







 , Yagmur Minareci 1, Canan Kucukgergin 2, Abdurrahman Fatih Aydin 2, Hamdullah Sozen 1, Mehtap Akin Efe 1, Atacem Mert Aytekin 1, Mehmet Yavuz Salihoglu 1, Samet Topuz 1
, Yagmur Minareci 1, Canan Kucukgergin 2, Abdurrahman Fatih Aydin 2, Hamdullah Sozen 1, Mehtap Akin Efe 1, Atacem Mert Aytekin 1, Mehmet Yavuz Salihoglu 1, Samet Topuz 11 Department of Obstetrics and Gynecology, Istanbul Faculty of Medicine, Istanbul University, 34093 Istanbul, Türkiye
2 Department of Biochemistry, Istanbul Faculty of Medicine, Istanbul University, 34093 Istanbul, Türkiye
Abstract
Endometrial cancer (EC) is the second most common gynecological malignancy and remains a major contributor to morbidity and mortality among women worldwide. Current diagnostic and prognostic tools have limited accuracy, highlighting the need for reliable, non-invasive biomarkers. Non-coding RNAs (ncRNAs), including long non-coding RNAs (lncRNAs) and microRNAs (miRNAs), have emerged as promising candidates. This study aimed to investigate serum lncRNA HOXA transcript antisense RNA myeloid-specific 1 (HOTAIRM1) and miR-182-5p expression levels in EC and evaluate their diagnostic value and association with clinicopathological features.
This prospective cohort study analyzed serum samples that were prospectively collected from 73 women with histologically confirmed EC and 76 controls with non-malignant gynecological conditions. Quantitative real-time polymerase chain reaction (qRT-PCR) was used to quantify serum lncRNA HOTAIRM1 and miR-182-5p expression levels. Associations with clinicopathological parameters and diagnostic performance were evaluated.
Serum expression levels of lncRNA HOTAIRM1 were significantly higher in EC patients (median [interquartile range (IQR)]: 1.36 [0.74–3.37]) than in controls (1.03 [0.58–2.03]; p = 0.043), whereas miR-182-5p levels showed no significant difference (p = 0.327). Receiver operating characteristic (ROC) curve analysis demonstrated that serum lncRNA HOTAIRM1 had high specificity (93.2%) but low sensitivity (29.6%) for EC diagnosis. No significant associations were identified between either biomarker or clinicopathological variables (p > 0.05).
This study provides one of the first evaluations of circulating lncRNA HOTAIRM1 and miR-182-5p in serum samples from patients with EC. Our findings suggest that serum lncRNA HOTAIRM1, but not miR-182-5p, may serve as a potential non-invasive biomarker for EC. Although its limited sensitivity restricts its role as a standalone diagnostic tool, its high specificity supports potential clinical relevance. These preliminary results should be interpreted with caution, as they represent an initial exploratory analysis of circulating lncRNA HOTAIRM1 and miR-182-5p in EC.
Keywords
- endometrial cancer
- lncRNA HOTAIRM1
- miR-182-5p
- non-coding RNAs
- serum
- biomarkers
- diagnosis
- prognosis
Endometrial cancer (EC) is the second most common gynecological malignancy and the fourth most frequently diagnosed cancer among women worldwide, representing a significant public health concern with notable morbidity, mortality, and socioeconomic burden [1]. Despite advances in imaging and histopathology, there are currently no validated, non-invasive biomarkers in clinical practice for early diagnosis, post-treatment monitoring, or prognostic assessment of EC.
Non-coding RNAs (ncRNAs), transcribed from approximately 98% of the human
genome that do not encode proteins, have emerged as critical regulators of gene
expression. They are broadly classified into long non-coding RNAs (lncRNAs,
miRNAs implicated in cancer pathogenesis are generally categorized as oncogenes or tumor suppressors. Oncogenic miRNAs are overexpressed in tumor cells, whereas tumor suppressor miRNAs show reduced expression. More than 2000 miRNAs have been identified in humans, with 754 reported as potential biomarkers in EC in the past five years [12, 13, 14]. Several of these miRNAs are associated with key clinical features such as lymph node (LN) involvement, disease stage, metastatic status, and histological subtype [12, 13, 14]. Among these, miR-182-5p has shown variable expression across cancer types, functioning in key signaling pathways involved in carcinogenesis, tumor progression, metastasis, and treatment response in gynecological cancers [15]. In EC, miR-182-5p has been identified as an oncogenic miRNA [15, 16].
Similarly, lncRNAs have been shown to regulate mRNAs, miRNAs, and proteins through various signaling pathways, thereby influencing tumor initiation, progression, cell differentiation, cell cycle regulation, and apoptosis [10]. The role of lncRNAs in EC has been highlighted in several studies. Among them, HOXA transcript antisense RNA myeloid-specific 1 (HOTAIRM1) has emerged as a cancer-related lncRNA that regulates HOXA1 gene expression and promotes cell proliferation, migration, and invasion in type I EC cells [17, 18]. Its expression, along with HOXA1, is significantly upregulated in type I EC tissues and correlates with FIGO (The International Federation of Gynecology and Obstetrics) stage and LN metastasis [17, 18].
The interplay between lncRNAs and miRNAs—often via a “molecular sponge” mechanism—can disrupt tumor suppressor miRNA activity, leading to dysregulation of downstream mRNA targets and contributing to EC progression [19].
Previous studies have reported elevated tissue expression of both lncRNA HOTAIRM1 and miR-182-5p in EC, yet their serum levels remain largely unexplored [20, 21]. The primary objective of this study was to evaluate the serum expression levels of lncRNA HOTAIRM1 and miR-182-5p as potential non-invasive diagnostic biomarkers for distinguishing EC from non-malignant gynecological conditions. The secondary objectives were to investigate their associations with key clinicopathological features and to explore potential correlations between lncRNA HOTAIRM1 and miR-182-5p expression levels.
This prospective cohort study utilized serum samples that were prospectively collected from 73 patients with histologically confirmed EC and 76 controls with benign gynecological conditions. The study was conducted at the Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Istanbul Faculty of Medicine, Istanbul University, in collaboration with the Department of Biochemistry. Patient enrollment and serum collection took place between 2018 and 2019. The initial approval from the Institutional Review Board and Ethics Committee was obtained in 2018 (Approval No: 2018/1609). As the scientific scope of the research expanded to include additional ncRNAs, further approval was granted in 2023 (Approval No: 2023/119), supported by the Istanbul University Scientific Research Projects Unit (Project ID: TTU-2023-39847). This study was initiated prior to the requirement for registration of prospective cohort studies. All procedures were conducted in accordance with the Declaration of Helsinki, and written informed consent obtained at baseline included permission for long-term storage and future use of biospecimens.
The study population included women with histologically confirmed EC, all diagnosed by endometrial biopsy and subsequently managed surgically. The control group consisted of women who presented to the general gynecology outpatient clinic for routine gynecological evaluation due to non-malignant indications and were confirmed to have no evidence of uterine or adnexal pathology on clinical, ultrasonographic, or laboratory assessment. To minimize potential confounding factors, women with uterine (cervical, myometrial, or endometrial) and/or ovarian/tubal pathologies—including benign gynecologic conditions such as uterine fibroids, ovarian cysts, endometrial polyps, and endometrial hyperplasia—were excluded. In particular, patients diagnosed with atypical and/or complex endometrial hyperplasia were explicitly excluded to avoid potential overlap with premalignant endometrial conditions. Exclusion criteria for the EC group included final histopathology not confirming EC, the presence of synchronous malignancies, recurrent disease, or prior oncology treatment (chemotherapy, radiotherapy, or immunotherapy).
All patients with EC were routinely followed up every three months after their initial surgery according to institutional protocol. Each follow-up visit included gynecological examination, transvaginal ultrasonography, and magnetic resonance imaging (MRI) to evaluate possible disease recurrence. Recurrence was defined as radiologically or histopathologically confirmed evidence of disease reappearance after initial treatment. In cases where MRI findings were unequivocally consistent with recurrent disease, diagnosis and treatment planning were based on radiological confirmation. For patients with indeterminate or atypical radiological or clinical findings, histopathological verification was obtained before initiating treatment. For recurrence-related analyses, only patients with complete recurrence data were included. Two patients had incomplete follow-up; their recurrence status was recorded as missing. We did not perform any imputation for missing data. A complete-case (available-case) analysis was therefore used for recurrence outcomes.
Both EC patients and controls were recruited consecutively during the predefined
study period. No prior sample size calculation was performed; however, based on
the total sample size, a post hoc power analysis was conducted using the G*Power
statistical software (version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf,
Düsseldorf, Germany). For a two-tailed t-test with an alpha level of
0.05 and a moderate effect size (d = 0.5), the calculated statistical power of
the study was 88%, indicating adequate power to detect clinically meaningful
differences between groups. A p-value
Venous blood samples were obtained from patients with EC at the time of
diagnosis and from controls during outpatient visits. All samples were
transferred to the Department of Biochemistry within 15 minutes of collection,
centrifuged, aliquoted, and immediately stored at –80 °C in RNase-free
tubes to avoid repeated freeze–thaw cycles and minimize RNA degradation. The
storage duration before RNA extraction ranged from 38 to 50 months. All EC and
control samples were processed and analyzed simultaneously to minimize batch
effects. Previous studies have demonstrated that circulating miRNAs remain stable
for years when stored at ultra-low temperatures [22, 23, 24], and current biospecimen
practice guidelines indicate that serum or plasma aliquots stored at
Expression levels of miR-182-5p and lncRNA HOTAIRM1 were quantified using a Rotor-Gene Q real-time PCR system (Qiagen, Germantown, MD, USA). Primers were purchased from Qiagen Technologies (Germantown, MD, USA): miRCURY LNA™ miRNA PCR Assay U6 (Cat. no. YP02119464), miRCURY LNA™ miRNA PCR Assay hsa-miR-182-5p (Cat. no. YP00206070), RT2 lncRNA qPCR Assay (HOTAIRM1) (Cat. no. 330701LPH10483A), and RT2 lncRNA qPCR Assay (GAPDH) (Cat. no. 330001PPH00150F). Relative expression levels were calculated using the 2-ΔΔCT method, normalizing to U6 (for miRNA) and GAPDH (for lncRNA). All qRT-PCR reactions were performed in triplicate (technical replicates) using the same instrument and reagent lots to ensure reproducibility. Negative (no-template) controls were included in every run. The average coefficient of variation (CV) for cycle threshold (Ct) values among replicates was below 2%, indicating high intra-assay precision. Moreover, all patient and control samples were analyzed within a single batch under identical reaction conditions to eliminate inter-assay variability.
Data analysis was performed using NCSS (Number Cruncher Statistical System) 2007
software (Kaysville, UT, USA). Descriptive statistics were expressed as mean
A total of 73 patients with EC and 76 control subjects were included in the
study. Age (mean
| Variable | EC Patients (n = 73) | Controls (n = 76) | p-value | |
| Mean |
Mean |
|||
| Age (years) | 57.84 |
55.44 |
0.171 (ns) | |
| BMI (kg/m2) | 33.20 |
33.75 |
0.563 (ns) | |
| n (%) | n (%) | |||
| Obesity | 0.841 (ns) | |||
| Non-obese (BMI |
21 (28.8) | 23 (30.3) | ||
| Obese (BMI |
52 (71.2) | 53 (69.7) | ||
| Smoking status | 0.210 (ns) | |||
| Non-smoker | 54 (74.0) | 49 (64.5) | ||
| Smoker | 19 (26.0) | 27 (35.5) | ||
| Hypertension | 0.124 (ns) | |||
| No | 37 (50.7) | 48 (63.2) | ||
| Yes | 36 (49.3) | 28 (36.8) | ||
| Diabetes mellitus | 0.099 (ns) | |||
| No | 50 (68.5) | 61 (80.3) | ||
| Yes | 23 (31.5) | 15 (19.7) | ||
Data are presented as mean
p
Among patients with EC (n = 73), preoperative serum CA-125 levels ranged from 5
to 745 U/mL (mean
Myometrial invasion was
Regarding surgical management, 9 patients (12.3%) underwent no LN dissection
(LND), 14 (19.2%) had pelvic–paraaortic LND, 50 (68.5%) had pelvic or sentinel
LND, and 31 (42.5%) underwent omental sampling or omentectomy. Among surgically
staged patients, LN counts ranged from 0 to 51 (mean
Recurrence data were available for 71 of the 73 patients; two patients were excluded from recurrence analysis due to incomplete follow-up. Among the evaluable cohort, recurrence was identified in 9 patients (12.7%) based on radiological or histopathological confirmation—managed with CT in 5 cases, surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) plus CT in 1, and combined CT and RT in 3.
Serum lncRNA HOTAIRM1 expression levels were significantly higher in EC patients compared to controls (median [IQR]: 1.36 [0.74–3.37] vs. 1.03 [0.58–2.03]; p = 0.043) (Fig. 1 and Table 2). In contrast, serum miR-182-5p expression levels did not differ significantly between groups (1.26 [0.09–4.39] vs. 1.71 [0.21–3.58]; p = 0.327) (Fig. 2 and Table 2).
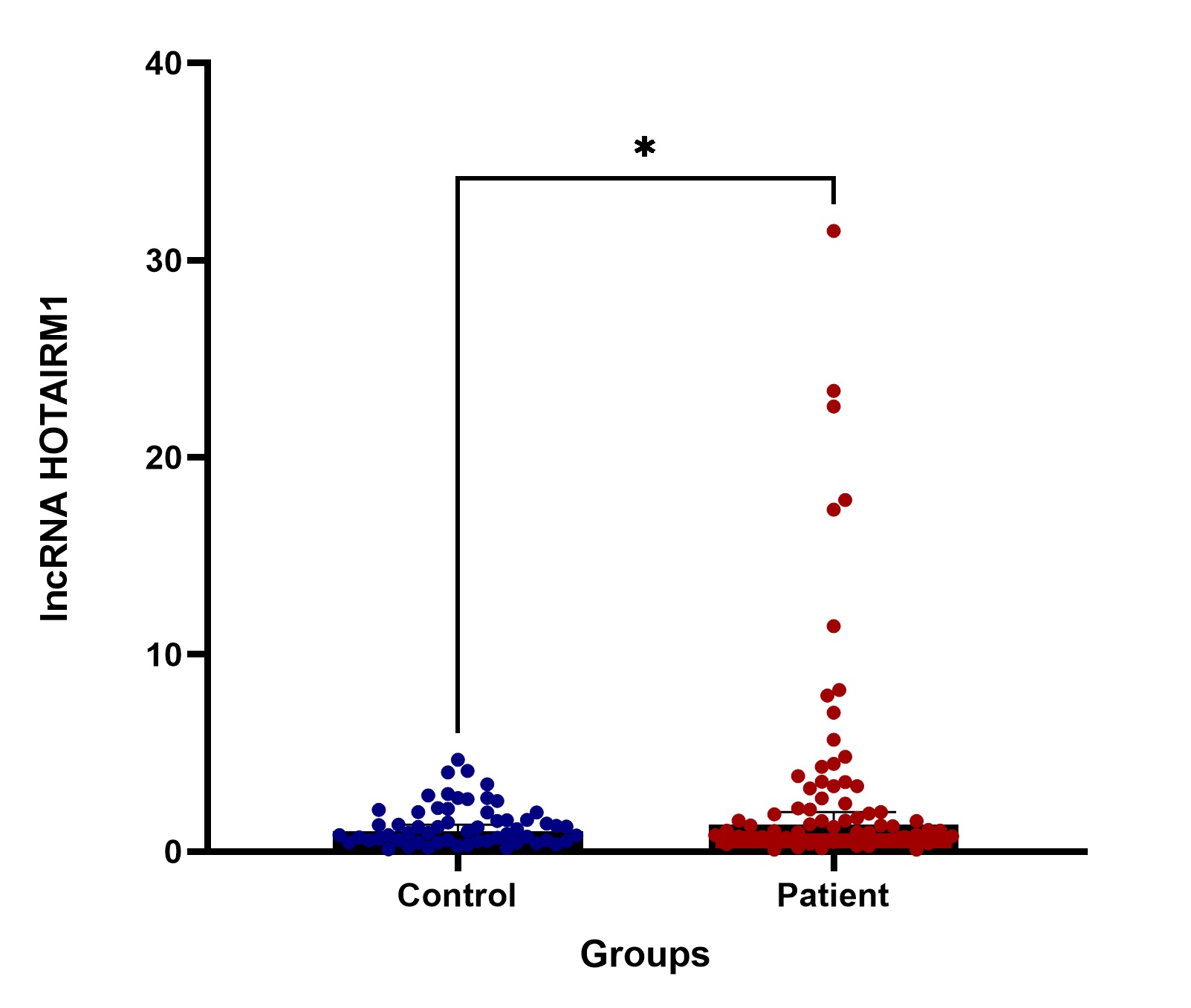 Fig. 1.
Fig. 1.
Comparison of serum lncRNA HOTAIRM1 expression between EC
patients and controls. * indicates statistical significance, defined as p
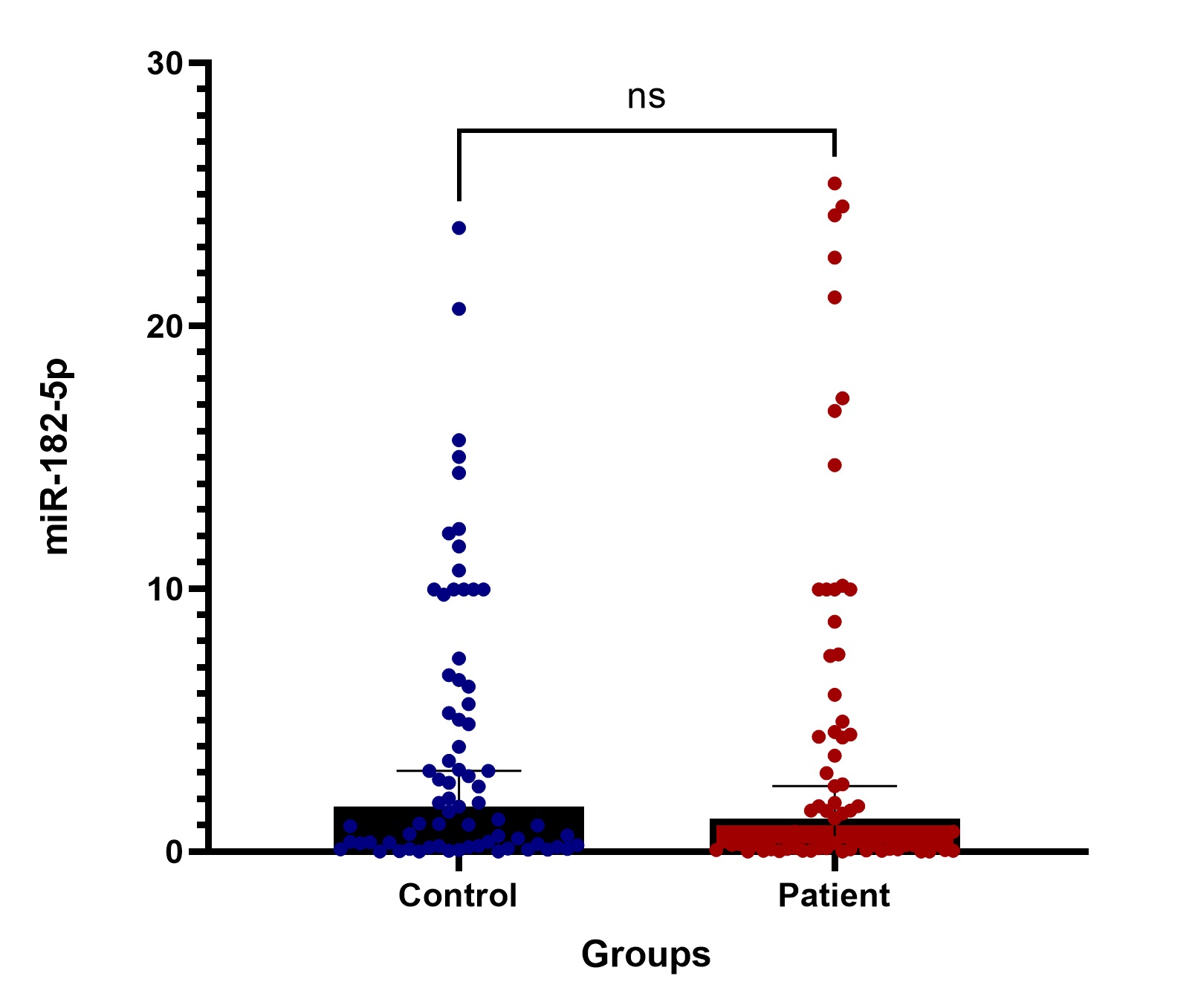 Fig. 2.
Fig. 2.
Comparison of serum miR-182-5p expression between EC patients and controls. ns denotes not statistically significant.
| Biomarker | Group | Median (IQR) | p-value |
| lncRNA HOTAIRM1 | Control | 1.03 (0.58–2.03) | 0.043* |
| lncRNA HOTAIRM1 | Patient | 1.36 (0.74–3.37) | |
| miR-182-5p | Control | 1.71 (0.21–3.58) | 0.327 |
| miR-182-5p | Patient | 1.26 (0.09–4.39) |
Values are presented as median (IQR). Statistical analyses were performed using the Mann-Whitney U test.
p
Spearman’s correlation analysis demonstrated no significant relationship between
serum lncRNA HOTAIRM1 and miR-182-5p expression in the EC groups (p
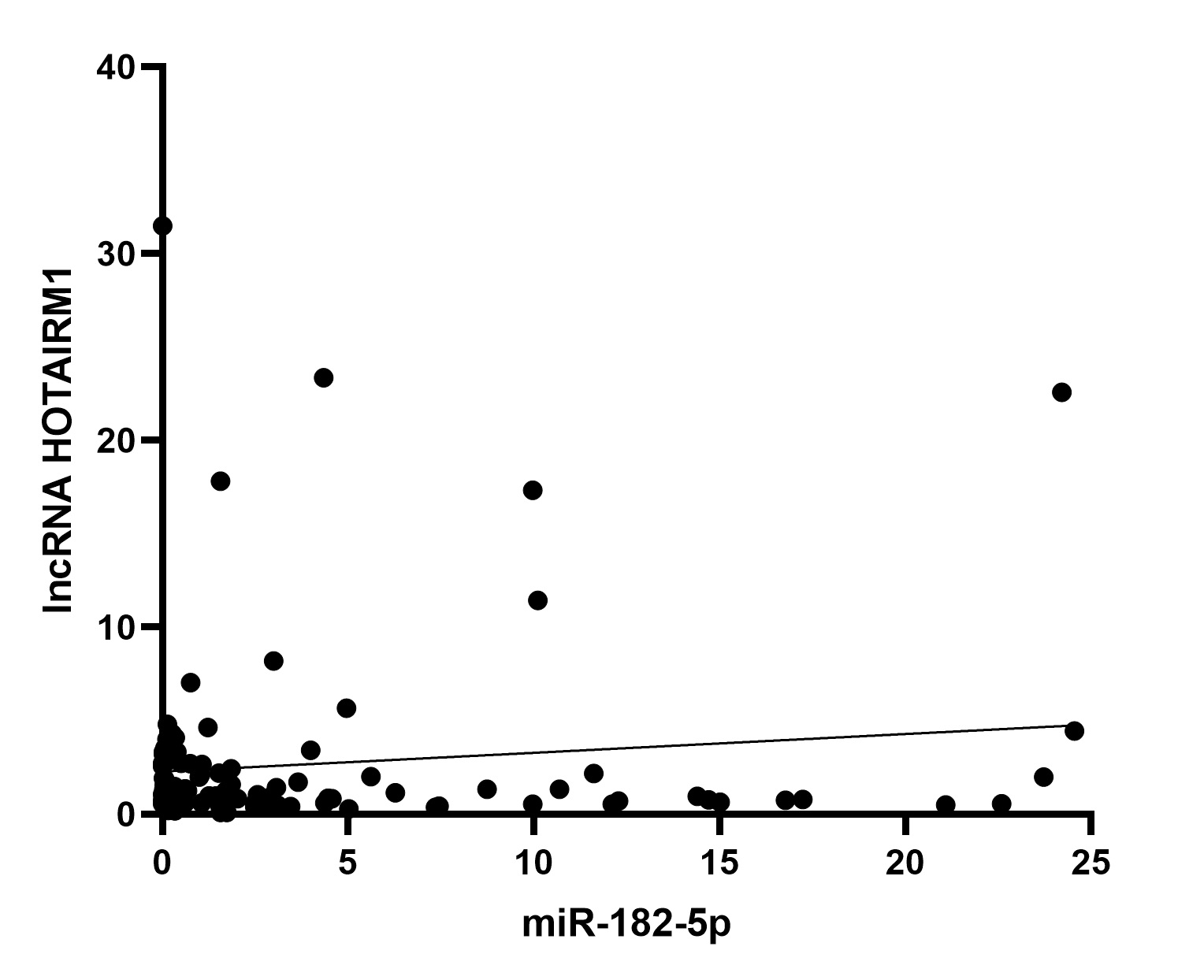 Fig. 3.
Fig. 3.
Correlation between serum lncRNA HOTAIRM1 and miR-182-5p expression in patients with EC.
ROC curve analysis demonstrated that serum lncRNA HOTAIRM1 had an area under the curve (AUC) of 0.606 (95% CI: 0.507–0.706; p = 0.037), indicating a statistically significant yet modest discriminative ability to distinguish EC patients from controls (Fig. 4 and Table 3). The optimal diagnostic cut-off value was 3.06, corresponding to 29.6% sensitivity and 93.2% specificity (Table 3). These findings indicate that, although serum lncRNA HOTAIRM1 has high specificity—reflecting a strong capacity to correctly identify non-EC cases—its low sensitivity limits its ability to detect all true positives. Therefore, serum lncRNA HOTAIRM1 alone may not be sufficient as a screening biomarker; however, its high specificity supports its potential utility as a confirmatory diagnostic or prognostic adjunct when used in combination with other molecular or clinicopathological parameters.
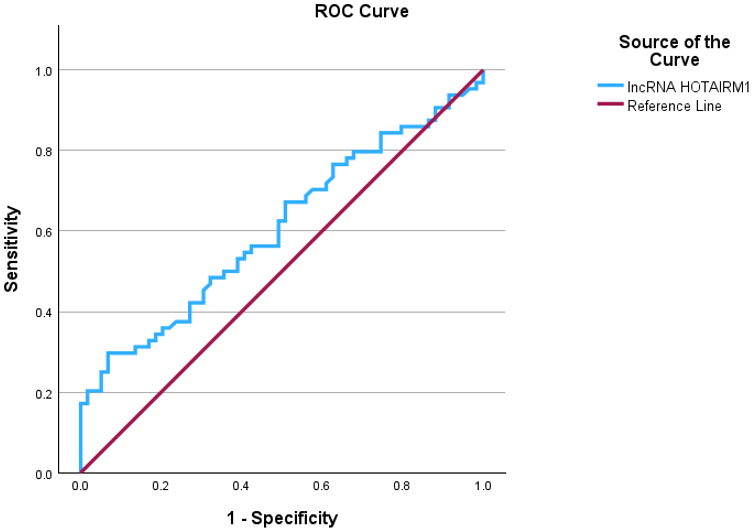 Fig. 4.
Fig. 4.
ROC curve of serum lncRNA HOTAIRM1 for the diagnosis of EC. ROC, receiver operating characteristic.
| Parameter | Sensitivity (%) | Specificity (%) | Cut-off value | AUC (95% CI) | p-value |
| lncRNA HOTAIRM1 | 29.6 | 93.2 | 3.06 | 0.606 (0.507–0.706) | 0.037* |
AUC, area under the ROC curve.
p
Overall survival (OS) was defined as the interval from diagnosis to death from
any cause, and disease-free survival (DFS) was defined as the interval from
surgery to disease progression or recurrence. In the study cohort, the follow-up
duration for DFS ranged from 0 to 75 months (mean
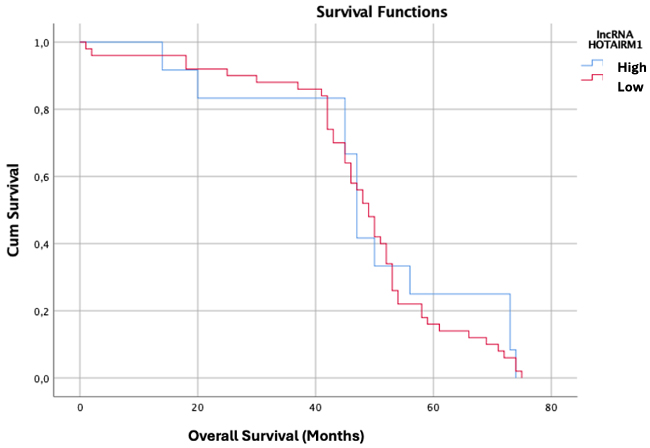 Fig. 5.
Fig. 5.
Kaplan-Meier survival analysis of serum lncRNA HOTAIRM1 expression in EC.
Subgroup analyses were performed to examine potential associations between serum lncRNA HOTAIRM1 and miR-182-5p expression levels and key clinicopathological parameters, including FIGO stage, tumor grade, recurrence status, disease-related mortality, LN involvement, deep myometrial invasion, LVSI, MELF pattern, cervical stromal or isthmic involvement, and distant metastasis.
When stratified by FIGO stage, no significant differences in serum lncRNA HOTAIRM1 or miR-182-5p expression were observed between early-stage (IA–IB; n = 58) and advanced-stage (II–IV; n = 15) groups (p = 0.968 and p = 0.180, respectively). Similarly, when categorized by tumor grade, expression levels did not differ significantly between low-grade (grades 1–2 endometrioid; n = 58) and high-grade (grade 3 endometrioid or non-endometrioid; n = 15) tumors (lncRNA HOTAIRM1: median [IQR] 1.32 [0.74–3.44] vs. 2.01 [0.71–3.70]; miR-182-5p: 0.76 [0.09–4.36] vs. 1.64 [0.13–5.87]; p = 0.606 and p = 0.728, respectively).
Although median miR-182-5p levels were higher in patients with advanced-stage disease (2.99 [0.17–19.12] vs. 0.76 [0.09–3.82]), LN involvement (4.46 [0.03–23.40] vs. 1.01 [0.10–3.99]), and recurrence (1.55 [0.39–4.46] vs. 0.75 [0.09–4.34]), these differences were not statistically significant (p = 0.180, p = 0.616, and p = 0.595, respectively). Similarly, lncRNA HOTAIRM1 expression showed a non-significant increase in patients with recurrence (3.44 [0.85–7.04] vs. 1.28 [0.73–2.83]; p = 0.087).
Additional subgroup analyses, including disease-related mortality, deep myometrial invasion, LVSI, MELF pattern, cervical stromal or isthmic involvement, and distant metastasis, also revealed no statistically significant differences in serum lncRNA HOTAIRM1 or miR-182-5p expression levels.
Overall, serum lncRNA HOTAIRM1 and miR-182-5p expression levels showed variability across clinical and pathological subgroups; however, none of the observed differences reached statistical significance. Given the limited sample sizes within certain subgroups and the absence of confidence interval calculation due to small subgroup counts, these findings should be interpreted with caution. Taken together, the results suggest that although these biomarkers may hold potential clinical relevance, their current utility in predicting disease progression, recurrence, or prognosis in EC remains limited. Detailed subgroup data for serum lncRNA HOTAIRM1 and miR-182-5p expression are presented in Tables 4A and 4B.
| Clinicopathological parameter | Group | n | Median (IQR) | p-value |
| FIGO stage | Early stage (IA–IB) | 58 | 1.47 (0.73–3.33) | 0.968 |
| Advanced stage (II–IV) | 15 | 1.30 (0.77–4.23) | ||
| Tumor grade | Low grade (G1–2) | 58 | 1.32 (0.74–3.44) | 0.606 |
| High grade (G3/non-endometrioid) | 15 | 2.01 (0.71–3.70) | ||
| LN involvement | Negative | 66 | 1.39 (0.74–3.33) | 0.880 |
| Positive | 7 | 1.07 (0.70–13.06) | ||
| Recurrence | Absent | 62 | 1.28 (0.73–2.83) | 0.087 |
| Present | 9 | 3.44 (0.85–7.04) |
Values are presented as median (IQR). Statistical analyses were performed using
the Mann-Whitney U test. p
Note. n = 71 for recurrence analysis (two patients excluded due to incomplete follow-up; recurrence status missing). FIGO, The International Federation of Gynecology and Obstetrics; LN, lymph node.
| Clinicopathological parameter | Group | n | Median (IQR) | p-value |
| FIGO stage | Early stage (IA–IB) | 58 | 0.76 (0.09–3.82) | 0.180 |
| Advanced stage (II–IV) | 15 | 2.99 (0.17–19.12) | ||
| Tumor grade | Low grade (G1–2) | 58 | 0.76 (0.09–4.36) | 0.728 |
| High grade (G3/non-endometrioid) | 15 | 1.64 (0.13–5.87) | ||
| LN involvement | Negative | 66 | 1.01 (0.10–3.99) | 0.616 |
| Positive | 7 | 4.46 (0.03–23.40) | ||
| Recurrence | Absent | 62 | 0.75 (0.09–4.34) | 0.595 |
| Present | 9 | 1.55 (0.39–4.46) |
Values are presented as median (IQR). Statistical analyses were performed using
the Mann-Whitney U test. p
Note. n = 71 for recurrence analysis (two patients excluded due to incomplete follow-up; recurrence status missing).
EC is primarily diagnosed through histopathological evaluation of biopsy specimens, and no non-invasive biomarkers are currently implemented in clinical practice. The rising incidence and mortality of EC underscore the need to better elucidate its underlying molecular mechanisms. Increasing evidence indicates that lncRNAs and miRNAs are dysregulated in EC and may serve as promising diagnostic and prognostic biomarkers with potential roles in predicting disease progression, LN involvement, metastasis, treatment response, and diverse pathological or molecular features. Moreover, ncRNAs may represent novel therapeutic targets in EC.
ncRNAs can be detected not only in tissues but also in biological fluids such as serum, plasma, and urine, where expression levels differ between healthy individuals and cancer patients. Although tissue-based analyses often yield distinct expression profiles, the optimal biological source for reliable EC biomarkers remains unclear. Circulating ncRNAs are particularly attractive because of their accessibility and the advantages of non-invasive sampling. Previous tissue-based studies have consistently demonstrated upregulation of both lncRNA HOTAIRM1 and miR-182-5p in EC, supporting their potential oncogenic role at the tissue level [17, 21, 26]. However, their circulating expression patterns remain poorly defined and have not been systematically explored. In this study, we evaluated serum levels of lncRNA HOTAIRM1 and miR-182-5p using qRT-PCR, as these molecules have been previously studied in EC tissues but remain largely unexplored in circulation.
In a systematic review, Donkers et al. [21] analyzed 26 studies including 2110 women (1400 with EC) that assessed miRNA expression across tissue, serum, plasma, urine, and liquid-based cytology samples. Some studies did not stratify patients by subtype, whereas others conducted subgroup analyses or focused on type 1 and type 2 EC. A total of 106 miRNAs were investigated, with notable variability in expression profiles. Importantly, miR-182-5p expression in EC was assessed in only one study analyzing both tissue and liquid-based cytology samples [21]. Kottaridi et al. [26] further demonstrated significantly elevated miR-182-5p expression, with a 27.3-fold increase in tissue, an 18.2-fold increase in liquid-based cytology, and a 22.7-fold overall increase in EC patients. Mechanistically, miR-182-5p is implicated in the regulation of the Wnt signaling pathway, which is essential for endometrial proliferation and differentiation; its dysregulation contributes to endometrial hyperplasia [27, 28]. Specifically, downregulation of Wnt5a and Smad4 has been observed in EC tissues, and miR-182-5p may target both genes, thereby disrupting Wnt signaling and promoting disease progression [28, 29, 30, 31]. Moreover, miRNA expression profiles differ across EC subtypes. Ratner et al. [32] identified subtype-specific miRNAs in endometrioid, serous, and carcinosarcoma subtypes, supporting the concept that EC exhibits distinct molecular behaviors. Additional studies have also suggested that certain miRNAs may predict LN involvement or LVSI, further underscoring their potential clinical relevance [33, 34].
In our study, we evaluated the diagnostic potential of miR-182-5p, which has been only minimally explored in EC. Although prior studies indicated elevated expression, our analysis revealed no significant differences in serum levels between patients and controls. These findings suggest that, while miR-182-5p may exert oncogenic effects within tumor tissue, its circulating levels have limited diagnostic value. Nonetheless, the trend toward higher expression in more aggressive disease warrants further investigation in larger cohorts.
Li et al. [17] demonstrated in tissue samples from 50 patients with type 1 EC that lncRNA HOTAIRM1 acts as an oncogene by regulating HOXA1, thereby promoting cell proliferation, migration, invasion, and epithelial–mesenchymal transition (EMT). Both HOTAIRM1 and HOXA1 were significantly upregulated and correlated with FIGO stage and LN involvement [17]. These findings suggest that the HOTAIRM1/HOXA1 axis plays a critical role in the initiation and progression of type 1 EC and may serve as both a prognostic biomarker and a therapeutic target [17].
In the present study, we demonstrated for the first time that serum lncRNA HOTAIRM1 expression levels were significantly elevated in EC patients compared with controls. While previous studies have focused primarily on tissue-based analyses, our findings provide novel evidence supporting its upregulation in serum, suggesting that serum lncRNA HOTAIRM1 may represent a promising non-invasive biomarker for EC. ROC curve analysis demonstrated high specificity but limited sensitivity, implying a strong positive predictive value but insufficient performance as a standalone diagnostic tool due to potential false negatives.
When compared with well-established serum biomarkers, cancer antigen 125 (CA125) and human epididymis protein 4 (HE4), our findings provide perspective on the relative diagnostic value of lncRNA HOTAIRM1. Both CA125 and HE4 are widely recognized markers in EC, consistently elevated in affected patients compared with healthy controls. Barr et al. [35] reported that the combination of CA125 and HE4 achieved an AUC of 0.77 (95% CI: 0.74–0.81) for EC detection, while HE4 alone demonstrated excellent diagnostic accuracy in premenopausal women (AUC = 0.91, sensitivity 84.5%, specificity 80.9%). Similarly, Bian et al. [36] found that HE4 outperformed CA125, CA19-9, and CA724 (AUC = 0.76, sensitivity 58%), and that combined testing (HE4 + CA125 + CA19-9 + CA724) improved discrimination (AUC = 0.82, sensitivity 59.1%, PPV 88%). These findings highlight HE4, particularly in combination with CA125, as a robust non-invasive biomarker correlated with advanced FIGO stage, deep myometrial invasion, and LVSI or LN involvement [35, 36]. Compared with these validated markers, serum lncRNA HOTAIRM1 in our study exhibited comparable specificity but lower sensitivity, indicating limited diagnostic strength at this stage. While lncRNA HOTAIRM1 may reflect underlying tumor biology and hold potential for future biomarker development, its current clinical applicability remains preliminary and warrants confirmation through larger, multicenter investigations.
The molecular pathogenesis of EC has gained increasing attention, as an improved understanding of ncRNA expression may enhance risk stratification and disease classification. Conventional histopathological criteria alone are often insufficient to predict recurrence risk, leading to potential over- or under-treatment. This underscores the need for reliable molecular biomarkers to refine therapeutic decision-making.
In this study, subgroup analyses were performed to evaluate associations between
serum lncRNA HOTAIRM1 and miR-182-5p expression levels and clinicopathological
parameters. Although higher miR-182-5p levels were observed in patients with
advanced-stage disease, LN involvement, or recurrence, and increased lncRNA
HOTAIRM1 expression was noted in patients with recurrence, these differences were
not statistically significant (p
Molecular subtype data (POLEmut, dMMR, p53abn, NSMP classification) were unavailable for this cohort, as such, analyses were not routinely performed during the study period. Therefore, stratified evaluation of circulating lncRNA HOTAIRM1 across molecular subtypes could not be conducted. Future studies incorporating molecularly characterized cohorts are warranted to determine whether serum lncRNA HOTAIRM1 expression differs across EC subgroups, given the prognostic and therapeutic implications of molecular classification.
lncRNAs and miRNAs can act as oncogenes or tumor suppressors, and their
dysregulation contributes to cancer initiation and progression. miRNAs regulate
tumorigenesis by binding to target mRNAs and suppressing translation, while
certain lncRNAs modulate miRNA function through competing endogenous mechanisms.
Increasing evidence supports complex lncRNA–miRNA–mRNA networks shaping
oncogenic pathways. For example, Sweef et al. [37] described the
HOTAIRM1/miR-182-5p/ERO1A axis in lung cancer, where upregulation of HOTAIRM1 and
ERO1A with concurrent miR-182-5p downregulation was associated with poor
survival. In EC, independent studies have also reported increased lncRNA HOTAIRM1
and miR-182-5p expression in tumor tissue [17, 21, 26]. Consistent with these
reports, we hypothesized a possible HOTAIRM1/miR-182-5p interaction in EC;
however, our correlation analysis found no significant association between their
serum levels (p
Taken together, these findings suggest that although circulating lncRNA HOTAIRM1 and miR-182-5p may reflect molecular alterations seen in EC tissues, their serum expression patterns show limited diagnostic and prognostic utility, suggesting that further exploration of these biomarkers should await stronger preliminary evidence.
This study has several limitations that should be acknowledged. First, the sample size was relatively small and derived from a single institution, which may restrict the generalizability of the results. Second, despite standardized sample handling, potential pre-analytical variations—such as storage duration, RNA stability, or variability in internal reference gene expression—might have influenced measured expression levels. Although U6 and GAPDH were selected as internal controls based on prior validation in serum-based ncRNA studies and demonstrated consistent amplification efficiency in our dataset, cohort-specific stability testing was not performed. Third, external validation in an independent cohort and functional in vitro assays were beyond the scope of this investigation. Lastly, although the control group consisted of women with non-malignant gynecological conditions and no uterine or adnexal pathology, they may not fully represent healthy individuals, introducing minimal background variability.
This study demonstrated that serum lncRNA HOTAIRM1 is significantly elevated in patients with EC compared with controls, whereas serum miR-182-5p showed no diagnostic or prognostic value. Although lncRNA HOTAIRM1 exhibited relatively high specificity, its low sensitivity and lack of consistent association with clinicopathological parameters limit its clinical applicability. Importantly, this work represents one of the first investigations assessing the circulating expression of lncRNA HOTAIRM1 and miR-182-5p in EC, suggesting their potential as non-invasive biomarkers. While the findings provide valuable preliminary data supporting the exploration of circulating ncRNAs in EC, the current evidence indicates insufficient diagnostic or prognostic power to support clinical implementation. Further validation in larger, well-designed multicenter studies using standardized methodologies is required to confirm the diagnostic and prognostic potential of these biomarkers and to clarify their biological significance.
The data supporting the findings of this study are available from the corresponding author upon reasonable request. These data are not publicly accessible due to privacy and ethical considerations regarding participant confidentiality.
HEU contributed to the conceptualization, methodology development, data collection and formal analysis. YM contributed to methodology development and supervised the study. CK and AFA were responsible for data curation and assisted in methodology development. HS and MYS contributed to study design, coordination of data acquisition, and interpretation of the data. MAE and AMA performed data analysis. ST contributed to study conception, supervised data acquisition and management and participated in the interpretation of the results. All authors contributed to the critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study protocol was reviewed and approved by the Institutional Review Board and Ethics Committee of Istanbul University (Initial Approval No: 2018/1609; Additional Approval No: 2023/119). All procedures were conducted in accordance with the ethical standards of the institutional and national research committees and with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to inclusion in the study, covering both immediate participation and future use of stored biospecimens.
We gratefully acknowledge the Istanbul University Scientific Research Projects Unit for their generous funding and essential support in facilitating this study. We also thank the anonymous peer reviewers for their constructive feedback, which significantly improved the manuscript.
This study was supported by the Istanbul University Scientific Research Projects Unit (Project ID: TTU-2023-39847). No additional financial support was received from public, commercial, or not-for-profit funding agencies.
The authors declare no conflict of interest.
During the preparation of this work the authors used ChatGPT-5 in order to check spell and grammar. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.