




 , Fatemeh Abdollahy Biroon 2,†, Reza Daghayeghi 3, Arina Ansari 4, Rasoul Hossein Zadeh 5, Qumars Behfar 6,*
, Fatemeh Abdollahy Biroon 2,†, Reza Daghayeghi 3, Arina Ansari 4, Rasoul Hossein Zadeh 5, Qumars Behfar 6,* , Niloofar Deravi 7,*
, Niloofar Deravi 7,*1 School of Medicine, Mashhad University of Medical Sciences, 91778-99191 Mashhad, Iran
2 School of Medicine, University of Maryland, College Park, MD 20742, USA
3 Institute of Fundamental Medicine and Biology, Kazan Federal University, 420008 Kazan, Russian Federation
4 Student Research Committee, School of Medicine, North Khorasan University of Medical Sciences, 94149-75516 Bojnurd, Iran
5 Student’s Research Committee, Faculty of Medicine, Mashhad University of Medical Sciences, 91778-99191 Mashhad, Iran
6 National Institute for Health Research, Tehran University of Medical Sciences, 14179-94378 Tehran, Iran
7 Student Research Committee, School of Medicine, Shahid Beheshti University of Medical Sciences, 19857-17413 Tehran, Iran
†These authors contributed equally.
Abstract
This meta-analysis aimed to evaluate the association between maternal smoking during pregnancy and the risk of Attention-Deficit/Hyperactivity Disorder (ADHD) in offspring. This association is complex and may be influenced by genetic confounding, as individuals with ADHD are at higher risk of engaging in smoking behaviors.
The PubMed, Scopus, Web of Science, and Cochrane Library databases were searched to identify relevant literature. Prospective cohort studies that met the inclusion criteria entered the data extraction process. Selected data for analysis included risk estimates in form of odds ratios (ORs), hazard ratios (HRs), or risk ratios (RRs), along with 95% CIs. Sensitivity and bias analysis were also performed.
A total of 14 prospective cohorts comprising 1,763,268 participants were eligible for the analysis. Smoking during pregnancy was associated with an increased risk ADHD in the offspring (pooled RR = 1.55 [95% CI: 1.25–1.86], p < 0.001). This association decreased slightly after subgroup analysis based on adjustment for maternal ADHD (RR = 1.47 [95% CI: 1.08–2.01], p < 0.001). This observation was replicated after adjustment for study location, maternal age, alcohol consumption, maternal socioeconomic status, and ADHD history.
Based on the evidence presented in this systematic review and meta-analysis, maternal smoking during pregnancy is associated with an increased risk of ADHD in offspring. Therefore, pregnant women should be encouraged to quit smoking and to avoid exposure to tobacco smoke.
The study has been registered on https://www.crd.york.ac.uk/PROSPERO/search (registration number: CRD420251274456; registration link: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251274456).
Keywords
- ADHD
- maternal smoking
- pregnancy
- prospective cohort
Attention-Deficit/Hyperactivity Disorder (ADHD) is the most common
neurodevelopmental disorder among school-aged children worldwide, with an
estimated prevalence of 5% to 7% in 2015 [1]. The disorder is characterized by
symptoms of inattention, hyperactivity, and impulsivity that often persist into
adulthood [2]. Research indicates that individuals with ADHD, regardless of
gender, are more likely to have comorbid mood disorders, disruptive behaviors
such as oppositional defiant disorder and conduct disorder, substance use
disorders, and poor verbal working memory [3, 4]. The financial burden of the
disorder is also considerable, with annual incremental costs in the USA alone estimated at
The pathophysiology of ADHD is not fully understood. However, substantial evidence suggests that both genetic factors and environmental exposures may contribute to the disorder’s development. Research has estimated the heritability of ADHD at 70% to 80%, confirming a genetic background for the disorder [6]. Several studies have also identified ADHD as a potential adverse outcome of exposure to environmental hazards, including lead [7], alcohol [8], and cigarette smoke [9].
Alarmingly, approximately 4.9% of pregnant women continue to smoke during pregnancy, posing significant risks to fetal development [10]. Newborns of smoking mothers are at an increased risk of facing adverse early-life outcomes, such as premature birth, low birth weight, and respiratory distress [11].
A recent evidence has also suggested a relationship between maternal smoking during pregnancy and ADHD, with children born to mothers who smoke during pregnancy are at an increased risk of developing ADHD. Although the exact fetal brain alterations caused by maternal smoking remain unclear, it is well established that maternal smoking during pregnancy increases the risk of neurotoxicity in the developing fetus [12]. Animal studies have also revealed that prenatal nicotine exposure induces hyperactivity in the offspring of rats, suggesting that maternal smoking during pregnancy may be a risk factor for ADHD [13, 14].
However, existing research remains inconsistent regarding the association between smoking during pregnancy and the development of ADHD. While some studies portray a strong association [15, 16], others find little or no effect [17]. Many researchers have also noted that findings suggesting a causal relationship may be confounded by factors such as the heritable nature of the disorder, socioeconomic status, geographic background, changes in smoking behavior due to preparation for conception or recognition of pregnancy, and other unknown differences between smokers and non-smokers [18, 19].
This inconsistency justifies the need to clarify the causal role of maternal smoking during pregnancy in the development of ADHD in children by using a meta-analytic approach. Confirming a significant association would strongly encourage healthcare policymakers to implement systematic efforts to raise awareness and promote smoking cessation during pregnancy. Longitudinal prospective cohort studies are the optimal approach for systematically evaluating the association between maternal smoking during pregnancy and the risk of ADHD in offspring, given the quality of evidence they provide and their ability to adjust for covariates. The most recent meta-analysis of prospective cohort study examining this association was conducted by He et al. [20]. Since then, several additional prospective cohort studies have been published, which warrant consideration for an updated meta-analysis. Therefore, our aims were to systematically review and meta-analyze prospective cohort studies examining the association between maternal smoking during pregnancy and ADHD in offspring, and to identify potential moderators through subgroup analysis.
Our goal in this systematic review and meta-analysis is to investigate the relationship between maternal smoking and ADHD in children. We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [21]. This study is registered in International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420251274456.
A comprehensive literature search was conducted up to August 4, 2023, to identify relevant papers from the Cochrane Library, Web of Science, PubMed, and Scopus databases. Three primary subgroups of free-text phrases and Medical Subject Headings (MeSH) included the search strategy. Terms related to ADHD (“attention deficit hyperactivity disorder” OR “ADHD”) comprised one subgroup, while terms associated with smoking (“smoke” OR “smoking” OR “tobacco”) and pregnancy (“pregnancy” OR “prenatal” OR “perinatal” OR “maternal”) comprised the other two. There were no limitations on the date, publication type, or language when combining the subgroups using the ‘AND’ operator. The search approach was modified according to the query format of each database. We also the reference lists of pertinent systematic reviews to ensure that no eligible publications were overlooked and included any additional research suitable for our analysis. Each stage was conducted independently by two reviewers, who discussed and resolved any disagreements.
Meta-analysis inclusion criteria were as follows:
(1) Prospective cohort design.
(2) Primary focus on evaluating the relationship between maternal smoking and the risk of ADHD in children.
(3) ADHD was defined in accordance with widely recognized scientific standards.
(4) Odds ratios (ORs), hazard ratios (HRs), or risk ratios (RRs), along with 95% CIs, were used to calculate the prevalence of ADHD.
The analysis did not include studies focusing on passive smoking, containing overlapping data, were conducted on animal models, or used other study designs. Systematic reviews, meta-analyses, narrative reviews, case reports, case series, cross-sectional, and case-control studies were specifically disqualified.
To determine eligibility for this meta-analysis, two independent reviewers, FZ and FAB, screened the titles and abstracts of all studies. Studies that did not meet the inclusion requirements were excluded. Full texts of the remaining studies were then reviewed, and eligible studies proceeded to the data extraction stage.
Data were extracted in three categories: (1) Study features (authors, location, year of publication); (2) Study design (number of participants, ADHD assessment method, follow-up duration, adjusted cofounders); (3) Outcomes (effect size as calculated by RRs and their corresponding 95% CIs). When a study reported risk estimates for multiple groups with varying risk levels (e.g., low, medium, and high), the estimate from the high-risk group was selected for analysis. In order to account for confounding factors, only the risk estimates with the most extensive of adjustment were retrieved from studies that reported results from multiple adjustment models. All indicators were regarded as RRs since the specific sort of relative risk estimate (such as OR, HR, or RR) was deemed irrelevant due to the very rare nature of ADHD. FZ and FAB utilized the Joanna Briggs Institute (JBI) critical appraisal checklists for cohort studies (https://jbi.global/critical-appraisal-tools) to evaluate the quality of the studies. In the event of a disagreement, a third author, QB, was involved in the resolution.
For our data analysis, we used STATA 13.1 (StataCorp LP, College Station, TX,
USA). The findings were shown graphically in a forest plot as pooled RRs with a
95% CI. Significant heterogeneity was indicated by I2
A total of 1605 studies were found after using the search approach outlined in Table 1, of which 995 were removed as duplicates. After further screening of the remaining abstracts, 530 studies were excluded for not meeting the inclusion criteria. Following full-text screening, 66 of the 80 studies were excluded for the reasons detailed in Fig. 1. Ultimately, only 14 studies satisfied the selection criteria and were included in the meta-analysis. The eligible studies were published from 2005–2022 and included a total of 1,763,268 mothers who were assessed for smoking during pregnancy with subsequent ADHD diagnosis in their children. The geographical distribution of the included studies consists of 5 studies conducted in the USA [17, 25, 26, 27, 28], 6 in Europe [15, 29, 30, 31, 32, 33], and 1 study each from Australia [16], Brazil [34], and Japan [35]. Maternal smoking status was commonly determined through self-report at various time points during pregnancy and prenatal visits, with only 1 study using nicotine metabolite levels to objectively determine smoking behavior [35]. At the time of the study, 10 studies [16, 17, 25, 26, 27, 28, 29, 31, 32, 33] used the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM) to diagnose ADHD. 3 studies applied the International Classification of Diseases, 10th edition (ICD-10) [15, 26, 32]. In only 2 studies, the authors chose the Strengths and Difficulties Questionnaire (SDQ) as diagnosis method of ADHD [30, 35]. The follow-up duration among studies ranged from 2–15 years. More details about the characteristics of included studies are described in Table 2 (Ref. [15, 16, 17, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35]).
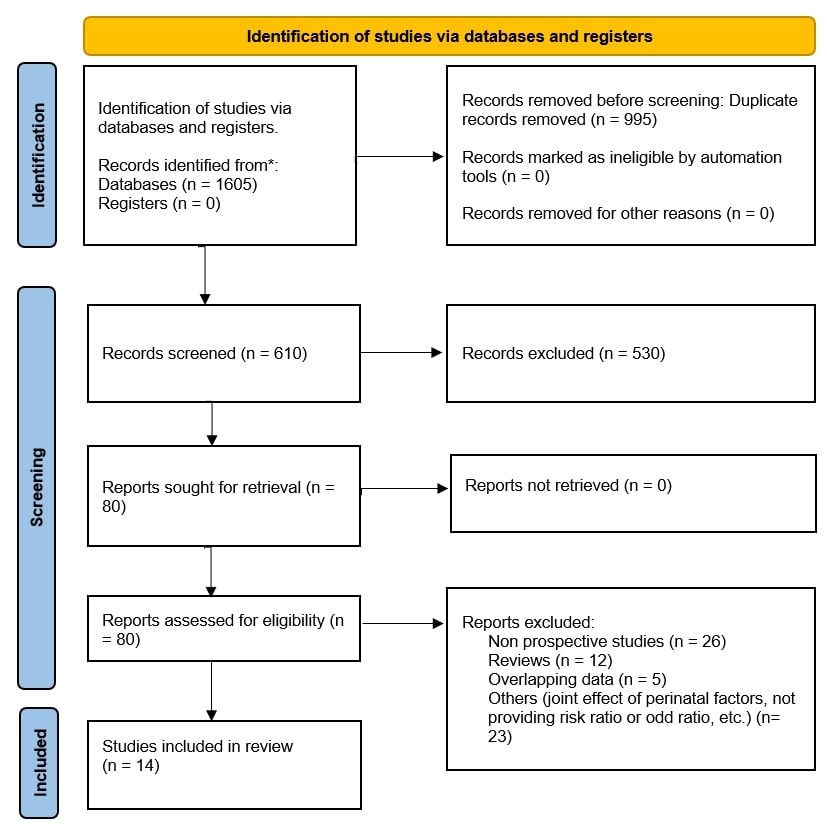 Fig. 1.
Fig. 1.
PRISMA diagram illustrating the study selection for the current systematic review and meta-analysis. * Databases: Cochrane Library, Web of Science, PubMed, and Scopus. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
| Search Strategy | |
| PubMed | |
| #1 | (“Smoking”[MeSH] OR “Tobacco Smoke Pollution”[MeSH] OR “smoke”[Title/Abstract] OR “smoking”[Title/Abstract] OR “tobacco”[Title/Abstract] OR “nicotine”[Title/Abstract]) |
| #2 | (“attention deficit hyperactivity disorder”[Title/Abstract] OR “Hyperactivity”[MeSH] OR “ADHD”[Title/Abstract]) |
| #3 | (“pregnant*”[Title/Abstract] OR “prenatal”[Title/Abstract] OR “perinatal”[Title/Abstract] OR “maternal”[Title/Abstract]) |
| Total: 379 | #1 AND #2 AND #3 |
| Cochrane Library | |
| #1 | MeSH descriptor: [smoke] explode all trees OR (smoke): ti,ab,kw OR (tobacco):ti,ab,kw OR (nicotine):ti,ab,kw |
| #2 | MeSH descriptor: [Pregnancy] explode all trees OR (pregnant*):ti,ab,kw OR (prenatal):ti,ab,kw OR (perinatal):ti,ab,kw OR (maternal):ti,ab,kw |
| #3 | MeSH descriptor: [ADHD] explode all trees OR (ADHD):ti,ab,kw OR (“attention deficit hyperactivity disorder”):ti,ab,kw |
| Total: 24 | #1 AND #2 AND #3 |
| Scopus | |
| #1 | (TITLE-ABS-KEY ((“smoke” OR “smoking” OR “tobacco” OR “nicotine”))) |
| #2 | (TITLE-ABS-KEY ((“attention deficit hyperactivity disorder” OR “ADHD”))) |
| #3 | (TITLE-ABS-KEY ((“pregnant*” OR “prenatal” OR “perinatal” OR “maternal”))) |
| Total: 582 | #1 AND #2 AND #3 |
| Web of Science | |
| #1 | (TS = (“smoke”) OR TS = (“smoking”) OR TS = (“tobacco”) OR TS = (“nicotine”)) |
| #2 | (TS = (“attention deficit hyperactivity disorder”) OR TS = (“ADHD”)) |
| #3 | (TS = (“pregnant*”) OR TS = (“prenatal”) OR TS = (“perinatal”) OR TS = (“maternal”)) |
| Total: 620 | #1 AND #2 AND #3 |
ADHD, Attention-Deficit/Hyperactivity Disorder; MeSH, Medical Subject Headings.
| First author (year) | Country | Evaluation of smoking habit | Diagnosis of ADHD | Sample size | Follow-up duration | Adjusted confounders | JBI score |
| Rodriguez (2005) [31] | Sweden | Self-report | DSMIV | 290 | 7 years | Maternal stress during pregnancy | 10/11 |
| Nigg (2007) [28] | USA | Self-report | DSM-III-R | 717 | 5 years | None | 10/11 |
| Biederman (2009) [25] | USA | Self-report | DSM-III-R | 536 | 10 years for boys and 5 years for girls | Gender, study location, proband identification method, prenatal alcohol/drug exposure, parental ADHD or conduct disorder, maternal and child age at baseline, parental socioeconomic status | 11/11 |
| Ball (2010) [17] | USA | Self-report | DSMIV | 2024 | 7 years | Recruitment source, family psychiatric background, mother’s education, child’s gender | 10/11 |
| Anselmi (2010) [34] | Brazil | Self-report | SDQ | 4452 | 11 years | Sex, ethnicity/skin tone, household income, prenatal alcohol exposure, intelligence level, behavior and emotion problems, mother’s psychiatric condition | 11/11 |
| Sciberras (2011) [16] | Australia | Self-report | DSMIV | 4464 | 2 years | Prenatal maternal alcohol consumption, postpartum depression in mother, newborn intensive care admission, infant birth weight, demographic and social variables, mother’s age at childbirth, number of household members, educational level of main caregiver, and marital condition | 9/11 |
| Langley (2012) [29] | UK | Self-report | DSMIV | 5637 | 7.6 years | Sex, ethnic background, twin/multiple delivery, prenatal alcohol exposure, family socioeconomic status | 10/11 |
| Sagiv (2013) [27] | USA | Self-report | DSMIV (pediatric medical records) | 604 | 8 years | Mother’s age, educational attainment, family income, marital condition, prenatal alcohol exposure, drug use, intelligence score, maternal depression symptoms, home environment (HOME) score, and child-related factors | 11/11 |
| Jaspers (2013) [33] | The Netherlands | Self-report | DSMIV | 1816 | 5 years | Sex, mother’s educational level, attention/hyperactivity difficulties, absence of positive behaviors reported by parents, adolescent ADHD or autism spectrum disorder (ASD) traits | 11/11 |
| Skoglund (2014) [32] | Sweden | Self-report | DSMIV and/or ICD-10 | 768,228 | 9 years | Sex, child’s birth year, number of previous births, maternal age, living arrangement with partner, mother’s educational level, and country of origin | 10/11 |
| Melchior (2015) [30] | France | Self-report | SDQ | 1113 | 7 years | Sex, preterm birth, infant birth weight, length of breastfeeding, mother’s age, psychological difficulties in pregnancy, depression after childbirth, maternal alcohol intake during pregnancy, smoking by mother after delivery, father’s tobacco use during and after pregnancy, research center, parents’ educational level, household income, separation of parents, presence of siblings, and adverse life events | 11/11 |
| Obel (2016) [15] | Denmark | Self-report | ICD-10 | 968,665 | 9 years | Sex, child’s birth year, number of previous births, and mother’s age | 11/11 |
| Minatoya (2019) [35] | Japan | Cotinine level of the third trimester | SDQ | 3216 | 5 years | Household income in pregnancy, mother’s alcohol consumption while pregnant, number of previous births, father’s smoking status during pregnancy, and sex of child | 10/11 |
| Cochran (2022) [26] | USA | Self-report | DSM-5/ICD-10 | 1506 | 15 years | Mother’s age category, educational attainment, participation in food assistance programs, use of public health insurance, marital condition, and ADHD family background | 11/11 |
DSMIV, Diagnostic and Statistical Manual of Mental Disorders (4th ed.); DSM-III-R, Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.); ICD, International Classification of Diseases; JBI, Joanna Briggs Institute; SDQ, Strengths and Difficulties Questionnaire.
The methodological quality of the included prospective cohort studies was evaluated using the JBI Critical Appraisal Checklist. All 14 studies demonstrated a high methodological quality, with scores ranging from 9/11 to 11/11 on the appraisal criteria. Specifically, 9 studies scored 11/11, 4 studies scored 10/11, and 1 study scored 9/11 (Table 2). The consistently high JBI scores indicate that the risk of bias across the included studies is low, bolstering the overall confidence in the findings.
A significant correlation was observed between maternal smoking during pregnancy and ADHD in children, as observed by the pooled adjusted RR of 1.55 (95% CI: 1.25–1.86) for offspring exposed to maternal smoking throughout gestation (Fig. 2). Due to considerable heterogeneity across the studies (I2 = 96.3%), subgroup analyses were performed.
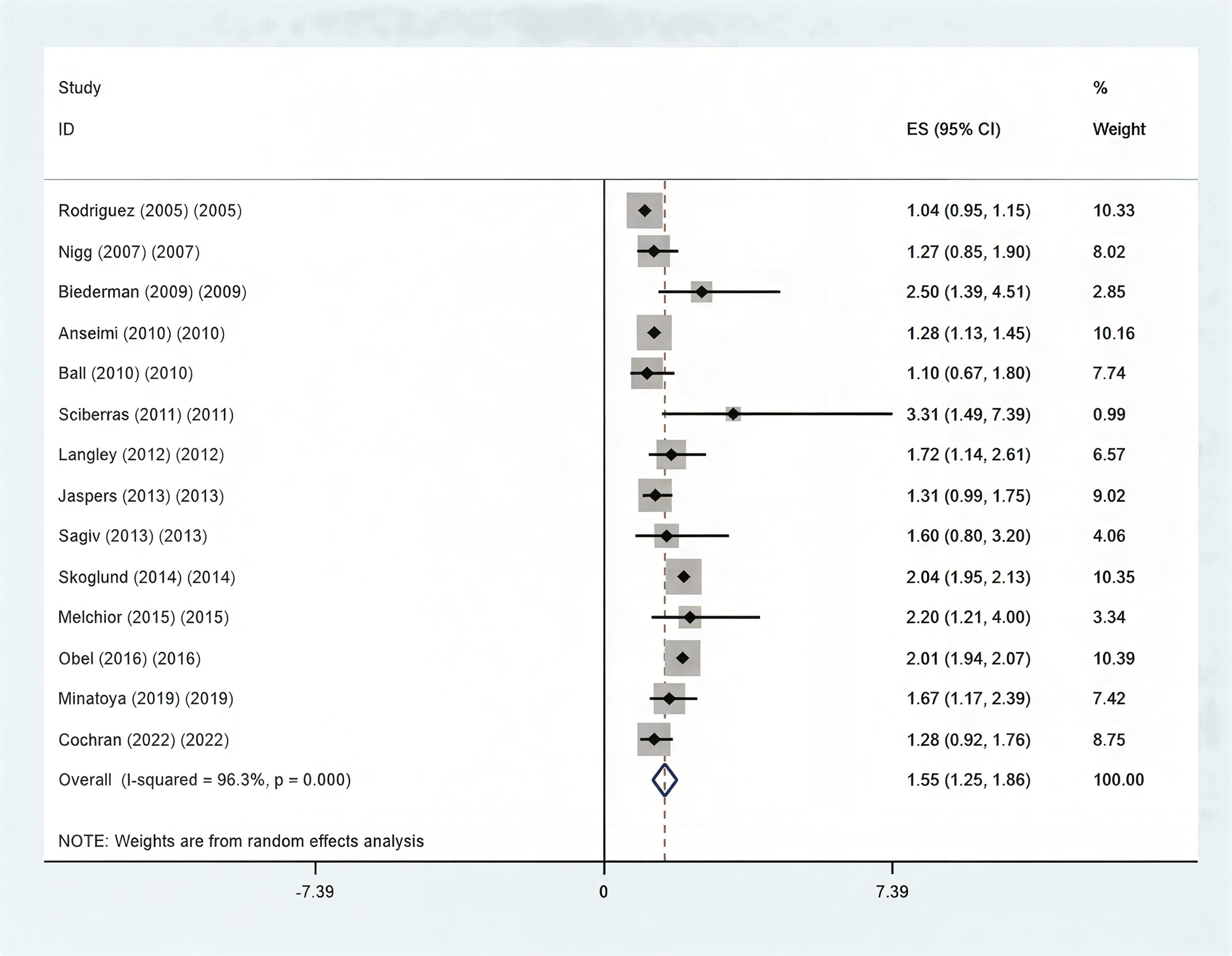 Fig. 2.
Fig. 2.
The relationship between maternal smoking habits during
pregnancy and the risk of ADHD in children is shown by forest plot of the pooled
RR. The total pooled RR is statistically significant (p
We conducted subgroup analyses based on research location, sample size, and confounder correction due to the significant heterogeneity (Table 3). The test for significance of the pooled RR within each subgroup is shown by the p-value in Table 3. With the exception of sample size, the main analysis’s findings held true for every subgroup.
| Subgroup | Number of studies | Pooled RR (95% CI) | Heterogeneity (I2) | p-value | ||
| Geographical location | ||||||
| USA | 5 | 1.28 (1.01–1.56) | 0.0% | 0.556 | ||
| Europe | 6 | 1.66 (1.21–2.11) | 98.3% | |||
| Others | 3 | 1.43 (1.01–1.85) | 38.2% | 0.198 | ||
| Sample Size | ||||||
| 9 | 1.65 (1.39–1.92) | 91.6% | ||||
| 5 | 1.18 (0.94–1.42) | 31.5% | ||||
| Adjustment for confounders | ||||||
| Maternal age | ||||||
| Yes | 6 | 1.94 (1.80–2.09) | 61.3% | |||
| No | 8 | 1.25 (1.07–1.43) | 53.9% | |||
| Socioeconomic status | ||||||
| Yes | 6 | 1.50 (1.20–1.79) | 22.4% | |||
| No | 8 | 1.49 (1.09–1.88) | 97.8% | |||
| Alcohol consumption | ||||||
| Yes | 7 | 1.75 (1.30–2.19) | 91.5% | |||
| No | 7 | 1.50 (1.20–1.79) | 29.4% | |||
| History of ADHD | ||||||
| Yes | 3 | 1.47 (1.08–2.01) | 51.9% | |||
| No | 11 | 1.58 (1.33–1.84) | 96.1% | |||
The statistical significance of the pooled RR for the relationship within the corresponding subgroup is shown in the p-value column.
Regarding the subgroup analysis based on study location, a significant but lower pooled RR was observed in studies conducted in the USA (RR = 1.28, 95% CI: 1.01–1.56), as well as in the “Others” subgroup (RR = 1.43, 95% CI: 1.01–1.85). Additionally, the heterogeneity in these studies was not statistically significant (USA: I2 = 0.0%, Others: I2 = 38.2%). However, for European studies, the pooled RR (RR = 1.66) increased. The heterogeneity was still substantial (I2 = 98.3%, RR = 1.66, 95% CI: 1.21–2.11). In studies with a sample size larger than 1000, smoking during pregnancy was significantly associated with an increased risk of ADHD, according to the subgroup analysis that focused on sample size (RR = 1.65, 95% CI: 1.39–1.92). Studies with a lower sample size, however, did not find this connection (RR = 1.18, 95% CI: 0.94–1.42).
The pooled RR increased after adjustment for maternal age and alcohol use. However, when accounting for parental ADHD history, the pooled RR dropped (RR = 1.47, 95% CI: 1.08–2.01). The association was minimally affected by socioeconomic level.
Table 2 offers a detailed overview of the adjusted confounders used across the included studies. Most studies adjusted for maternal sociodemographic factors such as maternal age (n = 10), socioeconomic status (n = 8), and maternal alcohol consumption during pregnancy (n = 7). Importantly, a small number of studies (n = 3) included adjustments for familial or genetic factors, specifically maternal or parental history of ADHD. This consistent adjustment for key social and environmental variables across the cohort studies enhances the robustness of the reported associations.
The sensitivity analysis demonstrated the robustness of our findings, showing that the RR and its corresponding 95% CI were not significantly impacted by the removal of any single study or group of trials with similar features. To find any publication bias, we also performed funnel plot analysis, Egger’s regression test, and Begg’s test. Although the funnel plot (Fig. 3) showed visual asymmetry, neither the Egger nor Begg tests showed evidence of publication bias.
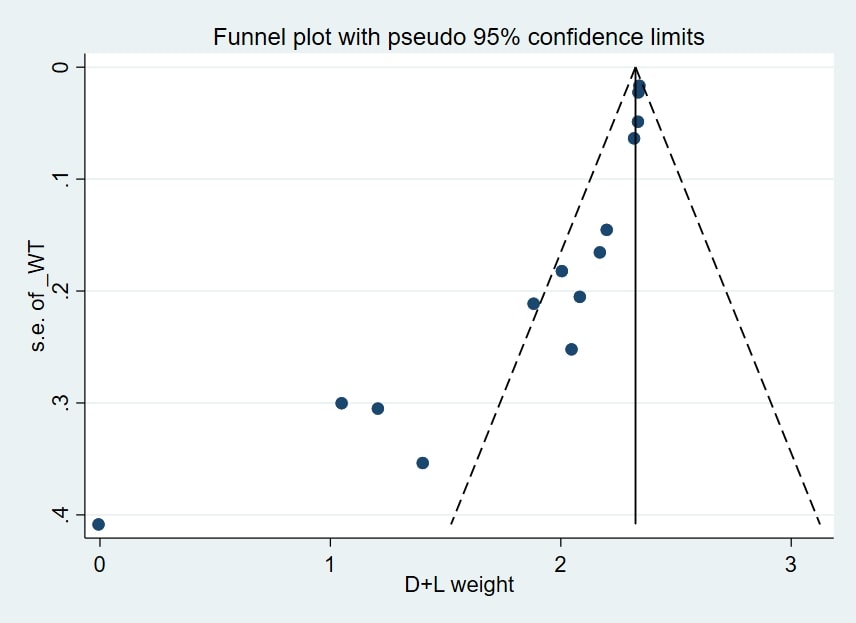 Fig. 3.
Fig. 3.
Funnel plot was used to evaluate the potential publication bias in the random-effects meta-analysis examining the link between maternal smoking habits during pregnancy and the risk of ADHD in offspring. WT, weight; s.e., standard error; D + L, dersimonian and laird.
Trim-and-fill analysis imputed 1 study on the left side, which, if included,
would have lowered the RR to 1.52 (95% CI: 1.30, 1.79, p
Our meta-analysis of 14 prospective cohort studies, with a total of 22,026 participants, demonstrates that maternal smoking during pregnancy is associated with a 1.55-fold increased risk of ADHD in offspring. This finding is consistent with the results of previous meta-analyses [36, 37, 38]. Direct measurement of cotinine levels, a metabolite of nicotine, in pregnant women during third-trimester also revealed that higher maternal nicotine levels were associated with a higher risk of ADHD in their children [35]. This association could be explained by several possible interpretations. Cigarettes smoke contains more than 4000 harmful chemicals, each of which can potentially disrupt normal fetal neurodevelopment [39]. Prenatal exposure to tobacco smoke thus represents a form of transgenerational neurotoxicity, directly impacting fetal brain development [40, 41]. Children with ADHD who were exposed to tobacco smoke in utero have been shown to exhibit a smaller cerebellum [42]. Furthermore, an animal study elucidated that maternal smoking is associated with a reduction in size and number of neurons in the hippocampus and somatosensory cortex, as well as impaired proliferation and differentiation of neuronal progenitor cells [43]. In this context, nicotine is responsible for the majority of smoking-related adverse effects. It has been found that nicotine can cross the placenta and reach the fetus, exerting direct teratogenic effects in utero [44]. Exposure to nicotine in the fetal brain leads to upregulation of nicotinic acetylcholine receptors (nAChRs), as nicotine acts as an acetylcholine agonist [45]. Another explanation is that shared nicotine exposure between mother and fetus contribute to subsequent behavioral problems in the offspring [32].
Given the high heterogeneity of the included studies, we performed a subgroup analysis stratified by study location, sample size, and the frequently adjusted confounders. The substantial heterogeneity (I2 = 96.3%) warrants further examination of its sources, which may include not only study location and sample size, but also differences in population characteristics, the ADHD assessment tool used (DSM, ICD-10, or SDQ) [16, 17, 25, 26, 27, 28, 29, 30, 31, 32, 33, 35], and variability in the confounding variables adjusted for across studies. The pooled RR of studies categorized based on location remained significant. Notably, the studies conducted in the USA exhibited the least heterogeneity and the smallest pooled RR compared to those performed in Europe and other locations. European studies displayed the highest levels of both heterogeneity and pooled RR, while studies from Australia, Brazil, and Japan ranked second. The difference between countries could be attributed to disparities in access to advanced prenatal care and the varying efforts made to prioritize pregnancy health. However, a limitation to consider is that most studies included in this meta-analysis were conducted in developed countries, specifically in Europe and North America. This geographic focus introduces a potential selection bias that limits the generalizability of our findings to populations in other regions and developing countries. Furthermore, Minatoya et al. [35] observed that mothers with limited socioeconomic support are at higher risk of continuing to smoke during pregnancy, further confirming this observation. Moreover, the association between maternal smoking and ADHD in offspring remained significant in subgroup analysis for sample size, and adjusted confounders such as maternal age, socioeconomic status, and drinking alcohol.
While our results strongly suggest an association, it is important to note that causality cannot be definitively established. Some previous studies, including a 2022 meta-analysis that examined observational studies not limited to prospective cohorts, reported no significant association between prenatal smoke exposure and ADHD [46, 47]. This inconsistency could be partially due to the differences in study design and the smaller number of included studies. However, the evidence also indicates a tendency to overlook possible moderating factors. Few studies in this field have implemented a genetic-based approach, despite the well-known confounding role of genetics in the association between maternal prenatal substance use and neurodevelopment outcomes in offspring. Studies have revealed that individuals with ADHD are significantly more likely to have nicotine dependence [48, 49], suggesting that a genetic predisposition to ADHD may be inherited from mothers who smoke. One study specifically highlighted the impact of nicotine exposure on the expression of the ADGRL3 gene, which is known to be associated with an increased risk of ADHD. Intriguingly, this effect was observed only in cells derived from adults with ADHD, further supporting the notion of a genetic link between nicotine exposure and ADHD [50].
Few studies have considered the role of maternal ADHD and its genetic transmission to the child as a potential confounding factor. This omission could influence the results and complicate the interpretation of the association between maternal smoking and ADHD in the offspring. However, we conducted subgroup analyses based on whether maternal ADHD was adjusted for, which resulted in a slight reduction in the calculated RR. For studies that accounted for maternal ADHD, the RR was 1.47 (95% CI: 1.08, 2.01) and remained statistically significant. These findings support the hypothesis that maternal smoking is related to the risk of ADHD in children, independent of its potential genetic contributions. Nonetheless, it is imperative to note that some degree of residual genetic confounding may still exist, as only a few studies (n = 3) were able to adjust for it. Future studies, especially those that utilize robust familial designs like sibling-controlled studies, will be better positioned to fully separate and evaluate the true causal effect, as they can more effectively control for shared genetic and familial environmental factors.
Furthermore, while our study did not identify alcohol consumption as a confounding factor, previous research has consistently shown an independent link between maternal alcohol consumption and behavioral difficulties in children [46]. Maitre et al.’s [51] study has also shown that while maternal smoking may be influential, it is not the sole determinant of child behavior outcomes, and additional factors include parental psychopathology, socio-economic status, paternal smoking habits, and the quality of the home environment, particularly in terms of emotional support for the child. Therefore, the association between maternal smoking and ADHD in offspring, while compelling, may be partially attributed to the combined effects of negative genetic and environmental factors.
This meta-analysis also has several limitations that should be considered. Firstly, the data collection method for assessing smoking status relied primarily on self-report and interviews. This approach introduces potential bias, as some individuals may underreport their smoking habits due to the stigma associated with smoking during pregnancy. This reliance on self-reported data, with only one study utilizing objective measures (cotinine levels), significantly increases the potential for misclassification bias, could underestimate true exposure and potentially attenuate the observed association. Secondly, there was evident variability among the studies regarding the diagnostic methods employed for ADHD. Although the selected methods (DSM, ICD-10, SDQ) all define similar symptoms for ADHD, the recommended approaches for establishing a diagnosis differ. Finally, it is essential to note that the research included in this meta-analysis primarily originated from Europe and America. Therefore, caution should be exercised when interpreting our findings and applying them to other regions or populations.
The findings of this systematic review and meta-analysis indicate that maternal smoking during pregnancy is associated with a higher risk of ADHD in the offspring. These results underscore the importance of encouraging pregnant women to quit smoking and avoid exposure to tobacco smoke.
The datasets used and analyzed during the current systematic review and meta-analysis are entirely derived from the published literature. All data supporting the findings of this study are available within the article and its supplementary information files, including the included studies’ characteristics and aggregated outcome data.
Writing—Original Draft Preparation, Conceptualization and Study Design: FZ, FAB, QB, RD, AA, RHZ, ND. Literature Search, Screening, and Data Extraction: FZ, FAB. Methodology and Statistical Analysis: ND, QB. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to express our sincere gratitude to all individuals who provided support and assistance during the completion of this systematic review. The authors would like to thank Dr. Vikas Malhotra for his valuable contributions during manuscript preparation, and Mr. Reza Parsaee for his assistance in strengthening the study through his academic input in the field of reproductive medicine.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG45653.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.