


 , Busra Soner 2, Reyhan Aslancan Bayram 3, Berna Aslan Cetin 3
, Busra Soner 2, Reyhan Aslancan Bayram 3, Berna Aslan Cetin 31 Department of Perinatology, Basaksehir Cam and Sakura City Hospital, 34480 Istanbul, Turkey
2 Department of Obstetrics and Gynecology, Gaziantep City Hospital, 27000 Gaziantep, Turkey
3 Department of Obstetrics and Gynecology, Basaksehir Cam and Sakura City Hospital, 34480 Istanbul, Turkey
Abstract
Cesarean hysterectomy is a common approach to managing placenta accreta spectrum (PAS); however, the morbidities related to cesarean hysterectomy are not yet fully understood. This study aimed to investigate urinary incontinence (UI) symptoms and sexual function in patients who underwent hysterectomy due to PAS.
This prospective cohort study was conducted at Basaksehir Cam and Sakura City Hospital in Istanbul, Turkey. The study group included 51 patients who had a cesarean hysterectomy due to PAS and 51 patients in the control group who underwent a cesarean section (CS) at term. Patients in both groups were evaluated 6 to 12 months after surgery. The patients completed the International Consultation on Incontinence Questionnaire for Female Lower Urinary Tract Symptoms Modules (ICIQ-FLUTS) for UI symptoms and the Female Sexual Function Index (FSFI). The PAS group was further divided into patients with and without bladder invasion of the placenta.
The ICIQ-FLUTS total score, as well as the filling, voiding, and incontinence subdomain scores, and post-void residual urine volume, were statistically significantly higher in the PAS group than in the control group (p < 0.05). The FSFI total score and the subdomain scores for arousal, lubrication, orgasm, satisfaction, and pain were statistically significantly lower in the PAS group than in the control group (p < 0.05). Subgroup analysis of the PAS group showed no statistically significant difference in UI and sexual function between hysterectomized patients with and without placental invasion of the bladder.
Patients with PAS who undergo cesarean hysterectomy have a higher incidence of UI and impaired sexual function postoperatively compared to patients who undergo ordinary CS, regardless of bladder invasion.
Keywords
- FSFI
- hysterectomy
- ICIQ-FLUTS
- PAS
- physiological sexual dysfunction
- placenta accreta spectrum
- urinary incontinence
Postpartum urinary incontinence (UI) is quite common, with about 20% of women experiencing UI after vaginal delivery. Comparatively, UI is much less common after cesarean section (CS) compared to vaginal delivery [1]. Although vaginal delivery seems to be more strongly associated with urinary symptoms, cesarean delivery is also linked to these symptoms due to the multifactorial nature of urinary retention and incontinence [2, 3]. Bladder trauma during CS or vaginal delivery, as well as prolonged catheterization, may lead to nerve fiber damage, resulting in detrusor dysfunction [4].
Placenta accreta spectrum (PAS) is an umbrella term that describes abnormal trophoblastic invasion into the myometrium, ranging from superficial adherence to deeper invasion and potential involvement of adjacent organs. PAS is a complication in approximately 3 in 1000 pregnancies and poses significant maternal risks, particularly due to massive obstetric hemorrhage at the time of placental separation. This condition is associated with a high likelihood of blood transfusion, perioperative complications, and the need for hysterectomy to control life-threatening bleeding. PAS-related complications may include injury to surrounding organs, coagulopathies, thromboembolism, infection, multisystem organ failure, and even maternal death [5]. A study confirms that hysterectomy, whether elective or postpartum, is associated with an increased incidence of UI [6]. Christoffersen et al. [6] reported a 2.6-fold higher adjusted hazard for stress UI (SUI) surgery after hysterectomy. Moreover, it has been postulated that bladder trauma during the procedure, through stretch injury or interruption of detrusor innervation, may lead to impaired detrusor function and consequential incontinence.
Although UI and urinary retention are commonly associated with parturition, sexual function is also an important issue that may differ after delivery. This subject has both physiological and psychological components. A study compared the mode of delivery and sexual function after childbirth [7]. However, research on sexual function following pregnancy-related hysterectomy remains limited.
Thus, this study aimed to examine the relationship between hysterectomy due to PAS and UI and sexual function by comparing patients who underwent CS with those who had a cesarean hysterectomy due to PAS.
This study was designed as a prospective cohort study at the Obstetrics and Gynecology and Perinatology Clinics of Basaksehir Cam and Sakura City Hospital between March 2022 and April 2023. All eligible patients within the specified timeframe were included; hence, no prior sample size calculation was performed. Ethical approval was obtained from the local ethical committee of Basaksehir Cam and Sakura City Hospital (Ethic Approval Number: KAEK/2023.05.179). Although the surgical procedures occurred between March 2022 and April 2023, prospective data collection (including administration of questionnaires and clinical follow-up) began only after ethical approval (Ethic Approval Number: KAEK/2023.05.179). No patient-reported data were collected before approval. A total of 51 patients in the PAS group and 51 patients in the control group were included in the study. The PAS group comprised patients who underwent cesarean hysterectomy due to PAS. These 51 patients were diagnosed in the perinatology clinic at our hospital based on ultrasound findings. Of these, 10 patients had placental invasion into the bladder, which was diagnosed via obstetric ultrasound and further confirmed during surgery. These patients were followed until the 34th week of gestation, after which a CS was planned with appropriate preparations for potential blood transfusion. Cesarean hysterectomies were performed by consultant specialist doctors of perinatology, without an attempt to remove the placenta. The control group consisted of 51 patients who underwent CS as the first scheduled cesarean case on the same day as the study group, primarily due to a history of a previous CS. Patients with multiple gestations, preterm labor, emergency hysterectomy, uterus-preserving segmental resection, renal dysfunction, renal failure, and neurological diseases were excluded from the study. A detailed study flowchart, including exclusion criteria, is shown in Fig. 1.
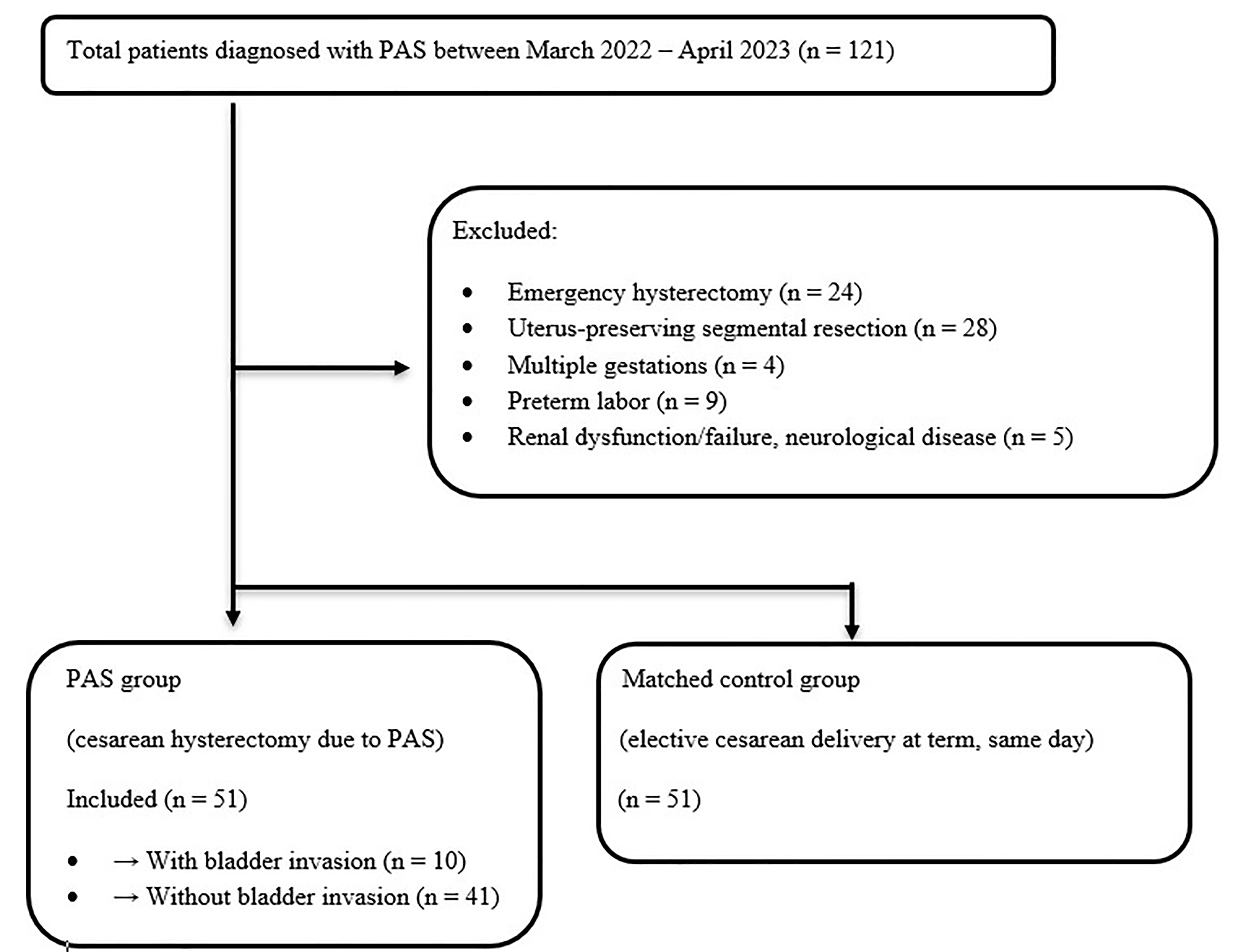 Fig. 1.
Fig. 1.
Study flowchart. PAS, placenta accreta spectrum.
UI was the primary outcome measure in the study, while the secondary outcome
measure was sexual function following surgery. Patients in both groups were
contacted and examined at our center regarding incontinence and sexual function
between six months and one year after surgery. After recording the medical
histories of each patient, the patients completed two questionnaires to assess
their micturition and sexual function history post-surgery. Next, the
Turkish-validated version of the International Consultation on Incontinence
Questionnaire for Female Lower Urinary Tract Symptoms Modules (ICIQ-FLUTS) was
used to evaluate UI and related impact on quality of life [8]. This questionnaire
comprised 12 questions, each scored from 0 to 4, to assess the daily urinary
routines of patients. Filling, voiding, and incontinence symptoms were subscaled
based on the scores of the relevant questions. To assess sexual function, the
Turkish-validated version of the Female Sexual Function Index (FSFI) was used
[9]. The FSFI questionnaire consists of 19 questions, rated from 0 to 6, focusing
on six main domains: desire, arousal, lubrication, orgasm, satisfaction, and
pain. Sexual dysfunction was defined as a FSFI total score
Statistical analysis was performed using the Statistical Package for the Social
Sciences (SPSS) v.19.0 (IBM Corp., Chicago, IL, USA). The normality of the data was
assessed using the Kolmogorov-Smirnov and Shapiro-Wilk test. For variables that
were normally distributed, data are presented as the mean
The demographic variables of 51 patients undergoing PAS hysterectomy (PAS group) and 51 patients undergoing CS (control group) are shown in Table 1. Age, parity, body mass index (BMI), number of previous CS deliveries, comorbidities, and medication use were similar between the two groups. A statistically significant difference was found in the mean gravidity between the two groups, with patients in the PAS group having a higher number of gravidities than those in the control group (p = 0.003) (Table 1).
| PAS group | Control group | p-value | ||
| n = 51 | n = 51 | |||
| Age (years) | 34.16 |
32.69 |
0.141 | |
| Gravida | 4.27 |
3.47 |
0.003 | |
| Parity | 3.27 |
3.24 |
0.833 | |
| BMI (kg/m2) | 28.92 |
29.37 |
0.641 | |
| Number of previous CS | 3.14 |
3.04 |
0.599 | |
| Comorbidity | 7 (13.7%) | 9 (17.6%) | 0.586 | |
| Medication use | 5 (9.8%) | 6 (11.8%) | 0.750 | |
| Preoperative Hb (mg/dL) | 10.39 |
11.69 |
||
| Hb drop (mg/dL) | 1.41 |
1.65 |
0.310 | |
| Postoperative PAS diagnosis (n) | - | - | ||
| Accreta | 12 (23.6%) | |||
| Increta | 6 (11.8%) | |||
| Percreta | 33 (64.8%) | |||
BMI, body mass index; CS, cesarean section; Hb, hemoglobin; n, number; PAS, placenta accreta spectrum.
The total scores from the ICIQ-FLUTS questionnaire, as well as the scores for
the filling, voiding, and incontinence subdomains, positive Valsalva stress test
results, and residual urine volumes for both groups, are presented in Table 2.
The ICIQ-FLUTS total score, filling, voiding, and incontinence subdomain scores
were statistically significantly higher in the PAS group than in the control
group (p
| PAS group | Control group | p-value | |
| n = 51 | n = 51 | ||
| ICIQ-FLUTS total score | 4.00 (1.00–9.00) | 1.00 (0.00–4.00) | |
| ICIQ-FLUTS f score (filling) | 2.00 (1.00–4.00) | 1.00 (0.00–2.00) | 0.002 |
| ICIQ-FLUTS v score (voiding) | 0.00 (0.00–1.00) | 0.00 (0.00–0.00) | 0.010 |
| ICIQ-FLUTS i score (incontinence) | 1.00 (0.00–3.00) | 0.00 (0.00–1.00) | 0.005 |
| Positive Valsalva stress test | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.094 |
| Residual volume (mL) | 5.54 (2.24–11.9) | 3.20 (1.09–5.82) | 0.004 |
Data are presented as the median (25th–75th percentile) for non-normally distributed variables. Normality was assessed using the Kolmogorov-Smirnov test. The Mann-Whitney U test was applied for non-normally distributed data.
ICIQ-FLUTS, International Consultation on Incontinence Questionnaire for Female Lower Urinary Tract Symptoms.
The FSFI total scores and the scores for desire, arousal, lubrication, orgasm,
satisfaction, and pain subdomains are presented in Table 3. The FSFI total score,
as well as the subdomain scores for arousal, lubrication, orgasm, satisfaction,
and pain, were statistically significantly lower in the PAS group compared to the
control group (p
| PAS group | Control group | p-value | |
| n = 51 | n = 51 | ||
| FSFI total score | 21.02 |
25.25 |
|
| FSFI desire score | 3.60 (2.40–3.60) | 3.60 (3.00–4.80) | 0.080 |
| FSFI arousal score | 3.32 |
3.83 |
0.018 |
| FSFI lubrication score | 3.70 |
4.24 |
0.010 |
| FSFI orgasm score | 3.60 (2.40–4.40) | 4.40 (4.00–4.80) | |
| FSFI satisfaction score | 4.40 (2.80–4.80) | 4.80 (4.40–5.60) | 0.005 |
| FSFI pain score | 3.40 |
4.34 |
Data are presented as the mean
A subgroup analysis within the PAS group (with vs. without bladder invasion) revealed no significant differences in urinary or sexual function outcomes (Table 4).
| PAS patients without bladder invasion (Group B, n = 41) | PAS patients with placental invasion of the bladder (Group A, n = 10) | p-value | |
| Age (years) | 35.20 |
33.90 |
0.452 |
| Gravidity | 4.29 (3.00–5.00) | 4.20 (2.75–5.50) | 0.708 |
| Parity | 3.27 (2.00–4.00) | 3.30 (2.75–4.00) | 0.892 |
| BMI (kg/m2) | 28.63 |
28.99 |
0.816 |
| Number of previous CS | 3.12 (2.00–4.00) | 3.20 (2.75–4.00) | 0.710 |
| ICIQ-FLUTS total score | 5.88 (1.00–9.50) | 4.10 (0.00–7.75) | 0.278 |
| ICIQ-FLUTS f score (filling) | 3.20 (1.00–4.50) | 1.90 (0.00–4.25) | 0.254 |
| ICIQ-FLUTS v score (voiding) | 0.00 (0.00–1.50) | 0.00 (0.00–0.00) | 0.053 |
| ICIQ-FLUTS i score (incontinence) | 1.90 (0.00–3.00) | 2.10 (0.00–5.00) | 0.910 |
| FSFI total score | 20.79 |
21.07 |
0.893 |
| FSFI desire score | 3.22 (2.40–3.90) | 3.48 (3.00–3.90) | 0.638 |
| FSFI arousal score | 3.48 |
3.28 |
0.619 |
| FSFI lubrication score | 3.33 |
3.79 |
0.414 |
| FSFI orgasm score | 3.24 |
3.46 |
0.603 |
| FSFI satisfaction score | 3.90 (2.80–4.80) | 3.88 (2.40–5.60) | 0.914 |
| FSFI pain score | 3.38 |
3.41 |
0.942 |
| Residual volume (mL) | 8.08 (2.07–12.74) | 7.41 (2.50–12.46) | 0.981 |
Data are presented as the mean
In the binary logistic regression analysis (Table 5), only PAS group status was significantly associated with postoperative sexual dysfunction odds ratio (OR) = 3.709, 95% confidence interval (CI) [1.121–12.280]; p = 0.032. Other variables, including age, gravidity, parity, BMI, bladder invasion, and ICIQ total score, were not found to be significant predictors.
| Predictor variable | B | SE | Wald |
p-value | OR | 95% CI |
| Age | 0.055 | 0.054 | 1.026 | 0.311 | 1.056 | [0.950–1.174] |
| Gravida | 0.359 | 0.256 | 1.976 | 0.160 | 1.433 | [0.868–2.365] |
| Parity | –0.101 | 0.380 | 0.070 | 0.791 | 0.904 | [0.429–1.905] |
| Bladder invasion | 0.524 | 0.820 | 0.408 | 0.523 | 1.689 | [0.338–8.427] |
| BMI | 0.025 | 0.055 | 0.214 | 0.644 | 1.026 | [0.921–1.142] |
| ICIQ total score | –0.014 | 0.054 | 0.070 | 0.792 | 0.986 | [0.887–1.096] |
| PAS group | 1.311 | 0.611 | 4.606 | 0.032 | 3.709 | [1.121–12.280] |
Logistic regression analysis was conducted to identify predictors of postoperative sexual dysfunction. The OR indicates the likelihood of the outcome occurring per unit increase in the predictor variable. A p-value less than 0.05 was considered statistically significant. B, regression coefficient; SE, standard error; OR, odds ratio; CI, confidence interval.
Sexual dysfunction was defined as an FSFI total score
PAS is a serious condition that can result in significant maternal and fetal morbidity and mortality. Research on UI in PAS patients is limited, particularly in those who undergo hysterectomy during CS. Therefore, this study aimed to investigate the symptoms of UI and sexual function in patients who had a hysterectomy during CS due to PAS. Demographic variables were similar between the two groups, with BMI being notably comparable. This is important as obesity is a major contributor to UI. Although UI and impaired sexual function are also observed after hysterectomy performed for other benign indications, the unique characteristics of PAS surgery may impose additional risk. Our findings indicate that UI symptoms, increased post-void urinary volume, and impaired sexual function are more common in patients who underwent hysterectomy due to PAS compared to those who underwent a CS at term. The only exception was the FSFI desire score, which was similar between the two groups. This may be due to desire being more psychological in nature, whereas arousal, lubrication, orgasm, and satisfaction are more closely related to the physiological components of sexual activity.
Bladder injury and Valsalva stress test positivity were similar between the two groups. This suggests two possible explanations: first, UI symptoms in the PAS group may be predominantly due to urge incontinence, as evidenced by the increased urinary retention; second, bladder injury and subsequent repair may not be the primary contributors to the observed UI symptoms. Additionally, intense bladder dissection during a PAS hysterectomy may contribute to detrusor dysfunction and increased urgency.
There were no significant differences in demographic variables, ICIQ-FLUTS scores, or FSFI total and subdomain scores between patients with PAS-related hysterectomy and bladder invasion of the placenta and those without bladder invasion. This indicates that the observed differences in UI symptoms and sexual function are not attributable to placental invasion or bladder injury during surgery. Rather, advanced bladder dissection during hysterectomy, compared to CS, and resulting detrusor trauma may be the contributing factors.
Crocetto et al. [11] compared 47 patients who underwent planned cesarean hysterectomy due to PAS with 100 patients who had a CS at term in terms of UI. Notably, Crocetto et al. [11] found that patients who underwent cesarean hysterectomy had a higher prevalence of UI. Moreover, SUI was significantly more common in the PAS group. However, the lack of an objective tool to diagnose UI in this study may limit the accuracy of the findings. In contrast, the validated questionnaires used in our study provide a more objective assessment of UI symptoms and sexual function.
Hysterectomy may influence UI symptoms, and several studies have investigated this in relation to UI and sexual function. Axelsen et al. [12] studied 100 patients who had a radical hysterectomy due to cervical cancer and found that 50 experienced UI symptoms, while the others were continent. This finding led Axelsen et al. [12] to suggest that a decrease in intraurethral pressure may contribute to UI. Heydari et al. [13] examined the relationship between SUI symptoms and hysterectomy in 120 patients and found that hysterectomized patients had significantly lower Valsalva leak point pressure, supporting the idea that hysterectomy increases the risk of SUI. These findings highlight that ligamentous defect, particularly the pubourethral ligament, after hysterectomy may lead to both stress and urge UI symptoms [14].
Dedden et al. [15] conducted a prospective multicenter study assessing sexual function after hysterectomy for benign indications and found that FSFI scores significantly improved over time, with the most notable changes occurring within the first 12 months postoperatively. In contrast, our study revealed that PAS-related cesarean hysterectomy was independently associated with higher rates of postoperative sexual dysfunction. One key difference may stem from the surgical context; meanwhile, the cohort in Dedden et al. [15] underwent elective hysterectomies primarily for benign conditions, our population experienced high-risk, semi-elective cesarean hysterectomies for PAS, often accompanied by factors that may contribute to postoperative morbidity and impaired sexual health. Berlit et al. [16] compared sexual function outcomes between total and subtotal hysterectomy patients and found that, although the subtotal hysterectomy group had higher FSFI scores at three months post-surgery, there were no statistically significant differences between the two groups at one-year post-surgery. In our study, while the FSFI scores were significantly lower in the PAS group, sexual function may have been influenced by the removal of the uterine cervix and vaginal shortening. Recent report also highlights a growing trend toward conservative surgical approaches and meticulous intraoperative planning to minimize complications, particularly bladder injury, during cesarean hysterectomy for PAS [17]. Techniques such as performing vesicouterine dissection before uterine incision, applying tourniquets to control bleeding, and achieving hemostasis before the uterus removal with the placenta have been proposed to reduce the risk of bladder trauma and improve surgical outcomes [17].
Our study has some limitations. First, we did not assess post-void residual volume preoperatively. However, since pregnancy is a known risk factor for increased urinary retention, a baseline measurement may not have significantly impacted our findings. Second, our control group did not consist of patients who underwent hysterectomy for benign indications. As such, the older age of patients and potential for higher baseline UI and sexual dysfunction may represent a confounding factor. Another important limitation is the absence of baseline FSFI data before surgery or pregnancy. Thus, without preoperative sexual function scores, determining the extent to which PAS or its surgical treatment contributes to postoperative dysfunction is difficult. Future studies should prospectively assess sexual function and urinary symptoms and assessments from early in the pregnancy or even before conception.
Female sexual function is a multifactorial phenomenon that is influenced by physiological factors and psychological, social, cultural, and economic conditions; in particular, low- and middle-income economic status can further complicate access to adequate care and follow-up in PAS cases [18, 19], especially in tertiary healthcare centers where patient volume is particularly high [20]. In particular, according to the mother-baby friendly facilities framework by the International Federation of Gynecology and Obstetrics (FIGO), this vulnerable patient group requires especially multidisciplinary extra care [21].
Additionally, we performed multivariate logistic regression analysis for sexual
dysfunction based on the FSFI cut-off score of
The strength of this study lies in the use of validated questionnaires (ICIQ-FLUTS and FSFI) to assess UI and sexual function, which provides a more objective evaluation of these outcomes. Moreover, to our knowledge, this is the first study to demonstrate the independent impact of PAS-related hysterectomy on sexual function. Nonetheless, long-term follow-up studies are needed to validate and expand upon our findings, particularly regarding the persistence or evolution of symptoms over time.
In conclusion, patients who underwent hysterectomy due to PAS experience more UI symptoms and lower sexual function compared to patients who underwent a CS at term. Given the significant morbidities associated with PAS and the substantial impact of UI on quality of life, further studies are needed to explore the relationship between UI and hysterectomy due to PAS.
The raw data will be publicly available as of the date of publication. All data reported in this paper will also be shared by the corresponding author upon request.
IP designed the research study. BS and RAB collected the data. IP wrote and revised the final version of the manuscript. BAC analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the Ethics Committee of Basaksehir Cam and Sakura City Hospital (Ethic Approval Number: KAEK/2023.05.179), and all of the participants provided signed informed consent.
The authors would like to thank Dr. Tugce Tunc Arslanoglu and Dr. Kubra Keskin Toptas for their valuable assistance during the early preparation stages of this manuscript.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work, the authors used ChatGPT-3.5 in order to check spelling and grammar for the discussion section. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.