






 , Abdulaziz Alshomrani 2,*, Afnan Meshal Alotaibi 1, Dalal Alhuian 1, Eynas Abdullah 3, Bappa Adamu 2, Suaad Elnour 1, Anum S. Hussaini 4
, Abdulaziz Alshomrani 2,*, Afnan Meshal Alotaibi 1, Dalal Alhuian 1, Eynas Abdullah 3, Bappa Adamu 2, Suaad Elnour 1, Anum S. Hussaini 41 Department of Obstetrics and Gynecology, College of Medicine, University of Bisha, 61922 Bisha, Saudi Arabia
2 Department of Internal Medicine, College of Medicine, University of Bisha, 61922 Bisha, Saudi Arabia
3 Department of Intensive Care, King Abdalla Hospital, Aseer Health Cluster, 67754 Bisha, Saudi Arabia
4 Department of Global Health & Population, Harvard T.H. Chan School of Public Health, Boston, MA 02115, USA
Abstract
The coronavirus disease-2019 (COVID-19) epidemic has emerged as a significant threat to global maternal health, especially with the increasing risk of serious consequences among a vulnerable population, including admission to the intensive care unit (ICU). Therefore, understanding the nature of outcomes in various populations is crucial for developing effective healthcare strategies. Thus, this study aimed to investigate the epidemiology, risk factors, and acute and long-term outcomes of COVID-19 among pregnant women in Bisha Province, Saudi Arabia. Our specific focus was on the determinants of ICU admission to ensure a thorough understanding of the impact of the disease.
This cohort study was conducted at King Abdalla Hospital from February 2020 to January 2023. This study included 88 pregnant women with COVID-19 admitted to the ICU (cases) and 120 pregnant women with COVID-19 not admitted to the ICU (controls). Electronic medical records (EMRs) were extracted for sociological, maternity, and clinical characteristics, as well as the results. A multivariable logistic regression model was used to identify independent risk factors for ICU admission and adverse outcomes.
This indicated that advanced maternal age [>35 years; odds ratios (ORs) = 2.5; p < 0.003], third-trimester gestation (ORs = 3.1; p < 0.010), low income (ORs = 2.9; p < 0.010), pre-existing hypertension (ORs = 4.8; p < 0.010), and lower educational level (ORs = 3.6; p < 0.010) were significant independent predictors of ICU admission. Furthermore, survivors of ICU admission experienced 2.5 to 3.2 times greater persistence of cardiovascular, respiratory, neurological, and mental health symptoms at 12 months post-infection compared to non-ICU patients.
This research has revealed a convergence of clinical and socioeconomic factors that significantly increases the likelihood of severe COVID-19 during pregnancy. The significant long-term morbidity among ICU survivors highlights the essential requirement for a comprehensive strategy. These findings can specifically help reduce risk for targeted delivery, improve healthcare access, particularly in post-COVID recovery clinics, and increase outcomes for this risk population in future epidemic responses.
Keywords
- COVID-19
- pregnancy
- intensive care unit
- maternal health
- long COVID effects
- short term COVID effects
- Saudi Arabia
The World Health Organization (WHO) defines the post-coronavirus disease-2019 (COVID-19) condition, or “Long COVID”, as the continuation or onset of new symptoms 3 months after the initial severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, with these symptoms lasting for at least 2 months and with no other explanation [1]. Thus, research into the impacts of COVID-19 in pregnant patients admitted to the intensive care unit (ICU) in Saudi Arabia is crucial, given the associated elevated risks [2]. Prior data have shown that women, particularly those of reproductive age, have a considerable level of post-COVID symptoms, such as fatigue and cognitive dysfunction. Moreover, the system of pregnant women is even more strained by the stresses of pregnancy and nursing. Meanwhile, a national study has shown that people who experience severe COVID-19, particularly in the ICU, are at the highest risk of long COVID; however, the epidemiology and long-term impact of this condition remain poorly understood. It is important to appreciate this burden to design appropriate follow-up care for Saudi mothers [2]. A significant percentage of pregnant women infected with COVID-19 require intensive care and respiratory support (42.3%), which leads to increased risk of ICU admission during pregnancy [1]. Fever, dyspnea, and hypoxemia are typical acute symptoms; in extreme situations, these symptoms can develop into acute respiratory distress syndrome (ARDS), which requires mechanical ventilation [2]. Furthermore, obstetric problems such as preterm birth, preeclampsia, and higher rates of cesarean delivery are closely associated with ICU hospitalization [3, 4]. In addition to many neonatal problems, infants born to moms with severe COVID-19 are more likely to experience [5]. Despite being uncommon, vertical transmission has been reported, which raises questions regarding possible long-term developmental repercussions in neonates exposed to it [4]. Long-term follow-up is also necessary because of new evidence that maternal COVID-19 may be a factor in postpartum respiratory and cardiovascular complications [6]. Pregnant women with COVID-19 have mild to moderate symptoms and are cured without serious consequences [2]. This variation emphasizes the importance of personal care in the management of COVID-19 among pregnant women [7, 8], highlighting the need for risk evaluation and individualized treatment strategies. According to research, one percent of pregnant women infected with COVID-19 require acute care and complementary oxygen therapy, which is closely associated with a high risk of ICU admission [9]. Fever, cough, and dyspnea are typical acute clinical signs; in severe cases, these symptoms can progress to acute respiratory distress requiring mechanical ventilation [10]. Additionally, a higher incidence of preterm labor and a higher rate of cesarean delivery are two adverse obstetric outcomes that are frequently linked to the need for ICU hospitalization [11, 12].
Long-term effects of COVID-19 on newborns, such as a higher chance of complications, including low birth weight and poorer Apgar scores, are a cause for concern. While vertical transmission is uncommon, this transmission does occur occasionally, and babies who test positive for SARS-CoV-2 may have long-term health and developmental consequences. Hence, it is important to consider the larger context of maternal health during the pandemic, including the acute and long-term effects of COVID-19 among pregnant women.
Specifically, COVID-19 in pregnant women has been linked to heightened chances of catastrophic maternal outcomes, such as ICU admissions and mechanical ventilation. To improve maternal–neonatal health outcomes and guide evidence-based therapies, this study aimed to present a thorough assessment of the acute and long-term effects of COVID-19 in severely ill pregnant women. Moreover, this study aimed to improve maternal health and clinical guidelines for future epidemic responses by combining data from Saudi Arabia and International Cohorts.
This was a cohort study conducted at King Abdullah Specialized Hospital and Terry Referral Hospital in Bisha province, Saudi Arabia. This design was chosen to investigate the exposure and clinical outcomes of pregnant women who were admitted to an ICU compared with those managed without ICU care. The data for this study were derived from the electronic medical records (EMRs) of King Abdalla Hospital in Bisha Province, Saudi Arabia. This study included pregnant women with laboratory-confirmed COVID-19 who were admitted between February 2020 and January 2023. All data were retrospectively collected and anonymized, with approval from the Institutional Review Board of the University of Bisha.
Pregnant women with a laboratory-confirmed positive result of SARS-CoV-2 [confirmed by reverse transcription-polymerase chain reaction (RT-PCR)] who were treated in the specified period from February 2020 to January 2023 in King Abdalla Hospital and met the inclusion criteria were enrolled.
Pregnant women with COVID-19 in the ICU for the treatment of severe or critical illness according to the WHO clinical progression scale (i.e., requiring non-invasive or invasive mechanical ventilation, vasopressor support, and/or having severe organ dysfunction) [1].
Pregnant women with confirmed COVID-19 during the same period (from February 2020 to January 2023), treated on a ward, isolation unit, or as outpatients who never required ICU care at any point during the infection period.
The following subjects were not included in the study: (1) women with a positive SARS-CoV-2 result but no documented symptoms of COVID-19; (2) patients with incomplete medical records detailing the management of COVID-19 or obstetric outcomes; (3) women who discharged from the hospital against medical advice or were transferred to an outside institution before resolution of acute illness and viable assessment of outcomes.
The sample size was calculated according to previous studies [1, 2]. The probability of a prominent risk factor (pre-existing hypertension) was 15% for the disease-free group and 30% for the case group. We estimated that a total of 138 participants would be needed to detect an effect size with 80% power at a two-sided alpha = 0.05. We recruited 88 cases and 120 controls to increase the statistical power and adjust for potential missing data. The same sampling procedures were used throughout the survey to identify all cases that met the selection criteria. We selected one uniform source from the population and provided detailed accounts for the time period of each sample.
The statistical analysis was performed using Stata Base version 19 (2024) (StataCorp LLC, College Station, Texas, USA). Descriptive statistics and regression analysis were performed. For the variable range, accurate Fisher tests were used.
COVID-19-specific information was collected, including date of diagnosis, presence of symptoms, illness severity classified according to the WHO guidelines, therapeutic interventions (e.g., oxygen therapy, corticosteroids, remdesivir), and clinical complications.
Maternal outcomes were categorized as primary and secondary measures. Primary outcomes included ICU admission, mechanical ventilation requirements, and maternal mortality; secondary obstetric outcomes comprised preeclampsia, preterm birth, mode of delivery, and postpartum hemorrhage. Newborn results included pregnancy at birth, birth weight, Apgar scores at 1 and 5 minutes, admission to the Neonatal Intensive Care Unit (NICU), and the SARS-CoV-2 RT-PCR test results for the infant. Uninsured refers to patients who did not have any form of government or private health insurance at the time of hospital admission, meaning the patients were fully responsible for all medical costs.
Short-term (acute) outcomes were defined as complications and clinical endpoints occurring during the initial hospitalization for COVID-19 [13]. These included the primary outcome of ICU admission, as well as secondary outcomes such as the requirement for mechanical ventilation, maternal mortality, obstetric complications (preeclampsia [14], preterm birth [15], mode of delivery [16], and postpartum hemorrhage [15]), and immediate neonatal outcomes (birth weight [16], Apgar scores [17], and NICU admission). Data for these outcomes were extracted directly from the EMRs for the admission period.
Long-term outcomes were assessed 12 months post-diagnosis through structured telephone interviews and a review of the EMRs. Symptoms were categorized into cardiovascular, respiratory, neurological, and mental health domains using a standardized questionnaire based on WHO post-COVID case definitions.
Follow-up percentages among ICU and non-ICU groups were tracked, and responders were compared with those lost to follow-up. Of the 88 ICU and 120 non-ICU patients, follow-up at month 12 was completed for 72 (81.8%) and 105 (87.5%), respectively. Loss to follow-up was mostly due to the individual becoming uncontactable (e.g., unavailable phone number) or refusal to be recorded. We also compared baseline characteristics (age, income, and comorbidities) between the responders and loss-to-follow-up groups; these were not significantly different, suggesting a non-differential response. We utilized the Benjamini-Hochberg false discovery rate (FDR) correction to compare persisting symptoms among different health domains and performed diagnostic procedures for our regression model, including checks of multicollinearity [variance inflation factor (VIF)], identification of outliers (Cook’s D), evaluation of model performance (area under the receiver operating characteristic, AUROC), and stability testing with bootstrap resampling (1000 times) for the coefficients.
All statistical analyses were performed using Stata Base, version 19 (2024).
Descriptive statistics were used to analyze all study variables for general
characteristics (Table 1) and the comparison of sociodemographic and clinical
characteristics between pregnant women with COVID-19 admitted to the ICU and
those not admitted (Table 2). The normality assumption for continuous variables
was assessed using the Shapiro-Wilk test and Q-Q plots. Continuous data that
showed approximately normal distribution were reported as the mean
| Characteristic | Category/statistic | Value |
| Age (years) | Mean |
31.9 |
| Age |
69 (33.2%) | |
| Gestational age (weeks) | Mean |
29.9 |
| Third trimester, n (%) | 80 (38.5%) | |
| Income level | Low income, n (%) | 110 (52.9%) |
| Middle/high income, n (%) | 98 (47.1%) | |
| Pre-existing conditions | Hypertension, n (%) | 40 (19.2%) |
| Diabetes, n (%) | 20 (9.6%) | |
| Education level | High school or lower, n (%) | 60 (28.8%) |
| College degree, n (%) | 148 (71.2%) |
n, number of participants.
| Characteristic | ICU cases (n = 88) | Non-ICU controls (n = 120) | p-value | |
| Age (years) | ||||
| Mean |
34.5 |
30.2 |
||
| Age |
45 (51.1%) | 24 (20.0%) | ||
| Gestational age (weeks) | ||||
| Mean |
32.1 |
28.5 |
||
| Third trimester | 50 (56.8%) | 30 (25.0%) | ||
| Socioeconomic factors | ||||
| Low income | 65 (73.9%) | 45 (37.5%) | ||
| Uninsured | 28 (31.8%) | 12 (10.0%) | ||
| Pre-existing conditions | ||||
| Hypertension (chronic) | 30 (34.1%) | 10 (8.3%) | ||
| DM (pre-gestational) | 15 (17.0%) | 5 (4.2%) | ||
| Education level | ||||
| High school or lower | 40 (45.5%) | 20 (16.7%) | ||
| College degree | 48 (54.5%) | 100 (83.3%) | ||
ICU, intensive care unit; COVID-19, coronavirus disease-2019; DM, diabetes mellitus.
Multivariable logistic regression analysis was used to identify factors
associated with the primary outcomes (ICU admission) and with combined adverse
maternal outcomes. The reference model included variables with a p-value
Model diagnostics were performed based on multicollinearity (tested with VIF:
all VIF
The final multivariable logistic regression model for ICU admission (Table 3)
was adjusted for the following covariates selected a priori based on clinical
relevance and bivariate analysis (p
| Variable | ORs | 95% CI | p-value |
| Age |
2.5 | 1.4–4.5 | |
| Third trimester | 3.1 | 1.8–5.5 | |
| Low income | 2.9 | 1.7–4.9 | |
| Uninsured | 4.5 | 2.0–10.3 | |
| Pre-existing hypertension | 4.8 | 2.2–10.4 | |
| Pre-existing diabetes | 2.3 | 1.1–5.0 | |
| High school education or lower | 3.6 | 1.9–6.7 |
OR, odds ratio. The final multivariable model was adjusted for all listed variables.
The final multivariable model for adverse outcomes was adjusted for the
covariates in the ICU model (Table 4), with the addition of multiparity and
obesity [body mass index (BMI)
| Factors | ORs | 95% CI | p-value |
| Age |
2.8 | 1.6–5.0 | |
| Third trimester | 3.4 | 2.0–5.8 | |
| Low income | 3.2 | 1.9–5.4 | |
| Uninsured | 4.8 | 2.3–10.7 | |
| Pre-existing hypertension | 5.1 | 2.4–10.9 | |
| Diabetes | 2.6 | 1.2–5.6 | |
| High school education or lower | 3.9 | 2.1–7.3 | |
| Multiparity (more than 2 children) | 2.1 | 1.1–4.0 | |
| Obesity (BMI |
3.0 | 1.5–6.0 |
BMI, body mass index. The final multivariable model was adjusted for all listed variables.
Variables with a p-value
A total of 208 pregnant women with a mean maternal age of 31.9 years (
A significant portion of the participants (33.2%, n = 69) were aged 35 years or
older. The mean gestational age at diagnosis was 29.9 weeks (
Table 2 presents the data for pregnant women with COVID-19, stratified by ICU
admission status. Significant differences were observed across multiple
variables. The mean maternal age was significantly higher among women admitted to
the ICU (34.5
Gestational age at diagnosis also differed significantly, with ICU patients
presenting at a later stage of pregnancy (32.1
Marked socioeconomic disparities were observed. Low-income status was reported
in 73.9% of the ICU patients versus 37.5% of the non-ICU patients (p
Pre-existing medical conditions were more prevalent among patients admitted to
the ICU. Pre-existing hypertension was reported in 34.1% of the ICU patients
versus 8.3% of the non-ICU patients (p
Educational attainment differed significantly between groups. Nearly half
(45.5%) of ICU patients had a high school education or lower, compared with
16.7% in the non-ICU group (p
The evaluation of risk factors associated with ICU admission among pregnant
women with COVID-19 (Table 3). Pregnant women aged over 35 years exhibited a
2.5-fold increased risk of ICU admission (ORs = 2.5, 95% CI: 1.4–4.5;
p
The need for ICU care (ORs = 4.8, 95% CI: 2.2–10.4; p
Women with a high school education or lower had an ORs of 3.6 (95% CI:
1.9–6.7; p
Model diagnostics and validation: The multivariable logistic regression models demonstrated good performance and calibration. The AUROC curve for the main ICU admission model (Table 3) was 0.85 (95% CI: 0.80–0.90), representing excellent discrimination. The model was acceptably calibrated, with a non-significant Hosmer-Lemeshow goodness-of-fit test (p = 0.42). Internal validation by bootstrap resampling (1000 iterations) yielded an optimism-corrected AUROC of 0.84. For a model predicting any adverse outcome (Table 4), the AUROC was 0.87 (95% CI: 0.82–0.92), and this model also had good calibration (Hosmer-Lemeshow p = 0.51), with an optimism-corrected AUROC for the area under the curve (AUC) of 0.86 vs. Steyerberg et al. [19]. Impact of country on bacteremia: The population blood culture positivity rate ranged from 2 to 52% across countries. There was no multicollinearity problem in either model, as all VIF values were below 2.5. Influence of observations: influential observations were not detected using Cook’s distance and DFBETAs, as no outliers were found to substantially affect the model coefficients.
The findings of the logistic regression analysis, including adverse outcomes
among pregnant women with COVID-19, are summarized in Table 4. This study
identified factors contributing to poor health outcomes for this population. More
than 35 pregnant women exhibited high OR values (2.8; 95% CI: 1.6–5.0;
p
Significant risk factors for ICU admission are revealed by the COVID-19 results
in pregnant women (Fig. 1). The likelihood of developing a serious illness
requiring intensive care is much higher for women over 35, those in the third
trimester, and those with lower incomes or no health insurance. Furthermore,
pre-existing diseases, such as pre-existing diabetes and hypertension, were shown
to increase the risk further. The robustness of these findings is further
supported by the statistically significant associations (p
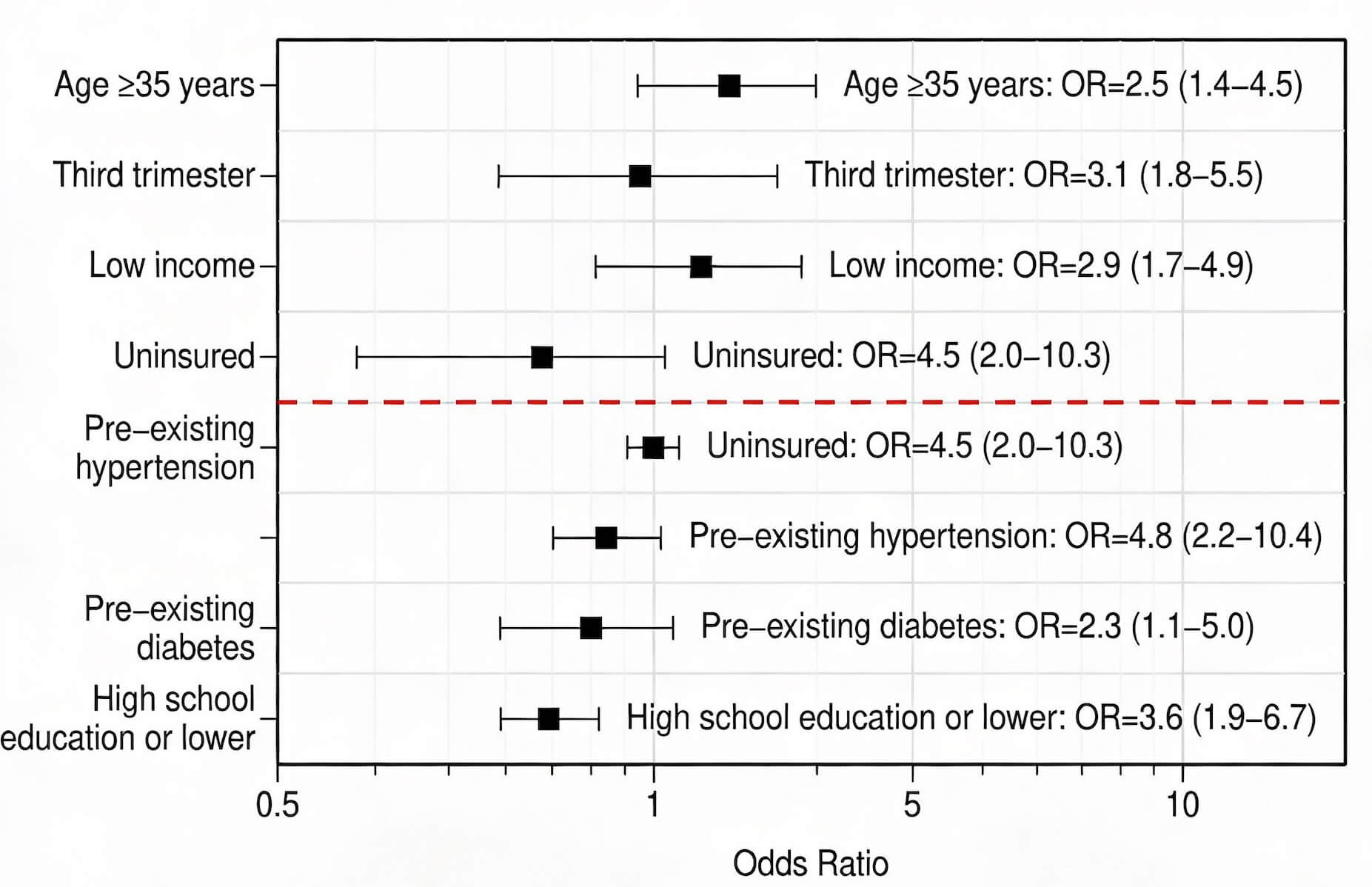 Fig. 1.
Fig. 1.
ORs for associated risk factors. The red dashed line indicates no increased risk (ORs = 1).
The analysis of the data in this study included visualizations of study group distributions, age-related trends, medical and socioeconomic circumstances, and risk factors for ICU admission to substantiate these conclusions. Meanwhile, future studies should examine specific issues in more detail, conduct more comprehensive statistical analyses, or introduce alternative visualizations.
Both the risk of ICU admission and the rate of complications increase significantly with increasing gestational age (Fig. 2), especially in the third trimester. Indeed, the third trimester is associated with more than twice the risk of the previous trimesters, with a risk ratio of 2.27. The risk ratios were significantly lower in the first and second trimesters. These results emphasize how crucial proactive care and careful observations are for pregnant women in advanced gestational stages who are infected with COVID-19.
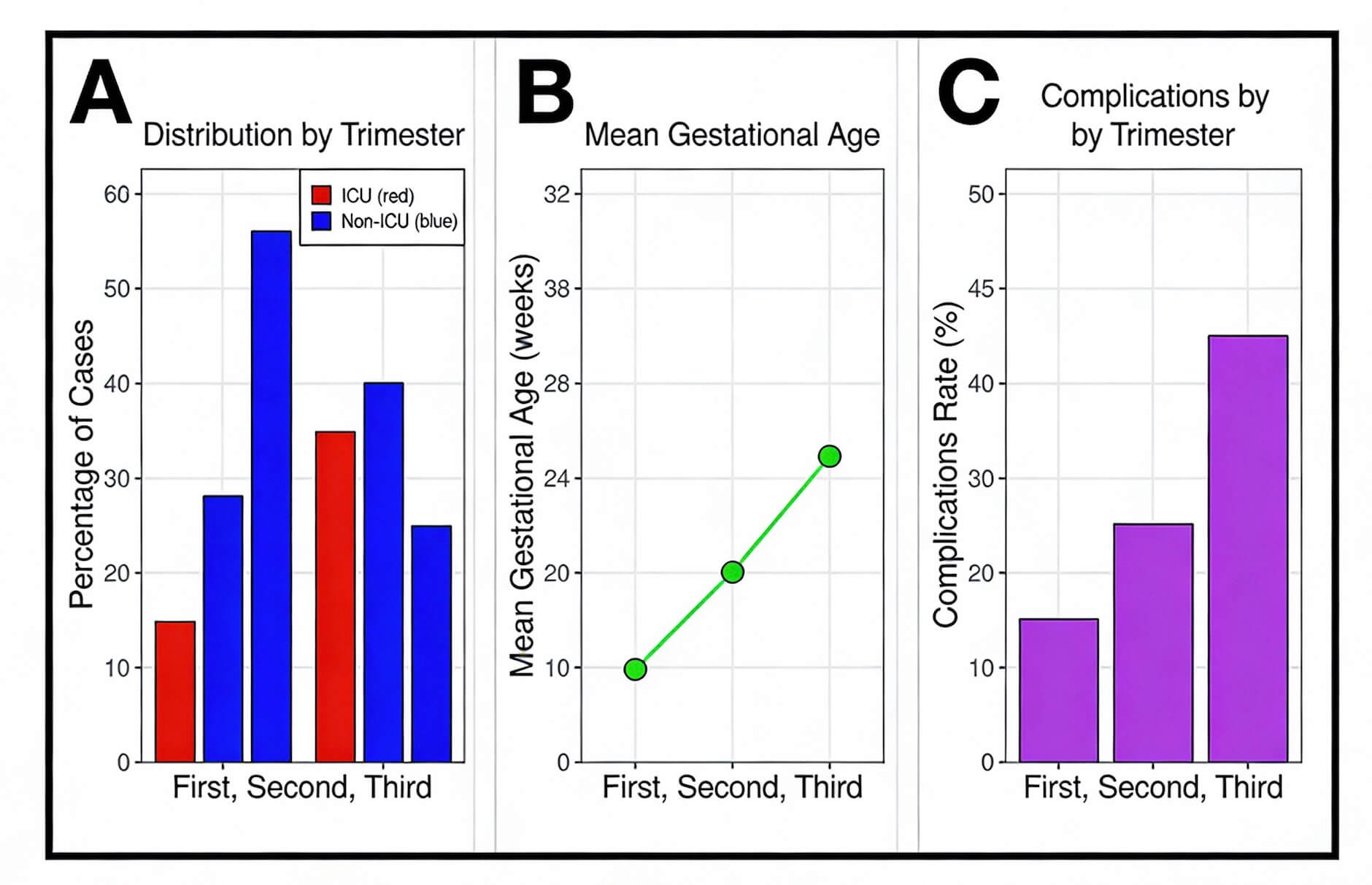 Fig. 2.
Fig. 2.
The risk ratios for ICU admission by trimester. (A) Distribution of cases by trimester, comparing ICU versus non‑ICU groups (percentage of cases in each trimester). (B) Mean gestational age (weeks) by trimester. (C) Complications rate by trimester.
Fig. 3 illustrates notable differences between pregnant women who required intensive care (ICU group) and those who did not (non-ICU group), based on a thorough examination of long-term COVID-19 outcomes. These data show that patients admitted to the ICU continue to face significant symptom burdens even after a year of infection.
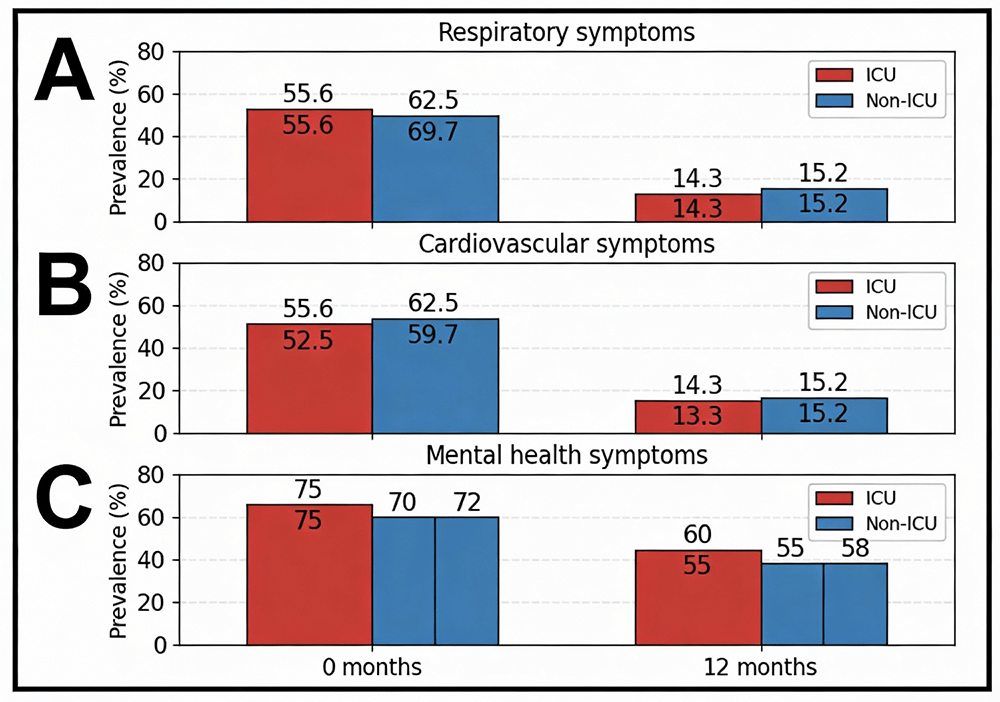 Fig. 3.
Fig. 3.
Long-term outcomes of COVID-19 in pregnancy. (A) Respiratory symptom prevalence at 0 and 12 months, comparing ICU versus non-ICU groups. (B) Cardiovascular symptom prevalence at 0 and 12 months, comparing ICU versus non-ICU groups. (C) Mental health symptom prevalence at 0 and 12 months, comparing ICU versus non-ICU groups.
The ICU group was 3.19 times more likely to have long-term problems than the non-ICU patients, with the most frequent cardiovascular complications. This firmness of symptoms, even after improvement in both groups, underscores the immediate need for long-term care and targeted treatments. The overall prevalence was 2.8 times higher in the ICU cohort, as ICU patients experienced a 20.22% reduction in symptoms compared with a 28.23% reduction in the non-ICU group.
The recovery rate for respiratory symptoms was nearly twice as high among non-ICU patients (32.43%) as among ICU patients (16.78%). This significant disparity of 15.65% underscores the long-term effects of severe COVID-19 on lung function, particularly in ICU patients.
The most significant disparities in recovery between groups were noted in mental health and fatigue (16.94% and 16.43%, respectively). Across all areas, non-ICU patients showed an improvement of over 29%, whereas ICU patients continued to experience difficulties (persistence ratios of 2.68 and 2.51, respectively).
Despite being the smallest recovery gap (2.05%), neurological symptoms had one of the highest firmness ratios (2.86), suggesting long-term difficulties with nerves and cognition.
With the ICU patients recovering by just 14.38% compared to 23.38% in the non-ICU group—a 9% difference—sleep problems remained moderately persistent. This persistence of sleep problems in the ICU patients underscores the need for continued care and support even after the acute phase of the disease.
According to the study, patients discharged from the ICU exhibited 2.5 to 3.2 times higher symptom persistence across all health categories than those not admitted to the ICU, indicating notable differences in long-term recovery from COVID-19. The most persistent symptoms over time were neurological and cardiovascular. Nevertheless, the most essential treatment interval was noted in mental health and exhaustion, which highlights the important requirement of integrated psychological support in post-ICU care. Non-ICU patients had a frequently high recovery rate, despite improvement being observed in both groups. This underscores the need for specialized, prolonged treatment for severe COVID-19 survivors and shows how the severity of the disease at the beginning predicts long-term prognosis. According to these findings, high-risk patients should have their cardiovascular, neurological, and mental health monitored as part of risk-stratified follow-up regimens. These results emphasize critical needs for pregnant patients for exceptional care and long-term monitoring, which recur from severe COVID-19, especially those who required ICU admission. Therefore, future studies should test targeted remedies to increase recovery rates in high-risk populations.
The persistence of symptoms at 12 months post-infection across cardiovascular, respiratory, neurological, and mental health domains was assessed (Table 5). As shown in Fig. 3, patients admitted to the ICU were significantly more likely to have symptoms persisting across all domains than those not treated in an ICU. To correct for multiple comparisons among these four major symptom domains, we applied the Benjamini–Hochberg method to the FDR. Symptom persistence between the ICU and non-ICU cohorts for each domain was treated as a family of tests for the FDR adjustment. Differences in chronicity remained significant across the four health domains after FDR correction.
| Symptom domain | Persistence in ICU cohort, N (%) | Persistence in non-ICU cohort, N (%) | Raw p-value | FDR-adjusted p-value (q-value) |
| Cardiovascular | 45/72 (62.5) | 14/105 (13.3) | ||
| Respiratory | 40/72 (55.6) | 15/105 (14.3) | ||
| Neurological | 38/72 (52.8) | 13/105 (12.4) | ||
| Mental health | 43/72 (59.7) | 16/105 (15.2) |
N = percetage; FDR, false discovery rate.
This study provides a critical evaluation of the risk factors and consequences
of ICU admission among pregnant patients with COVID-19 in the Bisha Province of
Saudi Arabia. Our results clearly show that the following factors are significant
and independent predictors of severe disease requiring intensive care:
pre-existing comorbidities (diabetes and hypertension), third-trimester
gestation, low socioeconomic status (as indicated by low income and lack of
health insurance), advanced maternal age (
After the acute period, we examined long-term outcomes and found a striking difference between the ICU and non-ICU patients. Cardiovascular, pulmonary, neurological, and mental health issues were among the symptoms that patients in critical care reported remaining present for 2.5 to 3.2 times longer at 12 months after infection. Thus, a substantial long-term morbidity burden that goes well beyond the immediate perinatal period is highlighted by the exceptionally high persistence of neurological and cardiovascular symptoms, as well as the large recovery gap in mental health and fatigue. The “long COVID” pattern in our obstetric cohort is consistent with findings in the general population, where prolonged recovery and multi-organ sequelae are predicted mainly by the initial severity of the disease [30, 31]. However, the prevalence of “long COVID” during the postpartum phase adds a complex dimension and may affect important processes, such as nursing, mother–infant bonding, and family dynamics, thereby increasing the burden on public health [32, 33]. Thus, psychological and psychiatric support must be urgently incorporated into standard postpartum follow-up protocols for severe COVID-19 survivors, as this area is frequently disregarded in traditional obstetric care, given the observed substantial mental health burden, which includes fatigue and likely elements of post-traumatic stress disorder from the ICU experience [34, 35].
A comprehensive public health and clinical response is necessary due to the confluence of clinical and socioeconomic risk factors identified in this study. Firstly, our results strongly support prioritizing early antiviral therapy and booster vaccinations for pregnant women, particularly those with comorbidities and in the third trimester, as these interventions are safe during pregnancy and have been shown to reduce disease severity significantly [36, 37]. Second, continuously increasing low-income support and promoting access to healthcare for pregnant women are strictly required, given the significant risk of socioeconomic disadvantage. To mitigate the effects, initiatives may include culturally sensitive patient education, strengthening social support networks, and access to prenatal care [38, 39]. Lastly, for women recuperating from severe COVID-19, long-term follow-up data require the creation of specialized, multidisciplinary postnatal clinics that provide integrated therapy to holistically treat the neurological, mental, and cardiac consequences [40, 41].
This study provides strong evidence of sufficient long-term sickness associated with severe COVID-19 during pregnancy, in addition to validating the risk variables known in settings related to Saudi Arabia. In light of the current and potential epidemic hazards, these conclusions are crucial for developing targeted interventions, informing health policy, and optimizing care for this vulnerable group.
Based on our research, we suggest a four-pillar structure for pandemic preparedness (Fig. 4): (1) improved prenatal risk assessment, (2) fair access to maternity care, (3) improved infection control during pregnancy, and (4) long-term follow-up after recovery. This comprehensive strategy prioritizes high-risk women, addressing both acute management and long-term outcomes, and ensures that the health system can protect maternal and newborn health through evidence-based, targeted interventions in the event of future medical emergency conditions.
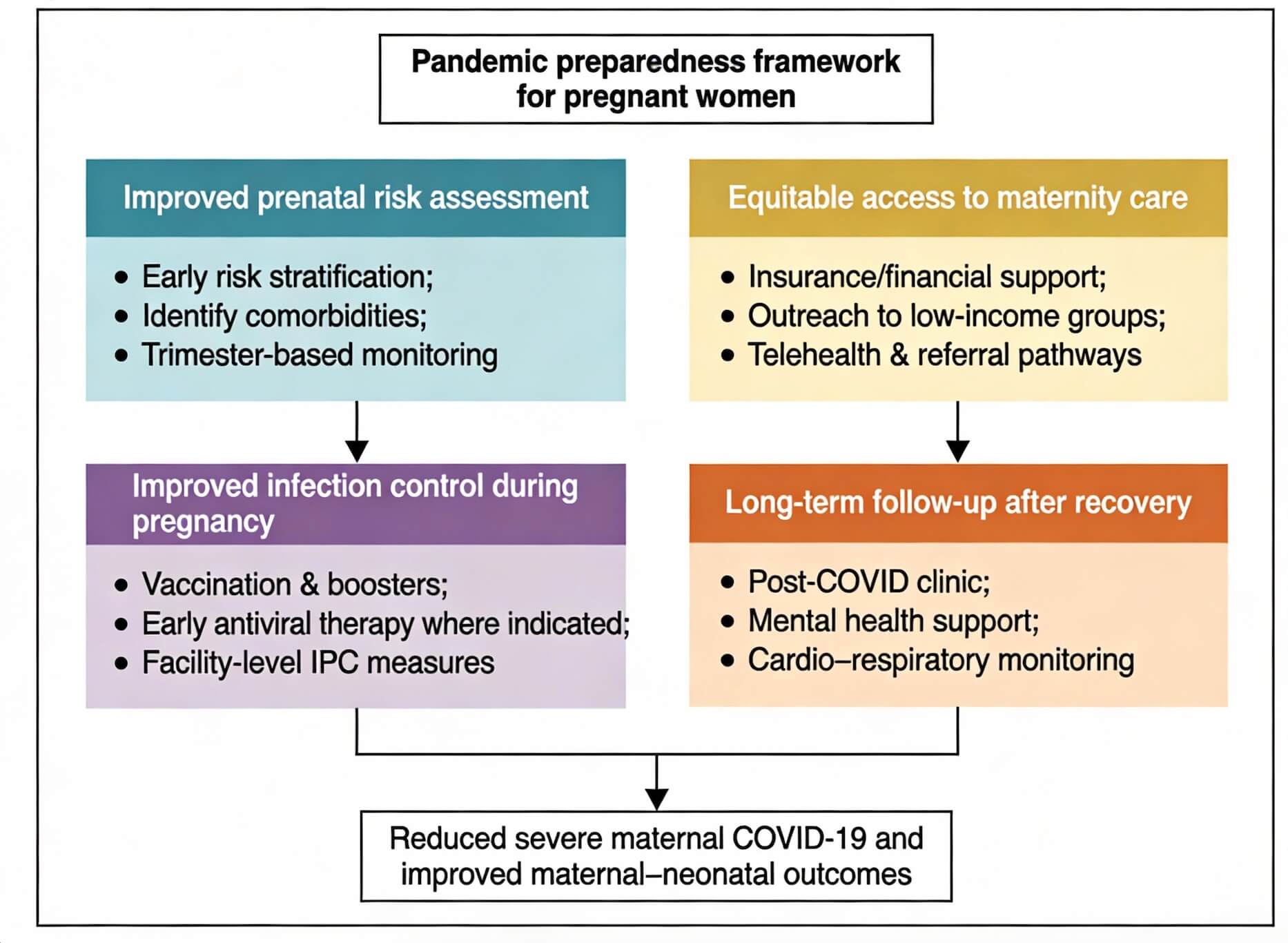 Fig. 4.
Fig. 4.
A framework for implementing targeted interventions for pregnant women during pandemics.
During an epidemic, this structure provides a broad, evidence-based approach to protect the health of mothers and their embryos. This framework encompasses a comprehensive range of care, from prenatal risk evaluation to postpartum recovery, and is centered around four key interactions.
This study has several limitations that should be considered when interpreting the findings. First, the single-center design at a tertiary care hospital in Bisha Province may limit the generalizability of the results to other regions or healthcare settings within Saudi Arabia. Second, the retrospective nature of the data collection is subject to potential biases from incomplete or inaccurate documentation in the EMRs; meanwhile, long-term outcomes were assessed via structured interviews, and recall bias remains a possible concern. Furthermore, although sufficient for the primary analysis, the sample size may have been underpowered to detect more subtle associations or rare adverse outcomes. Unmeasured confounding factors, such as detailed vaccination status, specific viral variants, or nuances in prenatal care adherence, could have influenced the results but were not accounted for in our analysis. Finally, the assessment of long-term outcomes via structured telephone interviews, while necessary for follow-up, is inherently susceptible to recall and reporting bias, which may affect the accuracy of the symptom persistence data.
This study identified a confluence of clinical and socioeconomic factors that significantly increase the risk of severe COVID-19 in pregnancy. The substantial long-term morbidity among ICU survivors underscores the critical need for a multifaceted approach. We recommend implementing targeted prenatal risk stratification, enhancing healthcare access, and establishing dedicated post-COVID recovery clinics to mitigate risks and improve outcomes for this vulnerable population in future pandemic responses.
COVID-19, coronavirus disease-2019; ICU, intensive care unit; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; ARDS, acute respiratory distress syndrome; NICU, Neonatal Intensive Care Unit; RT-PCR, reverse transcription-polymerase chain reaction; EMRs, electronic medical records; IQR, interquartile range; OR, odds ratio; aOR, adjusted odds ratio; BMI, body mass index; IRB, Institutional Review Board; WHO, World Health Organization; FDR, false discovery rate; VIF, variance inflation factor; AUROC, area under the receiver operating characteristic; AUC, area under the curve; DM, diabetes mellitus.
The data used in this study are available from the corresponding authors upon request.
EM and AA conceived and designed the study. AMA, DA, EA, and SE were responsible for data acquisition and patient enrollment. BA performed the statistical analysis. ASH contributed to the interpretation of data and critical revision of the manuscript for important intellectual content. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of University of Bisha [Ref No.: UB-RELOC H-06-BH-087/(1810.24)]. The requirement for informed consent was waived by the IRB due to the retrospective nature of the study. All patient data were handled with strict confidentiality. Data were anonymized and de-identified at the point of collection and stored on a password-protected hospital server, accessible only to the principal investigators, in compliance with the Declaration of Helsinki.
We gratefully acknowledge the contributions of the medical records department and the intensive care unit team at King Abdalla Hospital. Our thanks also go to the Institutional Review Board of the University of Bisha for their guidance and approval.
The authors extend their appreciation to the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project number (Ub-11-1442).
The authors declare no conflict of interest.
During the preparation of this manuscript, the authors mainly used Grammarly, 2025 for language polishing, grammar improvement, and proofreading purposes. The AI tool was employed to enhance the clarity, readability, and grammatical accuracy of the text when the authors developed the intellectual content fully. All scientific and analytical materials, including data interpretation, conclusions, and scholars, remain the basic work of writers. The use of grammar did not affect the research method, result, or intellectual direction of study. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.