








 , Mei Zhang 1, Chengen He 1,*
, Mei Zhang 1, Chengen He 1,*
1 Department of Neonatology, Renmin Hospital, Hubei University of Medicine, 442000 Shiyan, Hubei, China
Abstract
This study employed a meta-analysis approach to investigate the incidence of intrahepatic cholestasis of pregnancy (ICP) and its impact on adverse outcomes in both pregnant and postpartum women, as well as neonates.
We obtained studies published from the inception of the PubMed, Cochrane Library, and Web of Science databases through January 2024. A total of 21 original articles were included, reporting on ICP and its associated adverse outcomes in maternal and neonatal populations. The included studies involved 1,497,951 controls non-intrahepatic cholestasis of pregnancy (non-ICP) and 12,262 ICP patients. Sensitivity analyses and evaluations for publication bias were also conducted.
The pooled analysis estimated an ICP incidence of 3% (95% confidence interval [CI], 1%–7%), while the meta-analysis demonstrated the following risk ratios: postpartum hemorrhage showed a relative risk (RR, 0.82; 95% CI, 0.69–0.99), whereas significant increases were observed for preeclampsia (RR, 2.39; 95% CI, 2.21–2.59), Cesarean section (RR, 1.28; 95% CI, 1.15–1.42), preterm birth (RR, 2.71; 95% CI, 1.77–4.15), and maternal infection (RR, 3.22; 95% CI, 2.48–4.19). Other outcomes included labor induction (RR, 1.60; 95% CI, 0.51–4.99), gestational diabetes mellitus (GDM; RR, 1.29; 95% CI, 0.83–2.01), stillbirth (RR, 1.25; 95% CI, 0.64–2.42), and small for gestational age (SGA; RR, 1.06; 95% CI, 0.71–1.57), which were not statistically significant. Neonatal intensive care unit (NICU) admission (RR, 1.79; 95% CI, 1.35–2.37), with a significant increase in risk.
This meta-analysis demonstrates a global incidence of ICP at 3% and identifies significant associations with adverse maternal and neonatal outcomes. ICP is associated with increased risks of preeclampsia, Cesarean section, preterm birth, maternal infection, and neonatal intensive care needs. Interestingly, a relative risk of postpartum hemorrhage was observed, suggesting the need for further investigation into the underlying mechanisms. Although labor induction, GDM, and stillbirth showed non-significant trends toward increased risk, their clinical relevance persists. These findings underscore the necessity for risk-stratified surveillance in ICP management, emphasizing infection control and preterm prevention, alongside regionally tailored clinical protocols.
The study has been registered on https://inplasy.com/inplasy-2025-3-0132/ (registration number: INPLASY202530132).
Keywords
- intrahepatic cholestasis of pregnancy
- maternal health
- neonatal health
- risk factors
- meta-analysis
Intrahepatic cholestasis of pregnancy (ICP) is a liver condition that occurs during pregnancy. It is mainly characterized by intrahepatic cholestasis and heightened bile acid levels. Pruritus is often a significant symptom, especially in the third trimester of pregnancy [1]. ICP is the most common pregnancy-related liver disease that poses a threat on maternal-fetal health. It is associated with maternal risks, including preterm labor and postpartum hemorrhage, potential hepatic impairment in postpartum women, and neonatal complications such as asphyxia and meconium aspiration syndrome [2]. As reported, the global incidence of ICP varies widely by region, with significantly higher incidence rates observed in certain high-risk populations and regions [3]. In Scandinavia and several Asian countries, including China and India, the incidence of ICP exceeds the global average [3]. Women with a family history of the disease, advanced maternal age, or preexisting liver conditions or pregnancy complications are at higher risk of developing ICP [4]. These variations may be closely associated with genetic susceptibility, environmental factors, and the quality of prenatal care.
The pathophysiology of ICP involves hormonal fluctuations, bile acid dysmetabolism, and genetic susceptibility, with emerging evidence highlighting immune dysregulation as a contributor to its inflammatory nature [5, 6, 7]. ICP is associated with a range of maternal and neonatal complications, beyond the common symptoms of pruritus and liver dysfunction [8]. ICP increases the risk of preterm delivery, fetal distress, and other adverse fetal outcomes due to elevated bile acids, which can disrupt placental function, impair nutrient and oxygen transfer, and exacerbate intrauterine stress. Furthermore, ICP is linked to heightened risks of gestational diabetes mellitus (GDM), postpartum hemorrhage, and even fetal stillbirth, with cardiac arrhythmia being a primary cause of fetal death in severe cases [9]. While effective management can improve outcomes, the condition remains a significant obstetric risk, requiring careful monitoring and clinical attention [10, 11]. Therefore, this study aims to systematically evaluate the impact of ICP on maternal and neonatal outcomes, offering clearer evidence for optimizing clinical management.
Although existing literature has preliminarily explored the epidemiological features, pathological mechanisms, and the effects of ICP on pregnant and postpartum women, as well as neonates, significant heterogeneity exists in the quantitative assessment of ICP incidence and neonatal adverse outcomes. This variability arises from differences in study design, sample size, data quality, and regional factors. Current studies lack unified incidence data, and significant controversy remains regarding the factors influencing adverse outcomes, as incidence rates and baseline characteristics of patients vary across regions. This study aims to conduct a systematic evaluation and meta-analysis to integrate high-quality research data, accurately estimate the incidence of ICP, and quantify its specific impact on adverse outcomes in pregnant and postpartum women, as well as neonates. This study synthesizes robust epidemiological evidence to inform risk stratification models and optimize clinical decision-making for ICP. The findings supports the development of targeted screening protocols and preventive strategies, ultimately contributing to improved maternal-fetal health outcomes.
The study protocol was registered on INPLASY (registration number: INPLASY202530132) in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist.
A thorough search was performed in the PubMed (https://pubmed.ncbi.nlm.nih.gov), Cochrane Library (https://www.cochranelibrary.com), and Web of Science (https://www.webofscience.com) databases. Relevant papers published from the inception of these databases through January 2024 were included. The focus was on studying the incidence of ICP and its impact on adverse outcomes in pregnant and postpartum women, as well as neonates. Search terms encompassed: (“Intrahepatic cholestasis of pregnancy”) AND (“Emergency Cesarean sections” OR “Postpartum hemorrhage” OR “Cesarean delivery” OR “Preeclampsia” OR “Hemorrhage” OR “Unplanned cesarean sections” OR “Preterm birth” OR “Premature delivery” OR “Small for gestational age” OR “Stillbirth” OR “Neonatal intensive care unit” OR “NICU admission” OR “Neonatal outcomes” OR “Perinatal complications”). Search strategies were tailored to meet the requirements of each database. All references from the included studies were manually checked to identify any potentially overlooked research. Two researchers independently conducted the screening and cross-validated the results. If disagreements arose, a third researcher was responsible for making the final decision. The screening process involved reviewing titles, abstracts, and full texts.
Inclusion criteria were as follows: ① Participants (P) included pregnant women diagnosed with ICP; ② Intervention (I): ICP; ③ Control (C): pregnant women without ICP; ④ Outcomes (O): adverse maternal and neonatal outcomes; and ⑤ Study Design (S): clinical trials, observational studies, or systematic evaluations. The inclusion criteria comprised studies examining the impact of ICP on obstetric and neonatal outcomes, with comparisons between the ICP and non-intrahepatic cholestasis of pregnancy (non-ICP) groups.
Exclusion criteria: ① Studies not directly related to ICP or its associated factors; ② Articles focused on other liver diseases or conditions, rather than specifically targeting ICP; ③ Studies with unclear methodology; ④ Studies with small sample sizes (e.g., case reports, case series), lacking statistical power, or generalizability; ⑤ Animal studies, in-vitro experiments, or studies involving non-human subjects; ⑥ Articles published in languages other than English, without a reliable English translation; and ⑦ Studies with inaccessible full texts.
Relevant data were extracted from the included studies, including study type, groups, sample size, and average maternal age. Obstetric outcomes such as emergency Cesarean section (C-section) rate, preeclampsia, postpartum hemorrhage, gestational age, preterm delivery (spontaneous preterm birth), small for gestational age (SGA) infants, neonatal intensive care unit (NICU) admission rate, and stillbirth rate were also collected, with preterm delivery defined as gestational age less than 37 weeks. Additionally, risk assessment-related parameters from the studies were extracted. This comprehensive data extraction allowed us to assess the relationships between variables and their potential impact on maternal and neonatal health outcomes.
The ROBINS-I tool was used to assess the potential risk of bias in cohort studies. Two researchers independently evaluated the methodological quality of the included studies. Any discrepancies were resolved through consultation with a third researcher, who acted as an arbitrator. This rigorous process ensured a comprehensive and unbiased evaluation of the studies’ methodological strengths and limitations.
Relevant data were extracted from the included studies, including study design,
sample size, patient characteristics, and adverse outcomes. Two researchers
independently extracted the data and cross-validated the data. The 95%
confidence interval (CI) was calculated for each parameter. The I2 statistic
was employed to assess heterogeneity between studies. An I2 value greater
than 50% suggested significant heterogeneity. All meta-analyses were performed
using the RevMan 5.3 software (UK;
https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman).
For the assessment of publication bias, the trim and fill method was employed,
with detection conducted using both the Miller Method and the Harbord Method.
Common methods for calculating the pooled effect size include the Mantel-Haenszel
method for binary outcomes and the inverse-variance method for continuous
outcomes. Based on the heterogeneity results, a random effects model should be
chosen if p
A sensitivity analysis was performed to assess the impact of each study on the overall effect size. This involved repeating the meta-analysis by removing one study at a time. Any changes in the overall effect size were carefully observed. If removing any study did not lead to a notable change in the effect size, the meta-analysis results were considered stable.
Fig. 1 summarizes the results of the literature search and selection process. A total of 1526 articles were retrieved from the PubMed, Embase, and Web of Science databases. After a stepwise screening process, 21 original articles reporting on the correlation between ICP and adverse maternal and neonatal outcomes were included [9, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31]. Table 1 (Ref. [9, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31]) outlines the primary characteristics of these studies. The 21 studies encompassed 1,497,951 healthy controls and 12,262 ICP patients.
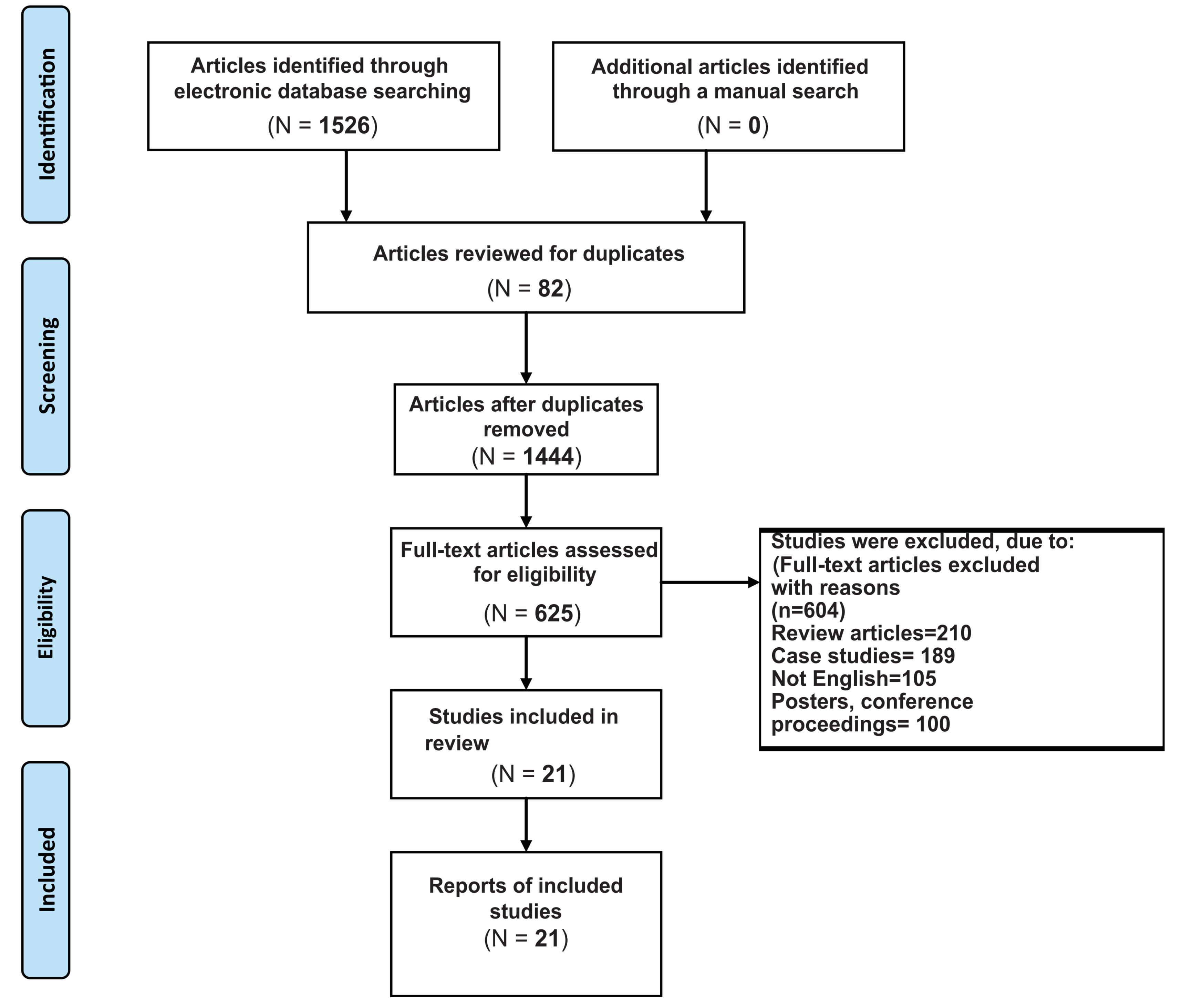 Fig. 1.
Fig. 1.
Literature screening flow chart.
| First Author | Heinonen et al. [29] | Turunen et al. [17] | Al Shobaili et al. [22] | Wikström Shemer et al. [19] | Martineau et al. [9] | Geenes et al. [13] | Kawakita et al. [28] | Furrer et al. [27] | Liu et al. [26] | Herrera et al. [23] | Ozel et al. [12] | Wang et al. [14] | Arthuis et al. [24] | Liu et al. [20] | Luo et al. [18] | Wu et al. [30] | Al-Obaidly et al. [25] | Begum et al. [16] | Li et al. [15] | Omeroglu et al. [21] | Chen et al. [31] | |
| Year of Publication | 1999 | 2010 | 2011 | 2013 | 2014 | 2014 | 2015 | 2016 | 2016 | 2018 | 2020 | 2019 | 2020 | 2020 | 2021 | 2022 | 2022 | 2023 | 2023 | 2023 | 2023 | |
| Country | Finland | Finland | Saudi Arabia | Sweden | UK | UK | USA | Switzerland | China | USA | Turkey | China | France | China | China | China | Qatar | India | China | Turkey | China | |
| Type of Study | PC | RC | PC | PC | RC | PC | RC | PC | PC | RC | CSC | RC | PC | PC | RC | RC | RC | PC | RCC | PCC | RC | |
| Numbers | ICP | 91 | 687 | 76 | 5477 | 143 | 669 | 26 | 345 | 129 | 487 | 40 | 40 | 140 | 911 | 114 | 1516 | 263 | 60 | 300 | 60 | 688 |
| non-ICP | 16,818 | 1374 | 200 | 1,208,191 | 57,581 | 2205 | 152 | 1725 | 1793 | 298 | 40 | 40 | 560 | 94,817 | 3725 | 38,226 | 31,230 | 60 | 300 | 60 | 38,556 | |
| Average Maternal age (years) | ICP | NA | 27.50 | 29.18 | NA | 30.80 |
29.60 | 30.20 | 27.50 | 32.40 | 29 |
NA | 29.50 |
29 | 30.80 | 30 | 31.20 | 35 | 27.63 | NA | NA | 29 |
| non-ICP | NA | 27.20 | 29.86 | NA | 30.60 |
29.00 | 29.70 | 27.70 | 30.70 | 29 |
NA | 29.50 |
29 | 30.60 | 30 | 31.13 | 35 | 26.73 | NA | NA | 29 | |
| Postpartum hemorrhage | ICP | NA | NA | 5.20% | NA | NA | NA | 12.70% | NA | NA | NA | NA | NA | 20.70% | 0.90% | 0.00% | 3.60% | 5.70% | NA | 1.00% | NA | 0.15% |
| non-ICP | NA | NA | 4.50% | NA | NA | NA | 9.90% | NA | NA | NA | NA | NA | 15.35% | 0.80% | 0.70% | 4.50% | 5.20% | NA | 0.70% | NA | 0.28% | |
| C-Section | ICP | 25.30% | 14.80% | 11.80% | 19.60% | 33.00% | 25.00% | 40.00% | 27.50% | NA | 32.00% | 37.50% | NA | 13.60% | 0.70% | 35.09% | 48.04% | 27.00% | 58.30% | NA | 50.00% | 51.31% |
| non-ICP | 15.80% | 10.60% | 8.50% | 15.60% | 29.00% | 23.00% | 38.20% | 27.70% | NA | 29.90% | 22.50% | NA | 10.90% | 0.30% | 21.93% | 38.50% | 31.30% | 35.00% | NA | 25.00% | 31.60% | |
| Preeclampsia | ICP | NA | NA | NA | 6.70% | NA | 6.60% | 7.30% | NA | 27.90% | NA | NA | NA | NA | 5.50% | 10.50% | 4.30% | 1.50% | NA | 8.00% | NA | 4.94% |
| non-ICP | NA | NA | NA | 2.70% | NA | NA | 7.20% | NA | 12.60% | NA | NA | NA | NA | 2.40% | 0.70% | 2.60% | 1.60% | NA | 0.70% | NA | 1.56% | |
| Preterm delivery | ICP | 14.30% | 44.00% | 11.80% | 0.50% | 2.10% | 25.00% | 46.20% | NA | 28.70% | 9.40% | NA | NA | 15.70% | 0.90% | 6.14% | 22.40% | 1.40% | 21.70% | 26.70% | NA | 18.60% |
| non-ICP | 5.50% | 12.00% | 9.00% | 0.70% | 0.30% | 6.50% | 14.50% | NA | 19.20% | 6.10% | NA | NA | 4.80% | 1.10% | 0.18% | 9.26% | 1.40% | 10.00% | 2.00% | NA | 4.87% | |
| Induction of labor | ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 82.10% | 4.10% | NA | NA | NA | 61.70% | NA | NA | NA |
| non-ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 18.40% | 6.70% | NA | NA | NA | 41.70% | NA | NA | NA | |
| Gestational diabetes mellitus | ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 18.40% | 20.20% | NA | NA | 13.30% | NA | 16.60% |
| non-ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 20.50% | 18.80% | NA | NA | 4.30% | NA | 14.00% | |
| Polyhydramnios oligohydramnios | ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0.90% | NA | NA | NA | 11.30% | NA | NA |
| non-ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 1.20% | NA | NA | NA | 3.70% | NA | NA | |
| Maternal infection | ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0.00% | 14.00% | NA | NA | 16.30% | NA | 13.50% |
| non-ICP | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0.70% | 5.10% | NA | NA | 2.70% | NA | 4.10% | |
| NICU admission | ICP | NA | NA | 15.70% | NA | NA | 12.00% | 20.40% | 15.90% | 50.20% | NA | 27.50% | NA | 2.90% | 29.50% | NA | 23.40% | 15.30% | 21.60% | NA | 23.30% | NA |
| non-ICP | NA | NA | 4.90% | NA | NA | 5.60% | 27.30% | 16.80% | 34.90% | NA | 0.00% | NA | 0.40% | 13.50% | NA | 14.60% | 11.80% | 5.00% | NA | 6.70% | NA | |
| Stillbirth | ICP | 0.00% | 1.20% | NA | 0.30% | 2.10% | 1.50% | 0.00% | 0.90% | NA | 2.90% | NA | NA | 0.00% | 0.10% | 0.00% | 0.77% | 0.40% | 0.00% | NA | NA | 0.15% |
| non-ICP | 0.40% | 0.70% | NA | 0.30% | 0.30% | 0.50% | 0.00% | 3.60% | NA | 0.30% | NA | NA | 0.00% | 0.30% | 0.00% | 0.71% | 0.70% | 0.00% | NA | NA | 0.44% | |
| Small for gestational age | ICP | 7.70% | NA | NA | 1.10% | NA | NA | NA | NA | 11.50% | 2.19% | NA | NA | 5.70% | 3.50% | NA | 4.25% | NA | NA | NA | NA | NA |
| non-ICP | 8.50% | NA | NA | 2.30% | NA | NA | NA | NA | 9.70% | 1.45% | NA | NA | 3.20% | 2.00% | NA | 4.71% | NA | NA | NA | NA | NA |
Note: UK, United Kingdom; USA, United States of America; PC, prospective cohort study; RC, retrospective cohort study; RCC, retrospective case-control study; PCC, prospective case-control study; CSC, cross-sectional case-control; ICP, intrahepatic cholestasis of pregnancy; non-ICP, non-intrahepatic cholestasis of pregnancy; NA, not available; C-Section, cesarean section; SGA, small for gestational age; GDM, gestational diabetes mellitus; NICU, neonatal intensive care unit.
We performed a meta-analysis on 7 different maternal outcomes based on the collected literature. After assessing heterogeneity, we used a fixed-effects model for postpartum hemorrhage and random-effects models for the other outcomes. Our results demonstrate that the incidence of ICP is 3% (95% CI: 1%–7%) (Fig. 2). ICP is significantly associated with increased risks of preeclampsia (relative risk [RR], 2.39; 95% CI, 2.21–2.59), C-section (RR, 1.28; 95% CI, 1.15–1.42), preterm delivery (RR, 2.71; 95% CI, 1.77–4.15), and maternal infection (RR, 3.22; 95% CI, 2.48–4.19), while showing a protective association with postpartum hemorrhage (RR, 0.82; 95% CI, 0.69–0.99), and no significant associations with labor induction (RR, 1.60; 95% CI, 0.51–4.99), or GDM (RR, 1.29; 95% CI, 0.83–2.01) (Fig. 3). These findings suggest a strong association between the occurrence of ICP and an increased risk of preeclampsia, C-section, preterm delivery, and maternal infection.
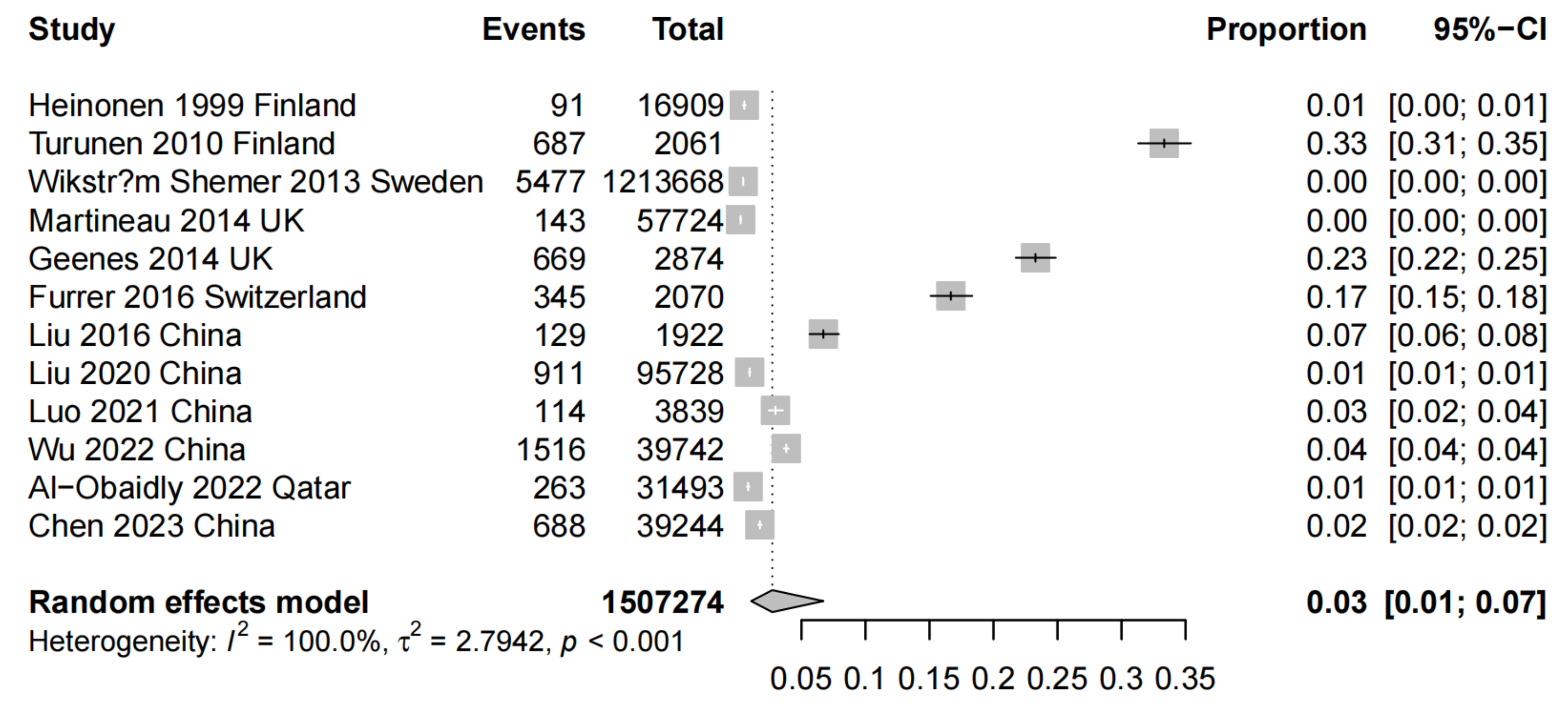 Fig. 2.
Fig. 2.
Forest plot of the prevalence of ICP. CI, confidence interval.
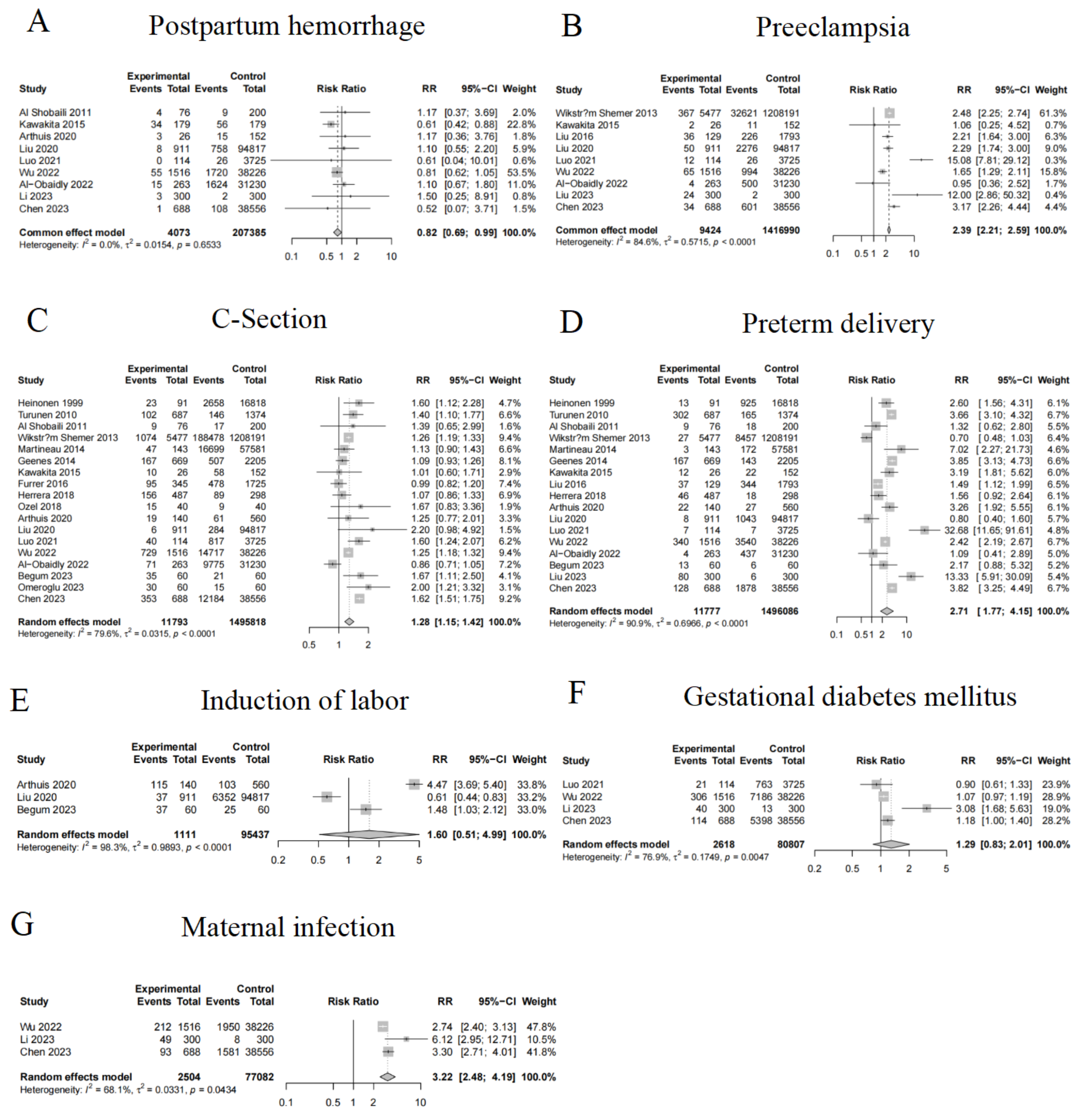 Fig. 3.
Fig. 3.
Forest plot of the meta-analysis comparing the ICP group and the
non-ICP group on adverse maternal outcomes. (A) displays the RR for “ICP and
Postpartum hemorrhage”. (B) shows the RR for “ICP and Preeclampsia”. (C)
illustrates the RR for “ICP and C-Section”. (D) presents the RR for “ICP and
Preterm delivery”. (E) displays the RR for “ICP and Induction of labor”. (F) shows
the RR for “ICP and Gestational diabetes mellitus”. (G) displays the RR for “ICP
and Maternal infection”. Note: 95% CI represents the 95% confidence interval. Based on the
heterogeneity results, a random effects model should be chosen if p
The sensitivity analysis results showed no significant changes, indicating that the meta-analysis results are robust and reliable (Fig. 4). The bias assessment results revealed that the funnel plots for all outcomes were generally symmetric, resembling an inverted funnel, and the p-values from bias detection tests were all greater than 0.05. This suggests that there is no strong evidence of publication bias, indicating a low likelihood of such bias and thereby enhancing the credibility and reliability of our conclusions (Fig. 5).
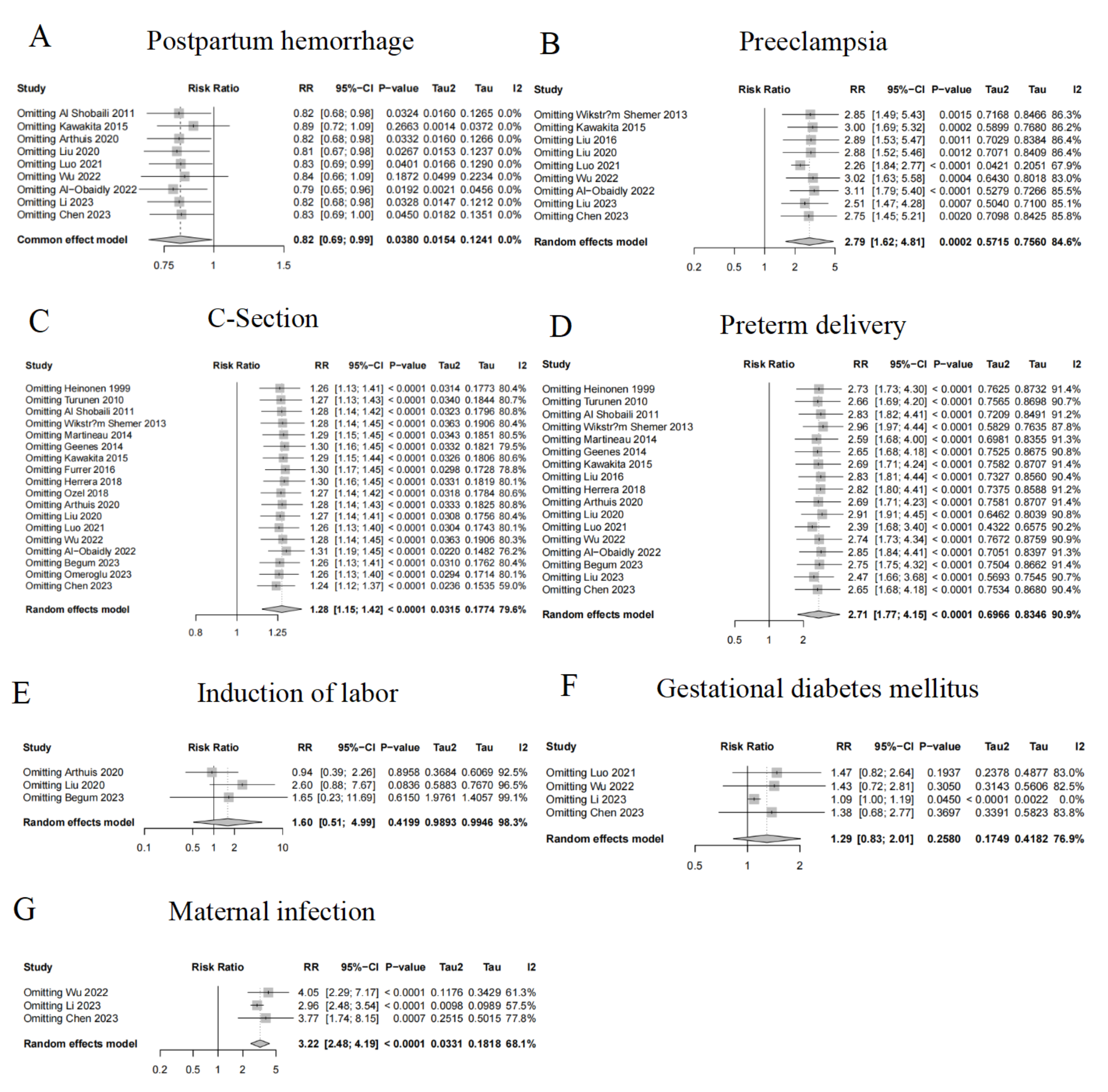 Fig. 4.
Fig. 4.
Sensitivity analysis of the ICP group vs. the non-ICP group on adverse maternal outcomes. (A) Sensitivity analysis of the ICP group vs. the non-ICP group on postpartum hemorrhage outcomes. (B) Sensitivity analysis of the ICP group vs. the non-ICP group on preeclampsia outcomes. (C) Sensitivity analysis of the ICP group vs. the non-ICP group on C-section outcomes. (D) Sensitivity analysis of the ICP group vs. the non-ICP group on preterm delivery outcomes. (E) Sensitivity analysis of the ICP group vs. the non-ICP group on Induction of labor outcomes. (F) Sensitivity analysis of the ICP group vs. the non-ICP group on gestational diabetes mellitus outcomes. (G) Sensitivity analysis of the ICP group vs. the non-ICP group on Maternal infection outcomes.
 Fig. 5.
Fig. 5.
Publication bias analysis of the ICP group vs. the non-ICP group on adverse maternal outcomes. (A) Funnel plot depicting publication bias for postpartum hemorrhage with the associated test results. (B) Funnel plot depicting publication bias for preeclampsia with the associated test results. (C) Funnel plot depicting publication bias for C-section with the associated test results. (D) Funnel plot depicting publication bias for preterm delivery with the associated test results. (E) Funnel plot depicting publication bias for Induction of labor with the associated test results. (F) Funnel plot depicting publication bias for gestational diabetes mellitus with the associated test results. (G) Funnel plot depicting publication bias for maternal infection with the associated test results. Each dot represents an individual study. SE, standard error; df, degrees of freedom.
A meta-analysis was conducted on 3 different neonatal outcomes using the collected literature. Random-effects models were applied to all indicators based on heterogeneity assessment. Our results demonstrate that ICP significantly increases the risk of NICU admission by 1.79-fold (RR, 1.79; 95% CI, 1.35–2.37), but does not significantly increase the risks of stillbirth (RR, 1.25; 95% CI, 0.64–2.42) or SGA (RR, 1.06; 95% CI, 0.71–1.57) (Fig. 6). These findings indicated that ICP is closely associated with an increased risk of NICU admission.
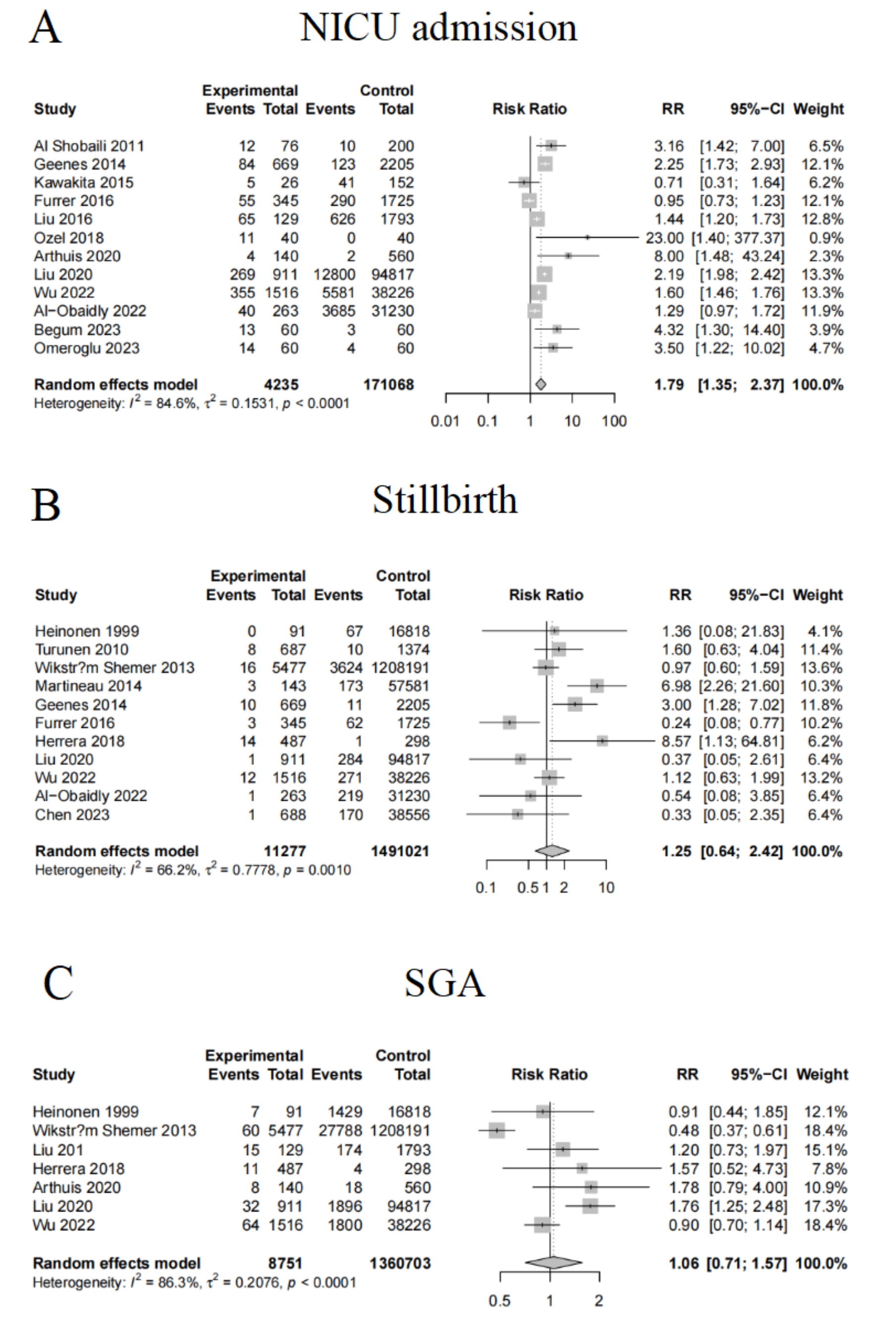 Fig. 6.
Fig. 6.
Forest plot of the meta-analysis on neonatal adverse outcomes in the ICP group and the non-ICP group. (A) displays the RR for “ICP and NICU admission”. (B) shows the RR for “ICP and Stillbirth”. (C) illustrates the RR for “ICP and SGA”. NICU, neonatal intensive care unit; SGA, small for gestational age.
The sensitivity analysis results showed no substantial changes across groups, indicating that the meta-analysis findings are robust and reliable (Fig. 7). The bias assessment results revealed that the funnel plots for all outcomes were generally symmetric, resembling an inverted funnel, and the p-values from bias detection tests were all greater than 0.05. This suggests no strong evidence of bias, implying a low likelihood of publication bias and further enhancing the credibility and reliability of the conclusion (Fig. 8).
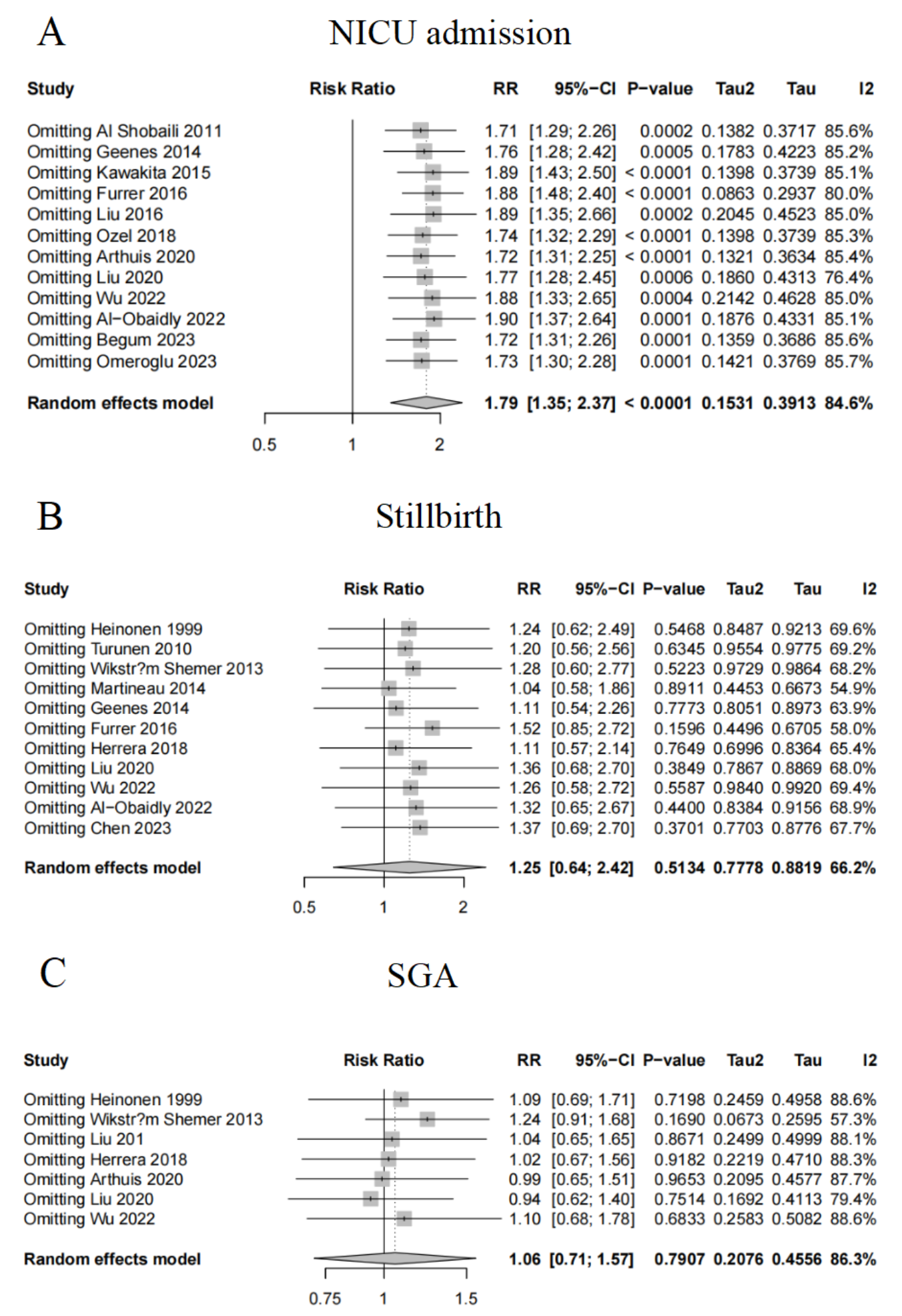 Fig. 7.
Fig. 7.
Sensitivity analysis of neonatal adverse outcomes in the ICP group and the non-ICP group. (A) Sensitivity analysis of the ICP group vs. the non-ICP group on NICU admission. (B) Sensitivity analysis of the ICP group vs. the non-ICP group on Stillbirth. (C) Sensitivity analysis of the ICP group vs. the non-ICP group on SGA outcomes.
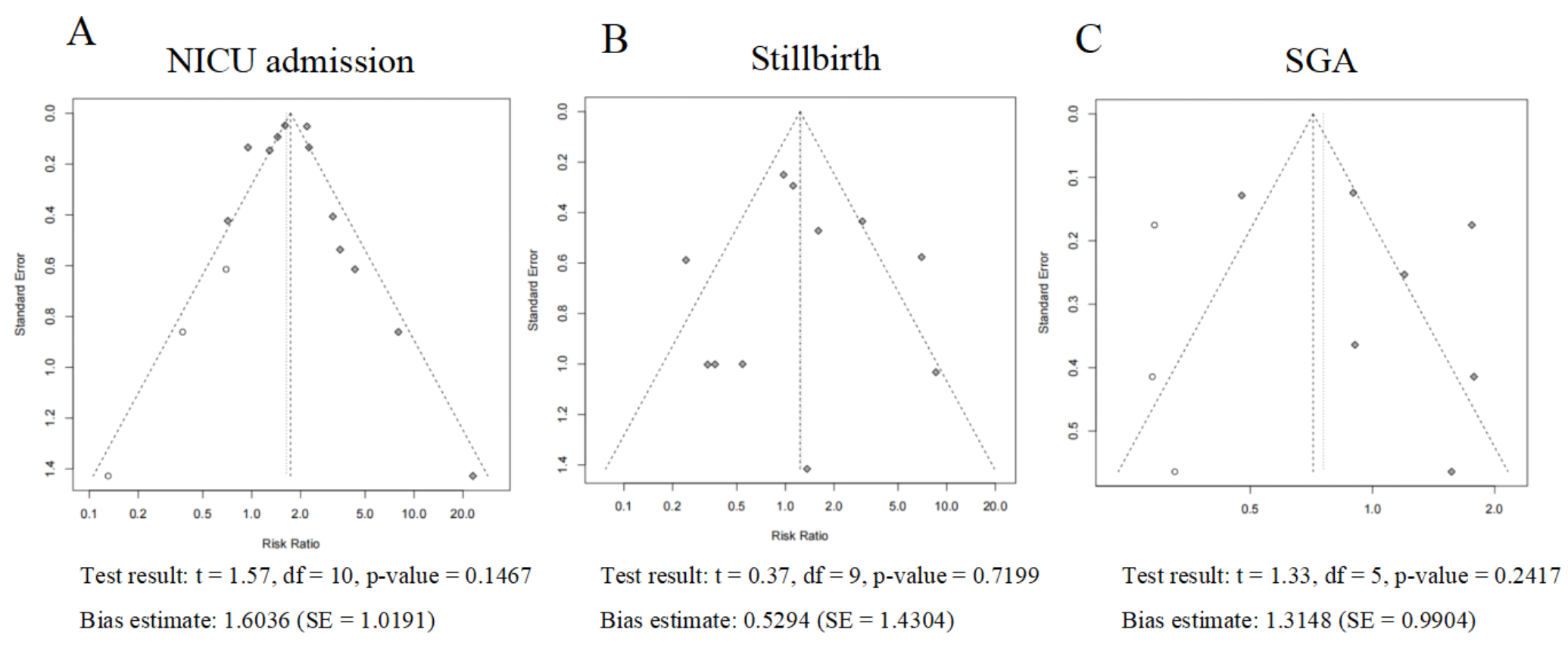 Fig. 8.
Fig. 8.
Publication bias analysis of neonatal adverse outcomes in the ICP group and the non-ICP group. (A) Funnel plot depicting publication bias for NICU admission with the associated test results. (B) Funnel plot depicting publication bias for Stillbirth with the associated test results. (C) Funnel plot depicting publication bias for SGA with the associated test results. Each dot represents an individual study.
Given the limited research on the quantitative analysis of the impact of ICP on maternal and neonatal adverse outcomes, as well as the insufficient exploration of its epidemiological features and pathological mechanisms, we conducted a systematic review and meta-analysis to comprehensively assess the effect of ICP on maternal and neonatal adverse outcomes. The following section further examines these findings, analyzing the potential impact of ICP on maternal health in the context of existing literature. It also explores directions for future research and implications for clinical management strategies.
This meta-analysis reveals significant geographical heterogeneity in the
incidence of ICP (I2 = 100%), with Finnish cohorts reporting rates as high
as 33%, whereas most Asian studies report rates below 5% [32, 33]. This suggests that
variations in diagnostic criteria and genetic predispositions may play a dominant
role in influencing the incidence risk. Although the random-effects model
estimates a pooled incidence of 3% (95% CI: 1%–7%), the extreme
heterogeneity (
Furthermore, we observed that ICP increased the risk of C-section, with a risk ratio of 1.28 (95% CI, 1.15–1.42). This aligns with other studies, highlighting a close relationship between ICP and C-section. Possible mechanisms include fetal intrauterine stress responses, particularly the occurrence of fetal distress. This often leads to an emergency C-section to protect both maternal and fetal lives [5, 25, 35]. ICP patients may also suffer from placental insufficiency, which affects fetal oxygen supply and growth. This contributes to the increased need for C-section [25]. Additionally, ICP patients frequently experience severe pruritus and elevated bile acid levels. These factors can affect maternal physical health and increase psychological stress. This may influence the choice of delivery method and clinical decision-making, further raising the risk of C-section [28].
As found in our study, ICP significantly increased the risk of preterm delivery. Preterm delivery is a common complication of pregnancy that directly impacts maternal and neonatal health, particularly concerning fetal growth and development. Elevated bile acid levels can affect fetal development through the placenta, potentially disrupting the intrauterine environment and promoting the onset of preterm delivery [35]. Bile acids can affect fetal oxygen and nutrient supply through the placenta and may also activate maternal immune responses, leading to complications like uterine contractions and premature rupture of fetal membranes. Preterm delivery is commonly correlated with higher neonatal mortality and birth defects. This finding highlights the need for early screening and intervention in ICP patients to prevent preterm delivery.
The risk of maternal infections in ICP patients is increased. This aligns with existing literature, indicating that elevated bile acid levels, liver dysfunction, and immune system dysregulation are likely mechanisms behind the increased risk of infection in ICP patients. These patients often exhibit abnormal immune function, making them more susceptible to infections. During labor, factors like surgical trauma or birth canal infections further elevate the risk of infections [36]. Therefore, ICP patients need treatment for heightened bile acid levels and liver dysfunction, along with special attention to prevent pregnancy-related infections, especially during labor.
Although this study primarily focused on maternal adverse outcomes, we also analyzed the potential impact of ICP on neonatal outcomes. As evidenced by the results, ICP is closely associated with an increased risk of neonatal admission to NICU. Indeed, the risk of neonatal NICU admission in the ICP group was 1.79 (95% CI, 1.35–2.37), highlighting the significant impact of ICP on neonatal health. Elevated bile acid levels not only impair maternal liver function but also cross the placenta, affecting fetal development and health. This can lead to fetal distress, increasing the likelihood of NICU admission. The heightened risk of intrauterine stress responses in the fetus may expose the fetus to more acute complications, raising the demand for NICU care [37].
The quantitative evidence from this study provides crucial decision-making support for the clinical management of ICP. Given the global incidence of 3% (95% CI: 1%–7%), it is recommended that systematic liver function screening begin at 24 weeks of gestation in high-risk regions, such as Asia, along with dynamic monitoring of pruritus symptoms for early diagnosis. In response to the significantly increased risks of preeclampsia (RR = 2.39), maternal infection (RR = 3.22), and preterm delivery (RR = 2.71), clinicians should establish a multidimensional monitoring system. For diagnosed patients, weekly monitoring of fetal heart rate and biophysical scoring should begin at 32 weeks of gestation, with the planned delivery time advanced to 37–38 weeks. During labor, routine dynamic monitoring of C-reactive protein and procalcitonin should be implemented, and an infection warning scoring system should be initiated within 48 hours postpartum. Notably, although the risk of C-section is increased (RR = 1.28), the risk of postpartum hemorrhage shows a paradoxical reduction (RR = 0.82), suggesting that regional guidelines should balance the use of uterotonic agents and thrombosis prevention strategies. For example, in Asian populations, the indications for uterotonic agents may be moderately relaxed, whereas European populations should maintain current standards. Additionally, the increased demand for neonatal intensive care (RR = 1.79) calls for collaborative perioperative transition plans between obstetric and pediatric teams. Future research should focus on elucidating the dose-response relationship between bile acid levels and complications, as well as conducting multicenter intervention trials to validate the generalizability of stratified management pathways, ultimately achieving comprehensive optimization from risk warning to precise intervention.
The main strength of this study lies in its systematic design and rigorous implementation, particularly in the application of various statistical tools during the literature search and data analysis. These included the use of fixed-effects and random-effects models, as well as sensitivity analysis and funnel plots to validate the stability of the results. These methods enhanced the credibility and reliability of the conclusions. By comprehensively analyzing multiple obstetric outcomes, this study provided detailed reference data for clinicians. It helps identify high-risk individuals among ICP patients and provides theoretical support for personalized management and early intervention. Our meta-analysis integrated a large amount of data and helped strengthen the scientific understanding of the association between ICP and maternal health risks. It also supports better clinical decision-making. While this systematic review and meta-analysis provide robust evidence through rigorous methodology, several limitations warrant consideration. First, the generalizability of findings is constrained by the geographical and ethnic composition of included studies. Over 80% of primary data originated from European and North American populations, potentially underrepresenting developing regions where ICP prevalence and risk profiles may differ substantially. Second, critical clinical variables such as maternal comorbidities, particularly pregestational diabetes, socioeconomic status, and longitudinal bile acid monitoring data were inconsistently reported across studies, limiting our ability to conduct stratified analyses. Third, despite employing random-effects models and sensitivity analyses to address heterogeneity, residual confounding may persist due to unmeasured factors like genetic predisposition and regional variations in obstetric care protocols. Additionally, while funnel plots showed no significant publication bias for maternal outcomes, the exclusion of gray literature and non-English studies might have skewed neonatal outcome estimates. Future research should prioritize prospective registries with standardized ICP diagnostic criteria and improved reporting of ethnodemographic confounders.
In summary, this study offers valuable evidence on the correlation between ICP and adverse outcomes in pregnant and postpartum women, as well as neonates. However, these results still need to be validated through broader, more methodologically rigorous future research. As our understanding of ICP deepens, future studies should not only focus on assessing the risk of obstetric complications but also explore its underlying pathophysiological mechanisms and biomarkers. This will help provide a solid theoretical foundation for the early diagnosis and personalized treatment of ICP.
This study, through systematic evaluation and meta-analysis, suggests a strong association between ICP and adverse outcomes in pregnant and postpartum women, such as preeclampsia, C-section, preterm delivery, GDM, and maternal infections. It provides valuable scientific evidence to inform clinical management. However, the heterogeneity observed in certain outcomes, the potential influence of confounding variables, and statistical limitations in the analysis of neonatal outcomes indicate that further validation is needed. Future research should focus on higher-quality, larger-scale prospective studies to further examine the mechanisms by which ICP impacts maternal and fetal health, thereby offering more precise guidance for clinical diagnosis and treatment.
The data and materials used in this meta-analysis are publicly available. The individual study data were retrieved from the PubMed, Embase, and Cochrane Library databases. The search strategies and inclusion/exclusion criteria are described in the Materials and Methods section.
PY and MZ conceived the study. PY, MZ, and CH developed the study protocol and data analysis plan. MZ and CH conducted the study quality assessment. PY, MZ, and CH performed the statistical analysis. PY, CH and MZ wrote the first draft of the manuscript. All authors reviewed and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to acknowledge the excellent teamwork within our research group. The collaborative and positive atmosphere within the team has been a driving force for the successful completion of this meta-analysis.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG37850.
During the preparation of this systematic review and meta-analysis, we used ChatGPT, an artificial-intelligence-based tool, to check spelling and grammar during the initial drafting stage of the manuscript. After composing the text, ChatGPT scanned it to identify potential spelling errors and improper grammar usage. Nevertheless, this tool was just a part of the overall writing process. We thoroughly reviewed and edited the content as required after using ChatGPT and remains fully responsible for the final content of the publication, including data accuracy, analysis validity, and result interpretation, thus ensuring the academic integrity and scientific rigor of the work.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.