



 , Apostolos P. Athanasiadis 3, Panayiota Papasozomenou 2, Efstratios Assimakopoulos 1, Demetrios Tsolakidis 1, Grigorios Grimbizis 1, Themistoklis Mikos 1,*
, Apostolos P. Athanasiadis 3, Panayiota Papasozomenou 2, Efstratios Assimakopoulos 1, Demetrios Tsolakidis 1, Grigorios Grimbizis 1, Themistoklis Mikos 1,*
1 1st Department of Obstetrics & Gynecology, Aristotle University of Thessaloniki, Papageorgiou General Hospital, 56429 Thessaloniki, Greece
2 School of Health Science, International Hellenic University, 57400 Thessaloniki, Greece
3 3rd Department of Obstetrics & Gynecology, Hippokratio Hospital, 54642 Thessaloniki, Greece
Abstract
Few studies have examined the impact of subsequent deliveries on levator hiatus morphology and no study has described its changes throughout gestation and postpartum in multiparous women. The aim of this study was to investigate the changes that occur in the levator hiatus (i) during pregnancy, and (ii) after labor in a cohort of multiparous women. Pregnant women with a history of vaginal birth were compared to those with a history of cesarean section (CS).
Prospective cohort longitudinal study, consisting of 82 multiparous women who were examined and recruited at an antenatal clinic. All participants underwent real-time three-dimensional transperineal ultrasound (3D-TPUS) evaluation of the levator ani at 12, 22, and 32 weeks of pregnancy, as well as 4–6 months after delivery. 3D volumes were acquired and stored for offline analysis.
Data from 66 women with at least two measurements were available for analysis. 31 had a history of vaginal delivery (VD) and no history of CS (Group 1), while 35 had a history of previous CS and no history of vaginal birth (Group 2). When comparing levator ani dimensions at rest, during Valsalva, and pelvic floor muscle contraction (PFMC) in the third-trimester to those in the first-trimester, almost all hiatal dimensions were statistically significantly enlarged. Postpartum hiatal dimensions were lower compared to third-trimester measurements in both groups. The incidence of new levator trauma in Group 1 was 3.7%.
In multiparous women: (a) ultrasound (US) measurements of the levator hiatus increased significantly between the first-, second-, and third-trimester, and (b) many of the levator hiatus dimensions decreased significantly postpartum, regardless of whether the delivery was a non-traumatic vaginal birth or a CS. The incidence of new levator trauma is reduced in multiparous women with a history of previous vaginal births who deliver vaginally.
Keywords
- levator ani muscle (LAM)
- levator ani muscle hiatus
- mode of delivery
- 3D/4D transperineal ultrasound
- multiparous
Three-dimensional transperineal ultrasound (3D-TPUS) assists in obtaining images of pelvic structures related to the support of pelvic organs [1, 2, 3, 4, 5, 6, 7, 8]. Magnetic resonance imaging (MRI) has also been used [9], but 3D-TPUS is generally quicker and easier to perform in everyday clinical practice. The axial plane has been used to represent the levator ani muscle (LAM), an anatomical-functional unit that plays a pivotal role in normal physiology of the pelvis. The sonographic images obtained with 3D-TPUS focus mainly on (a) the presence of any LAM trauma, defined as a sonographic defect in the muscle, and (b) the dimensions of the LAM. Both LAM trauma and increased dimensions have been consistently associated with the presence of symptomatic pelvic organ prolapse (POP) [1, 2, 3, 10].
The origins of LAM trauma are primarily associated with vaginal delivery (VD), as this is when damage to the pelvic floor is most likely to occur due to the descending presenting part of the fetus. Immediately postpartum, LAM trauma can be depicted sonographically [11], and its incidence as assessed using 3D-TPUS ranges from 10 to 35% [12, 13, 14, 15, 16]. In some cases, lesions initially diagnosed may not be confirmed in later scans [17, 18]. Nevertheless, the majority of LAM injuries can still be recognized sonographically at anytime after the puerperium [17, 18, 19, 20, 21].
Recently, changes in LAM dimensions throughout gestation and the postpartum period have been studied [16, 22, 23, 24, 25, 26, 27, 28]. Several prospective studies in nulliparous womenhave shown that LAM dimensions expand throughout pregnancy, continuing to increase until the late third-trimester [22, 23, 24, 25, 26, 27]. All these studies have attempted to describe the changes in LAM dimensions both in nulliparous women with levator trauma and those without. They concluded that trauma is the major cause of the expansion of LAM dimensions after delivery [22, 23, 24, 25, 26, 27]. Only a few studies have examined the impact of subsequent deliveries on levator hiatus morphology [29, 30]. Moreover, no study has described the changes in LAM dimensions throughout gestation and the postpartum period in multiparous women. The rationale for such a study would be to define the role of multiple vaginal deliveries in the physiology of the pelvic floor support. As such, the aim of this study was to investigate the changes in LAM dimensions (1) during pregnancy and (2) after labor in a cohort of multiparous women.
The present study was conducted prospectively between 2011 and 2014 at a tertiary center. The study protocol was approved by the Ethics Committee of the Medical School of the Aristotle University of Thessaloniki, Greece (Protocol No. 3767/2011). The study design included the recruitment of consecutive pregnant women attending the local antenatal clinic. The study population consisted of 82 multiparous women. Inclusion criteria were (i) pregnant women between 10 and 14 weeks of gestation, (ii) aged 18 years or older, and (iii) with a history of at least one previous delivery. Exclusion criteria were (i) non Greek speakers, (ii) women with a history of pre-existing POP or urinary incontinence (UI), and (iii) patientswho hadcomorbidities that would prohibit a Valsalva maneuver (such as heart and lung problems, rheumatic disease, other). Written informed consent was obtained from all participants before enrollment in the study.
At baseline, all participantsprovided a thoroughmedical history and underwent a pelvic examination. If genitalprolapse was detected, then it was graded according to the Pelvic Organ Prolapse Quantifications (POP-Q) system. At study enrollment and postpartum, all participants completed standardized questionnaires for UI (International Consultation on Incontinence Questionnaire, ICI-Q), sexual life (Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire, PISQ-12), and quality of life (European Quality of Life 5 Dimension, EQ-5D).
The primary outcome of the study was the LAM dimensions in multiparous women during the first-, second-, and third-trimester, as well as postpartum. The secondary outcome of the studywas the comparison of LAM dimensions in multiparous women with a history of VD and no history of cesarean section (CS) versus those with a history of previous CS and no history of vaginal birth. Levator ani dimensions were expressed as anterior-posterior (a-p) and left-right (l-r) diameters in cm, and in hiatal area in cm2, measured at rest, during maximum Kegel, and maximum Valsalva maneuver.
All women were examined using real-time 3D-TPUS (5–9 MHz, Voluson 730, GE Healthcare, Chicago, IL, USA) of the levator ani at 12, 22, and 32 weeks’ gestation, as well as 4–6 months after delivery (Fig. 1). The same investigator conducted all the ultrasound (US) examinations (AS). During the US examination, all women were in the supine position. The perineum was examined at rest, during pelvic floor muscle contraction (PFMC) (selecting the best out of three efforts), and at maximum Valsalva maneuver (selecting the best out of three efforts). 3D volumes obtained with 3D-TPUS were stored and analyzed later by two investigators (AS, TM). The US data were analyzed using 4D view Free Version 7 software (GE Healthcare, Chicago, IL, USA). The methodology of volume analysis followed protocols established in previously published seminal studies [12, 31, 32]. During offline analysis of each volume, the region of interest (ROI) was focused on the minimal dimensions of the levator hiatus. For each patient, a sonographic box was created that contained the posterior margin of the symphysis pubis anteriorly and the anterior margin of the levator plate posteriorly. This plane was initially used for measurement acquisition and later for tomographic representation, which allowed for the qualitative assessment of detachment of the LAM from the lateral wall of the pelvis and, subsequently, the diagnosis of LAM trauma. The tomographic analysis involved slicing the volumes from 5 mm below to 12.5 mm above the minimal hiatal dimensions, at 2.5 mm intervals, producing eight slices per ROI. The presence of levator detachment in three consecutive slices was considered diagnostic for LAM trauma (Fig. 2A,B) [32]. Intra-observer and inter-observer variability were assessed as previously reported [27].
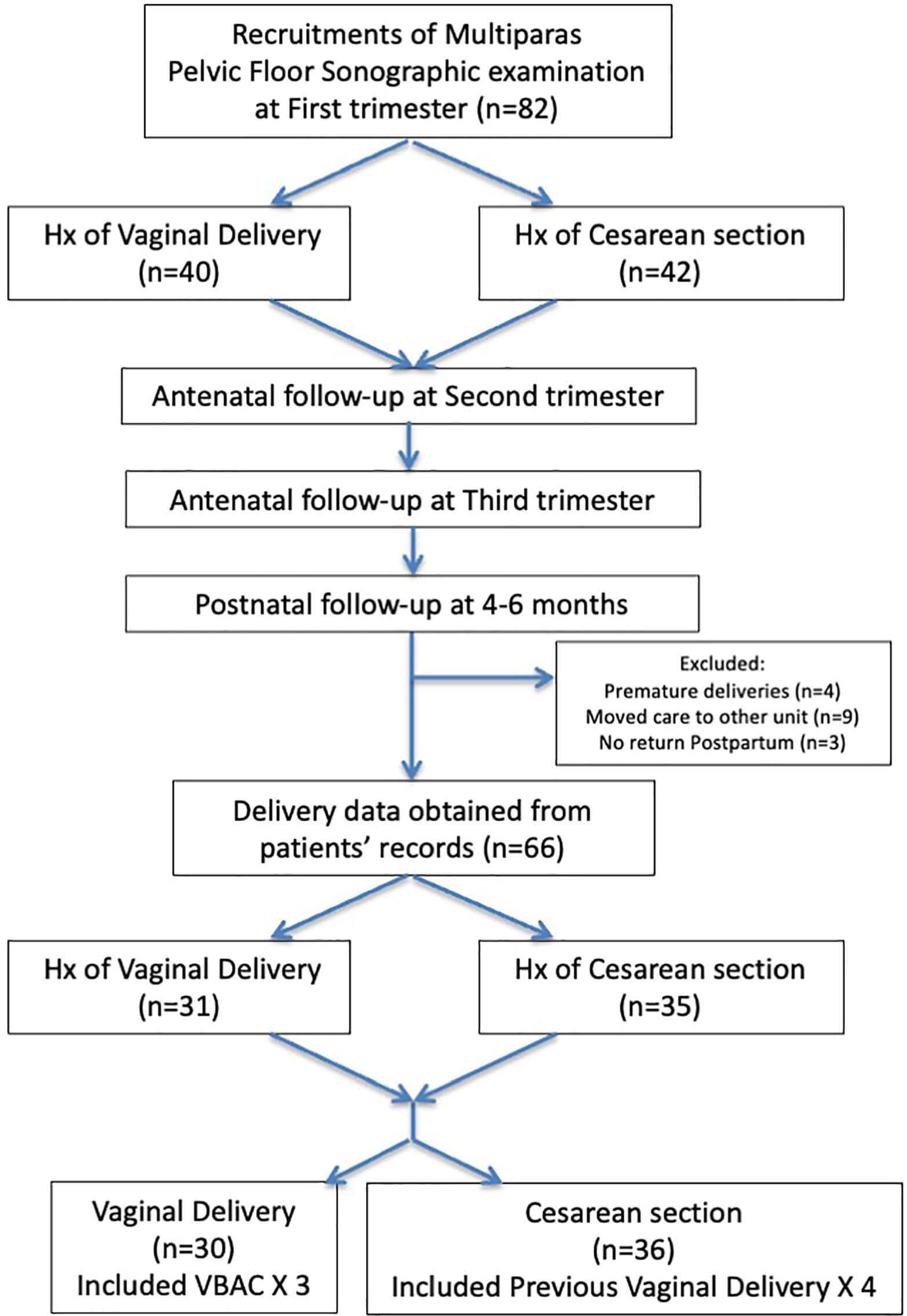 Fig. 1.
Fig. 1.
Flowchart of the recruitment process and the attendance of the 4–6 months postpartum examination. Hx, history; VBAC, vaginal birth after cesarean section.
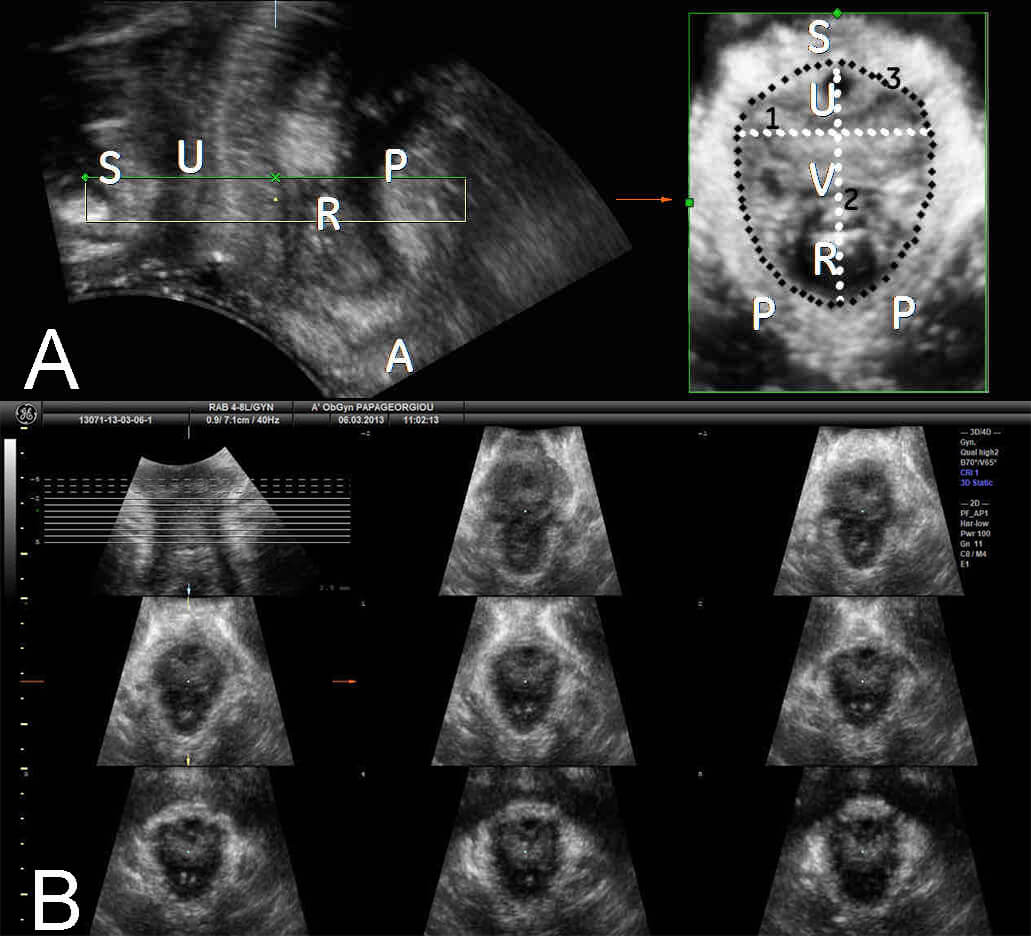 Fig. 2.
Fig. 2.
Three-dimensional transperineal ultrasound (3D-TPUS) imaging of the levator hiatus. (A) 3D-TPUS imaging of minimal dimensions of the levator hiatus during PFMC at the saggital plane (left), and reconstruction at the axial plane (right). (B) Tomographic ultrasound image (TUI) of the minimal dimensions of the levator hiatus during PFMC. PFMC, pelvic floor muscle contraction; S, symphysis pubis; U, urethra; R, rectum; P, puborectalis muscle; A, anus; V, vagina; 1, left-right diameter; 2, anterior-posterior diameter; 3, hiatal circumference.
Data regarding labor, delivery and the puerperium were compiled from (i) medical records and (ii) phone calls with the study participants. Details recorded included the mode of delivery, duration of the second stage of labor, use of instrumental delivery, perineotomy, and whether a CS was performed during the first or second stage of labor.
During study design, we conducted an appropriate power analysis [27]. A sample
size of 60 women was found adequate, with a minimum of 23 in each group, allowing
for a maximum of 20% of missed follow-ups. This sample size was calculated to
detect 15% differences in hiatal area dimensions between the first- and
third-trimester of pregnancy, with type I error
82 women were initially enrolled in the study. 16 women were excluded from
further analysis for the following reasons: (i) missing at least two US
examinations due to prematurity (n = 4), (ii) receiving further treatment at
another hospital (n = 9), and (iii) not returning for postpartum follow-up (n = 3)
(Fig. 1). Details from 66 women with at least two US measurements were available
for analysis. 31 had a history of VD and no history of CS (Group 1), while 35 had
a history of previous CS and no history of vaginal birth (Group 2). At baseline,
the mean maternal age was 32.6
| Total | History of VD | History of CS | p-value | |
| N | 66 | 31 | 35 | n.a. |
| Maternal age (years) | 32.60 |
32.45 |
32.71 |
n.s. |
| Maternal height (cm) | 163.94 |
164.61 |
163.34 |
n.s. |
| Maternal weight (kg) | 65.56 |
67.74 |
63.63 |
n.s. |
| Maternal BMI (kg/m2) | 24.1 |
24.7 |
23.6 |
n.s. |
| Parity | 2.30 |
2.29 |
2.40 |
n.s. |
| Gestational age at birth (weeks) | 38.14 |
38.29 |
38.00 |
n.s. |
| Neonatal weight at birth (g) | 3186.34 |
3256.15 |
3129.61 |
n.s. |
| VD | 30/66 (45.45%) | 27/31 (87.10%) | 3/35 (8.57%) | n.a. |
| VBAC | 3/66 (4.54%) | n.a. | 3/35 (8.57%) | n.a. |
| CS | 36/66 (54.54%) | 4/31 (12.90%) | 32/35 (91.43%) | n.a. |
| Elective CS | 36/66 (54.54%) | 4/31 (12.90%) | 32/35 (91.43%) | n.a. |
| 1st stage CS | 0/66 (0%) | 0/31 (0%) | 0/35 (0%) | n.a. |
| 2nd stage CS | 0/66 (0%) | 0/31 (0%) | 0/35 (0%) | n.a. |
| Prolonged second stage | 1/66 (1.51%) | 1/27 (3.70%) | 0/35 (0%) | n.a. |
| Instrumental VD | 3/66 (4.54%) | 3/27 (11.11%) | 0/35 (0%) | n.a. |
| Spontaneous perineal tears | 2/66 (3.03%) | 2/27 (7.40%) | 0/35 (0%) | n.a. |
| Perineotomy | 22/66 (33.33%) | 19/27 (70.37%) | 3/35 (8.57%) | n.a. |
VD, vaginal delivery; CS, cesarean section; VBAC, vaginal birth after cesarean section; n.a., not applicable; n.s., not significant; BMI, body mass index.
In the previous VD subgroup, almost all hiatal dimensions were statistically significantly increased between the first- and the second-trimester, and between the second- and the third-trimester of pregnancy, both at rest, during PFMC, and at maximum Valsalva effort (Table 2 and Fig. 3). In the previous CS subgroup, most hiatal dimensions were similarly statistically increased between the first- and the second-trimester, and between the second- and the third-trimester, both at rest, during PFMC and at maximum Valsalva effort (Table 3 and Fig. 3).
| First-trimester | Second-trimester | Third-trimester | Postpartum | First vs. Second | Second vs. Third | First vs. PP | Second vs. PP | Third vs. PP | ||
| n1 = 31 | n1 = 27 | n1 = 27 | n1 = 26 | n2 = 27 | n2 = 27 | n2 = 26 | n2 = 26 | n2 = 26 | ||
| At rest | ||||||||||
| a-p diameter (cm) | 5.15 |
5.44 |
5.72 |
5.57 |
0.0231† | 0.0162† | 0.0420† | n.s. | ||
| l-r diameter (cm) | 3.82 |
3.95 |
4.09 |
3.91 |
0.0033† | 0.0399† | 0.0001† | n.s. | n.s. | |
| Hiatal area (cm2) | 14.95 |
16.16 |
17.40 |
16.48 |
0.0076† | 0.0122† | n.s. | n.s. | ||
| At max Kegel | ||||||||||
| a-p diameter (cm) | 4.28 |
4.62 |
4.78 |
4.64 |
n.s. | n.s. | n.s. | n.s. | 0.0241‡ | |
| l-r diameter (cm) | 3.74 |
3.73 |
3.88 |
3.64 |
n.s. | n.s. | n.s. | n.s. | n.s. | |
| Hiatal area (cm2) | 12.19 |
13.00 |
14.32 |
13.12 |
n.s. | 0.0071† | 0.0329† | n.s. | 0.0212‡ | |
| At max Valsalva | ||||||||||
| a-p diameter (cm) | 5.41 |
5.56 |
6.03 |
5.80 |
0.0174† | 0.0039† | 0.0033† | n.s. | n.s. | |
| l-r diameter (cm) | 4.22 |
4.26 |
4.44 |
4.22 |
n.s. | n.s. | n.s. | n.s. | n.s. | |
| Hiatal area (cm2) | 17.76 |
17.95 |
20.09 |
19.22 |
n.s. | 0.0024† | n.s. | n.s. | n.s. | |
VD, vaginal delivery; PP, postpartum; †, statistically significant increase; ‡, statistically significant decrease; n.s., notsignificant; n1, number of subjects; n2, number of comparisons; a-p, anterior-posterior; l-r, left-right.
| First-trimester | Second-trimester | Third-trimester | Postpartum | First vs. Second | Second vs. Third | First vs. PP | Second vs. PP | Third vs. PP | ||
| n1 = 35 | n1 = 33 | n1 = 32 | n1 = 28 | n2 = 33 | n2 = 32 | n2 = 27 | n2 = 28 | n2 = 28 | ||
| At rest | ||||||||||
| a-p diameter (cm) | 5.08 |
5.10 |
5.44 |
5.26 |
0.0358† | 0.0223† | 0.0404† | 0.0333† | n.s. | |
| l-r diameter (cm) | 3.68 |
3.79 |
3.96 |
3.68 |
n.s. | n.s. | n.s. | n.s. | 0.0198‡ | |
| Hiatal area (cm2) | 14.00 |
14.50 |
16.40 |
14.76 |
0.0038† | 0.0013† | 0.0184† | n.s. | 0.0192‡ | |
| At max Kegel | ||||||||||
| a-p diameter (cm) | 4.20 |
4.32 |
4.47 |
4.25 |
0.0001† | n.s. | n.s. | n.s. | n.s. | |
| l-r diameter (cm) | 3.53 |
3.62 |
3.62 |
3.57 |
n.s. | n.s. | n.s. | n.s. | n.s. | |
| Hiatal area (cm2) | 11.06 |
11.65 |
12.45 |
11.48 |
0.0022† | 0.0402† | n.s. | n.s. | n.s. | |
| At max Valsalva | ||||||||||
| a-p diameter (cm) | 5.20 |
5.24 |
5.85 |
5.26 |
0.0311† | 0.0002† | n.s. | n.s. | 0.0060‡ | |
| l-r diameter (cm) | 3.96 |
4.04 |
4.24 |
3.93 |
N.S. | 0.0021† | n.s. | n.s. | 0.0082‡ | |
| Hiatal area (cm2) | 15.69 |
15.98 |
18.92 |
16.00 |
0.0155† | 0.0003† | n.s. | n.s. | 0.0013‡ | |
CS, cesarean section; PP, postpartum; †, statistically significant increase; ‡, statistically significant decrease; n.s., notsignificant; n1, number of subjects; n2, number of comparisons; a-p, anterior-posterior; l-r, left-right.
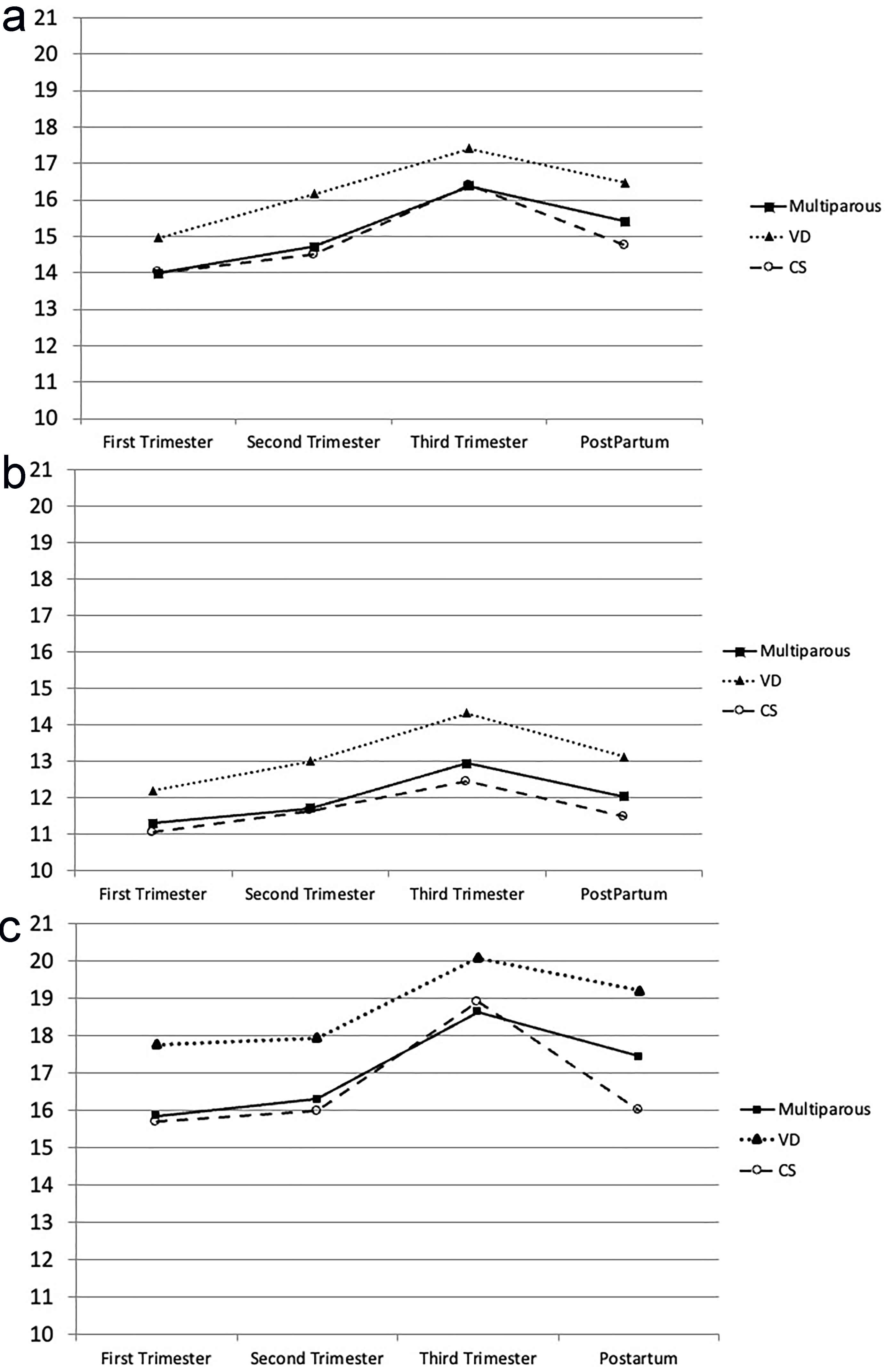 Fig. 3.
Fig. 3.
Diagrams showing changes of the levatorhiatal area in different subgroupsthroughout pregnancy and postpartum. (a) at rest (cm2); (b) during PFMC (cm2); (c) at maximum Valsalva (cm2); solid line: all women with a previous history of vaginal birth (multiparous); round dot line: all women with a history of VD; dash line: all women with a history of CS. VD, vaginal delivery; CS, cesarean delivery; PFMC, pelvic floor muscle contraction.
Postpartum evaluation of hiatal appearance postnatally showed that only 1 woman experienced LAM trauma after spontaneous VD (1/27, 3.7%); this trauma occurred on the left LAM of a woman who already had a trauma on the right LAM during a previous delivery. No patient suffered trauma after CS. 3 women with a history of CS delivered vaginally; of these, 1 was diagnosed with LAM trauma, representing 33.3%.
In the previous VD subgroup, the hiatal area postpartum was increased compared to the first- and the second-trimesters, and decreased compared to the third-trimester during TPUS (Table 2 and Fig. 3).
In the previous CS subgroup, the hiatal area postpartum was increased compared to the first- and the second-trimesters, and decreased compared to the third-trimester during TPUS (Table 3 and Fig. 3).
ICI-Q scores were non-significantly increased in both subgroups: from 2.4 in the
first-trimester to 3.5 postpartum in the VD subgroup, and from 0.9 in the
first-trimester to 1.1 postpartum in the CS delivery subgroup. EQ-5D scores were
non-significantly changed in both subgroups: from 83.7 in the first-trimester to
89.6 postpartum in the VD subgroup, and from 87.0 in the first-trimester to 86.9
in the CS subgroup. PISQ-12 score was significantly reduced only in the CS
subgroup (from 52.7 in the first-trimester to 51.6 in the postpartum,
p
| a-p diameter (cm) | l-r diameter (cm) | Hiatal area (cm2) | ||||||||
| VD | CS | p-value | VD | CS | p-value | VD | CS | p-value | ||
| During pregnancy | 31 | 35 | 31 | 35 | 31 | 35 | ||||
| First-trimester | ||||||||||
| N | 25 | 26 | 25 | 26 | 25 | 26 | ||||
| At rest | 5.15 |
5.08 |
n.s. | 3.82 |
3.68 |
n.s. | 14.95 |
14.00 |
n.s. | |
| At max Kegel | 4.28 |
4.20 |
n.s. | 3.74 |
3.53 |
n.s. | 12.19 |
11.06 |
n.s. | |
| At max Valsalva | 5.41 |
5.20 |
n.s. | 4.22 |
3.96 |
n.s. | 17.76 |
15.69 |
n.s. | |
| Second-trimester | ||||||||||
| N | 26 | 34 | 26 | 34 | 26 | 34 | ||||
| At rest | 5.44 |
5.10 |
n.s. | 3.95 |
3.79 |
n.s. | 16.16 |
14.50 |
n.s. | |
| At max Kegel | 4.62 |
4.32 |
n.s. | 3.73 |
3.62 |
n.s. | 13.00 |
11.65 |
n.s. | |
| At max Valsalva | 5.56 |
5.24 |
n.s. | 4.26 |
4.04 |
n.s. | 17.95 |
15.98 |
n.s. | |
| Third-trimester | ||||||||||
| N | 22 | 32 | 22 | 32 | 22 | 32 | ||||
| At rest | 5.72 |
5.44 |
n.s. | 4.09 |
3.96 |
n.s. | 17.40 |
16.40 |
n.s. | |
| At max Kegel | 4.78 |
4.47 |
n.s. | 3.88 |
3.62 |
n.s. | 14.32 |
12.45 |
n.s. | |
| At max Valsalva | 6.03 |
5.85 |
n.s. | 4.44 |
4.24 |
n.s. | 20.09 |
18.92 |
n.s. | |
| Postpartum* | ||||||||||
| N | 21 | 31 | 21 | 31 | 21 | 31 | ||||
| At rest | 5.57 |
5.26 |
n.s. | 3.91 |
3.68 |
0.0167† | 16.48 |
14.76 |
0.0310† | |
| At max Kegel | 4.64 |
4.25 |
n.s. | 3.64 |
3.57 |
n.s. | 13.12 |
11.48 |
0.0145† | |
| At max Valsalva | 5.80 |
5.26 |
0.0475† | 4.22 |
3.93 |
0.0125† | 19.22 |
16.00 |
0.0120† | |
VD, vaginal delivery; CS, cesarean section; *, patients who had CS have been excluded from the VD group, and patients who had VD have been excluded from the CS group; †, statistically significant; n.s., not significant; a-p, anterior-posterior; l-r, left-right; N, number.
In this prospective study, pregnant women with a history of VD were compared with those with a history of CS. We have shown that during pregnancy, US measurements of the levator hiatus in multiparous women significantly increased from the first- to the second- and third-trimesters. Furthermore, this study demonstrates that in multiparous women, many dimensions of the levator hiatus decrease significantly postpartum, whether following a non-traumatic vaginal birth or a CS. Finally, this study indicates that the incidence of new levator trauma during VD is reduced in women with a history of previous vaginal births.
In the present study, there was only one new LAM trauma in the women of the VD subgroup (1/27, 3.7%). This finding confirms the already low published rates of new LAM avulsion after a second VD. Chan et al. [21] evaluated 151 multiparous women after their second delivery and found a 0.9% rate of new LAM avulsion. Another important issue is the possibility of LAM injury following VBAC. Epidemiologically, CS appears to offer partial protection against POP. This could be explained because of the very low rates of LAM trauma following CS. In the literature, Horak et al. [30] reported a new case of avulsion following VBAC in 6 women who had a successful VBAC (1/6, 16.7%). In the present study, 3 women delivered via VBAC, and 1 suffered a LAM injury (1/3, 33.3%). These findings highlight a potential risk for LAM injury in multiparous women attempting VBAC, which may have implications for future symptoms of POP.
Changes in the dimensions of the levator hiatus in nulliparous women during pregnancy and after delivery have been investigated in several studies. These studies have shown that the dimensions of the hiatal opening increase as pregnancy progresses [22, 23, 24, 25, 26, 27]. Following delivery, parameters influencing hiatal dimensions include (i) the mode of delivery, and (ii) the presence of pelvic floor trauma [22, 23, 24, 25, 26, 27]. In multiparous women, hiatal dimensions are expected to exhibit trends quite similar to those observed in primiparous during pregnancy and after delivery. Antenatal measurements appear to support this expectation. Both VD and CS subgroups of multiparous womenexhibit a similar trend, with an increase in hiatal dimensions as pregnancy progresses towards term. Paradoxically, postnatal measurements do not enterally align with the observations from nulliparous cohorts. On the one hand, as expected, the CS subgroup exhibits a significant reduction in hiataldimensions postpartum. On the other hand, the VD subgroup also demonstrates a significant reduction in the hiatal dimensions following delivery. Despite differing initial measurements in the first-trimester, the two subgroups exhibit nearly identical trends in the alterations to the leavator hiatus (LH) area sustain during pregnancy and after delivery. The most likely explanation for these findings is the absence of new levator trauma in women with previous VD. Apparently, the effects of childbirth primarily impact the pelvic floor muscles during the first VD, with subsequent vaginal births not significantly affecting their integrity.
According to our results, all hiatal dimensions are significantly increased in the VD subgroup compared with the CS delivery subgroup. This finding is consistent with the published literature. In detail, Kamisan Atan et al. [33] conducted a retrospective study using 3D-TPUS to examine women with POP symptoms. They found that multiparous women who had delivered vaginally exhibited a significantly larger LH area during Valsalva compared to those who had undergone CS [33].
Changes in hiatal dimensions and pelvic floor trauma during pregnancy and delivery are key factors associated with the developmentof POP later in life. A third influential epidemiological parameter contributing to the development of POP is the number of pregnancies, particularly the number of VD. Epidemiologically, the incidence of POP appears to increase in direct proportion to parity [34, 35]. Our study results cast doubt on the precise role of multiparity in the pathophysiology of POP. Apparently, pregnancy alone does not appear to be traumatic enough to induce the prerequisites for POP. If it were, one might expect that multiparous women who delivered by CS would also have POP symptoms. However, this has not been confirmed in epidemiologically. Therefore, we could presume that LAM trauma sustained during VD is the single most important peripartum factor leading to POP in multiparous women with a history of VD.
Our results are in agreement with recent literature and challenge the significance of subsequent VDs in the development of POP later in life. Jundt et al. [29], in a small study, concluded that a second VD did not further compromise the pelvic floor. Kamisan Atan et al. [33] retrospectively studied a large cohort of urogynecology patients and concluded that subsequent deliveries do not appear to have any effect on hiatal dimensions. Horak et al. [30] concluded that a second pregnancy and delivery do not appear to have a major effect on levator function and bladder support. Overall, it appears that subsequent vaginal deliveries do not negatively impact the pathophysiology of POP in women with a history of VD, especially in the absence of new LAM trauma.
The findings of this study indicate that (i) the likelihood of LAM trauma during subsequent vaginal births is low and (ii) there is a peripartum reduction in hiatal area in multiparous women, regardless of their previous delivery mode. These findings differ from data on nulliparous women in the literature and may imply that most pelvic floor injuries to the occur duringthe first VD. Such a conclusion could only be reached through detailed prospective studies where multiparous women with history of traumatic VD are compared with those multiparous women with history of non-traumatic VD, and both groups are followed for a long period of time. As such, other important perinatal, genetic or behavioral factors could be identified and further investigated. However, postpartum identification of LAM trauma could potentially serve as a screening tool for clinical surveillance of women at high risk of developing symptomatic POP later in life.
To the best of our knowledge, this is the first study that prospectively followed multiparous women from the first-trimester through to the postpartum period using 3D-TPUS to investigate ongoing LAM changes. Multiparous women appear to exhibit a different trend in the alterations of the levator hiatus after delivery compared to the nulliparous women. Studies involving nulliparous women can serve as a basis for comparison with our findings and vice versa.
Limitations of our study include: (i) the relatively small sample size and the increased number of missing follow-up examinations; (ii) the high rates of CSs in tertiary referral centers in Greece; (iii) the lack of analysis of different grades of multiparity, which may reduce the statistical power of our sample; (iv) the scheduling of the third-trimester US scan at 32 weeks, which may miss any additional changes before birth and hinders direct comparisons with findings from other published studies.
This study found that in multiparous women who deliver vaginally, the dimensions of levator hiatus increase during pregnancy and decrease after delivery. A similar trend is identified in multiparous women who deliver with CS. The incidence of new LAM trauma is reduced in multiparous women with a history of previous vaginal births who deliver vaginally. Further studies involving multiparous women who deliver vaginally, both with and without levator hiatus trauma, are warranted in order to elucidate the influence of multiple deliveries (traumatic or otherwise) on the pelvic floor.
All data points generated or analyzed during this study are included in this article and there are no further underlying data necessary to reproduce the results.
AS clinical and ultrasound examinations of patients, data collection and analysis, drafting of the manuscript; TM study conception, design and supervision; APA and EA study conception and design; MZ and GG analysis and interpretation of data, revision of the manuscript for important intellectual content; PP and DT analysis and interpretation of data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Medical School of the Aristotle University of Thessaloniki, Greece (No. 3767/2011).
We would like to thank all those from the medical and nursing staff of the 1st Department of Obstetrics and Gynecology of the Aristotle University of Thessaloniki who helped us conduct this study. We would like to express our gratitude to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.