










 , Huan Mao 3, Ying Dai 2,4, Lu Luo 1,2, Mingming Wang 1,2, Yinqin Zhong 2,5,*
, Huan Mao 3, Ying Dai 2,4, Lu Luo 1,2, Mingming Wang 1,2, Yinqin Zhong 2,5,*
1 Department of Operating Room, Shenzhen Hospital (Futian) of Guangzhou University of Chinese Medicine, 518034 Shenzhen, Guangdong, China
2 6th Clinical Medical College, Guangzhou University of Chinese Medicine, 518034 Shenzhen, Guangdong, China
3 Faculty of Nursing, Guangzhou University of Chinese Medicine, 518034 Shenzhen, Guangdong, China
4 Hemodialysis Center, Shenzhen Hospital (Futian) of Guangzhou University of Chinese Medicine, 518034 Shenzhen, Guangdong, China
5 Department of Nursing, Shenzhen Hospital (Futian) of Guangzhou University of Chinese Medicine, 518034 Shenzhen, Guangdong, China
Abstract
Perioperative hypothermia and shivering are common in patients undergoing cesarean section; however, the effectiveness of active warming (AW) compared to passive warming (PW) in preventing perioperative outcomes for pregnant females and their offspring remains controversial.
A search was performed for randomized controlled trials (RCTs) on the impact of AW devices on perioperative hypothermia in mothers undergoing cesarean section in the Cochrane Library, PubMed, Embase, and Web of Science databases (inception–October 2024). Two researchers independently screened studies and performed a meta-analysis using Review Manager 5.4.
A total of 12 articles were included, encompassing 1184 patients. The meta-analysis results indicated that AW devices can mitigate the decrease in core body temperature in cesarean section mothers postoperatively (mean difference [MD] = 0.26, 95% confidence interval [CI]: (0.10, 0.43); p = 0.002), reduce the incidence of hypothermia (relative risk [RR] = 0.69, 95% CI: (0.60, 0.80); p < 0.00001), and decrease the occurrence of shivering (RR = 0.54, 95% CI: (0.40, 0.74); p = 0.0001.
This meta-analysis demonstrates that AW devices effectively mitigate perioperative hypothermia in patients undergoing cesarean section, reducing hypothermia and shivering incidence and improving temperature management.
The study has been registered on https://www.crd.york.ac.uk/prospero/ (registration number: CRD42024592013; registration link: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024592013).
Keywords
- active warming
- cesarean section
- inadvertent perioperative hypothermia
Body temperature is one of the vital signs of human life, and its stability is fundamental for maintaining the normal functioning of various physiological processes in the body [1]. Inadvertent perioperative hypothermia (IPH) refers to the unintentional decrease in body temperature that occurs during surgery under anesthesia, which is one of the common complications in anesthesia and surgical procedures [2]. Cesarean section, as a method to resolve dystocia and maternal and neonatal complications, has been widely recognized for its safety. Over the past 20–30 years, the rate of cesarean sections has been steadily increasing in many countries, including both developed and developing nations. In the United States, a developed country, the rate rose from 23% in 2000 to 31.7% in 2019 [3]; in Brazil, a developing country, it increased from 38.02% in 2000 to 55.9% in 2018 [4] and in China, it rose from 28.8% in 2008 to 34.9% in 2019 [5]. Females undergoing cesarean sections represent a surgical population that is particularly prone to intraoperative hypothermia, with a study indicating that the incidence of low body temperature during cesarean sections can be as high as 38% to 75% [6]. Intraoperative hypothermia during cesarean sections can increase the incidence of perioperative complications, raise the rate of surgical site infections, disrupt coagulation function, prolong the duration of action of anesthetic drugs, and reduce the secretion of pituitary prolactin. Decreased prolactin can affect the successful breastfeeding of newborns and may also impact their birth outcomes, increasing the incidence and mortality rates of neonates [7].
As research into standardized perioperative temperature management progresses, an increasing number of warming devices and measures are being applied in clinical practice. However, there is currently a lack of routine temperature monitoring for patients, and the prevention and management of this issue is in urgent need of improvement. Temperature protection measures are often limited to passive warming (PW) methods, such as covering with cotton blankets and adding surgical drapes; whereas the effectiveness of active warming (AW) devices, such as forced-air warming (FAW), conductive heating pads, circulating water mattresses, and radiant heaters, remains a matter of debate in clinical practice [8]. A study by Shaw et al. [9] have shown that AW devices can significantly reduce the incidence of hypothermia in perioperative patients; however, a systematic review by Li and colleagues [5] indicated that there was no difference in the incidence of hypothermia and shivering between patients with and without FAW devices.
Therefore, the aim of this study is to systematically analyze the results of randomized controlled trials (RCTs) on the intervention of AW devices for hypothermia in cesarean section patients during the perioperative period, both domestically and internationally. The goal is to further explore the efficacy of AW devices and to provide evidence-based support for their clinical application.
The study has been registered on https://www.crd.york.ac.uk/prospero/ (registration number: CRD42024592013; registration link: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024592013).
① Study Type: RCTs in both Chinese and English.
② Study Subjects: Patients aged 18 years or older who have chosen to undergo cesarean section.
③ Intervention Measures: The experimental group received AW devices, including FAW, conductive heating pads, circulating water mattresses, and radiant heaters, while the control group received routine warming methods, such as cotton blankets and woolen blankets.
④ Outcome Measures: The primary outcome is core body temperature at the end of surgery or upon arrival in the post-anesthesia care unit (PACU), as well as the incidence of hypothermia (Core body temperature below 36 °C) [10]. Secondary outcomes include the incidence of shivering and thermal comfort. Core body temperature is measured using tools such as oral thermometers, infrared tympanic thermometers, temporal artery scanners, bladder temperature sensing catheters, and rectal thermometers.
① No available full text, no data articles and studies with excessively low quality.
② Case reports, reviews, dissertations, and other literature that are duplicate publications, or secondary analyses.
Computer-assisted searches were conducted in databases such as PubMed, The Cochrane Library, Web of Science, Embase to collect RCTs on AW devices for hypothermia in cesarean section patients during the perioperative period, with the search period being from the inception of the database to October 2024. Search Strategy: The search strategy was determined based on the (patient, intervention, comparison, outcome) PICO principle, with main search terms including Cesarean Section, Post Cesarean Section, and Heating. All searches combined subject headings with free-text words, and the search strategy was finalized after several pre-searches. Expanded Search: Hand searches and gray literature database searches were conducted, searching for relevant databases of ongoing trials (clinical trial registries), databases related to clinical practice guidelines, public search engines, and tracing references. Hand searches of published journals and searching for relevant conference information were performed to comprehensively collect clinical trials that meet the inclusion criteria. The specific search history is shown in Supplementary Table 1.
Literature was screened based on the pre-established inclusion criteria, and duplicate documents in the databases were removed by Zotero (version 7.0.0; Corporation for Digital Scholarship, Vienna, VA, USA). The titles and abstracts of the obtained literature were read to preliminarily exclude documents that clearly did not meet the inclusion criteria. Full texts of potentially eligible documents were reviewed, and data was extracted from documents that met the inclusion criteria. If there was any doubt about a document, a decision was made after contacting the original author to obtain relevant information or after analysis and evaluation. The “snowball” method was used to trace the references cited in the included documents. All steps were independently conducted by two evaluators, with cross-checking. Disagreements were resolved through discussion or by seeking the opinion of a third party.
The methodological quality of the included studies were evaluated using the “Risk of Bias Assessment” tool recommended by the Cochrane Handbook 5.0, which includes: ① Randomization process, the method used to generate the random sequence; ② Allocation, the implementation of the allocation concealment; ③ Blinding, whether blinding methods were used; ④ Completeness of outcome data; ⑤ Selective reporting of study results; ⑥ Presence of other sources of bias. The assessment results were identified as “low risk”, “high risk”, or “unclear”. The evaluation levels were divided into three categories: A (all items are at low risk), B (some items are at low risk), and C (no items are at low risk). Studies with a grade of C were excluded.
Data were analyzed using the Review Manager 5.4. (Cochrane Collaboration,
Oxford, UK) Software for Meta-analysis. Because not all studies reported every
endpoint, the number of trials and participants contributing to each
meta-analysis varies; we reported the sample size per outcome. Binary data such
as the incidence of hypothermia and shivering were expressed using the relative risk
(RR) and 95% confidence interval (CI). Heterogeneity among studies was assessed
using the chi-squared test and the I2 statistic. When there was
statistical homogeneity among the studies (p
A total of 440 articles were initially identified. After a step-by-step screening process, 12 RCTs [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22] were ultimately included, involving a total of 1184 patients. The literature screening process and results are shown in Fig. 1.
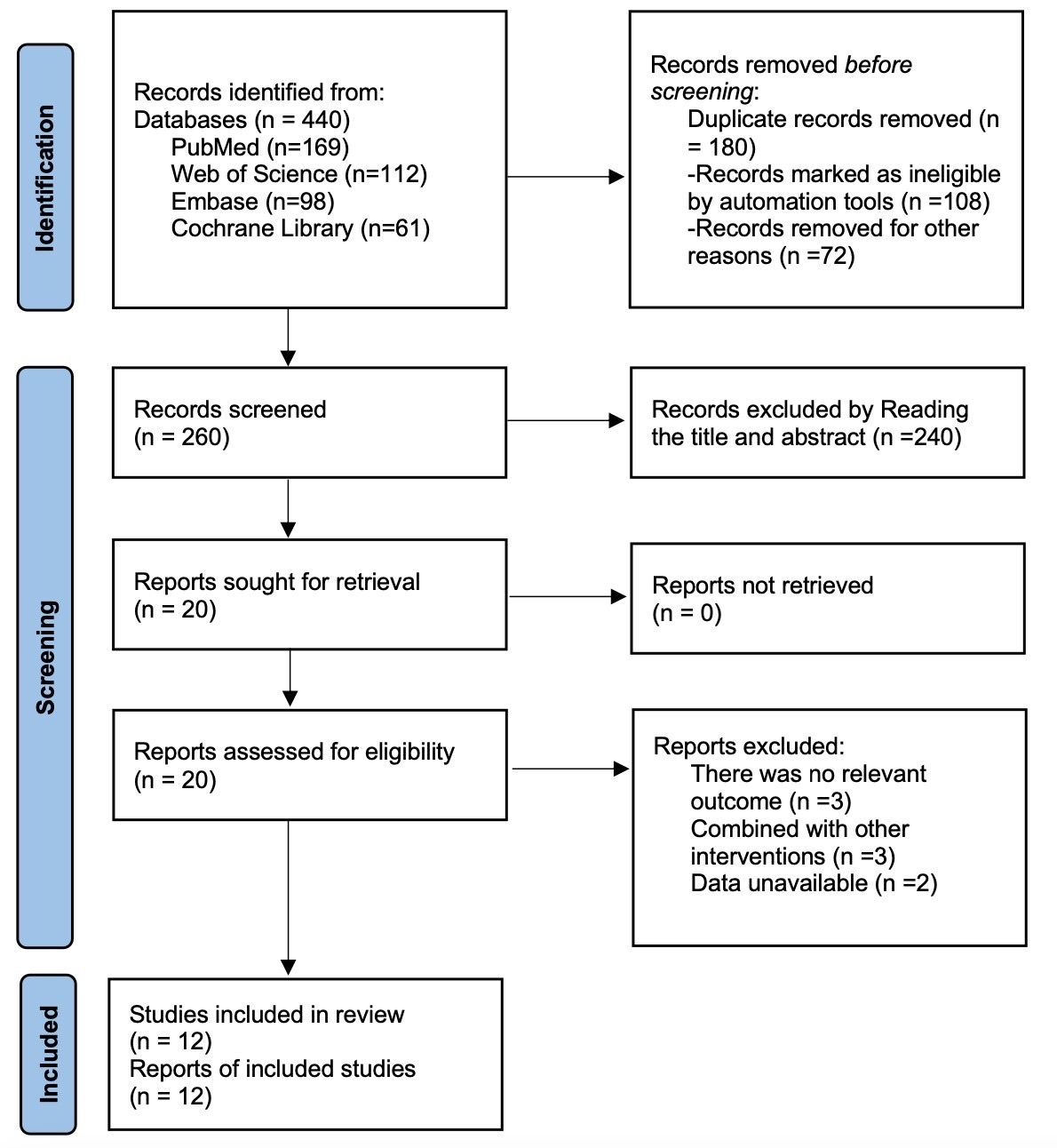 Fig. 1.
Fig. 1.
Literature search flow chart.
The basic characteristics of the included studies are presented in Table 1 (Ref. [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22]). The included literature encompasses studies from the United States, the United Kingdom, Germany, Canada, South Korea, and other countries, with a total of 1184 patients across the included studies, of which 591 were in the experimental group and 593 in the control group. 9 articles provided detailed reports on randomization methods, 11 articles described the concealment of the allocation sequence, 6 articles described how blinding was implemented for the study subjects and interventionists, and 4 articles introduced blinding for outcome assessors. The specific results of the risk of bias assessment for the included studies are shown in Fig. 2. In this study, grade rating was used for analysis. The results of the analysis (Table 2) suggested that the results of surgery/core temperature at the time of PACU entry, incidence of hypothermia, and incidence of shivering were of low quality.
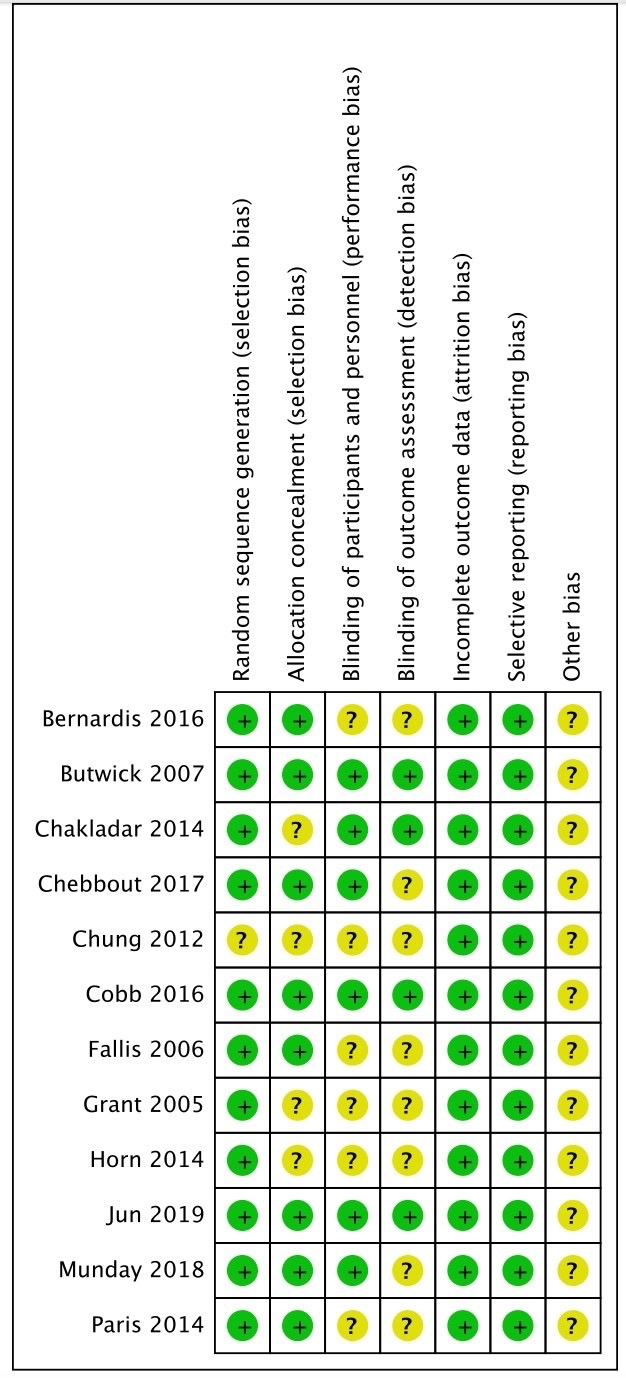 Fig. 2.
Fig. 2.
Risk bias of graph.
| First author | Country | Types of anesthesia | ASA level | Measuring tools | Sample size | Intervention device | Outcome measures | ||
| Control Group | Experimental Group | Control Group | Experimental Group | ||||||
| de Bernardis 2016 [19] | Brazil | Subarachnoid block anesthesia | I, II | Infrared tympanic thermometer | 20 | 20 | Cotton blanket | FAW + Fluid warming | ①③ |
| Butwick 2007 [17] | United States | Subarachnoid block anesthesia | I, II | Oral thermometer | 15 | 15 | Cotton blanket | FAW | ②③ |
| Chakladar 2014 [21] | United Kingdom | Subarachnoid block anesthesia/Epidural block anesthesia | I, II | Temporal artery scanner | 58 | 58 | Cotton blanket | Heat conduction pad + Fluid warming | ①②③ |
| Chung 2012 [15] | South Korea | Subarachnoid block anesthesia | I, II | Infrared tympanic thermometer | 15 | 15 | Cotton blanket | Fluid warming | ③ |
| Chebbout 2017 [14] | United Kingdom | Subarachnoid block anesthesia | None | Oral thermometer | 43 | 44 | Cotton blanket | FAW | ①③ |
| Cobb 2016 [13] | United States | Subarachnoid block anesthesia | I, II | Temporal artery scanner | 22 | 22 | Cotton blanket | FAW + Fluid warming | ①②③ |
| Fallis 2006 [18] | Canada | Subarachnoid block anesthesia/Epidural block anesthesia | None | Oral thermometer | 30 | 32 | Cotton blanket | FAW | ①③ |
| Grant 2015 [12] | United States | Subarachnoid block anesthesia/Epidural block anesthesia | None | Oral thermometer | 241 | 243 | Cotton blanket | Heat conduction pad + Fluid warming | ①② |
| Horn 2014 [22] | Germany | Epidural block anesthesia | I, II | Oral thermometer | 21 | 19 | Cotton blanket | FAW | ①②③ |
| Jun 2019 [16] | South Korea | Subarachnoid block anesthesia | None | Infrared tympanic thermometer | 25 | 23 | Cotton blanket | FAW + Fluid warming | ②③ |
| Munday 2018 [20] | Australia | Subarachnoid block anesthesia | I, II | Infrared tympanic thermometer | 25 | 25 | Cotton blanket | FAW + Fluid warming | ②③ |
| Paris 2014 [11] | United States | Subarachnoid block anesthesia | None | Bladder temperature sensing catheter | 76 | 77 | Cotton blanket | Heat conduction pad | ② |
Note: ASA, American Society of Anesthesiologists; FAW, forced-air warming; ①, Core body temperature; ②, Incidence of hypothermia; ③, Incidence of shivering.
| Outcome | Number of studies | Study design | Inconsistency | Indirectness | Imprecision | Other considerations | Certainty |
| Core body temperature | 8 | Randomized controlled study | not serious | not serious | not serious | serious | Low |
| Incidence of hypothermia | 8 | Randomized controlled study | not serious | not serious | not serious | serious | Low |
| Incidence of shivering | 10 | Randomized controlled study | not serious | not serious | not serious | serious | Low |
A total of 8 studies compared the impact of AW devices on the core temperature
of cesarean section during the perioperative period, involving 1026 patients. The
results indicated significant heterogeneity among the studies. Therefore, a
subgroup analysis was conducted based on the different times of core temperature
measurement (end of surgery and upon entry to PACU). The results showed a
significant reduction in heterogeneity, but it remained substantial
(I2 = 89%, p
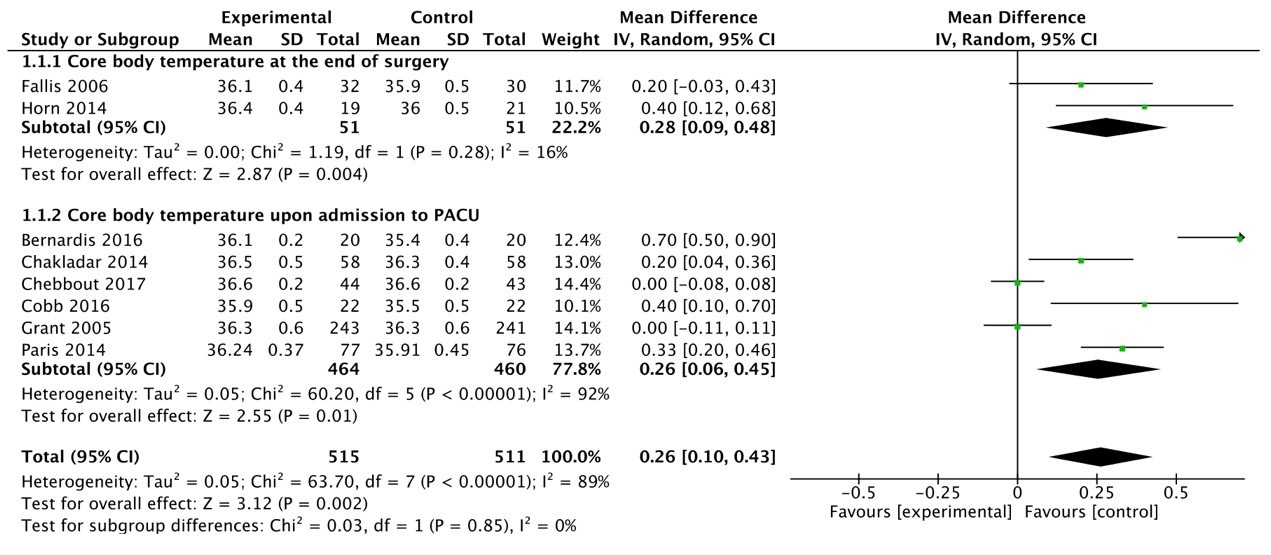 Fig. 3.
Fig. 3.
Forest plot of core temperature meta-analysis. CI, confidence interval; PACU, post-anesthesia care unit.
A total of 8 studies were included to compare the impact of AW devices on the
incidence of hypothermia in cesarean section patients during the perioperative
period, involving 965 patients. There was a certain degree of heterogeneity among
the studies (I2 = 47%, p = 0.07), hence a fixed-effects
model was selected. The results showed that the incidence of hypothermia in the
experimental group of cesarean section patients was significantly lower than that
in the control group [RR = 0.69, 95% CI: (0.60, 0.80), p
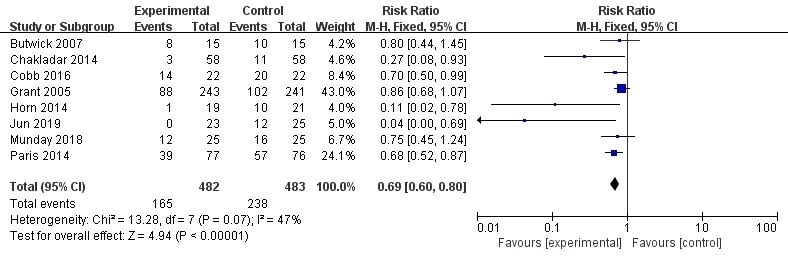 Fig. 4.
Fig. 4.
Meta-analysis forest plot fixed effects model of incidence of hypothermia. M-H, Mantel-Haenszel.
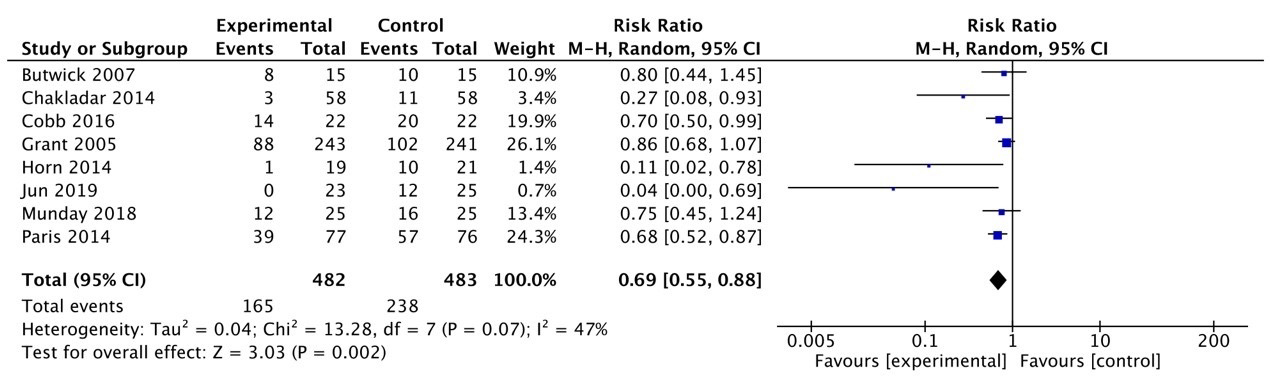 Fig. 5.
Fig. 5.
Meta-analysis forest plot random effects model of incidence of hypothermia.
A total of 10 studies were included to compare the impact of AW devices on the incidence of shivering in cesarean section patients during the perioperative period, involving 689 patients. There was low heterogeneity among the studies (I2 = 34%, p = 0.14), thus a fixed-effects model was used. The results indicated that the incidence of shivering in the experimental group of cesarean section patients was significantly lower than that in the control group [RR = 0.54, 95% CI: (0.40, 0.74), p = 0.0001]. See Fig. 6.
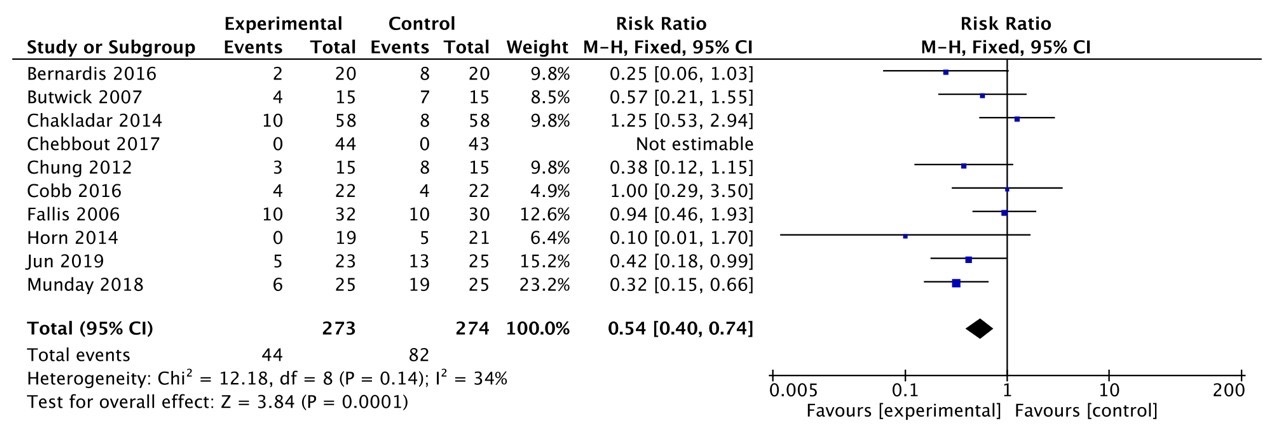 Fig. 6.
Fig. 6.
Meta-analysis forest plot fixed effects model of incidence of shivering.
Funnel plots and the Egger test were used to evaluate the publication bias of this study (Figs. 7,8,9). The results showed that core temperature at the end of surgery/core temperature at the time of PACU entry (p = 0.742), incidence of shivering (p = 0.136) suggested that the possibility of publication bias is small. The funnel plot of Incidence of Hypothermia (p = 0.001) was asymmetric, so that publication bias was more likely. The trim-and-fill results of this study suggest that there is a publication bias in the incidence of shivering and hypothermia, which does not affect this conclusion.
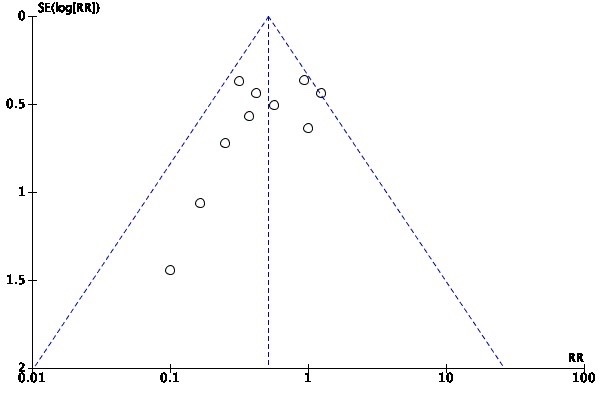 Fig. 7.
Fig. 7.
Funnel plot of the meta-analysis of core temperature at the end of surgery/core temperature at the time of post-anesthesia care unit (PACU) entry.
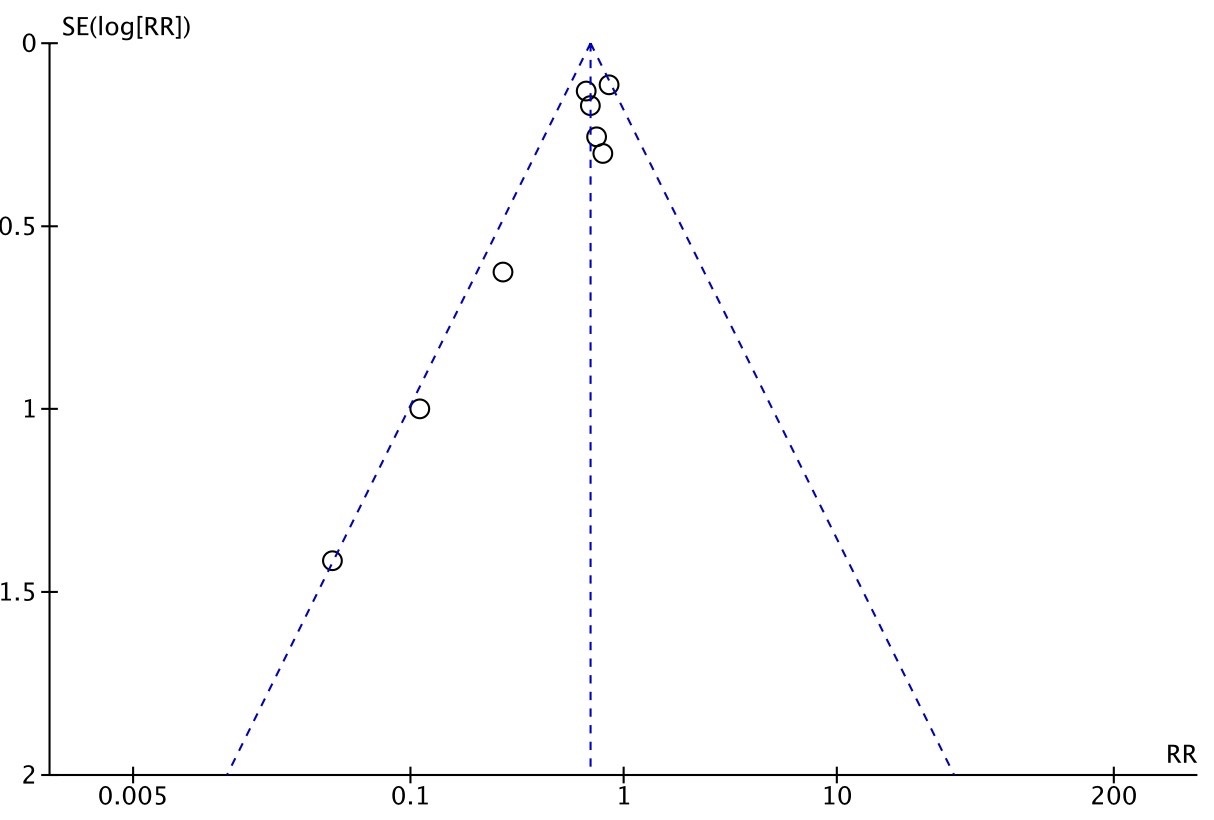 Fig. 8.
Fig. 8.
Funnel plot of the meta-analysis of incidence of hypothermia.
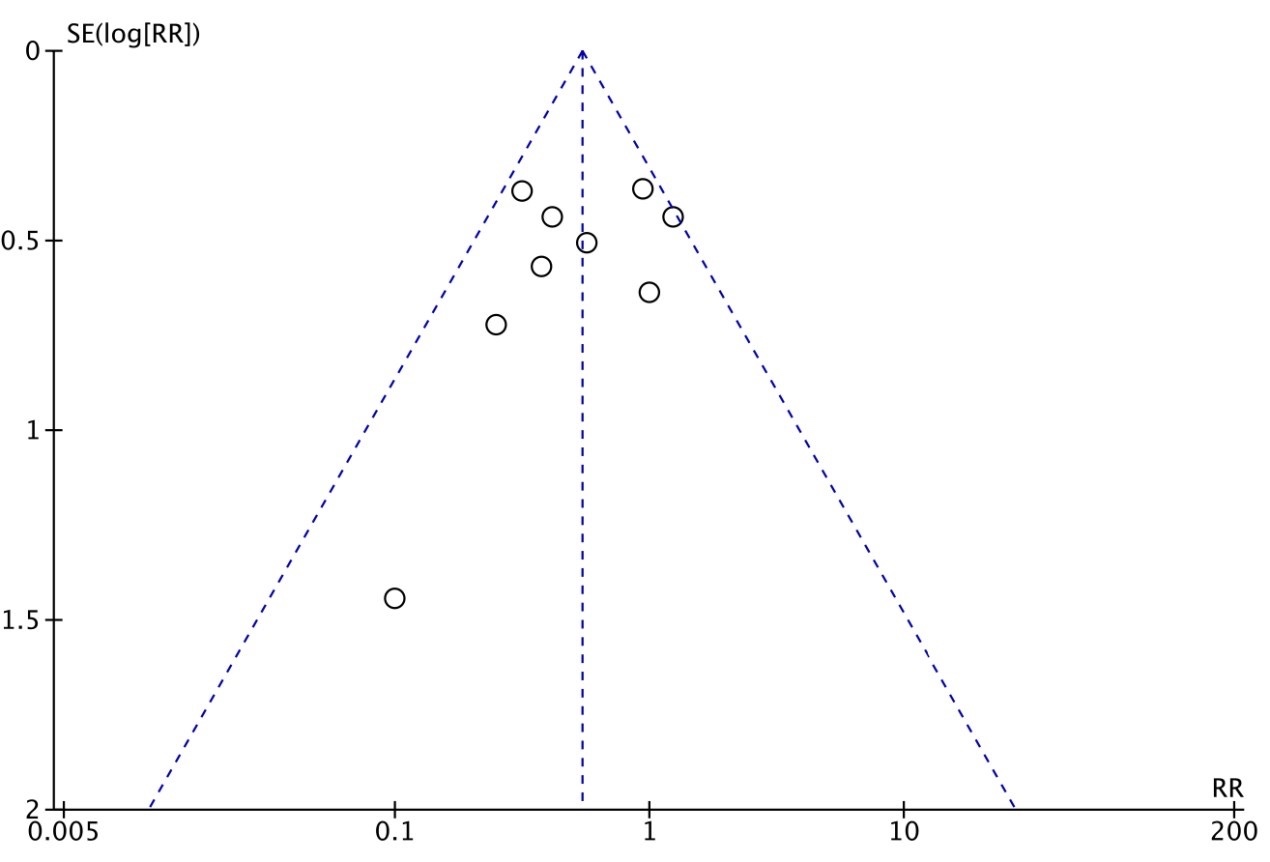 Fig. 9.
Fig. 9.
Funnel plot of the meta-analysis of incidence of shivering.
In this study, Meta regression analysis was conducted according to heating method, starting time, anesthesia method, temperature measurement site, and country. The analysis results (Table 3) suggested that the heating method, starting time, anesthesia method, temperature measurement site, and country were not the source of heterogeneity.
| Outcomes | Variable | Coef. | Standard error | p | 95% CI |
| Core body temperature | warming modality | 0.138 | 0.133 | 0.318 | [–0.147, 0.424] |
| initiation timing | 0.016 | 0.117 | 0.894 | [–0.236, 0.267] | |
| anesthesia type | 0.012 | 0.014 | 0.429 | [–0.196, 0.043] | |
| temperature measurement site | 0.076 | 0.197 | 0.591 | [–0.127, 0.753] | |
| country | 0.016 | 0.568 | 0.176 | [–0.198, 0.486] |
The constancy of body temperature is fundamental for maintaining various physiological functions. Effective monitoring and regulation of body temperature are one of the most important measures to ensure the success of surgery and anesthesia and to reduce postoperative complications [23]. The findings of this study indicate that the use of AW devices effectively maintains core body temperature in cesarean section patients during and after surgery, with significantly higher temperatures observed at the conclusion of surgery and upon arrival in the PACU compared to the control group. This helps reduce the incidence of perioperative hypothermia, improves postoperative recovery, and lowers the risk of complications such as shivering. Therefore, the application of AW devices in cesarean section surgery has clinical significance. It significantly enhances patients’ temperature management outcomes, thereby improving postoperative comfort and overall recovery. Cesarean section surgeries often use spinal anesthesia, and in special circumstances, general or local anesthesia may be used. Spinal anesthesia can lead to heat loss in patients during surgery, mainly through vasodilation and redistribution of blood, while also impairing peripheral and central thermoregulatory centers [24]. Therefore, during major or prolonged surgeries under spinal anesthesia, patients may experience severe hypothermia. The results of this meta-analysis show that the core temperature of the experimental group after surgery/upon entry to PACU is higher than that of the control group, and the incidence of hypothermia is lower than that of the control group, consistent with the results of the study by Mackeen et al. [25]. AW devices mainly provide additional heat for active insulation, with air warming and fluid warming being the two most common types. Air warming increases skin temperature through peripheral conduction and convection, while fluid warming increases skin temperature through peripheral and central conduction, which is related to the distribution of fluid throughout the body in a short time via blood circulation [6, 26]. However, in a systematic review by Dumont et al. [27], the effectiveness of FAW devices in preventing perioperative hypothermia in patients undergoing joint replacement surgery was evaluated, and the results showed no difference in the incidence of hypothermia with or without the device. There are several reasons for these observations. In this systematic review, only six RCTs with a total of 287 patients were included, which is a relatively small sample size and may not yield accurate results. Although the effect size for core body temperature (MD = 0.26 °C) was statistically significant, its clinical significance may be limited. While this change achieved statistical significance, a 0.26 °C temperature variation may be insufficient to produce a clinically meaningful improvement in patient outcomes in clinical practice. Therefore, caution is warranted when interpreting these findings regarding their practical relevance in clinical applications.
Shivering is one of the most common complications of spinal anesthesia, often manifesting as rapid rhythmic contractions of the skeletal muscles, which is a compensatory response of the body to hypothermia [27]. Shivering can increase a patient’s oxygen consumption, leading to myocardial ischemia and arrhythmias in patients with underlying medical conditions [28]. The mechanism of shivering is likely related to factors such as the distribution of core temperature heat to the periphery, heat loss, and a lower threshold for response. Low temperatures suppress the thermogenic center and excite cold-sensitive neurons, causing muscle tremors to generate heat and maintain thermal balance, thereby inducing shivering [29]. The results of this study show that the incidence of shivering in the experimental group during the perioperative period was significantly lower than that in the control group, consistent with the findings of the study by Pu et al. [30]. The body temperature regulation of cesarean section patients during surgery can be influenced by multiple factors. To maintain normal body temperature during surgery, the key is to perform active and PW measures simultaneously and strengthen heat management, so as to ensure that the body temperature is maintained at a normal level [31]. AW measures are important for maintaining the normal body temperature of patients, reducing the incidence of hypothermia, and preventing shivering. Zhao et al. [32] used a warming blanket with an intermittent warming mode to keep cesarean section patients warm, providing a stable core temperature while avoiding skin damage. Although PW has been convenient and easy to use, it is limited in its effectiveness in improving hypothermia in patients, mainly relying on the patient’s body temperature for warmth. The insulating effect of surgical drapes and blankets during surgery can also be affected by wet fluids. Compared to the effect of size on core body temperature, the reduction in hypothermia (RR = 0.69) and shivering (RR = 0.54) holds greater clinical significance. Hypothermia and shivering are common complications during cesarean section. Controlling these factors not only enhances patient comfort but also promotes postoperative recovery. Therefore, these findings more directly reflect the clinical efficacy of warming interventions, particularly their contribution to reducing hypothermia and shivering.
The results of this study showed significant heterogeneity. Subgroup analyses were conducted to explore the sources of this heterogeneity, but they did not significantly alter the heterogeneity of the results. There are certain limitations to this study, as it did not include more outcome measures, such as patient thermal comfort and the incidence of adverse outcomes. Further research is needed on various AW devices to explore the optimal heating device and to assess whether the use of multiple devices in combination offers more advantages than a single mode. However, differences in blinding methods and allocation concealment exist in the studies, which may introduce certain biases, particularly when evaluating the effectiveness of active and passive heating devices. Such biases are more common in thermal insulation trials, as operators and patients may be unable to completely avoid cognitive or behavioral biases. We acknowledge this limitation and recommend that future studies have strict controls over blinding and allocation concealment to enhance the credibility of the research and the reliability of the results. Although we assessed publication bias using funnel plots, the results revealed asymmetry in certain outcomes. This asymmetry may stem from publication bias, particularly when studies with negative or non-significant results are underreported. Furthermore, funnel plot asymmetry may also be associated with small sample sizes or methodological differences. Therefore, while we have made every effort to assess and control for bias, it is important to note that this limitation may exert some influence on the conclusions of this study.
This meta-analysis demonstrates that AW devices effectively mitigate perioperative hypothermia in patients undergoing cesarean section, reducing the incidence of hypothermia and shivering, thereby improving temperature management. Although preliminary evidence suggests a potential positive impact on reducing adverse events, this requires further validation through high-quality, large-scale RCTs. Consequently, current research does not support direct inferences regarding the long-term clinical outcomes of AW devices.
The data used for the analyses are available upon reasonable request from the first author. The data sets supporting the conclusions of this article are included within the article and its supplementary materials.
FY: data curation, formal analysis, methodology, visualization; HM: methodology; YD, LL, MW, and YZ: data curation. All authors contributed to the critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. At the same time, we all thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG45563.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.