




1 Department of Obstetrics, Women and Children’s Hospital of Ningbo University, 315012 Ningbo, Zhejiang, China
†These authors contributed equally.
Abstract
Cesarean section (CS) is a key obstetric surgery, postoperative wound, uterine incision, and pelvic infections are relatively common, so clinicians must pay close attention to the prevention and early detection of surgical site infections. To investigate the risk factors and management strategies for severe uterine incision infections with pelvic abscesses following CS.
We conducted a retrospective study of CS cases performed at our hospital from January 2018 to December 2023. The observation group included 27 patients who developed severe uterine incision infections and pelvic abscesses postoperatively. Each case was matched with 3 controls (total number = 108) who did not develop these complications, selected from the same source population during the study period.
Univariate logistic regression analysis demonstrated a statistically significant difference in the incidence of chorioamnionitis, premature rupture of membranes, and preterm delivery between the two groups (p < 0.05). Multivariate stepwise logistic regression further identified preterm delivery (odds ratio [OR] = 4.084, 95% confidence interval [CI] = 1.261–13.224) and chorioamnionitis (OR = 4.388, 95% CI = 1.370–14.058) as independent risk factors for severe pelvic abscess.
Chorioamnionitis and preterm delivery are independent risk factors for severe uterine incision infection with pelvic abscess following CS, underscoring the need for heightened perioperative vigilance and targeted preventive strategies in at-risk patients.
Keywords
- uterine incision infection
- cesarean section
- pelvic abscess
- pelvic infection
- risk factors.
Cesarean section (CS) is an important surgical intervention in obstetrics [1]. Due to the special timing of the procedure, amniotic fluid and blood from the uterine cavity may directly overflow into the abdominal cavity and the abdominal wall incision during surgery [2]. Postoperative wound infection is a common postoperative complication after CS in both developed and developing countries [3]. If other clinical factors exist at the same time, uterine incision infection and pelvic infection become more likely [4]. Therefore, prevention and timely detection of surgical site infection of the uterine incision and pelvis are issues that clinicians must be vigilant about [5]. In this study, we retrospectively analyzed 27 cases of severe uterine incision infection and severe pelvic infection that occurred after CS in the Women and Children’s Hospital of Ningbo University and aimed to investigate the risk factors and management strategies for severe uterine incision infection and pelvic abscess following CS.
This retrospective study recruited patients from January 2018 to December 2023 at Women and Children’s Hospital of Ningbo University. This study adhered to the principles outlined in the Declaration of Helsinki and obtained approval from the Ethics Committee of Women and Children’s Hospital of Ningbo University (approval number: NBFE-2025-KY-149). The requirement for written informed consent was waived by the committee due to the retrospective nature of the study and all data were analyzed anonymously.
In this study, ‘severe uterine incision infection’ was diagnosed as an organ/space surgical site infection (SSI) following CS, based on the United States of America (USA) Centers for Disease Control (CDC) and Prevention criteria. [1, 2]. The diagnosis required the infection to occur within 30 days post-surgery and met at least one of the following conditions: (1) Purulent drainage from the uterine incision site or pelvic cavity obtained via puncture or drainage; (2) Isolation of microorganisms from aseptically collected fluid or tissue cultures from the pelvic cavity; (3) Evidence of an abscess or infection at the uterine incision site or in the pelvic cavity confirmed by direct examination, reoperation, histopathology, or radiological imaging (e.g., ultrasound or computed tomography (CT)); (4) A diagnosis of organ/space SSI made by the attending surgeon or physician.
Exclusion criteria:
(1) Pre-existing non-genital tract infections (such as pneumonia);
(2) Incomplete medical records.
All patients were delivered by CS and relevant information was
retrospectively collected. A total of 27 women experienced the complication of
severe pelvic infection after CS and formed the observation group
with 81 CS cases with uneventful postoperative courses during the
same period making up the control group, with no incision infection in the
latter. Controls were matched to cases at a 1:3 ratio based on age (
Based on literature review, potential risk factors were identified, including
age of mother, body mass index (BMI), gravidity, parity, abortion, previous
cesarean section, preterm birth (
(1) Conservative treatment consisted of the standard management of pelvic abscess according to both domestic and international authoritative guidelines, including the Chinese “Guidelines for the Diagnosis and Treatment of Pelvic Inflammatory Disease (2019 revised edition)” [7].
(2) Surgical treatment for cases where conservative measures failed mainly involved debridement and drainage of the infected tissues. For pelvic abscess, drainage was performed via the posterior fornix of the vagina or through an abdominal incision.
Statistical analyses were performed using SPSS for Windows, Version 20.0
(Armonk, NY, USA: IBM Corp.). The normality of continuous variables was assessed
using the Shapiro-Wilk test. Normally distributed data are presented as mean
During the study period, a total of 11,671 pregnant patients underwent CS, of whom 0.231% (27/11,671) were diagnosed with severe uterine incision infection (Fig. 1).
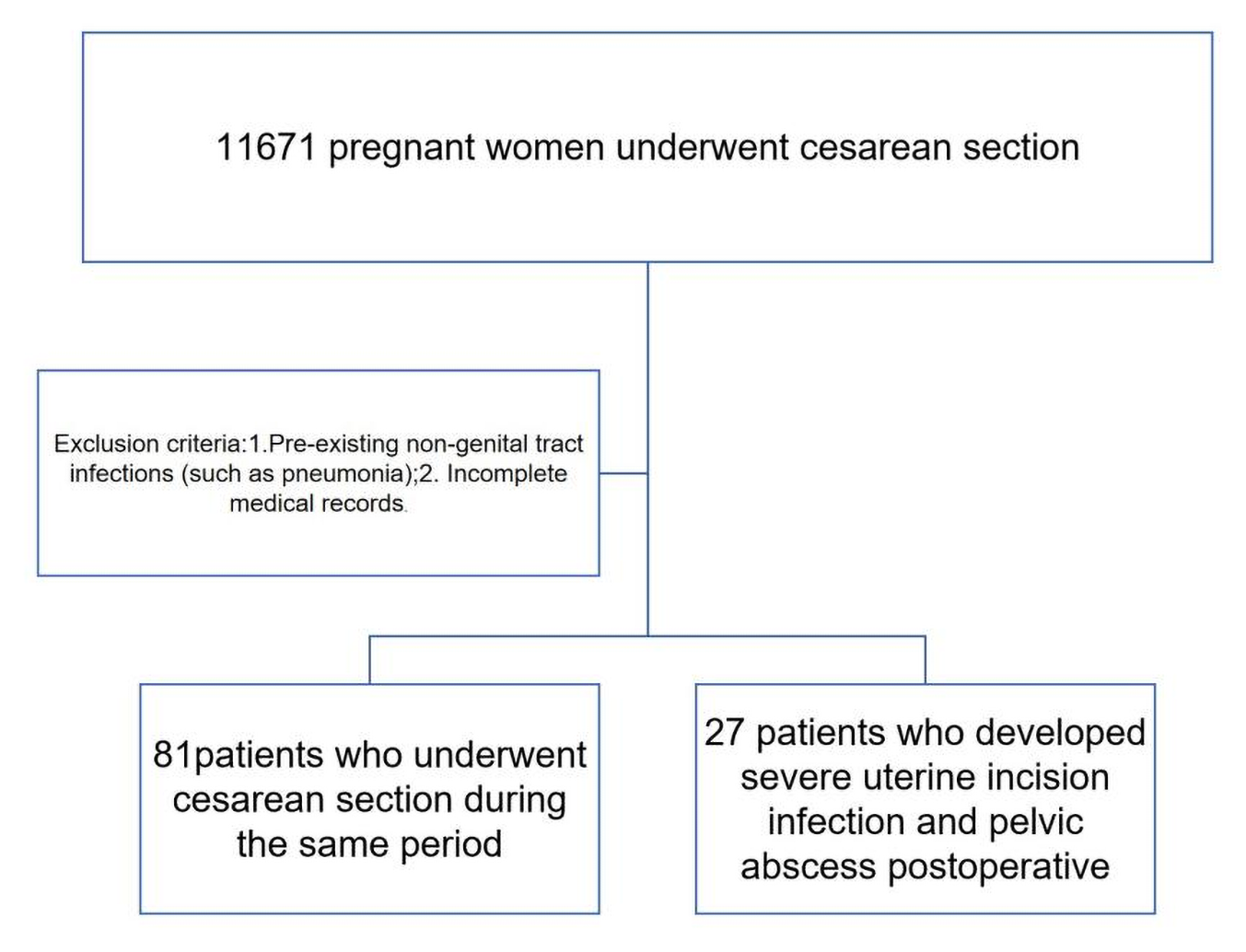 Fig. 1.
Fig. 1.
Flow diagram of patient selection.
Table 1 presents the demographic and clinical characteristics of all study participants.
| Clinical parameters | Control patients (n = 81) | Case patients (n = 27) | p value | |
| Age of mother (years) | 30.4 |
28.8 |
0.145 | |
| BMI (kg/m2) | 26.5 |
27.4 |
0.274 | |
| Gravidity, n (%) | 0.088 | |||
| 51 (63.0%) | 19 (70.4%) | |||
| 3–4 | 25 (30.9%) | 6 (22.2%) | ||
| 5 (6.1%) | 2 (7.4%) | |||
| Parity, n (%) | 0.677 | |||
| 57 (70.4%) | 21 (77.8%) | |||
| 24 (29.6%) | 6 (22.2%) | |||
| Abortion, n (%) | 0.652 | |||
| 72 (88.9%) | 22 (81.5%) | |||
| 9 (11.1%) | 5 (18.5%) | |||
| Previous cesarean section, n (%) | 23 (28.4%) | 10 (37.0%) | 0.370 | |
| Preterm birth ( |
11 (13.6%) | 13 (48.1%) | 0.021 | |
| PROM, n (%) | 8 (9.88%) | 7 (25.9%) | 0.035 | |
| Twin pregnancy, n (%) | 5 (6.2%) | 5 (18.5%) | 0.116 | |
| Hypertensive disorders complicating pregnancy, n (%) | 9 (11.1%) | 4 (14.8%) | 0.609 | |
| GDM, n (%) | 16 (19.8%) | 8 (29.6%) | 0.278 | |
| Placental abruption, n (%) | 12 (14.8%) | 7 (25.9%) | 0.185 | |
| Chorioamnionitis, n (%) | 7 (8.6%) | 10 (37.0%) | 0.001 | |
Data are shown as n (%), mean
There were no statistically significant differences between the 2 groups in
terms of maternal age, body mass index, gravidity, or parity (p
Univariate logistic regression analysis revealed that at the
| Characteristics | Coefficient (β) | ORa | 95% CI | p valuea |
| Age of mother (years) | –0.148 | 0.868 | 0.744–1.008 | 0.314 |
| BMI (kg/m2) | 0.471 | 1.590 | 0.780–3.235 | 0.402 |
| Gravidity, n (%) | –0.562 | 0.561 | 0.330–0.967 | 0.286 |
| Parity, n (%) | –0.112 | 0.891 | 0.241–3.359 | 0.677 |
| Abortion, n (%) | 0.910 | 2.467 | 0.510–11.948 | 0.677 |
| Previous cesarean section, n (%) | –1.451 | 0.239 | 0.048–1.160 | 0.481 |
| Preterm birth ( |
1.931 | 3.582 | 1.022–12.560 | 0.020 |
| PROM, n (%) | –0.379 | 0.704 | 0.100–4.680 | 0.152 |
| Twin pregnancy, n (%) | 1.150 | 0.210 | 0.532–1.602 | 0.302 |
| Hypertensive disorders complicating pregnancy, n (%) | –0.959 | 0.377 | 0.056–2.594 | 0.677 |
| GDM, n (%) | 1.229 | 3.420 | 0.704–16.647 | 0.402 |
| Placental abruption, n (%) | –2.510 | 0.084 | 0.006–1.117 | 0.344 |
| Chorioamnionitis, n (%) | 1.279 | 3.612 | 1.370–12.300 | 0.013 |
| Constant | –6.238 |
ORa, adjusted odds ratio; CI, confidence interval; BMI, body mass index; p valuea, adjusted p value.
A stepwise selection procedure was used for the multivariate logistic
regression, with the entry criterion set at p
| OR | 95% CI | p value | |
| Chorioamnionitis (yes) | 4.388 | 1.370–14.058 | 0.013 |
| Preterm birth ( |
4.084 | 1.261–13.224 | 0.020 |
OR, odds ratio; CI, confidence interval.
Among the 27 cases of severe uterine incision infection and pelvic abscess, all patients were initially managed with antibiotics as conservative treatment, and 20 responded successfully. The remaining 7 required surgery; all of these were complicated by poor healing of the abdominal incision. Five cases improved after the placement of an abdominal cavity drainage tube via the abdominal incision. One patient underwent secondary suturing of the abdominal incision, but continued to have fever postoperatively and recovered after further posterior fornix abscess drainage. Another patient developed a uterine-abdominal wall fistula, and after changing dressings at the abdominal incision and administration of gonadotropin-releasing hormone (GnRH) analogues to suppress ovarian function and menstruation for 2–3 months, hysterosalpingography indicated closure of the uterine fistula.
During the 5-year study period, 11,671 patients underwent CS, among whom 27 (0.231%) developed postoperative pelvic abscess. The results of this study indicated that chorioamnionitis was a significant risk factor for severe uterine incision infection and pelvic abscess (OR = 4.388, 95% CI = 1.370–14.058), which is consistent with the report by Dotters-Katz et al. [8]. Preterm birth (OR = 4.084, 95% CI = 1.261–13.224) was also a risk factor for poor uterine incision healing. Perhaps, in this at risk population, women with chorioamnionitis and preterm birth are somehow predisposed to developing postpartum morbidity secondary to infection.
Clinical chorioamnionitis is a syndrome characterized by maternal and fetal signs of local and systemic inflammation, primarily resulting from intraamniotic infection or sterile intraamniotic inflammation [9, 10]. This study identified chorioamnionitis as a significant risk factor for severe uterine incision infection and pelvic abscess. In general, the normal female vagina possesses innate defense mechanisms against exogenous pathogens [11]. Under normal circumstances, pregnancy and childbirth do not elevate the mother’s risk of infection. Infection occurs when the balance between host immunity and the virulence or burden of pathogens is disrupted. During delivery or surgical procedures, certain pathogens may proliferate excessively, leading to chorioamnionitis and subsequent severe complications such as uterine incision infection and pelvic abscess [12]. According to a study by Dotters-Katz et al. [8], among 213 women with clinical chorioamnionitis who underwent cesarean delivery, 32 (15%) developed surgical site infections [13]. Nevertheless, effective management of clinical chorioamnionitis requires an index of suspicion, timely diagnosis, prompt antibiotic administration, and expedited delivery, all of which are crucial to mitigating potentially severe maternal and neonatal outcomes [14, 15].
This study has demonstrated that preterm birth is primarily caused by infection
(OR = 4.084, 95% CI = 1.261–13.224). Although CS was associated
with improved neonatal outcomes, there was increased short-term maternal
morbidity in this group [16, 17]. Horowitz et al. [18] reported that
maternal morbidity was increased with CS including longer hospital
stay (p
This study has several limitations. First, it is a retrospective study conducted at a single center. Second, the sample size was relatively small, which was particularly evident when subgroup analyses were performed. Third, although known confounding factors were adjusted for using multivariate analysis, some potential and important confounders were not included in the analysis. These factors include, but are not limited to, specific surgical techniques (such as skin-to-skin operative time), the timing of antibiotic prophylaxis, and the assessment and documentation of intraoperative blood loss. These unmeasured factors may have influenced the study outcomes, and therefore, the associations observed could have been affected by these residual confounders. Future studies with larger sample sizes and multicenter, prospective designs are warranted to further validate and refine these findings.
In conclusion, in our study chorioamnionitis and preterm birth are independent risk factors for severe uterine incision infection and pelvic abscess after CS. Therefore, high vigilance, proactive preoperative optimization, and targeted prophylactic antibiotic regimens should be considered for these at risk populations to mitigate postoperative morbidity secondary to infection.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
XLW: Data collection, manuscript writing and data analysis; DML: Data collection, manuscript editing; AEC and XBH: Data collection, analysis and drafting the manuscript; CDZ: Design of the work, the acquisition, analysis, and interpretation of data for the work, and manuscript editing. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work. All the authors reviewed and approved the final version of the manuscript.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethnic Committee of the Women and Children’s Hospital of Ningbo University (approval number: NBFE-2025-KY-149). All of the participants provided written informed consent.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This study was supported by Medical Science and Technology Project of Zhejiang Province, China (2024KY1574) and funded by the project of Ningbo Leading Medical & Health Discipline (2010-S04 and 2023Z183).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.