


 , Elif Dönmez 2, Mahmut Talha Uçar 3,4,*
, Elif Dönmez 2, Mahmut Talha Uçar 3,4,* , Yasmin Mohamud Jama 5, Tülay Ortabağ 6
, Yasmin Mohamud Jama 5, Tülay Ortabağ 61 Department of Midwifery, Faculty of Health Sciences, Istanbul Topkapi University, 34065 Istanbul, Türkiye
2 Department of Oncology Nursing, Hamidiye Faculty of Nursing, University of Health Sciences, 34668 Istanbul, Türkiye
3 Department of Public Health, Hamidiye Faculty of Medicine, University of Health Sciences, 34668 Istanbul, Türkiye
4 Now with Saray District Health Directorate, Tekirdag Provincial Health Directorate, Ministry of Health, 59600 Tekirdağ, Türkiye
5 Department of Midwifery, Somalia Mogadishu Recep Tayyip Erdoğan Faculty of Health Sciences, University of Health Sciences, Mogadishu, Somalia
6 Department of Nursing, Faculty of Health Sciences, Istanbul Topkapi University, 34065 Istanbul, Türkiye
Abstract
Family planning is a crucial aspect of reproductive health that allows individuals to determine the number and timing of their children. The main reasons include the very low use of contraceptives (approximately 7% among married women aged 15–49, with only 1–2% using modern methods) and limited access to family planning services. Unintended pregnancies are a major contributor to maternal mortality, resulting from delayed or inadequate antenatal care, unsafe abortions, high-parity births, and short birth intervals. In Somalia, the gap between high levels of awareness and low rates of utilization of family planning, as well as the uncertainties regarding attitudinal and sociocultural determinants, is particularly noteworthy. Somali society follows strict norms based on religious beliefs and cultural values, which influence family decision-making and often limit women’s ability to plan their fertility or use family planning methods. Additionally, due to health policies such as the illegality of elective pregnancy termination, the country’s high fertility rate poses a serious public health concern. Studies have shown that the use of family planning methods remains low across East African countries, including Somalia. Understanding women’s attitudes toward family planning is essential to addressing this issue. This study aimed to examine the attitudes of married women in Mogadishu toward family planning and to identify the sociodemographic and obstetric factors associated with contraceptive use.
This descriptive cross-sectional study was conducted among 286 married women aged 18–49 years who attended gynecological outpatient clinics in Mogadishu, Somalia. Data were collected through structured face-to-face interviews using a validated Family Planning Attitude Scale (FPAS). Data were analyzed using means, standard deviations, medians, frequencies, and percentages using the Statistical Package for the Social Sciences (SPSS) version 21.0.
The mean age of participants was 28.7 ± 5.57 years. Although 30.8% of women were aware of family planning methods, 82.2% did not use any form of contraception. Oral contraceptive pills were the most widely recognized method (14.3%), while implants were the most commonly used (4.5%). Women with no formal education had significantly more traditional views toward childbirth (p < 0.05).
The findings indicated low contraceptive utilization despite high awareness, with cultural and religious beliefs strongly influencing attitudes. Active participation in decision-making and increased knowledge of family planning were significantly associated with enhanced contraceptive use. These results highlight the need for targeted educational programs and policies that promote reproductive autonomy to improve family planning adoption in Mogadishu, Somalia. Achieving desirable women’s health outcomes requires improvements in national health service provision, strengthened efforts by non-governmental organizations (NGO), and the integration of these efforts into development goals.
Keywords
- family planning
- reproductive health
- maternal health
- Somalia
- health promotion
According to the World Health Organization (WHO) [1], family planning is a crucial component of reproductive health; family planning encompasses methods enabling individuals to have children at their desired time and in their preferred number, while also regulating pregnancy intervals. By providing individuals with the opportunity to choose and use contraceptive methods, family planning helps prevent unintended pregnancies and protects the health of both women and children. Additionally, these methods contribute to improving overall health by reducing maternal and child morbidity and mortality [2]. In developing countries, the rise in unintended pregnancies and shortening of birth intervals are major contributors to mortality among women of reproductive age [3].
Currently, the WHO considers maternal mortality rates in many parts of the world to be unacceptably high. The fact that a significant proportion of these deaths are preventable highlights the insufficient use of effective family planning methods, and most importantly, the lack of adequate access to reproductive health services. According to data from 2020, approximately 287,000 women lost their lives during pregnancy and childbirth, with 95% of these deaths occurring in low- and lower-middle-income countries. Sub-Saharan Africa and South Asia accounted for approximately 87% (253,000 deaths) of estimated global maternal deaths in 2020. While maternal mortality in Eastern European countries decreased from 38 to 11 per 100,000 live births, the African region recorded 531 deaths per 100,000 live births in the same year, representing 69% of global maternal deaths [4].
In these countries, humanitarian crises, conflicts, and post-conflict situations, particularly in conflict zones, limit access to health care services, thereby reducing women’s ability to have safe deliveries and benefit from family planning services. According to the Fragile States Index, nine countries (Somalia, Yemen, South Sudan, the Syrian Arab Republic, the Democratic Republic of the Congo, the Central African Republic, Chad, Sudan, and Afghanistan) are categorized at a “very high alert” or “high alert” level in terms of maternal mortality [5].
In sub-Saharan Africa, Somalia, long affected by civil war, has seen its health system severely weakened by ongoing conflict and political instability, restricting access to essential reproductive health services, and consequently, maternal health care, contributing to persistently high maternal mortality rates in the country [6].
In Somalia, approximately 692 women per 100,000 live births die due to pregnancy, childbirth, or postpartum complications. Despite this high maternal mortality rate, fertility remains high, with a total fertility rate of 6.9 [6, 7]. Although 81% of the women are aware of modern contraceptive methods, 94% do not use any method [7]. Additionally, unsafe abortions performed under poor conditions are among the leading causes of maternal deaths in the country [8]. These data indicate that in addition to limited access to healthcare services, structural barriers such as cultural and religious norms, low health literacy, and widespread poverty also play a significant role [9].
According to the WHO (2024), family planning is a fundamental component of reproductive health that includes methods that enable individuals to determine the timing and number of children, while also regulating pregnancy intervals. By providing individuals with the opportunity to choose and use contraceptive methods, family planning helps prevent unintended pregnancies and protect the health of both women and children. Additionally, these methods contribute to improving overall health by reducing maternal and child morbidity and mortality [2]. Global estimates indicate that preventing unintended pregnancies can reduce maternal deaths by 35%, emphasizing the importance of contraceptive use and the need for health policies focused on preventing unintended pregnancies [10].
The low utilization of family planning methods and high prevalence of unplanned pregnancies in Somalia pose significant challenges for reproductive health services. Identifying the factors associated with women’s attitudes toward family planning, increasing their knowledge of contraceptive methods, correcting misconceptions with accurate information, and promoting the adoption and continued use of contraceptive methods will serve as a guide for reproductive health action plans.
This study aimed to examine the knowledge and attitudes of married women of reproductive age toward family planning.
The study population comprised 1652 women who were registered at the Gynecology and Obstetrics Clinic during the study period. The sample size was calculated with an expected frequency of 50%, a 95% confidence interval, and a design effect of 1.0, resulting in a target sample size of 312 women (calculated at http://www.raosoft.com/samplesize.html). The data collection period lasted for three months, and during this time, women who visited the hospital and voluntarily agreed to participate were included in the study without any sampling selection. When the collected data were examined, it was determined that 26 participants provided incomplete responses to the scale items, and the missing data were excluded from the analysis. The remaining 286 valid data represented 91% of the target population. The Cronbach’s alpha coefficient of the scale used in the study was calculated as 0.88, and since the internal consistency was found to be high, the data collection process was terminated, and all analyses were conducted on the 286 valid data sets. Participants were selected using convenience sampling and voluntarily agreed to participate. Eligible participants were identified by the Somali author (YMJ), who obtained informed consent from each participant. The questionnaires used for data collection were originally prepared in Turkish and translated into Somali by a bilingual researcher (YC) fluent in Turkish and Somali. Subsequently, for verification and feedback, the questionnaires were re-translated into Turkish by four academicians proficient in Somali. All academicians involved in the research were experts in their respective fields of study. The eligibility criteria for participation were:
⚫ Married women aged 18–49 years.
⚫ Willingness to participate in the study.
Before conducting the main study, the authors piloted a questionnaire with 10 women to assess its feasibility, clarity, and potential challenges. No questions were modified after the pilot implementation. Before data collection, the researchers conducting the survey were trained and the process was standardized. Women who visited the hospital where the study was conducted were selected for the pilot study. Data collection was carried out by the Somali author (YMJ and ED) through face-to-face interviews with women attending the Gynecology and Obstetrics Clinic. Those who agreed to participate were interviewed in a quiet room within the clinic. The researcher read each question aloud and recorded the participants’ responses as they selected the appropriate answers. Completing the questionnaire took approximately 20–30 minutes per participant. Women involved in the pilot study were excluded from the main study.
The independent variables included sociodemographic factors (age, education, employment, spouse’s employment, income, place of residence, family type, and duration of marriage), participation in family decision-making, prenatal factors (number of pregnancies, pregnancy complications, miscarriage, induced abortion, unintended pregnancy, birth complications, cesarean section history, number of cesarean section, number of children, and plans for future pregnancy), and knowledge of family planning methods. The dependent variables were attitudes toward family planning methods.
Based on current literature, the questionnaire consisted of three sections. The first section gathered sociodemographic details of the women, including gender, age, education level, marital status, employment status, income level, health status, and family structure. The second part of the questionnaire assessed women’s obstetric characteristics such as pregnancy history, miscarriages, number of planned and unplanned pregnancies, parity, number of children, knowledge, and use of family planning methods [2, 8, 10, 11].
The third part of the questionnaire assessed attitudes toward family planning using the Family Planning Attitude Scale (FPAS). The FPAS was developed by Örsal and Kubilay [12]. The scale is Likert-type and consists of 34 items. Each statement on the scale is scored from 1 to 5. The response “I strongly agree” is assigned 1 point, “I agree” is assigned 2 points, “I am undecided” is assigned 3 points, “I disagree” is assigned 4 points, and “I strongly disagree” is assigned 5 points. There are no reverse-coded statements on the scale. A minimum of 34 points and a maximum of 170 points can be obtained from the scale.
The scale has three sub-dimensions: “Social Attitudes Toward Family Planning”, “Attitudes Toward Family Planning Methods”, and “Attitudes Toward Childbirth”. The subscale “Social Attitudes Toward Family Planning” consists of 15 items, with possible scores ranging from 15 to 75. The subscale “Attitudes Toward Family Planning Methods” consists of 11 items, with a possible score range of 11 to 55. The subscale “Attitudes Toward Childbirth” consists of 8 items, with a possible score range of 8 to 40. The Cronbach’s alpha of the original scale was 0.90, which was found to be 0.88 in our study.
Data were analyzed using means, standard deviations, medians, frequencies, and
percentages using the Statistical Package for the Social Sciences (SPSS) version
21.0 (IBM Corp., Armonk, NY, USA). The reliability of the FPAS was evaluated
using Cronbach’s alpha. Statistical significance was determined using a
two-tailed test with a significance level of p
The study was completed with the participation of a total of 286 women. The
sociodemographic characteristics of the women included in the participants are
presented in Table 1. The mean participant age was 28.7
| Variable | Frequency (Percentage) | |
| Age (years, mean |
28.7 | |
| Education status | ||
| No education, did not complete school | 64 (22.4) | |
| Attended school | 222 (77.6) | |
| Employment status | ||
| Yes | 95 (33.2) | |
| No | 191 (66.8) | |
| Spouse’s employment status | ||
| Yes | 214 (74.8) | |
| No | 72 (25.2) | |
| Income level | ||
| Poor | 46 (16.1) | |
| Medium | 199 (69.6) | |
| Good | 41 (14.3) | |
| Longest place of residence | ||
| Province (City) | 72 (25.2) | |
| District | 157 (54.9) | |
| Village | 57 (19.9) | |
| Family type | ||
| Nuclear | 101 (35.3) | |
| Extended | 185 (64.7) | |
| Duration of marriage | ||
| Less than 5 years | 23 (8.1) | |
| 5–10 years | 111 (38.8) | |
| More than 10 years | 152 (53.1) | |
| Participation in family decision-making processes | ||
| Yes | 176 (61.5) | |
| No | 110 (38.5) | |
Obstetric characteristics, knowledge of family planning, and contraceptive use
of the participants are presented in Table 2. The average number of pregnancies
was 4.7
| Variable | N (%) | |
| Number of pregnancies | 1–16 (Min–Max), 4.7 | |
| Complications experienced during the last pregnancy | ||
| Yes | 74 (25.9) | |
| No | 212 (74.1) | |
| Have you had a miscarriage? | ||
| Yes | 67 (23.4) | |
| No | 219 (76.6) | |
| Have you had an induced abortion? | ||
| Yes | 23 (8.0) | |
| No | 263 (92.0) | |
| Have you experienced an unintended pregnancy? | ||
| Yes | 43 (15.0) | |
| No | 243 (85.0) | |
| Number of unintended pregnancies | 1–2 (Min–Max), 1.84 | |
| Did you experience any complications during your last birth? | ||
| Yes | 31 (10.8) | |
| No | 255 (89.2) | |
| Have you given birth via cesarean section? | ||
| Yes | 72 (25.2) | |
| No | 214 (74.8) | |
| How many of your deliveries were cesarean sections? | ||
| 1 | 32 (11.2) | |
| 2 | 28 (9.8) | |
| 3 | 6 (2.1) | |
| 4 and above | 6 (2.1) | |
| How many children do you have? | 1–14 (Min–Max), 4.38 | |
| Do you plan to become pregnant again? | ||
| Yes | 277 (96.9) | |
| No | 9 (3.1) | |
| Knowledge of family planning methods | ||
| Yes | 88 (30.8) | |
| No | 198 (69.2) | |
| Known family planning method (s) | ||
| Oral contraceptive pills | 41 (14.3) | |
| Intrauterine device (IUD) | 20 (7.0) | |
| Condom | 17 (5.9) | |
| Implant | 21 (7.3) | |
| Withdrawal method | 5 (1.7) | |
| Use of family planning methods | ||
| Yes | 51 (17.8) | |
| No | 235 (82.2) | |
| Which family planning method do you use? | ||
| Oral contraceptive pills | 7 (2.4) | |
| Intrauterine device (IUD) | 4 (1.4) | |
| Condom | 9 (3.1) | |
| Implant | 13 (4.5) | |
| Withdrawal method | 4 (1.4) | |
The majority of the women participating in the study responded with “agree” or “strongly agree” to the questions on the scale. The percentages of the responses are presented in Fig. 1, and the questions are listed in Table 3 (Ref. [12]).
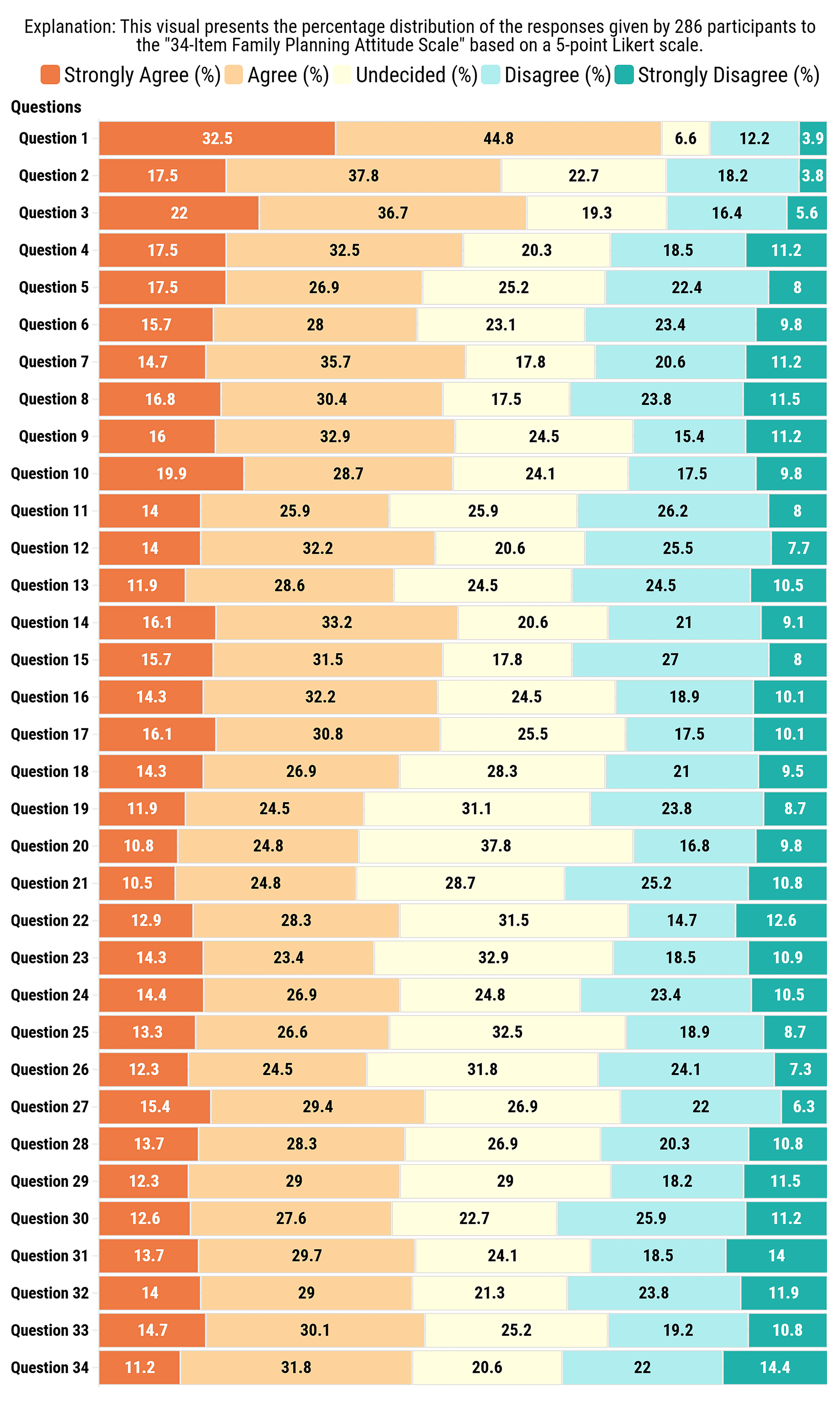 Fig. 1.
Fig. 1.
Percentage distribution of responses to the 34-Item Family Planning Attitude Scale (FPAS).
| Sub-dimensions | No | Question |
| Social attitudes toward family planning | 1- | More children show the power of a man |
| 2- | More children provide social power in the society | |
| 3- | Families want to have more children to share the workload | |
| 4- | There is no harm in the family having many children as the children can take care of each other | |
| 5- | To have many children in the family means that siblings will support each other in the future | |
| 6- | A male child is a must to prevent the division of assets | |
| 7- | The adage that a woman’s primary duty is to give birth is true | |
| 8- | The family must have two girls and two boys | |
| 9- | “God” provides sustenance for every child that is born | |
| 10- | Birth control method is imposed by western countries | |
| 11- | Mothers-in-law do not allow birth control | |
| 12- | If there is a boy, it is said that I have a child | |
| 13- | A man has a male son-in-law | |
| 14- | A man has a boy child | |
| 15- | If there is a girl, it is said that I have a child | |
| Attitudes toward family planning methods | 16- | Spiral causes headache |
| 17- | The rope of the spiral reduces sexual intercourse | |
| 18- | There is a fear that the spiral will leak into the stomach | |
| 19- | There is a fear that birth control pills will cause cancer | |
| 20- | It is thought that Birth control methods will negatively effect sexual intercourse | |
| 21- | Couples who use birth control methods have less sexual pleasure/desire | |
| 22- | It is difficult for women who use birth control to have children again | |
| 23- | A man who has his ducts tied does not enjoy sexual intercourse | |
| 24- | A woman who has her ducts tied does not enjoy sexual intercourse | |
| Attitudes toward childbirth. | 25- | Men whose ducts are tied lose their sexual power |
| 26- | Women whose channels are tied lose their sexual power/become masculine | |
| 27- | I do not believe that getting pregnant at intervals of less than two years is harmful to the child’s health. | |
| 28- | I do not believe that getting pregnant at intervals of less than two years is harmful to the health of the mother | |
| 29- | Pregnancy makes a women attractive | |
| 30- | Families with multiple children can closely follow the development of each child | |
| 31- | In terms of health, it is better to give birth than to use birth control | |
| 32- | It is not right for unmarried people to use family planning methods | |
| 33- | You should be married with the Girls who have no knowledge of birth control methods | |
| 34- | I think there is no need to learn birth control methods |
Adapted from [12].
This study examined the knowledge and attitudes of married women of reproductive age toward family planning. These findings indicate a negative tendency in women’s attitudes and behaviors toward family planning methods. It was observed that the women lacked knowledge about family planning methods and their benefits, supported having many children as a status symbol, and hesitated to use contraceptive methods for religious and cultural reasons. Among those who used contraceptive methods, oral contraceptive pills and implants were the most preferred.
According to the Somalia Health and Demographic Survey (SHDS) [7], the average age of Somali women is relatively young, reflecting the country’s overall youthful demographic structure. In terms of educational level, most women in Somalia have minimal or no formal education. The sociodemographic characteristics of the women in this study, including mean age, education level, employment status, and spousal employment status (Table 1), were consistent with the SHDS 2020 report data [7].
It was determined that, on average, the women in this study had experienced five pregnancies and had four living children. These findings align with the existing literature [13, 14]. The Total Fertility Rate (TFR) represents the average number of children a woman is expected to have by the end of her reproductive period, assuming current fertility rates remain constant across age groups [15]. The TFR in Somalia is reported to be 6.9 [7], while the findings of this study indicate a slightly lower fertility rate than the SHDS report data.
However, considering the mean age of the participants in this study (28.7
The women who participated in this study generally stated that they had given birth via the vaginal route (Table 2). Considering that almost all participants intended to conceive again, it is understood that their preference for vaginal birth was primarily driven by their desire to have more children and the perception that undergoing multiple cesarean section could limit their ability to give birth to additional children. Moreover, during the interviews, the women verbally expressed this belief.
Currently, approximately half of the women of reproductive age worldwide use some form of family planning. In sub-Saharan Africa, the prevalence of family planning use among women of reproductive age has increased to 29% over the past decade [16]. The overall contraceptive prevalence rate is 26% in Africa [17] and 20.42% in Ethiopia. However, this rate is significantly lower in Afar (12%) and Somalia (1%) [18].
In this study, 82.2% of the participants reported not using any family planning method (Table 2). In Somalia, only 7% of women of reproductive age use any form of contraception, while the percentage of women using modern methods remains below 1%. Additionally, 37% of Somali women reported that their family planning needs were unmet, a figure substantially higher than the sub-Saharan African regional average of 23.7% [7, 19].
Approximately 60% of the 88 women who reported being aware of family planning methods indicated that they had used them (Table 2). This finding shows that approximately two out of every three women with knowledge of family planning actually practiced a method. In this context, enhancing women’s awareness of family planning and fertility and promoting positive attitudes toward the use of family planning would be highly beneficial through collaboration with nongovernmental organizations, revision of national health policies, inclusion of family planning in international development goals, and preparation of a sustainable education plan for family planning methods, which could contribute to reducing high fertility rates and mitigating this issue as a significant public health concern.
Although the proportion of women using family planning methods in this study appears to be higher than that in the SHDS report, it is still not at a desirable level. Furthermore, the fact that most participants were unaware of family planning methods and did not use them suggests that a significant proportion of women’s family planning needs remained unmet (Table 2).
The relatively higher family planning utilization rate observed in this study compared to the SHDS 2020 [7] report data may be attributed to several factors. The study was conducted in a central fee-based hospital, where participants may have had better access to healthcare services. The participants were likely to have a higher economic status, enabling them to seek healthcare services. Most of the participants had some level of education, making them more informed than the general female population in Somalia.
Like all Somali women, the participants in this study exhibited lower rates of family planning method utilization than the global average. This discrepancy is thought to be influenced by several factors including limited access to healthcare services, low socioeconomic status, and religious and cultural barriers.
Long-term and permanent methods such as female and male sterilization, intrauterine devices (IUDs), and implants are most effective in preventing unintended pregnancies [20]. However, in sub-Saharan Africa, family planning method preferences tend to favor short-term contraceptive methods. The widespread use of injectables, pills, male condoms, the calendar method, and withdrawal is considered a major contributing factor to the region’s high fertility rates [16]. Among modern contraceptive methods, injectables are the most commonly used in the region, with a prevalence of 39.5%, followed by implants/Norplant methods at 26.5% [21].
Similarly, in this study, although oral contraceptive pills (14.3%) were the most well-known family planning method, implants (4.5%) were the most commonly used. This finding suggests that the ease of use and follow-up associated with implants may contribute to their higher utilization compared with other methods.
When the attitudes of the participating women toward family planning methods were assessed using the FPAS, more than half held similar views. Most women believe that having many children demonstrates a man’s strength, provides social power within the community, and helps families distribute their workload more effectively. Additionally, they expressed that having many children is not problematic, as siblings can take care of each other, and having a large number of children ensures mutual support among siblings in the future (Fig. 1 and Table 3).
In Somali society, attitudes toward family planning are shaped by a combination of traditional values, Islamic teachings, and modern influences. Islam emphasizes child welfare and responsible parenting. Although the acceptance of family planning has increased in recent years, some communities remain distant from modern contraceptive methods, preserving traditional practices [22].
Factors such as a lack of education, limited access to healthcare services, and deeply rooted cultural beliefs, including viewing children as a form of social and financial security, are believed to contribute to the reluctance of individuals in Somalia and other Sub-Saharan African countries to use family planning methods [10, 23, 24].
In Somali society, large families are widely perceived as beneficial in multiple ways. There is a strong societal belief that children will support their parents in old age and assist younger siblings [25]. In particular, community and religious leaders view modern family planning methods as barriers that limit the number of children an individual can have, leading to negative attitudes toward birth control methods [26].
Children are considered socially and economically significant for various reasons, including sustaining population growth, protecting communities and land, and providing labor for livestock care. Due to these reasons, Somali women often aspire to have large families [25, 26]. The findings of this study align with the existing literature, further suggesting that this societal perspective constitutes a major barrier to the adoption of modern family planning methods.
Half of the women included in this study stated that a woman should have at least four children, God provides sustenance for every child born, and the use of family planning methods is a Western imposition (Fig. 1 and Table 3).
In several sub-Saharan African countries with majority-Muslim populations, [27] modern family planning methods (such as condoms, IUDs) are not used because of the belief that they contradict Islamic teaching. Birth control is perceived as an intervention in God’s plan, and there is a strong belief that each child is a gift from God, who also provides for them. Additionally, many people in the region hold the religious conviction that Islam encourages individuals to reproduce and populate the earth. In line with these religious and cultural perspectives, there is a widespread perception that having more children enhances social status and respectability [25, 28, 29, 30, 31, 32, 33].
Similarly, in a qualitative study conducted by Gele et al. [10] in Mogadishu, Somalia, women perceived family planning methods as Western practices that contradicted their norms and traditions, which in turn hindered the adoption of these methods. The study also highlighted that the participants believed Westerners had introduced a family planning culture to Somalia [10].
A study examining the influence of religious beliefs on family planning in Western Ethiopia revealed that Ethiopian Muslim women believed that if a woman had an implant or any contraceptive device in her body at the time of death, her soul would be unable to enter heaven [34]. Similarly, Abdi et al. [34] reported that women perceived the use of birth control pills as equivalent to killing an unborn child [35].
The findings of this study are consistent with the existing literature demonstrating that traditional and religious values exert a strong influence on women’s perceptions of fertility and family planning. These findings reflect the prevailing societal belief that fertility is a natural process dictated by religious faith, and highlight the widespread conviction that encourages high fertility rates within the community.
In this study, half the women stated that they believed giving birth is a woman’s primary duty (Fig. 1 and Table 3) and that having male children was superior.
Research conducted in sub-Saharan Africa, particularly Somalia, Kenya, and Uganda, has shown that women prefer to have many children to increase their social status and as a sign of respect toward their husbands [36]. Similarly, men perceive having many children as a status symbol in society [37]. For instance, in Kenya, it has been reported that men expect women to continue giving birth until menopause, considering it a means of ensuring the continuation of their lineage [35].
According to Msoka et al. [37], in Tanzania, men do not support birth control until they reach a certain age and have fathered a sufficient number of children from multiple wives. Similarly, in a study conducted in Ethiopia by Davidson et al. [24] women perceived the ten-year duration of IUDs as too long, preferred to give birth before the ten-year period ended, and believed that IUDs could cause infertility, leading to their reluctance to use this method [25].
However, some studies conducted in sub-Saharan African countries report that women who wish to prevent pregnancy or regulate birth intervals often secretly use contraceptive pills and injectable methods without informing their husbands [38, 39]. Some women who use oral contraceptives reportedly remove the pills from their packaging and store them in an envelope to hide them from their husbands, fearing that their husbands will become angry if they discover their contraceptive use [38].
Additionally, some women avoid obtaining contraceptives from healthcare facilities because they fear that healthcare workers may violate their confidentiality. Instead, they secretly purchase contraceptive pills from street vendors [39]. The primary reason behind this secrecy is the fear that if husbands discover their limited reproductive capacity, they may seek additional wives, and women aim to prevent this from happening [40, 41].
A similar study conducted in Uganda found that women who use modern birth control methods often use them in secret because of fear of stigma. Consequently, some women chose to visit health centers at night to receive Depo-Provera injections [42].
The findings of this study support the existing literature by demonstrating how patriarchal family structures and traditional gender roles exert significant pressure on women’s fertility choices.
When examining the attitudes of the women in this study toward childbirth, more than 40% stated that they did not believe that pregnancies occurring at less than two-year intervals posed any risk to maternal health. Additionally, they believed that giving birth is better for a woman’s health than using contraceptive methods (Fig. 1 and Table 3).
In sub-Saharan African countries, when providing expert advice on birth control to Muslim women, the term “birth spacing” is preferred over “family planning”. In Islam, certain birth control practices (such as the calendar method and breastfeeding) are believed to be permissible because they support maternal and child health by allowing birth spacing [29]. Therefore, women who wish to increase the interval between births tend to choose these methods [10, 28, 29, 31, 32].
The fact that nearly half the women in this study were unaware of the importance of birth spacing in maternal health was a significant finding. Although Islam supports birth spacing for maternal and infant health, the belief that frequent childbirth is correct and healthy is attributed to cultural influences. These findings indicate that women may not be fully aware of the potential health burdens and risks associated with pregnancy and childbirth, and may not fully understand the benefits of family planning methods.
Women’s decision-making power in family planning is defined as their ability to make independent choices regarding their needs and preferences or to discuss these issues with their partners [43]. Decision-making power specifically refers to a woman’s ability to independently decide on her family planning needs and preferences or discuss them with her partner [43]. Active participation in household decision-making processes plays a crucial role in increasing the use of family planning methods for birth control [43, 44].
In this study, the participation rate of Somali women in the household
decision-making processes was 61.5%. In many African societies, women tend to
become more independent as they age, and their participation in healthcare
decision-making processes increases accordingly [45]. When women’s participation
in decision-making processes is evaluated in relation to their mean age (28.7
However, according to the SHDS report, men generally dominate household decision-making processes in Somalia. The report indicated that 45% of the women stated that their husbands made major household financial decisions, and more than half reported that their husbands decided on family visits [7].
The higher rate of women’s participation in decision-making processes (61.5%) observed in this study compared to the SHDS report is likely due to the higher education levels of the study participants and the fact that this research was conducted among women who attended a private fee-based hospital in an urban center.
Although most women in South Africa participate in joint decision-making, a 2024 study conducted in Ethiopia reported that the rate of making family planning decisions jointly with a spouse or partner was 37% [48]. In Somalia, 45% of women reported that their husbands predominantly make healthcare-related decisions, whereas 34% stated that they made these decisions with their husbands [7].
A qualitative study conducted in Mogadishu, Somalia revealed that health professionals require spousal approval for modern contraceptive methods, except for oral contraceptive pills, to prevent women from making independent decisions regarding contraceptive use [10].
In this study, despite women participating in household decision-making processes, 69.2% were unaware of family planning methods, suggesting that this lack of knowledge did not influence their decision to use family planning methods. This finding highlights the significant barrier to the adoption of contraceptive methods among women.
The results of this study emphasize the importance of women having agency over their reproductive health and family planning decisions. It is crucial to enhance women’s knowledge and awareness, encourage their participation in decision-making processes along with their spouses, and create opportunities for them to express their needs and preferences while making autonomous healthcare decisions.
This study indicated that women’s awareness of family planning methods is positively associated with their use of these methods. Previous studies have shown that increasing women’s knowledge of family planning is one of the most effective ways to enhance their utilization rates and reduce unmet family planning needs [19, 48]. The findings of this study are consistent with the existing research and emphasize that organizing educational programs to address knowledge gaps is a crucial step in increasing the use of family planning methods among Somali women.
This study examines the attitudes and behaviors of married women of reproductive age in Somalia regarding family planning. However, this study had several limitations.
This study was conducted in a specific geographical region and included women who sought care at a central healthcare facility. This may limit the generalizability of our findings to all Somali women. The sample size was relatively small compared to the overall population, indicating that broader and more diverse samples could provide more comprehensive results.
Although the target sample size was calculated to be 312 women, the study was completed with 286 participants because only women who visited the hospital and consented to participate were included.
Additionally, because of religious and cultural beliefs, some participants may have been reluctant to openly discuss certain topics, potentially affecting the accuracy and completeness of the data. The study relied on self-reported data, which may have been influenced by social desirability bias, leading some participants to withhold or alter their opinions.
Because this was a cross-sectional study, we did not establish a cause-and-effect relationship. Furthermore, language differences and translation processes during the participant interviews may have resulted in misinterpretation or loss of information.
In addition, the study’s limitations include the inclusion of only women who were able to visit a private hospital because the Somali region is a conflict area and the decision not to collect quantitative data through home visits for the safety of the researchers. Therefore, only women who visited the hospital were included in this study. This is a limitation of our study.
In Somalia, societal views on childbearing are rooted in religious values, which may lead women to perceive family planning methods as negative from a cultural perspective. Consequently, they may be hesitant to openly state that they are knowledgeable about or use these methods; this should be taken into account, as it may affect the accuracy of their responses to the study questions. This situation created a limitation in obtaining information about family planning from participants.
This study provides important findings regarding the attitudes and behaviors of married women of reproductive age in Somalia toward family planning. The results indicated that most women lack knowledge of family planning methods and do not use them. Traditional and religious beliefs were found to have a significant influence on women’s acceptance of family planning methods. Additionally, women’s participation in household decision-making processes is associated with an increased likelihood of using family planning methods. The perception of fertility as a form of social and economic security further reinforces the tendency for women to have larger families.
Furthermore, limited access to modern family planning methods and insufficient information on these methods have been identified as major barriers in preventing unintended pregnancies. These findings highlight the urgent need to implement comprehensive education and awareness campaigns aimed at enhancing Somali women’s knowledge about family planning and improving their access to reproductive healthcare. Additionally, policies and programs that encourage the greater inclusion of women in household decision-making processes should be developed and promoted.
The family planning usage rates among women in Mogadishu are low. However, it is believed that collaborating with non-governmental organizations, improving health policies to increase women’s awareness, and providing education on family planning will positively influence their attitudes toward the use of family planning methods.
Moreover, the development of health policies that facilitate access to family planning methods for women in the Somali region is an important step toward increasing method use and raising fertility awareness among women.
This study provides important insights into Somali women’s attitudes and behaviors toward family planning and serves as a basis for future quantitative and qualitative research. However, further research is needed to gain a deeper understanding of the factors that influence the use of contraceptive methods and decision-making processes in this population. Future research should focus on the following areas:
⚫ Longitudinal studies should be conducted to track how Somali women’s attitudes toward family planning evolve over time and evaluate the effectiveness of interventions aimed at increasing contraceptive use.
⚫ Given the strong influence of cultural and religious beliefs on contraceptive use, qualitative research should explore the perspectives of religious leaders and community elders on family planning, and how their views shape women’s choices.
⚫ Studies evaluating the effectiveness of educational programs designed to raise awareness of family planning and empower women in the decision-making processes are crucial for identifying effective strategies for increasing contraceptive use.
⚫ Research should investigate structural and systemic barriers to accessing family planning services, particularly in relation to healthcare infrastructure, economic accessibility, and the attitudes of healthcare providers.
⚫ Future studies should examine the role of male partners in contraceptive decision-making and develop strategies to encourage greater male involvement in family planning.
⚫ Comparative studies should explore differences in family planning attitudes and access to services between women living in rural and urban areas of Somalia.
Addressing these research gaps will contribute to the development of more comprehensive policies and programs aimed at increasing family planning use among Somali women. This, in turn, is a critical step toward improving maternal and child health outcomes.
Data is available from the corresponding author on reasonable request.
EY: Study design and planning, data interpretation, and manuscript drafting. ED: Data collection, data analysis, data interpretation, and manuscript drafting. MTU: Data analysis, data interpretation, and manuscript drafting. YMJ: Data collection, Result interpretation, and manuscript drafting. TO: Data interpretation, drafting of the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Somali Mogadishu Recep Tayyip Erdoğan Research and Training Hospital Scientific Research Ethics Committee (Document Date and Number: 30.03.2024/972). Informed consent was obtained from all patients who agreed to participate in the study, and the principles of the Declaration of Helsinki were strictly followed to ensure the protection of participants’ rights.
The authors thank the women who voluntarily participated in the study and the health professionals working in the hospitals.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.