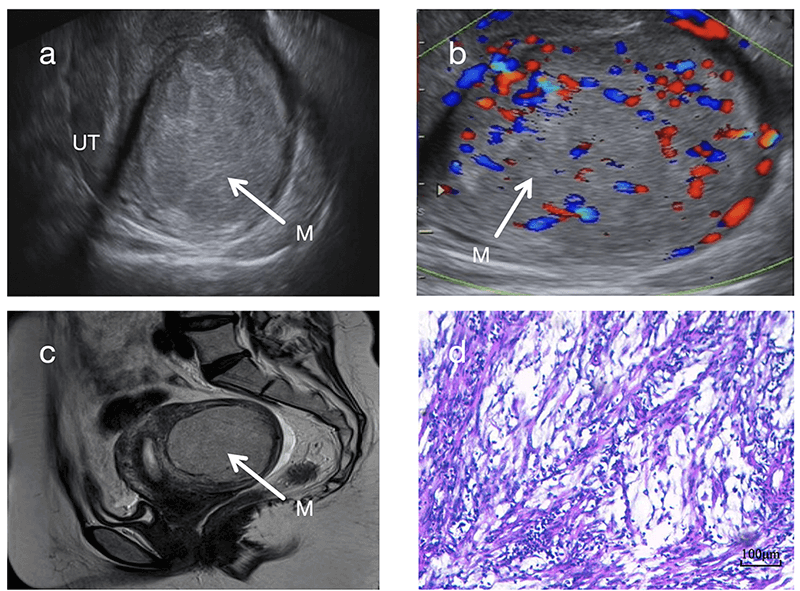 Fig. 1.
Fig. 1.
Ultrasonographic and Pathological Images of Case 2. (a)
Sagittal 2D ultrasound image showing a hyperechoic mass in the posterior uterine
wall with a “blurred halo sign”. (b) Color Doppler ultrasound demonstrating
abundant intralesional blood flow signals (Adler grade 3) with a “colorful
mosaic sign”. (c) T2-weighted MRI revealing a slightly hyperintense mass. (a,b,c)
White arrows indicate the tumor masses. (d) HE staining (100
In this study, all 6 cases of UIMT presented as solid masses, in agreement with the findings of Bai et al. (2024) [6]. Therefore, the presence of solid components may be considered a characteristic sonographic feature of UIMT. Zhao et al. (2022) [10] described a case of UIMT containing cystic components, possibly arising from inflammatory infiltration, intratumoral hemorrhage, or cystic necrosis.
From the perspective of tumor size and growth characteristics, UIMT masses are often relatively large. The median maximum diameter of UIMT masses in this study was 6.9 cm, slightly larger than the 5 cm reported by Bai et al. [6]. Additionally, the color Doppler flow signals in this cohort were more abundant, suggesting that a rich vascular supply may contribute to tumor enlargement. Notably, the masses in Case 2 and Case 3 showed rapid growth over a short period, likely reflecting the biologically active proliferation nature of UIMTs. The combination of “rapid enlargement over a short period and abundant blood flow signals” should be regarded as an important diagnostic alert for UIMT. Recognition of this pattern may prevent clinicians from overlooking potentially borderline tumors that appear morphologically benign. Ultrasonographic evaluation revealed ill-defined margins in Cases 4 and 6, which corresponded pathologically to infiltrative growth into the surrounding smooth muscle. This finding highlights the diagnostic value of evaluating tumor margins during ultrasonography. Compared with typical uterine leiomyomas, UIMTs showed richer color Doppler flow signals (Fig. 2b,d). In particular, Cases 1 and 2 exhibited extremely abundant vascularity, forming a characteristic “colorful mosaic sign” (Fig. 1b, Fig. 2b).
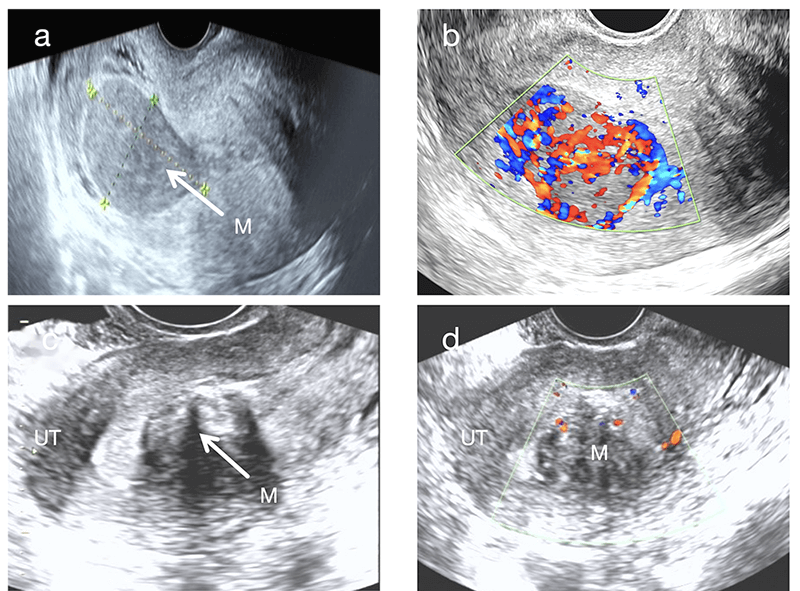 Fig. 2.
Fig. 2.
Comparison of sonographic images between submucosal UIMT (Case 1) and typical submucosal uterine leiomyoma. (a) Sagittal ultrasonographic view of the submucosal UIMT mass. White arrows indicate the tumor masses. (b) CDFI showing abundant blood flow signals within the submucosal UIMT mass (Adler grade 3) with a “colorful mosaic sign”. (c) Sagittal ultrasound view of a typical submucosal uterine leiomyoma. White arrows indicate the tumor masses. (d) CDFI showing sparse blood flow signals in the typical submucosal uterine leiomyoma (Adler grade 1).
A key observation in this study was the “blurred halo sign”, identified as a typical ultrasonographic feature of UIMT. This sign is characterized by scattered strip-like or patchy hyperechoic areas within a hypoechoic background (Fig. 1a, Fig. 2a). It is clearly distinguishable from the “whorled pattern” typically observed in conventional leiomyomas (Fig. 2c). In leiomyomas, heterogeneous hypoechoic or isoechoic areas create whorled textures due to interwoven smooth muscle cells and connective tissue fibers. In contrast, UIMT lesions display more homogeneous, dense internal echoes. Its signal on magnetic resonance imaging (MRI) also appears relatively homogeneous (Fig. 1c), whereas leiomyomas generally show lower and more disorganized echogenicity (Fig. 2a,c). However, overlap in imaging features may occur when leiomyomas undergo degenerative changes, such as mixed echogenicity or cystic transformation [11]. In such instances, the diagnostic utility of the “blurred halo sign” when combined with abundant blood flow signals becomes even more prominent.
Although most UIMTs are benign, they can infiltrate adjacent tissues or recur postoperatively [12]. Therefore, when sonography reveals a large uterine mass with patchy hyperechoic areas, indistinct margins, and abundant blood flow, clinicians should maintain a high index of suspicion for UIMT to differentiate it from ordinary leiomyomas.
UIMT can occur in women across different reproductive age groups [13, 14]. In this study, the main clinical manifestations included prolonged menstrual periods, increased menstrual flow, and dysmenorrhea. This is consistent with the findings of Bai et al. (2024) [6], who reported that “abnormal uterine bleeding is the most common symptom of UIMT”. The UIMT masses in this study were generally large, with 2 located in the submucosa. Mechanical compression of the endometrium by the masses likely contributed to increased menstrual volume and prolonged menstrual periods. Fifty percent (3 cases) of patients had dysmenorrhea, possibly due to the release of local inflammatory mediators by the tumor [15]. This proportion is slightly higher than that reported by Bai et al. (2024) [6], which may be attributed to the smaller sample size. In terms of laboratory findings, all 6 patients presented varying degrees of anemia, possibly resulting from chronic blood loss secondary to prolonged or heavy menstruation. Case 4 exhibited elevated white blood cell counts, and Cases 2 and 3 showed both elevated CA125 and white blood cell levels, findings potentially linked to local inflammatory responses elicited by the tumor stimulating the immune system. This agrees with the conclusion by Bennett et al. (2017) [15] that “UIMT exhibits significant inflammatory infiltration characteristics”. In this study, 2 patients (33.3%) had a history of thyroid disease—1 with hyperthyroidism and one with papillary thyroid carcinoma (postoperatively managed). This comorbidity may not be coincidental. Rodríguez-Castelán et al. (2019) [16] showed in rabbit models that hypothyroidism induces uterine hyperplasia and inflammation by altering sex hormone receptor expression—consistent with UIMT’s core pathological features of myofibroblastic proliferation and inflammatory infiltration, sharing a common “hormonal regulation-tissue hyperplasia-inflammation” pathway. Shinderman-Maman et al. (2018) [17], though focusing on ovarian cancer, confirmed that thyroid hormones promote tumorigenesis through transcriptional regulation, offering a potentially translatable molecular mechanism underlying UIMT-thyroid associations. Notably, no studies have quantified their co-occurrence rate, and our limited sample size precludes causal inference. Future case-control studies with larger cohorts should measure thyroid hormone levels in UIMT patients (and correlate them with tumor size or invasiveness) and assess co-expression of thyroid-related and UIMT driver genes to clarify the underlying mechanisms. In conclusion, the clinical features of UIMT are non-specific, and asymptomatic patients warrant active screening. Abnormal uterine bleeding and pelvic masses in women of childbearing age should be evaluated comprehensively.
UIMT comprises differentiated myofibroblasts and abundant inflammatory infiltration, showing intermediate biological behavior with potential for recurrence and metastasis [18, 19, 20]. Approximately 50% of cases harbor ALK rearrangement, with 87.5%–100% ALK positivity [21, 22, 23]. Here, all 6 cases showed ALK gene break signals, supporting ALK’s role in tumorigenesis and its diagnostic value as a key molecular marker [24]. Heterogeneous CD10 and H Caldesmon expression patterns further reflect molecular diversity; 2 cases had infiltrative growth into surrounding tissues, highlighting the tumor’s non-negligible invasiveness.
According to the latest WHO classification, UIMT includes three histological subtypes: (1) Loosely arranged myofibroblasts with mucus, rich vessels, and inflammatory infiltration; (2) Densely packed spindle cells with mucus or collagen regions; and (3) Scar-like hyperplasia with scattered inflammatory cells. All 6 cases in this study presented features of the myxoid and dense spindle-cell types (Fig. 1d), with mild cellular atypia and abundant cytoplasm—features that can lead to misdiagnosis as uterine leiomyoma or spindle cell sarcoma [25, 26]. Thus, accurate diagnosis requires an integrated assessment combining histopathology and immunohistochemistry, with ALK expression and rearrangement serving as key criteria.
All 6 patients underwent surgical treatment, and no recurrence or metastasis was observed during 21–57 months of follow-up. The surgical approach should be individualized based on tumor location, size, invasion depth, and the patient’s fertility requirements. Recent studies indicate that minimally invasive techniques—such as laparoscopy and hysteroscopy—are preferred for UIMT. For patients desiring fertility preservation, careful monitoring and long-term follow-up are essential [27].
This study has several limitations, including a small sample size, a retrospective design, and potential selection bias. As inflammatory myofibroblastic tumors are rare, current knowledge—derived mainly from short-term follow-up cases—remains limited. The application of contrast-enhanced ultrasound to assess lesion perfusion may enhance diagnostic accuracy.
Future studies should address the complexity of UIMT and patient heterogeneity (e.g., age, gender, genetic background). Integrating high-throughput sequencing and artificial intelligence (AI) to investigate the tumor microenvironment could elucidate the molecular mechanisms and genetic underpinnings of UIMT, thereby facilitating precision medicine, early diagnosis, and individualized treatment strategies [28].
UIMT is a rare borderline tumor characterized by typical sonographic features including a solid mass with heterogeneous echotexture (“blurred halo sign”) and abundant color Doppler flow (“colorful mosaic sign”). Ultrasound effectively delineates the tumor’s location, size, echotextural characteristics, and boundaries; moreover, it allows dynamic monitoring of lesion progression, making it an ideal tool for assessing disease evolution and postoperative recurrence. Given UIMT’s potential for invasiveness, clinicians should maintain a high index of suspicion and include it in the differential diagnosis. A deeper understanding of UIMT’s sonographic and clinical features is crucial for improving diagnostic accuracy and patient prognosis.
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
YTM: Contributed to data collection and organization, data analysis, and writing and revision of the original manuscript; MHL: Participated in data collection and organization and manuscript review; KY: Participated in data collection and organization; XD: Participated in imaging data collection and organization; HYK: Participated in study design and conception, assisted in data organization, and participated in manuscript revision; YCL: Participated in study design and conception, assisted in data organization, and participated in manuscript revision; YL: were responsible for study design, original draft, supervision and review. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethics Committee of Hunan Provincial Maternal and Child Health Hospital in 2025 (ethical approval number: No.: JSKY-2025-11-002); Relevant information has been fully disclosed to the patients, and informed consent has been obtained. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
We would like to express our sincere gratitude to all individuals who contributed to the preparation of this manuscript.
(1) Hunan Provincial Science and Technology Innovation Program (2021SK50607). (2) Scientific Research Program of Hunan Provincial Health Commission (202209023037.00).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.