





 , Kaihe Lin 1, Feijian Wu 1, Binlin Ruan 1,2, Jingjing Xie 1, Suying Wu 1
, Kaihe Lin 1, Feijian Wu 1, Binlin Ruan 1,2, Jingjing Xie 1, Suying Wu 11 Department of Radiology, The First Hospital of Putian City, 351100 Putian, Fujian, China
2 Department of Nuclear Medicine, The First Hospital of Putian City, 351100 Putian, Fujian, China
Abstract
Multiparametric magnetic resonance imaging (mpMRI), including dynamic contrast-enhanced (DCE) imaging, can assess deep myometrial invasion (DMI) and cervical stromal invasion (CSI) in endometrial cancer (EC). However, the need for gadolinium injection increases potential risks. Thus, whether comparable diagnostic performance can be achieved without gadolinium becomes a critical clinical question.
We retrospectively analyzed 138 patients with EC from the first hospital of Putian City. T2-weighted imaging (T2WI) was combined with diffusion-weighted imaging (DWI) and DCE to form the T2&DWI and T2&DCE groups, respectively. Two senior radiologists independently evaluated each image set according to standardized criteria and were blinded to the pathology. A case was categorized as positive if either DMI or CSI was identified on any sequence within the image set. A more senior radiologist resolved any discrepancies. Two additional combinations were formed to generate a high-sensitivity group and a high-specificity group for secondary analysis. The diagnostic performance of the four image sets was evaluated using postoperative pathology as the reference standard.
Among all cases, 31 had DMI, and 12 had CSI. Agreement between the two readers for the same sequence combination and between sequence combinations for the same reader was high. For DMI, the sensitivity, specificity, accuracy, and receiver operating characteristic (ROC) analysis for the area under curve (AUC) were as follows: T2&DWI group, 0.806, 0.935, 0.906, and 0.871; T2&DCE group, 0.710, 0.935, 0.884, and 0.822; high-sensitivity group, 0.839, 0.916, 0.899, and 0.877; high-specificity group, 0.774, 0.944, 0.906, and 0.811. For CSI, the corresponding results were: T2&DWI group, 0.833, 0.984, 0.971, and 0.909; T2&DCE group, 0.917, 0.984, 0.978, and 0.950; high-sensitivity group, 0.917, 0.976, 0.971, and 0.946; high-specificity group, 0.833, 0.992, 0.978, and 0.913. DeLong’s pairwise comparisons showed no statistically significant differences (p > 0.05), with the Holm correction for multiple comparisons yielding consistent results. The McNemar test for paired comparisons among the four sequence combinations also revealed no significant differences between the groups.
The T2&DWI group demonstrated diagnostic performance comparable to that of the other groups to evaluate DMI and CSI, with no statistically significant differences, suggesting it may serve as a non-contrast alternative to mpMRI with DCE in specific clinical settings.
Keywords
- endometrial cancer
- diffusion-weighted imaging
- deep myometrial invasion
- cervical stromal invasion
- non-enhanced MRI
Endometrial cancer (EC) is one of the most common malignancies of the female reproductive system, and its incidence continues to rise globally, particularly in high-income countries [1]. According to statistics from the American Cancer Society, approximately 69,120 new cases and 13,860 related deaths are expected in the United States in 2025 [2]. EC has become a significant threat to women’s health worldwide, reducing quality of life and placing a considerable burden on healthcare systems.
In recent years, advances in imaging technology have made imaging evaluation pivotal in determining treatment strategies for EC. Multiparametric magnetic resonance imaging (mpMRI) enables comprehensive assessment of tumor characteristics, depth, and extent, including evaluation of deep myometrial invasion (DMI) and cervical stromal invasion (CSI) [3, 4]. mpMRI is increasingly recognized by gynecologists and has become a routine pre-treatment examination.
Previous study has demonstrated that different sequences, such as T2-weighted imaging (T2WI), diffusion-weighted imaging (DWI), and dynamic contrast-enhanced MRI (DCE-MRI), vary in their diagnostic efficacy for detecting tumors, as well as assessing DMI and CSI [5]. The current consensus on routine scanning protocols for EC includes T2WI, T1WI, DWI, and DCE-MRI sequences. Although this comprehensive protocol provides detailed information, the use of contrast agents prolongs scan time, increases examination costs, and adds to the burden on patients and healthcare systems. Moreover, gadolinium-based contrast agents may lead to adverse reactions in certain patients, such as nephrogenic systemic fibrosis, deposition of free gadolinium ions in tissues, and allergic responses (including anaphylactic shock), and in sporadic cases, can even result in a persistent vegetative state or fatality. The long-term clinical implications of gadolinium deposition remain uncertain [6]. Nevertheless, DCE-MRI is still widely performed in daily clinical practice.
The 2019 European Society of Urogenital Radiology (ESUR) guidelines note that whether the combination of T2WI and DWI is superior to DCE-MRI remains uncertain [7]. Therefore, identifying a method that relies solely on non-contrast sequences (e.g., T2WI and DWI) while maintaining diagnostic efficacy is clinically important.
In this study, we performed a retrospective analysis to maximize efficiency and reduce costs by using existing data, while enabling comparison across a relatively large sample size [8]. By evaluating different mpMRI sequence combinations and comparing their efficacy in assessing DMI and CSI, we aimed to determine whether diagnostic performance equivalent to conventional protocols can be achieved without contrasting agents, thereby potentially reducing the healthcare burden. Few studies have explored this topic, and our findings may provide new insights and form the basis for future clinical practice.
We retrospectively collected data from patients with suspected EC who underwent mpMRI using a Siemens 3.0 T superconducting MRI scanner (manufacturer’s software platform NUMARIS/4 [version syngo MR E11], Manufacturer name: Siemens Healthcare GmbH, Location: Erlangen, Germany) at the first hospital of Putian City between August 2020 and April 2025. The inclusion criteria were as follows: (1) preoperative mpMRI with an intact uterus and image quality sufficient for diagnosis; (2) histologically confirmed, untreated EC scheduled for surgery; and (3) surgical treatment, including total hysterectomy, performed within 2 weeks after the MRI examination, with complete postoperative pathological results available.
Although tumor subtraction is theoretically feasible in patients with stage IV EC, these patients were excluded because those with distant metastases typically do not undergo surgery and instead receive other treatments.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki. The protocol was approved by the Ethics Committee of the First Hospital of Putian City (Approval Number: 2022-020), and no specific informed consent was required because anonymized patient records were used.
All patients were confirmed to have no absolute contraindications to MRI. Examination procedures and precautions were explained to patients beforehand. Patients were instructed to empty the bowel and bladder prior to scanning to reduce peristaltic motion and minimize image artifacts.
Imaging was performed in the head-first supine position using a total imaging matrix (TIM) coil combined with a body phased-array surface coil. Sagittal and coronal fast spin-echo T2-weighted imaging (T2WI) of the uterine corpus were acquired, followed by axial T1WI, T2WI, reduced field-of-view DWI, and DCE sequences. All sequences were acquired with high spatial resolution, a small field of view, and no interslice gap. The key parameters of the sequences relevant to this study are presented in Table 1.
| Parameters | Axial T2WI | DWI | DCE |
| Acquisition Voxel (mm3) | 0.9 |
2.2 |
1.3 |
| Reconstruct Voxel (mm3) | 0.7 |
1.1 |
0.9 |
| Excitation angle | 90° | 90° | 13° |
| Field of view (mm) | 220 |
260 |
280 |
| Slices | 44 | ||
| Phase encoding direction | RL | AP | RL |
| TR (ms) | 2690 | 6100 | 5.63 |
| TE1/TE2 (ms) | 103 | 66/106 | 2.46/3.69 |
| Scanning time (s) | 23 |
MRI, magnetic resonance imaging; T2WI, T2-weighted imaging; DWI, diffusion-weighted imaging; DCE, dynamic contrast-enhanced; RL, right-left; AP, anterior-posterior; TR, repetition time; TE1, echo time 1; TE2, echo time 2.
To standardize the evaluation criteria, all participating radiologists received uniform training before formal image analysis, following the 2018 ESUR guidelines for EC MRI staging (published in European Radiology, 2019 [7]). The initial phase of the training focused on defining the tumor’s signal characteristics across different MRI sequences, as detailed below. On T2WI sequences, tumors typically show slightly higher signal intensity than normal endometrium, deep myometrium, and cervical stroma, while relatively low-signal bands appear as more pronounced high-signal areas. On DWI sequences, tumors exhibit high signal intensity relative to normal myometrium and cervical stroma, corresponding to low signal on apparent diffusion coefficient map (ADC_map). During early and late phases of DCE, tumors generally show relatively low signal, although some lesions may demonstrate high signal in the early phase. The signal differences between tumor and normal tissue were used to determine the depth of myometrial invasion and the extent of cervical stromal infiltration on MRI [1, 7, 9]. Subsequently, the training established the imaging diagnostic criteria for DMI and CSI. DMI is defined as tumor invasion that reaches or exceeds half of the myometrial thickness. Measurements were performed on axial oblique images oriented perpendicular to the uterine cavity. A reference line was first drawn parallel to the presumed inner border of the myometrium. Two perpendicular lines were then drawn: one measuring the full thickness of the myometrium, and the other measuring the maximum depth of tumor invasion into the myometrium. The depth of myometrial invasion was determined by the ratio of the lengths of these two lines. CSI is defined as tumor infiltration into the cervical stroma without extension beyond the uterus. Notably, tumor extension that is limited to the endocervical canal or solely involves the cervical mucosa is not classified as CSI [7].
All cases were evaluated by gynecologists with the rank of attending physician or higher to determine the surgical procedure and postoperative pathological stage. Pathological assessments were independently confirmed by two physicians, and in cases of disagreement, confirmation was made by a more senior physician.
T2WI was combined with either DWI and DCE to form the T2&DWI group and the T2&DCE group. Two senior radiologists with over 8 years of experience independently assessed DMI and CSI on the T2&DWI images, and after 60 days, on the T2&DCE images. A case was considered positive if DMI or CSI was visible on any sequence within the combination. Discrepancies were resolved by a third radiologist with over 15 years of experience.
All data were analyzed using IBM SPSS Statistics (version 23.0; IBM Corp.,
Armonk, NY, USA) and R, version 4.3.1 (R Project for Statistical Computing,
Vienna, Austria) was evaluated using the Kappa statistic. Kappa values
A total of 138 patients were included in this study, with a mean age of 56.312
Agreement between the two sequence combinations was high for both readers. Kappa values for DMI assessment were 0.815 and 0.841, and for CSI assessment were 0.877 for both readers. Inter-reader agreement for the T2&DWI and T2&DCE groups was also high, with Kappa values of 0.809 and 0.899 for DMI, 0.909 and 0.859 for CSI (for details, see Supplementary Table 1.1 and Supplementary Table 1.2).
DMI assessment by the T2&DWI and T2&DCE groups showed high concordance, both between readers for the same sequence combination, as well as for the same reader between the two sequence combinations. After arbitration by a third physician, the T2&DWI group correctly identified DMI in 25 cases, 21 of which were also correctly assessed by the T2&DCE group. In comparison, the T2&DCE group underestimated DMI in 4 cases. In the T2&DCE group, 22 cases were correctly assessed, while the T2&DWI group underestimated 1 case.
The T2&DWI group underestimated 6 cases, 1 of which was correctly assessed by the T2&DCE group, and T2&DCE also underestimated the remaining 5. The T2&DCE group underestimated 9 cases, 4 of which were correctly assessed by T2&DWI. Both groups overestimated 7 cases, 6 of which were identical, and correctly assessed the absence of DMI in 100 cases, 99 of which were identical.
In secondary analysis, the high-sensitivity group correctly identified DMI in 26
cases, underestimated it in 5 cases, and overestimated it in 9 cases. The
high-specificity group correctly identified 24 cases, underestimated 7 cases, and
overestimated 6 cases. The efficacy indices and ROC AUCs of all groups are shown
in Table 2 and Fig. 1 (for details, see Supplementary Table 2.1–2.4).
Pairwise comparisons using the DeLong test showed no statistically significant
differences between any groups (all p
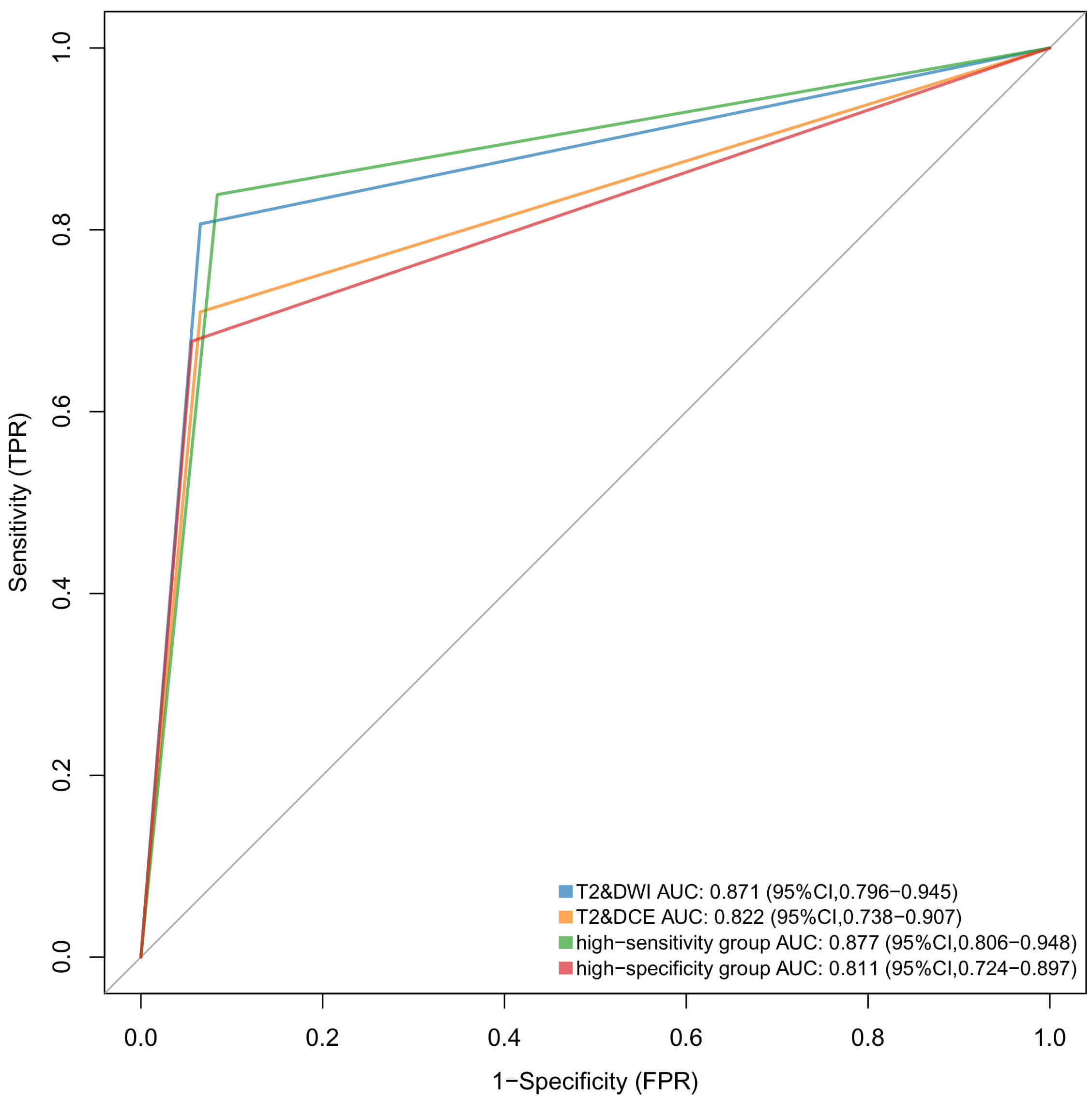 Fig. 1.
Fig. 1.
Comparison of AUC for each sequence combination in assessing DMI. The AUC of the high-sensitivity group was slightly higher than that of the T2&DWI combination (p = 0.697), both of which were higher than those of the T2&DCE and high-specificity groups.
| T2&DWI group | T2&DCE group | High-sensitivity group | High-specificity group | |
| Sensitivity | 0.806 (0.625, 0.926) | 0.710 (0.520, 0.858) | 0.839 (0.663, 0.946) | 0.774 (0.486, 0.833) |
| Specificity | 0.935 (0.870, 0.973) | 0.935 (0.870, 0.973) | 0.916 (0.846, 0.961) | 0.944 (0.882, 0.979) |
| PPV | 0.781 (0.600, 0.907) | 0.759 (0.565, 0.897) | 0.743 (0.567, 0.876) | 0.778 (0.577, 0.914) |
| NPV | 0.943 (0.881, 0.979) | 0.917 (0.849, 0.962) | 0.952 (0.890, 0.984) | 0.910 (0.841, 0.956) |
| Accuracy | 0.906 (0.844, 0.949) | 0.884 (0.819, 0.932) | 0.899 (0.836, 0.943) | 0.906 (0.819, 0.932) |
| AUC | 0.871 (0.796, 0.945) | 0.822 (0.738, 0.907) | 0.877 (0.806, 0.948) | 0.811 (0.724, 0.897) |
In parentheses are 95% confidence intervals (CI).
PPV, positive predictive value; NPV, negative predictive value; AUC, area under the curve; ROC, receiver operating characteristic; DMI, deep myometrial invasion; T2&DWI, T2WI combined with DWI group; T2&DCE, T2WI combined with DCE group.
| Variable | DMI | CSI | ||||
| AUC of ROC | p-value of DeLong test | p-value after Holm correction | AUC of ROC | p-value of DeLong test | p-value after Holm correction | |
| T2&DWI group vs. T2&DCE group | 0.871 vs. 0.822 | 0.181 | 0.725 | 0.909 vs. 0.950 | 0.322 | 1.000 |
| T2&DWI group vs. high-sensitivity group | 0.871 vs. 0.877 | 0.697 | 1.000 | 0.909 vs. 0.946 | 0.368 | 1.000 |
| T2&DWI group vs. high-specificity group | 0.871 vs. 0.811 | 0.053 | 0.319 | 0.909 vs. 0.913 | 0.317 | 1.000 |
| T2&DCE group vs. high-sensitivity group | 0.822 vs. 0.877 | 0.078 | 0.399 | 0.950 vs. 0.946 | 0.317 | 1.000 |
| T2&DCE group vs. high-specificity group | 0.822 vs. 0.811 | 0.495 | 1.000 | 0.950 vs. 0.946 | 0.368 | 1.000 |
| High-sensitivity group vs. high-specificity group | 0.877 vs. 0.811 | 0.054 | 0.319 | 0.946 vs. 0.913 | 0.422 | 1.000 |
CSI, cervical stromal invasion.
CSI was assessed by both the T2&DWI and T2&DCE groups, showing high concordance among readers for the same sequence combination, as well as within the same reader across the two combinations. Pathological examination confirmed 12 cases of CSI (12/138, 8.70%).
The T2&DCE group correctly identified CSI in 11 cases, 10 of which were also correctly assessed by the T2&DWI group. The T2&DWI group underestimated 1 case, and both combinations underestimated another case. Both groups overestimated CSI in 2 cases, one of which was identical. Both groups correctly assessed the absence of CSI in 124 cases, 123 of which were similar, with one case overestimated by each group.
In secondary analysis, the high-sensitivity group correctly identified CSI in 11
cases, underestimated 1 case, and overestimated 3 cases. The high-specificity
group correctly identified 10 cases, underestimated 2 cases, and overestimated 1
case. The diagnostic performance and ROC AUC of each group are shown in Table 4
and Fig. 2 (for details, see Supplementary Table 4.1–4.4). Pairwise
comparisons using the DeLong test revealed no statistically significant
differences between the four groups (all p
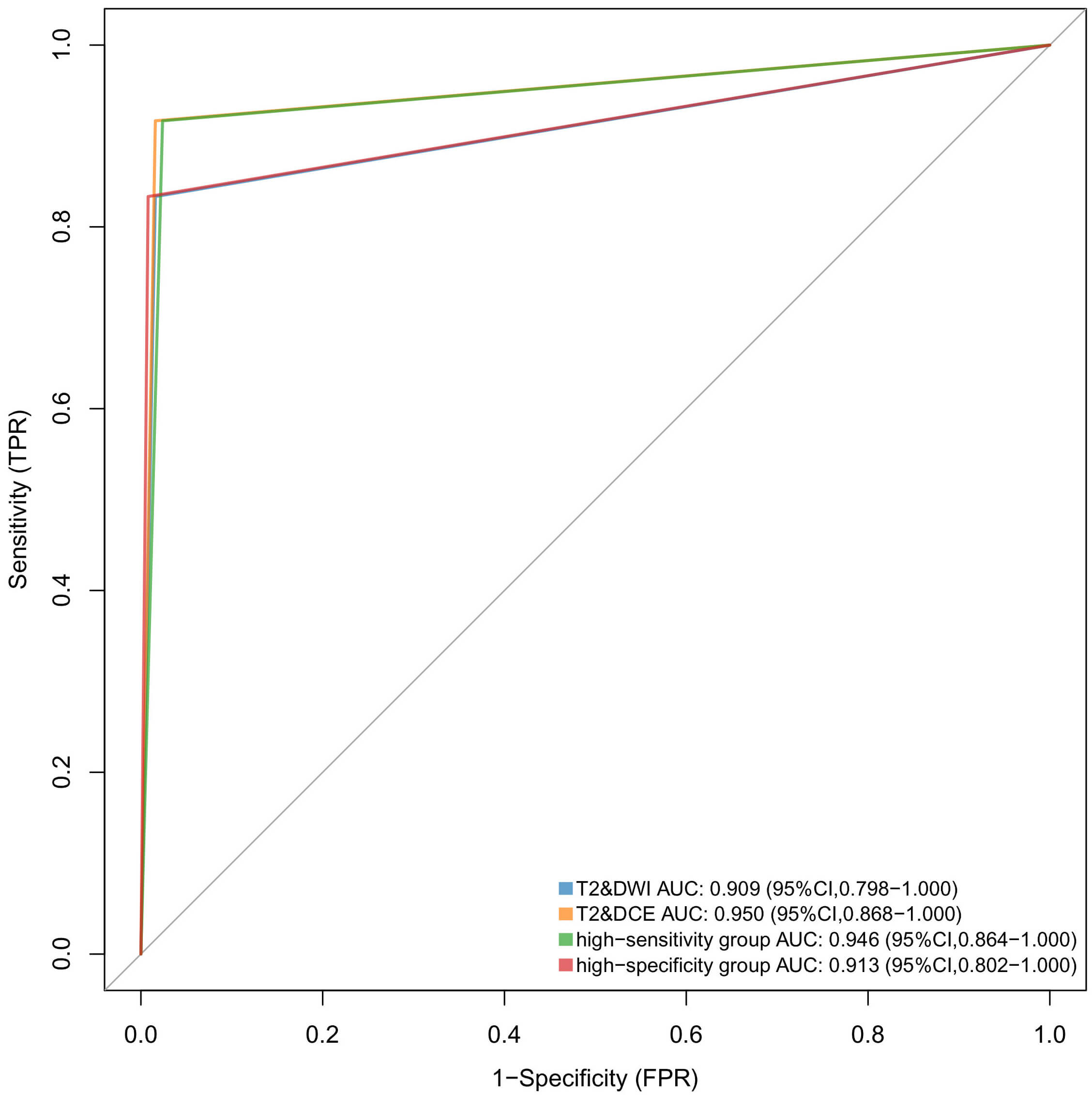 Fig. 2.
Fig. 2.
Comparison of the AUC of CSI assessed across sequence groups. The AUC of all four groups exceeded 0.900, and the AUC of the T2&DCE group was similar to that of the high-sensitivity group (p = 0.317) and higher than that of the T2&DWI group (p = 0.322), and the high-specificity of groups (p = 0.368).
| T2&DWI group | T2&DCE group | High-sensitivity group | High-specificity group | |
| Sensitivity | 0.833 (0.516, 0.979) | 0.917 (0.615, 0.998) | 0.917 (0.615, 0.998) | 0.833 (0.516, 0.979) |
| Specificity | 0.984 (0.944, 0.998) | 0.984 (0.944, 0.998) | 0.976 (0.932, 0.995) | 0.992 (0.957, 1.000) |
| PPV | 0.833 (0.516, 0.979) | 0.846 (0.545, 0.981) | 0.786 (0.492, 0.953) | 0.909 (0.587, 0.998) |
| NPV | 0.984 (0.944, 0.998) | 0.992 (0.956, 0.998) | 0.992 (0.956, 1.000) | 0.984 (0.944, 0.998) |
| Accuracy | 0.971 (0.927, 0.992) | 0.978 (0.938, 0.992) | 0.971 (0.927, 0.992) | 0.978 (0.938, 0.996) |
| AUC | 0.909 (0.798, 1.000) | 0.950 (0.868, 1.000) | 0.946 (0.864, 1.000) | 0.913 (0.802, 1.000) |
The choice of treatment strategy for EC depends on the local tumor stage, which
involves evaluating the depth of myometrial invasion (
Pre-treatment MRI staging of EC is critical. The depth of myometrial invasion serves as a surrogate marker for lymph node metastasis and is associated with poorer prognosis. Therefore, accurate identification of DMI by MRI is essential, not only for local staging but also as a recognized adverse prognostic factor [12]. Axial MRI of the uterine corpus provides optimal visualization of the myometrium, allowing layer-by-layer assessment of tumor depth and extent.
Neves et al. [13] reported that T2WI combined with DWI achieved 92.1% accuracy in assessing myometrial invasion, comparable to the 90.52% observed in the T2&DWI group in our study. Stanzione et al. [14] analyzed 92 EC cases and found no significant difference in diagnostic accuracy among DWI, DCE, and conventional comprehensive MRI protocols for identifying DMI, consistent with our findings. Bonatti et al. [15] previously reported that DWI outperformed DCE in predicting DMI, although not statistically significant.
Wang et al. [16] conducted a meta-analysis of 19 studies involving 961 patients, which showed that in a subgroup of 7 studies, the AUCs of DWI combined with T2WI and DCE combined with T2WI for diagnosing DMI in EC were 0.959 (95% confidence interval [CI]: 0.932–0.986) and 0.929 (95% CI: 0.847–1.000), respectively, with no statistically significant difference between the two. The study further indicated that the use of DWI alone, DCE alone, or the combination of DWI and DCE were all reasonable approaches for diagnosing DMI. In addition, sensitivity analysis suggested that DWI may be more sensitive than DCE in detecting DMI. This conclusion is consistent with our findings. To corroborate this, we present a representative case from our study (Fig. 3), illustrating the potential advantage of DWI in identifying DMI. Based on our results and previous studies, individualized MRI protocols without DCE are feasible, offering advantages such as avoiding contrast agents, reduced invasiveness, lower cost, shorter acquisition time, and maintenance of diagnostic reliability for DMI.
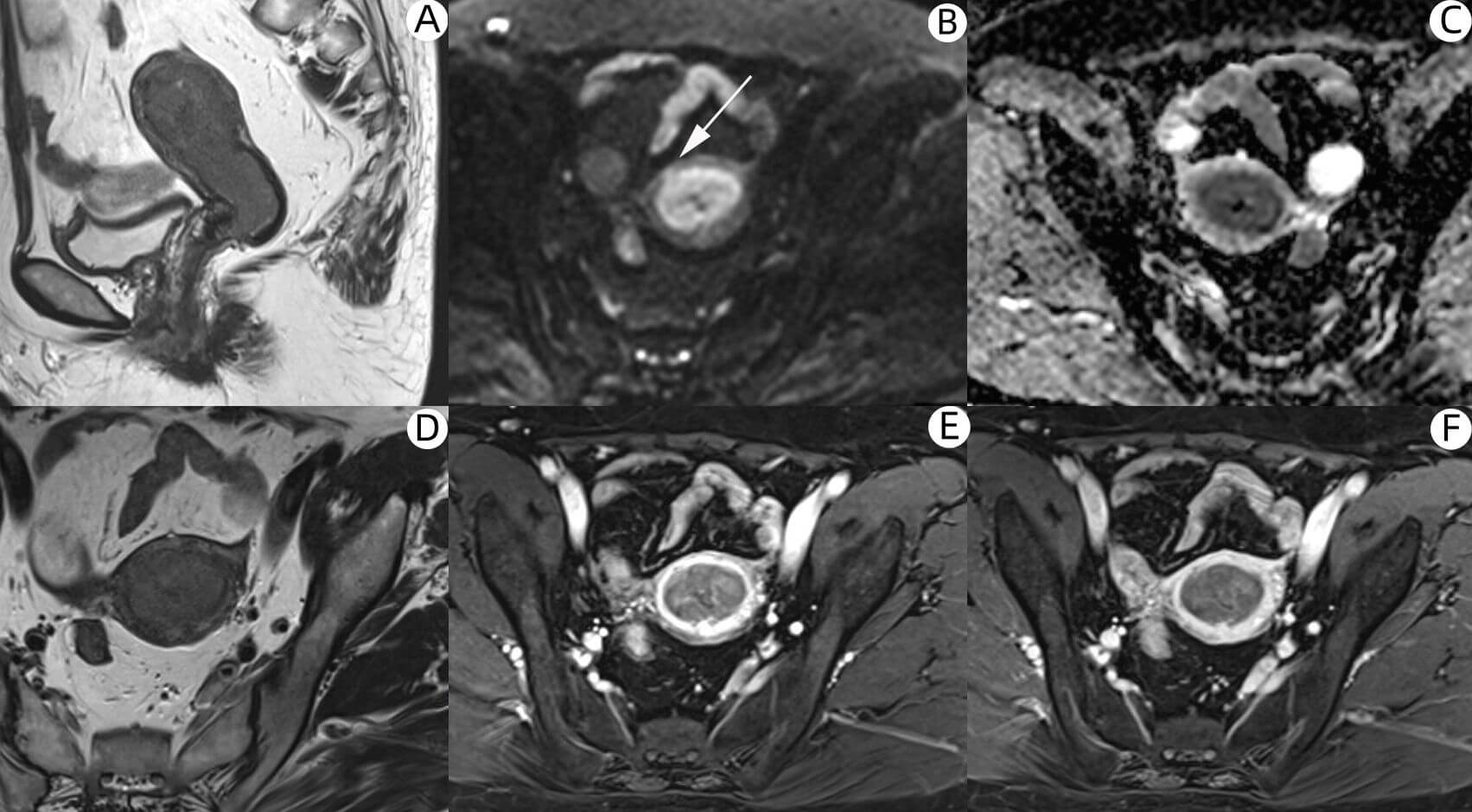 Fig. 3.
Fig. 3.
In a 54-year-old patient with EC, postoperative pathology confirmed the presence of DMI. (A) Sagittal T2WI of the uterine body. (B–F) Axial images of the uterine body: (B) DWI (b = 800), (C) ADC_map, (D) T2WI, (E) early-phase, and (F) late-phase DCE images. Fig. 3B showed DMI of the anterior wall of the uterine corpus with a high signal area (as indicated by the white arrows). The corresponding ADC_map showed a slightly low signal shadow. However, the dynamic enhancement scans of early and late images did not show DMI. EC, endometrial cancer.
In the analysis of imaging characteristics of misdiagnosed cases in this study, we found that when tumor involvement reached approximately half of the uterine wall thickness, it was often difficult to measure the depth of infiltration accurately, leading to misinterpretation. We also observed that assessment inaccuracies were likely to occur under the following conditions, causing significant thinning or deformation of the myometrium: (1) large tumor volume; (2) presence of substantial intrauterine fluid and/or hematometra; and (3) marked atrophy of the uterine body. In such scenarios, a comprehensive MRI protocol should be employed for improved assessment accuracy. Through analysis of accurately assessed case imaging features, we found that when the T2&DWI group shows small tumor volume, no definite tumor signal, or no apparent signs of superficial myometrial invasion, the T2&DCE group usually yields similar assessment conclusions. Similarly, when the T2&DWI group clearly indicates DMI, the evaluation results of the two sequence groups are largely consistent. However, when the assessment of DMI is ambiguous in the T2&DWI group, the supplementary information provided by the T2&DCE group may offer additional value for the final evaluation. Based on these findings, we recommend that when the T2&DWI group can clearly determine either the absence of superficial myometrial invasion or the presence of DMI, the DCE sequence may not be strictly necessary. However, when image quality is suboptimal for assessing the superficial myometrium or when tumor involvement approximates half of the myometrial thickness, performing a DCE sequence may provide valuable assistance in evaluating DMI.
EC invades the cervical stroma in two main patterns [17, 18]: (1) simultaneous invasion of both the cervical mucosa and stroma, and (2) direct penetration of the cervical stroma through the uterine myometrium, bypassing the mucosa. EC with CSI is associated with lymph node metastasis and poor survival [19]. Assessment of CSI can help tailor surgical planning and provide fertility-preserving treatment options for young women without CSI [20].
In a 1.5 T MRI study for localized EC staging, including CSI, the accuracy, sensitivity, and specificity of DWI were 95%, 98%, and 80%, respectively. Based on these findings, Bonatti et al. [15] concluded that DWI could reliably replace contrast-enhanced MRI. Bi et al. [17] conducted a meta-analysis of 42 studies involving CSI and found that 3.0 T MRI offered higher diagnostic sensitivity, and DWI alone demonstrated higher sensitivity than DCE or T2WI alone. Lin et al. [21] analyzed 83 EC patients using 3.0 T MRI and reported that DWI, including ADC_maps, had significantly higher diagnostic efficacy for CSI compared with DCE (p = 0.009) or T2WI (p = 0.013). Hori et al. [22] studied 71 EC patients, including 6 cases of CSI and showed that DWI and DCE had almost identical performance in accuracy, sensitivity, and specificity for CSI at 3.0 T MRI. Our study enrolled a total of 138 EC patients, of whom 12 were pathologically confirmed to have CSI. Statistical analysis indicated that there was no statistically significant difference between the T2&DWI and T2&DCE groups in assessing CSI, a finding consistent with previous studies.
Analysis of misdiagnosed cases based on imaging features revealed that underestimation by both sequence combinations was attributed to the absence of definitive signs of CSI on MRI. Overestimation in two cases by the T2&DWI group was due to imaging features suggesting suspected minimal tumor involvement of the cervical stroma. Furthermore, underestimation by the T2&DWI group and overestimation by the T2&DCE group were primarily caused by the larger tumor tissue extending into the cervical canal, resulting in marked thinning of the cervical wall and altered signal intensity, which made it difficult to distinguish the tumor from the surrounding cervical stroma. Based on these findings, we recommend that the DCE sequence may not be strictly necessary when the T2&DWI group shows no tumor involvement of the uterine isthmus. In contrast, DCE should be considered when the tumor extends deeply into the isthmus or endocervical canal to aid in diagnosis.
In this study, we compared the T2&DWI group with the T2&DCE group, as well as high-sensitivity and high-specificity combinations of MRI sequences. Preliminary results indicated that the T2&DWI group had a diagnostic performance similar to the other groups for assessing DMI and CSI, with no statistically significant differences. Based on the above findings, we propose that in clinical practice, the combination of T2WI and DWI may replace contrast-enhanced imaging under specific conditions. When the T2&DWI group clearly demonstrates either the absence of superficial myometrial invasion or the presence of DMI, and when the tumor does not involve the uterine isthmus, DCE may not be strictly necessary. This approach is particularly suitable for patients with contraindications, such as renal impairment or allergies to contrast agents [23]. Adopting a contrast-free MRI protocol consisting solely of T2WI and DWI can help reduce the medical burden on patients while maintaining diagnostic accuracy. However, when the T2&DWI combination provides unclear visualization of the superficial myometrium, suggests tumor involvement of approximately half of the myometrial thickness, or indicates tumor extension into the isthmus or the endocervical canal, the addition of DCE is recommended to improve diagnostic reliability. In actual clinical decision-making, patients’ overall health status and economic factors should also be comprehensively considered. This study may offer new perspectives for optimizing the MRI evaluation pathway in EC.
Although the findings of this study hold significant clinical implications, several limitations should be acknowledged. First, the sample size of pathologically confirmed DMI or CSI cases was relatively small, particularly for the latter. This limitation may introduce statistical bias and, to some extent, restrict the generalizability of our conclusions. Second, because this was a retrospective study based on previously recorded data, information bias or missing data may exist. Third, the study lacked long-term follow-up, preventing assessment of long-term outcomes associated with mpMRI in EC. Finally, the absence of multicenter validation warrants caution when extrapolating findings to other populations and clinical settings. Future studies should aim to expand sample size, include multicenter data, and use prospective designs to enhance the reliability of conclusions.
In summary, the T2WI & DWI combination demonstrated comparable efficacy to the T2WI & DCE combination for preoperative assessment of DMI and CSI in EC, with no statistically significant differences. These findings provide new evidence supporting the use of unenhanced MRI protocols in specific patient populations, particularly those with contrast allergies or renal insufficiency. Future research should continue to explore more efficient, contrast-free MRI protocols to optimize assessment of EC extent.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
JJL, BLR, and SYW designed the research study. FJW and SYW provided assistance and recommendations for the MRI scanning protocol and image interpretation standards. JJX was responsible for collecting and organizing the cases. KHL and JJX each evaluated the patients’ imaging studies, and FJW served as the arbitrator for disputed cases. JJL and JJX performed statistical analysis on the data and interpreted the results. JJL and KHL drafted this manuscript, with revisions provided by BLR and SYW. All authors contributed to the manuscript revision, and all approved the final version. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki. The protocol was approved by the Ethics Committee of the First Hospital of Putian City (Approval Number: 2022-020), and no special informed consent was required because anonymous patient records were used.
We want to express our gratitude to all those who helped us in writing this manuscript. We also thank the peer reviewers for their valuable comments and suggestions. We wish to acknowledge the Editor for their valuable input and assistance with this manuscript.
The study was supported by the Putian University Scientific Research Fund Project (Grant No.: 2022098).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG45908.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.