




 , Haihua Lin 1,†, Yanfen Liao 2,*
, Haihua Lin 1,†, Yanfen Liao 2,*
1 Department of Continuing Nursing Service, The First Affiliated Hospital of Jinan University, 510630 Guangzhou, Guangdong, China
2 Department of Fetal Medicine, The First Affiliated Hospital of Jinan University, 510630 Guangzhou, Guangdong, China
†These authors contributed equally.
Abstract
The health benefits of exclusive breastfeeding (EBF) are well established; however, adherence to recommended durations remains suboptimal. This study investigates how maternal breastfeeding self-efficacy (SE), postpartum depressive symptoms, and perceived social support interact to influence EBF duration, providing evidence to guide comprehensive interventions.
This prospective cohort study included 312 postpartum women and divided them into tertiles based on their scores on the Breastfeeding Self-Efficacy Scale (BSES): low (n = 83), moderate (n = 122), and high (n = 107). EBF duration was analyzed using Kaplan–Meier survival curves and Cox proportional hazards regression models. Postpartum depression, measured by the Edinburgh Postnatal Depression Scale (EPDS), was evaluated as a mediator using bootstrap mediation analysis, while perceived social support, assessed by the Personal and Social Performance Scale (PSP), was examined as a moderator through interaction analysis.
Median EBF duration was 5.6 months in the low SE group, 5.8 months in the moderate SE group, and was not reached (>6 months) in the high SE group (log-rank p < 0.001). When BSES was modeled categorically, higher breastfeeding self-efficacy was associated with a reduced hazard of discontinuing EBF (high tertile vs. low tertile: hazard ratio [HR] = 0.55, 95% confidence interval [CI]: 0.39–0.78, p = 0.001). Mediation analysis indicated a significant indirect effect of SE on EBF duration through EPDS (indirect effect: –0.18, 95% CI: –0.24 to –0.12), accounting for approximately 40% of the total association between SE and breastfeeding duration. The interaction between BSES and Postpartum Social Support Scale (PSP) was statistically significant (HR for interaction = 0.97, 95% CI: 0.95–0.99, p = 0.030). Stratified analyses showed that the protective association between higher BSES and sustained EBF was strongest among women reporting higher perceived social support.
Maternal SE is associated with prolonged EBF, partly through its association with reduced postpartum depressive symptoms. Perceived social support independently promotes EBF persistence and strengthens the beneficial association between SE and breastfeeding duration. Integrated interventions that foster maternal confidence, identify and manage postpartum mood disturbances, and mobilize social support networks are recommended.
Keywords
- breastfeeding SE
- EBF
- postpartum depression
- social support
- mediation-moderation
Exclusive breastfeeding (EBF) plays a crucial role in supporting infant growth, strengthening immune function, and promoting maternal well-being, offering benefits such as reduced maternal cancer risk and improved postpartum recovery [1, 2]. Despite broad recognition of its benefits, maintaining EBF for the full six months recommended by the World Health Organization (WHO) remains uncommon worldwide. Early cessation not only diminishes these health benefits but also highlights ongoing challenges in breastfeeding promotion [3]. Previous research has primarily focused on the socioeconomic and clinical determinants of breastfeeding [4]. More recently, however, attention has shifted toward psychological and social factors—such as maternal confidence, emotional well-being, and the presence of supportive networks—which are equally vital for sustaining breastfeeding [5, 6, 7]. Yet, an integrative framework that examines these factors collectively, rather than in isolation, to elucidate how self-efficacy (SE), mental health, and social context jointly influence maternal feeding behaviors remains lacking [8].
Postpartum depression represents a particularly important component of this framework. Depressive symptoms may diminish motivation, deplete coping resources, and weaken the mother–infant bond, thereby shortening breastfeeding duration [9]. Although associations between depression and early weaning have been well documented [10], less is known about whether depressive symptoms partially mediate the relationship between maternal confidence and breastfeeding persistence. Concurrently, social support—long recognized as a buffer against stress and a reinforcer of health-promoting behaviors [11]—may amplify the influence of SE on breastfeeding outcomes. However, this hypothesis has rarely been examined using quantitative approaches. Without addressing these gaps, it remains difficult to design interventions that operate on multiple levels: enhancing maternal confidence, improving emotional well-being, and leveraging social resources to sustain breastfeeding [12].
Theoretical models of health behavior emphasize the dynamic interplay between cognitive beliefs, emotional states, and contextual supports [13]. Within the breastfeeding literature, SE theory posits that a mother’s belief in her ability to breastfeed successfully enhances her resilience when challenges arise and supports more effective emotional regulation [14]. As a key affective factor, postpartum depression may act as a mediator by diminishing motivation and impairing coping strategies, thereby directly reducing breastfeeding duration. Although this conceptual pathway is theoretically plausible, it remains underexplored in large prospective cohorts [15]. Similarly, social support frameworks propose that emotional, informational, and practical assistance can strengthen SE and buffer stress, yet empirical evidence for its moderating role in breastfeeding duration remains limited to small-scale or cross-sectional studies.
To bridge these gaps, we conducted a prospective cohort study with three primary objectives: (1) to estimate the effect of breastfeeding SE on EBF duration using survival and hazard models; (2) to test whether postpartum depression mediates this association; and (3) to evaluate whether perceived social support moderates the effect of SE. By integrating cognitive, emotional, and contextual predictors into a unified analytic framework, this study seeks to inform comprehensive, and multidimensional strategies to support sustained EBF.
Inclusion criteria were as follows: (1) age between 18 and 45 years; (2) term
delivery (gestational age
Data collection included administration of the BSES [16], the Edinburgh
Postnatal Depression Scale (EPDS) [17, 18, 19], and the Personal and Social
Performance Scale (PSP) [20], conducted by trained nursing staff. In this study,
the BSES, EPDS, and PSS demonstrated good internal consistency, with Cronbach’s
The BSES is a 14-item instrument that measures mothers’ confidence in their ability to breastfeed. Each item is rated on a 5-point Likert scale (1 = not at all confident to 5 = always confident), producing a total score range of 14–70, with higher scores indicating stronger SE. The EPDS is a 10-item questionnaire evaluating mood over the past seven days, with each item scored from 0 to 3 (total score range: 0–30), where higher scores reflect more severe depressive symptoms. The PSS evaluates perceived emotional, informational, and practical support using four items, each rated on a 7-point Likert scale, yielding total scores from 1 to 100; higher scores indicate stronger perceived support. Sociodemographic and clinical characteristics were also collected.
Follow-up assessments were conducted at 1, 3, and 6 months postpartum via telephone interviews, during which EBF duration was recorded by the same investigator to ensure consistency (Fig. 1).
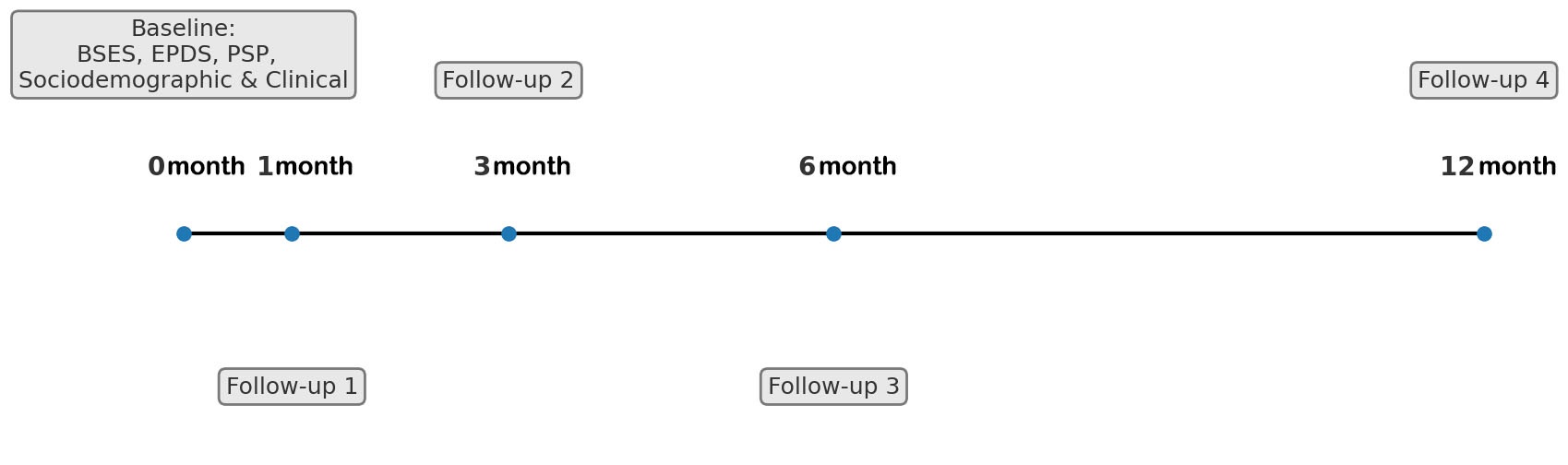 Fig. 1.
Fig. 1.
Timeline of data collecting. The timeline details the postnatal assessment schedule. Baseline (0 month) measures (postpartum days 4–7) included BSES, PSP (social support), EPDS (depression), and demographics. Follow-up assessments (at 1 month, 3 months, 6 months, and 12 months) tracked EBF status and duration via telephone interview. The 6 mo time point served as the primary censoring point for the outcome. BSES, Breastfeeding Self-Efficacy Scale; EPDS, Edinburgh Postnatal Depression Scale; PSP, Postpartum Social Support Scale.
Baseline variables included maternal age, pre-pregnancy body mass index (BMI), parity, education, marital status, employment, and smoking history. Clinical variables included delivery mode, gestational age, birthweight, and breastfeeding intent. EBF was defined per WHO criteria as feeding the infant only breast milk without supplemental formula, liquids, or solids. Time-to-event was the age in months at cessation.
Statistical analysis was performed using SPSS (Version 26.0, IBM Corp., Armonk,
NY, USA) and R 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Baseline characteristics were compared across groups to confirm comparability.
Baseline continuous variables were summarized as mean
To ensure comparability across groups, we first examined baseline
characteristics among the low (n = 83), mid (n = 122), and high (n = 107) SE
cohorts (Table 1). Baseline characteristics differed significantly across SE
groups in age, pre-pregnancy BMI, parity, education, EPDS, PSP scores, and
breastfeeding intent (all p
| Characteristic | Low SE (n = 83) | Mid SE (n = 122) | High SE (n = 107) | Test statistic | p-value | |
| Age (years), mean |
28.5 |
29.7 |
30.2 |
F = 3.94 | 0.020 | |
| Pre-pregnancy BMI (kg/m2), mean |
24.8 |
23.9 |
23.2 |
F = 3.29 | 0.040 | |
| Parity | χ2 = 9.21 | 0.010 | ||||
| Primipara, n (%) | 45 (54%) | 55 (45%) | 38 (36%) | |||
| Multipara, n (%) | 38 (46%) | 67 (55%) | 69 (64%) | |||
| Mode of delivery | χ2 = 0.04 | 0.980 | ||||
| Vaginal, n (%) | 60 (72%) | 88 (72%) | 78 (73%) | |||
| Cesarean, n (%) | 23 (28%) | 34 (28%) | 29 (27%) | |||
| Gestational age (weeks), mean |
39.1 |
39.0 |
39.2 |
F = 0.30 | 0.750 | |
| Infant birthweight (g), mean |
3220 |
3280 |
3310 |
F = 1.21 | 0.300 | |
| Education | χ2 = 25.1 | |||||
| 50 (60%) | 49 (40%) | 27 (25%) | ||||
| 33 (40%) | 73 (60%) | 80 (75%) | ||||
| Marital status | χ2 = 1.60 | 0.450 | ||||
| Married, n (%) | 80 (96%) | 118 (97%) | 105 (98%) | |||
| Unmarried, n (%) | 3 (4%) | 4 (3%) | 2 (2%) | |||
| Employment status | χ2 = 2.40 | 0.300 | ||||
| Employed, n (%) | 55 (66%) | 85 (70%) | 80 (75%) | |||
| Unemployed, n (%) | 28 (34%) | 37 (30%) | 27 (25%) | |||
| Smoking status | χ2 = 4.60 | 0.100 | ||||
| Yes, n (%) | 10 (12%) | 8 (7%) | 5 (5%) | |||
| No, n (%) | 73 (88%) | 114 (93%) | 102 (95%) | |||
| Breastfeeding intent | χ2 = 18.25 | |||||
| High, n (%) | 20 (24%) | 30 (25%) | 50 (47%) | |||
| Medium, n (%) | 40 (48%) | 60 (49%) | 40 (37%) | |||
| Low, n (%) | 23 (28%) | 32 (26%) | 17 (16%) | |||
| EPDS score, mean |
12.5 |
9.1 |
6.8 |
F = 110.50 | ||
| PSP, mean |
45.2 |
52.3 |
58.9 |
F = 85.12 | ||
Note: BMI, body mass index; SE, self-efficacy.
Kaplan–Meier analysis demonstrated a statistically significant difference in
EBF duration among the three SE groups (Fig. 2; Log-rank p
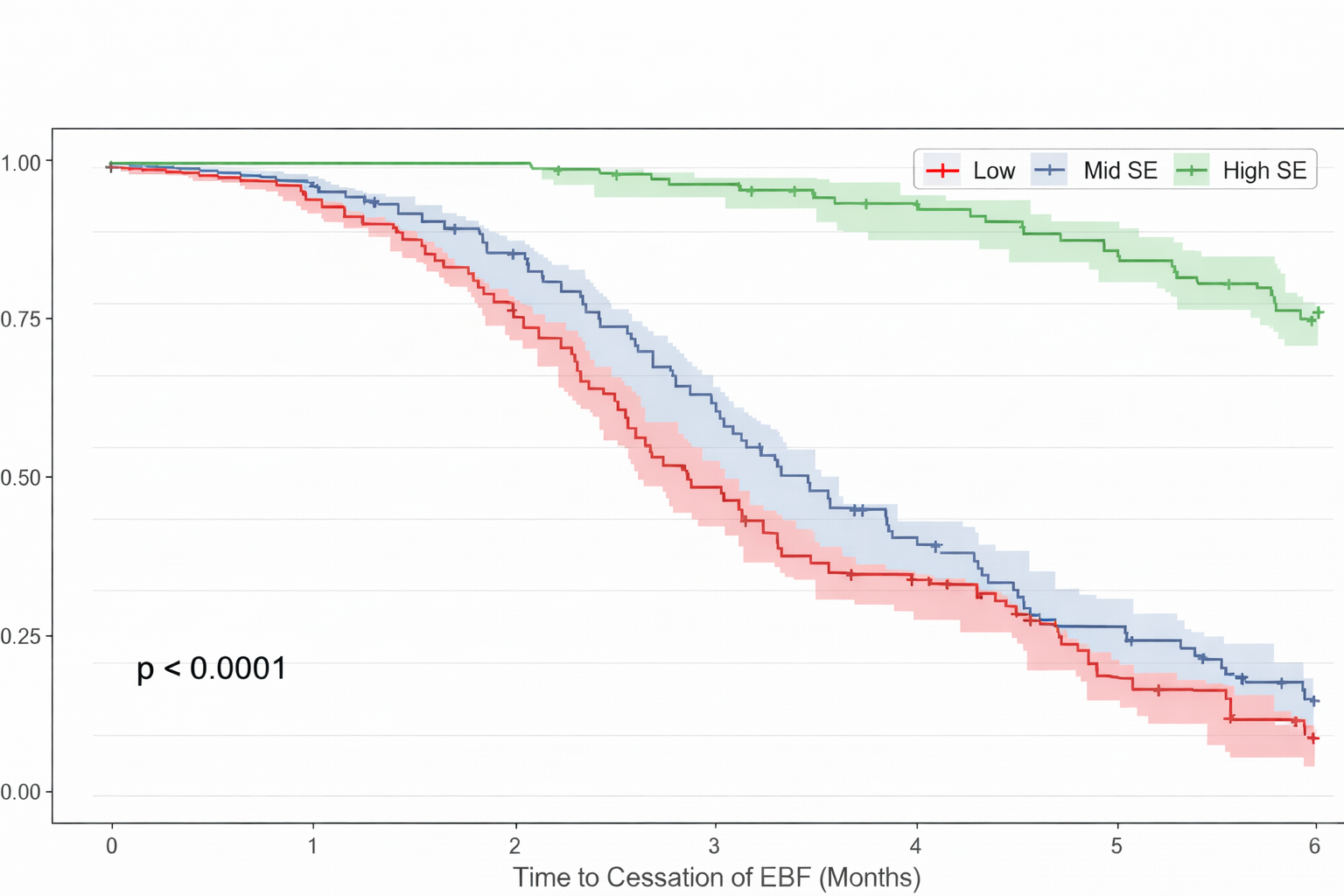 Fig. 2.
Fig. 2.
Breastfeeding survival probability over time stratified by SE groups.
| Group | Median duration (months) | Log-rank statistic (χ2) | Log-rank p-value |
| Low SE group | 5.6 | - | - |
| Mid SE group | 5.8 | - | - |
| High SE group | χ2 = 30.70 |
| Variable | HR (95% CI) | p-value | |
| BSES, tertiles | |||
| Low (ref) | 1.00 | - | |
| Medium | 0.72 (0.53–0.98) | 0.038 | |
| High | 0.55 (0.39–0.78) | 0.001 | |
| EPDS, tertiles | |||
| Low (ref) | 1.00 | - | |
| Medium | 1.28 (0.94–1.74) | 0.110 | |
| High | 1.75 (1.28–2.38) | ||
| PSP, tertiles | |||
| Low (ref) | 1.00 | - | |
| Medium | 0.80 (0.59–1.09) | 0.160 | |
| High | 0.60 (0.44–0.83) | 0.002 | |
Note: Models adjusted for baseline characteristics with significant inter-group differences: maternal age, pre-pregnancy BMI, parity, education, and breastfeeding intent (EPDS and PSP are included as primary variables of interest). CI, confidence interval; HR, hazard ratio.
To explore whether postpartum depression mediated the self-efficacy effect, we
conducted a bootstrap mediation analysis. Results demonstrated a significant
indirect effect of BSES via EPDS (–0.18; 95% confidence interval [CI]: –0.24
to –0.12; p
| Path | Estimate | SE | 95% CI |
| SE |
–0.45 | 0.05 | –0.55 to –0.35 |
| SE |
–0.18 | 0.03 | –0.24 to –0.12 |
| SE |
–0.27 | 0.06 | –0.39 to –0.15 |
Finally, we evaluated social support as a moderator of the SE effect. The
interaction term BSES
| Variable | HR (95% CI) | p-value |
| BSES (continuous) | 0.87 (0.82–0.92) | |
| Social support (PSP, continuous) | 0.94 (0.90–0.98) | 0.010 |
| BSES × PSP interaction | 0.97 (0.95–0.99) | 0.030 |
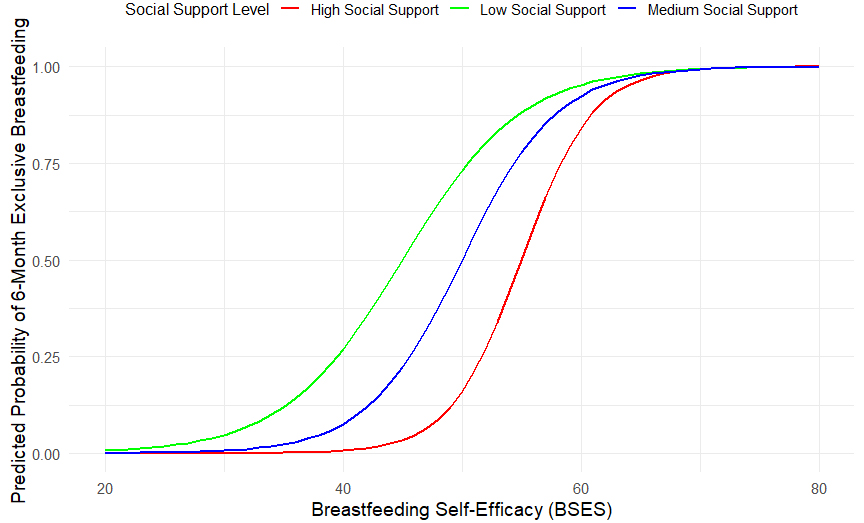 Fig. 3.
Fig. 3.
Predicted probability of 6-month EBF by BSES under low (–1 SD) and high (+1 SD) social support.
Subgroup analyses by social support (stratified at mean
| Social support level | Score range | n | Events (discontinuation within 6 mo) | Events (%) | HR (per 10-point BSES) (95% CI) | p-value |
| Low ( |
50 | 38 | 76.0% | 0.95 (0.88–1.02) | 0.150 | |
| Medium (mean |
43.6–61.8 | 212 | 98 | 46.2% | 0.88 (0.82–0.95) | 0.001 |
| High ( |
50 | 12 | 24.0% | 0.80 (0.72–0.89) |
Note: Events represent the number of mothers who discontinued EBF prior to the 6-month censoring point.
SE postpartum depression, and social support were strongly associated with breastfeeding duration. Higher SE was linked to longer breastfeeding persistence [21], while postpartum depression partially mediated this association [22]. Moreover, every 10-point increase in social support was associated with approximately a 25% improvement in breastfeeding outcomes [23]. In summary, to prolong EBF duration, nursing staff should aim not only to enhance mothers’ SE but also support their emotional well-being and strengthen their social support networks.
Our findings demonstrated that each one-point increase in the BSES score was
associated with a 15% reduction in the risk of breastfeeding cessation. Mothers
with high SE exclusively breastfed for an average of 6.8 months, compared with
only 3.2 months among those with low SE (HR = 0.85; 95% CI: 0.80–0.90;
p
Clinical nursing interventions aimed at enhancing new mothers’ confidence, expanding their social networks, and alleviating postpartum depressive symptoms could therefore be effective in promoting sustained breastfeeding. One potential explanation is that mothers with higher SE are more likely to develop coping strategies to overcome feeding challenges, thereby maintaining lactation [24]. This aligns with Bandura’s theory of SE [25] and with prior research emphasizing the central role of psychological resources in sustaining long-term EBF [26].
Bootstrap mediation analysis further supported these mechanisms, showing that postpartum depression significantly mediated the relationship between SE and breastfeeding continuation, accounting for approximately 40% of the total effect [27]. These findings suggest that women with lower SE may be more vulnerable to postpartum depression, which in turn increases the likelihood of early breastfeeding cessation [28, 29]. Depressive symptoms may hinder mothers’ ability to cope with breastfeeding-related difficulties and diminish their motivation. Consistent with a previous study reporting an association between postpartum depression and premature weaning [30], our results provide quantitative evidence of this mediating pathway.
Furthermore, we observed a significant interaction between BSES and PSS (HR = 0.97; 95% CI: 0.95–0.99; p = 0.030; Table 5), indicating that the positive effects of SE on six-month EBF were amplified among mothers with higher levels of social support [27]. Although social support independently reduced the risk of breastfeeding cessation within six months by 6% (HR = 0.94 per unit increase), its influence was particularly pronounced among mothers with high SE. Positive social support appeared to enhance EBF duration both directly and indirectly, by reinforcing maternal confidence and by strengthening internal coping resources.
Social support is thought to provide informational, emotional, and practical assistance through interpersonal connections, thereby reinforcing mothers’ internal capacity to overcome challenges. Mothers with both high SE and high social support sustained breastfeeding for significantly longer periods. The moderating effect of social support suggests that mothers in highly supportive environments derive greater benefit from SE compared with those in less supportive settings. In this context, social support functions as both a mediator and a moderator, transmitting and amplifying the protective effects of SE. These findings support the resource-buffer theory and the socioecological model of feeding behavior [29, 31], consistent with previous evidence that family and community support improve breastfeeding outcomes [32].
As this was a single-center observational study, generalizability may be limited due to insufficient participant heterogeneity. Additionally, measures of SE, postpartum depression, and social support were based on self-report questionnaires and therefore may be subject to bias, despite efforts to control for potential confounding factors during the study design. Although adjustments were made for potential confounding factors such as age, pre-pregnancy BMI, parity, education level, economics status, and professional income, the influence of other unmeasured or unascertainable factors on the outcomes cannot be ruled out. We did not account for maternal occupational or household factors, which may influence their SE and feeding behaviors. Furthermore, the 6-month follow-up period limited the assessment of longer breastfeeding outcomes, potentially leading to an underestimation of the protective effect of social support and sustained breastfeeding.
This study described the independent and interactive effects of maternal breastfeeding SE, postpartum depression, and social support on EBF duration. Results indicated that each one-point increase in maternal SE was associated with a 13% reduction in the risk of discontinuing EBF, and mothers in the high-SE group had more than double the median EBF durations compared with those in the low SE group. Emotional well-being partially mediated this relationship , accounting for 40% of SE on EBF. Additionally, social support not only directly helped EBF maintenance, but also amplified the effect of protective effect of SE, offering recommendations for combination with increasing of SE, detection and assistance of postpartum mood, and building assistance network for prolonging EBF duration.
Clinical trial data cannot be shared publicly due to patient privacy but are available upon reasonable request from the corresponding author after signing a Data Use Agreement and approval by the Ethics Committee.
ZC and HL conceived and designed the experiments. ZC, HL, and YL performed the experiments. ZC and HL analyzed the data. All authors contributed materials/analysis tools. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Jinan University (approval number: KY-2024-075).
Not applicable.
Funding Project: Nursing Research Special Fund of the First Clinical School of Jinan University in 2023 (802302).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG45587.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.