


 , Ye Xu 2, Ye Shen 2,*
, Ye Xu 2, Ye Shen 2,* , Wenjun Song 1
, Wenjun Song 11 Department of Obstetrics and Gynecology, Taihu Sanatorium of Jiangsu Province, 214086 Wuxi, Jiangsu, China
2 Department of Obstetrics and Gynecology, Wuxi Maternal and Child Health Hospital, 214002 Wuxi, Jiangsu, China
Abstract
Uterine rupture (UR) is a rare but severe obstetric complication that significantly affects maternal and neonatal health. Despite extensive ongoing research on UR risk factors, controlling for confounding variables remains crucial to ensure accurate risk assessment and the development of effective preventive measures. Therefore, this study aimed to explore the potential risk factors for UR during pregnancy to improve preventive measures and therapeutic strategies.
A retrospective analysis was conducted on medical records of pregnant women with UR from January 2019 to December 2023 across 11 hospitals in Jiangsu province, China. For comparison, a control group without UR (non-UR group) comprising twice the number of UR cases, was randomly selected from the pool of women with uncomplicated pregnancies during the same period. Subsequently, patients diagnosed with UR (UR group) were matched 1:1 with those without UR (non-UR group) based on age, body mass index, blood pressure, and adequacy of prenatal care. The association between group status and risk factors was examined using multivariable analysis.
Among 306,336 singleton pregnancies across 11 hospitals, 72 UR cases were identified, leading to a rupture rate of 2.4 per 10,000 deliveries. Following propensity score matching (PSM), 62 patients in the UR group were compared with 62 patients in the non-UR group. Univariate analyses revealed a significantly higher incidence of cesarean section and a history of uterine surgery history among UR patients compared to non-UR patients. Multivariable analysis identified multiple uterine surgeries as an independent risk factor for UR (odds ratio [OR]: 3.141; 95% confidence interval [CI]: 1.903–5.183; p < 0.001).
This study emphasizes the significance of multiple uterine surgeries as a potential independent risk factor for UR. Recognizing such risk factors is pivotal for refining perinatal management strategies aimed at reducing the incidence of UR. Ultimately, this reduction can significantly enhance maternal and neonatal health outcomes.
Keywords
- cesarean section
- gynecologic surgical procedures
- hysteroscopy
- pregnancy
- uterine rupture
Uterine rupture (UR) is a rare but severe complication of pregnancy, especially occurring in women with a history of cesarean sections or uterine surgeries [1, 2]. This condition often leads to critical outcomes for maternal and fetal outcomes [1, 2]. The incidence exhibits variability among different demographic cohorts, revealing a markedly increased prevalence among women who have experienced cesarean sections or alternative uterine surgical interventions. According to the World Health Organization (WHO), UR prevalence is reported as 0.053% in community-based studies, while a higher incidence of 0.31% is observed in medical institution-based studies [3]. The primary causes for UR consist of widespread poverty, illiteracy, cultural factors, advanced age, grand multiparity, unskilled delivery, and misuse of uterotonics, particularly in developing countries [4]. Despite significant economic progress, the prevalence of UR during pregnancy in China has not markedly improved over recent years [5].
Accurate UR diagnosis is complicated by symptom heterogeneity and the lack of established predictive criteria [6, 7]. Early and accurate risk assessment is crucial to prevent adverse maternal and neonatal outcomes [7, 8]. Considering these challenges, the incidence of UR and the outcomes for pregnant women and their unborn children vary, influenced by differences in socio-demographic conditions, preparedness, access to skilled midwives, and the efficiency of health systems across regions [9]. Particularly, the cesarean section rate in China has remained high over several decades, with reports indicating rates range from 40% to 60% in most Chinese hospitals. In some hospitals, this rate has exceeded 70% [10]. This cesarean delivery trend contributes to cesarean scar pregnancy (CSP), a unique variant of ectopic pregnancy, where fertilized eggs and trophoblastic cells implant onto the cesarean section scar [11]. It is widely believed that CSP significantly increases the risk of UR [12, 13]. Thus, previous cesarean delivery (CD) is one of the most vital independent risk factors for UR [12].
Despite early investigations into UR risk factors, many studies have yet to effectively control for confounding variables [5, 14, 15]. Furthermore, most current research has centered on evaluating risk factors for cesarean scar pregnancy and UR during a trial of labor. However, it remains ambiguous whether increased risk correlates with rising CD rates [13, 16]. Additionally, the 2019 American College of Obstetricians and Gynecologists (ACOG) guidelines, along with a Chinese expert consensus group, do not mention maternal age or parity effects on UR [17, 18]. Thus, the association between maternal age, parity, previous cesarean section count, and UR risk remains controversial [13, 16]. Ultimately, more studies are necessary to systematically explore risk factors associated with UR.
This study addresses gaps using a retrospective method and propensity score matching (PSM) to rigorously manage confounding factors [19]. The goal is to pinpoint crucial risk factors, thereby advancing risk assessment and informing clinical strategies to lessen UR incidence and improve maternal-neonatal outcomes.
We conducted a retrospective analysis of the medical records of pregnant women with UR at 11 hospitals in Jiangsu province, China, between January 2019 and December 2023. Diagnostic criteria included: (1) an anatomic separation of the uterine muscle (with or without symptoms); (2) a disruption or tear of the uterine muscle and the visceral peritoneum; or (3) a separation of the uterine muscle with extension to the bladder or the broad ligament [20]. The control participants without UR during pregnancy were selected randomly to minimize selection bias. Inclusion criteria were those who met the diagnostic criteria. Exclusion criteria included: (1) patients lacking complete medical records; or (2) cases of multiple gestations. This study was conducted in accordance with the Declaration of Helsinki. Given the retrospective nature of this study, informed consent was not required.
UR refers to rupture of the uterine body or the lower segment of the uterus during pregnancy or childbirth [21]. Based on severity, UR can be divided into complete UR and incomplete UR. Complete UR is characterized by a full-thickness laceration in the uterine wall, extending through all layers, including the serosa, myometrium, and endometrium [22]. Conversely, incomplete UR is characterized by a partial tear in the uterine wall that does not extend through all layers. Incomplete UR refers to a partial or complete rupture of the myometrium, with the serosal membrane layer remaining intact, and the uterine cavity not connecting to the abdominal cavity [23].
This study stratified pregnant women into two distinct cohorts: those with a history of uterine surgery and those without. A history of uterine surgery is defined by procedures resulting in uterine scarring, including cesarean section, myomectomy, uterine horn resection, and cervical cerclage [24, 25]. Previous uterine surgical history encompasses procedures that may compromise the integrity of the myometrium or endometrium, consequently affecting uterine elasticity and strength. Uterine surgery, beyond the aforementioned procedures, also includes curettage, induced abortion, hysteroscopic procedures, and endometrial ablation [26]. Normal prenatal care refers to receiving prenatal care according to the Pregnancy Health Record, with no more than three missed appointments in total and no consecutive missed appointments.
Patients were divided into four groups based on gestational age at UR: less than
26 weeks gestational age, 26–36 weeks gestational age, 37–38 weeks gestational
age, and more than 38 weeks. Other variables included the number of prior
pregnancies, number of prior births, years from uterine surgeries to conception,
and age (non-advanced age group:
With respect to maternal and neonatal outcomes, the classification for fetal
delivery was either vaginal delivery or cesarean section delivery. Other
variables included fetal weight, Apgar score (Apgar score
The data were analyzed utilizing SPSS statistical software (version SPSS 22.0,
IBM Corporation, Armonk, NY, USA). Categorical data are presented as percentages.
Continuous data that conformed to the normal distribution were expressed as
mean
Across 11 hospitals in Jiangsu Province, China, 72 instances of UR were
recorded, between January 2019 and December 2023 among 306,336 pregnant women
with a singleton pregnancy, corresponding to a rupture rate of 2.4 per 10,000
deliveries. For comparative analysis, 144 healthy pregnant women were randomly
selected from a larger cohort of pregnancies during the same period, constituting
the non-UR group. Following the application of PSM based on variables such as
age, BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), and the
adequacy of prenatal care, we conducted a comparative analysis between 62
patients in the UR group and 62 patients in the non-UR group. Fig. 1 illustrates
the flowchart of patient data included in this study. Three patients in the UR
group were hospitalized due to abdominal pain accompanied by vaginal bleeding at
8–17 weeks of gestation. Three patients in the UR group were hospitalized due to
abdominal pain accompanied by vaginal bleeding at 8–17 weeks of gestation. Upon
confirmation of the UR diagnosis through palpation and ultrasound examination,
the patients underwent pregnancy termination and scar excision. The remaining 59
cases were delivered beyond 33 weeks of gestation. The median age was 31.74
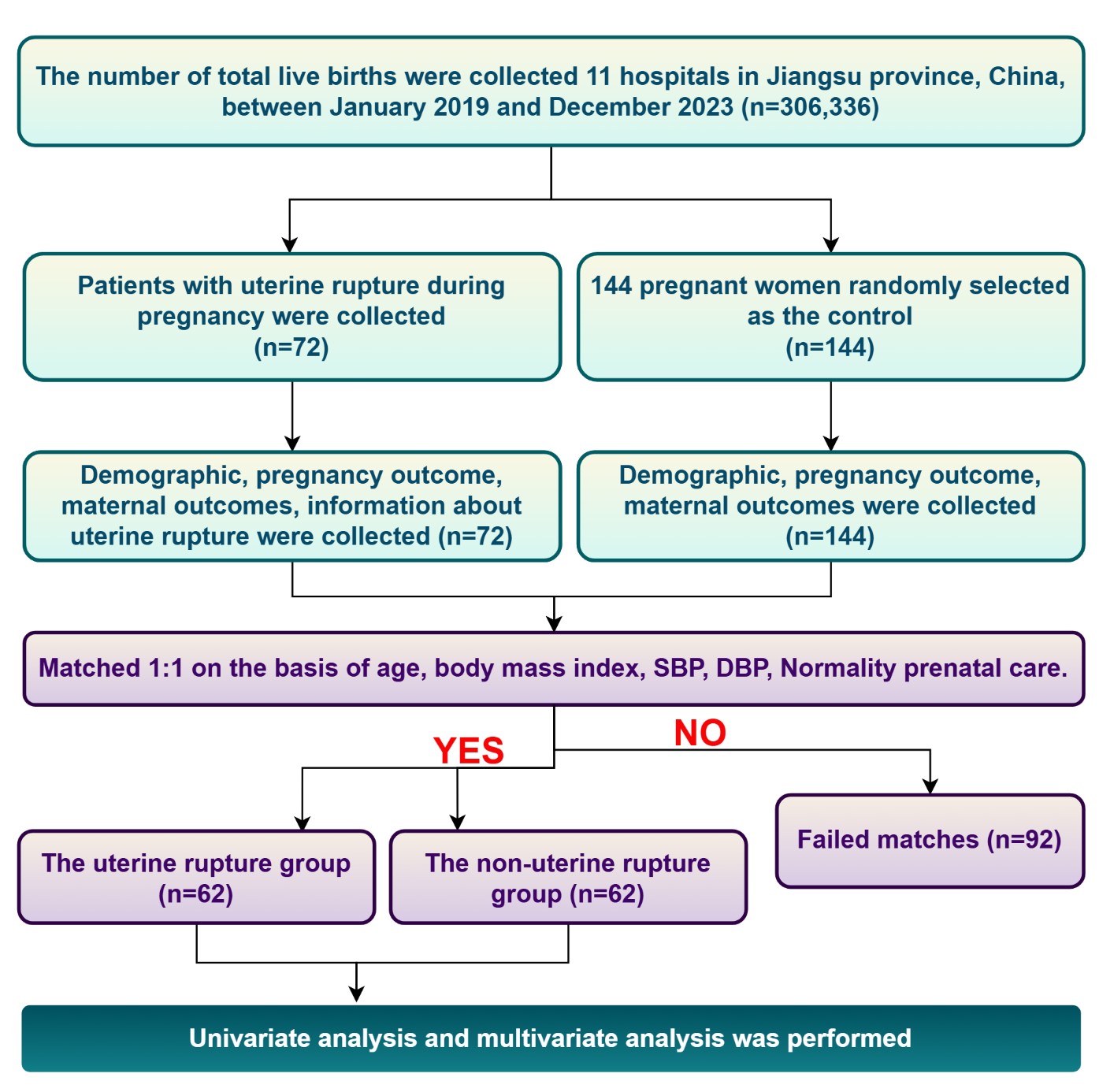 Fig. 1.
Fig. 1.
Flowchart of patient identification and uterine rupture diagnosis. SBP, systolic blood pressure; DBP, diastolic blood pressure.
| Characteristic | UR group (n = 62) | Non-UR (n = 62) | p-value |
| Age (years) | 31.74 |
31.94 |
0.826 |
| Body mass index (kg/m2) | 27.48 |
27.65 |
0.780 |
| SBP (mmHg) | 121.44 |
120.98 |
0.864 |
| DBP (mmHg) | 77.95 |
77.50 |
0.829 |
| Normality prenatal care | 54 (87.10%) | 55 (88.71%) | 0.783* |
Notes: UR, uterine rupture; SBP, systolic blood pressure; DBP, diastolic blood pressure. Normality prenatal care refers to receiving prenatal care according to the Pregnancy Health Record, with a total of no more than three missed appointments and no consecutive missed appointments; * using Pearson’s chi-square test.
Table 2 demonstrates the univariate and multivariate analyses of risk factors
associated with UR. The univariate analysis revealed no significant differences
in the number of prior pregnancies (3.66
| Characteristic | Univariate analysis | Multivariate analysis | |||
| UR group (n = 62) | Non-UR group (n = 62) | p-value | OR (95% CI) | p-value | |
| Number of prior pregnancies | 3.66 |
3.37 |
0.305 | - | - |
| Number of prior given birth | 1.18 |
1.19 |
0.909 | - | - |
| History of cesarean section | 48 (77.4%) | 36 (58.1%) | 0.021* | 0.380 (0.153–0.943) | 0.370 |
| Number of uterine surgeries | 2.87 |
1.53 |
3.141 (1.903–5.183) | ||
Notes: UR, uterine rupture; OR, odds ratio; 95% CI, 95% confidence interval; * using Pearson’s chi-square test. Uterine surgery refers to any surgical procedure performed on the uterus, including cesarean section, myomectomy, uterine horn resection, cervical cerclage, curettage, induced abortion, hysteroscopy, and endometrial ablation.
Additional analysis focused on pregnant women with no prior cesarean sections,
as shown in Fig. 2. The data revealed no statistically significant differences in
the number of pregnancies or births between the UR and non-UR groups (p
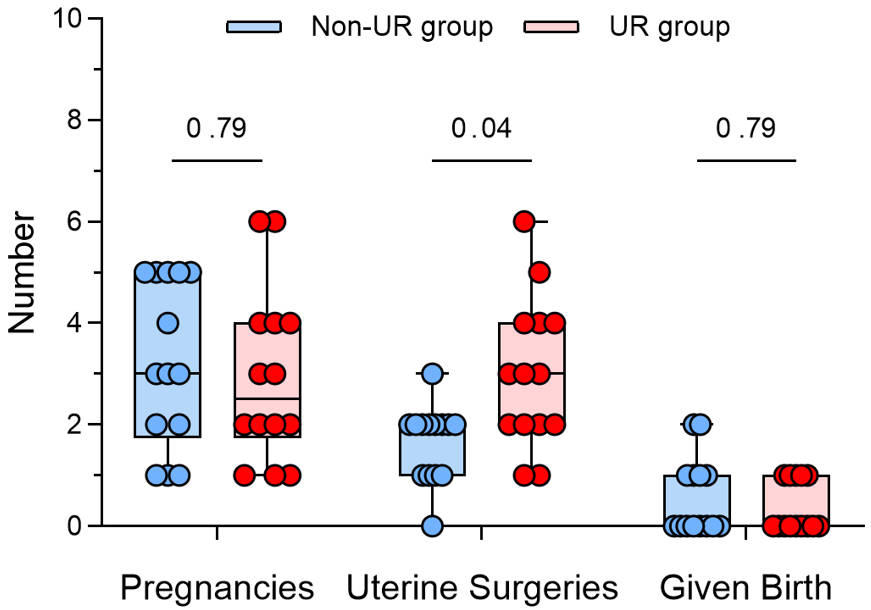 Fig. 2.
Fig. 2.
Analysis of risk factors for UR in pregnant women with no prior cesarean sections. UR, uterine rupture.
Analysis of fetal outcomes revealed no statistically significant differences in Apgar scores, birth weight, or miscarriage rates between the UR and non-UR groups, with p-values of 0.058, 0.867, and 0.619. Within the UR group, three pregnant women experienced abdominal pain and vaginal bleeding prior to labor, were diagnosed with UR via ultrasound, and subsequently terminated their pregnancies following medical advice. However, the estimated blood loss significantly differed between the UR and non-UR groups (p = 0.041). The incidence of vaginal delivery was significantly lower in the UR group at 6.45%, compared to 27.42% in the non-UR group (p = 0.003). The risk of UR in women with a history of cesarean sections often discourages clinicians from recommending vaginal birth after cesarean section [29]. According to the Expert Consensus on Cesarean Section by the Chinese Medical Society of Obstetrics and Gynecology, CD is recommended for pregnant women with previous cesarean section or an estimated fetal birth weight exceeding 4250 g [10]. This clinical directive significantly influenced patient management, resulting in only four parturients among 62 patients in the UR group undergoing vaginal delivery. Notably, all four cases of UR occurred during labor and were identified postpartum. Detailed information is presented in Table 3.
| Characteristic | UR group (n = 62) | Non-UR (n = 62) | p-value | |
| Fetal outcomes | ||||
| Apgar score† | 8.76 |
9.52 |
0.058# | |
| Birthweight† | 3078.87 |
3054.76 |
0.867# | |
| Miscarriage | 3 (4.84%) | 1 (1.61%) | 0.619 | |
| Maternal outcomes | ||||
| Vaginal delivery | 4 (6.45%) | 17 (27.42%) | 0.003 | |
| Cesarean section | 58 (93.55%) | 45 (72.58%) | ||
| Estimated blood loss (median [IQR]), mL | 300 [237.5, 350.0]† | 300 [250.0, 700.0] | 0.041## | |
Note: UR, uterine rupture; IQR, interquartile ranges. † four miscarriage cases were excluded. # Independent samples t-test, ## Mann-Whitney U test, other p-values are based on Fisher’s exact test.
Sixty-two cases of UR were divided into two groups—the incomplete rupture group (n = 45) and the complete rupture group (n = 17)—for comparative analysis to investigate factors influencing maternal outcomes. Statistical analysis revealed no significant differences in age distribution (p = 1.000) between the groups, nor were there any significant differences in the number of prior pregnancies (p = 0.058) or deliveries (p = 0.549). The interval from uterine surgery to conception was not significantly different between the two groups (p = 0.743), and the proportion of patients with a history of cesarean section was also not significantly different (p = 0.178), suggesting that prior cesarean surgery might not be significantly related to the integrity of UR. Nonetheless, the distribution of gestational weeks was statistically significant between the groups (p = 0.024), with a notably higher proportion of complete UR occurring between 26 and 36 weeks gestation in the complete rupture group compared to the incomplete rupture group (41.18% vs. 13.33%, respectively), indicating a potentially increased risk of complete UR during this period. Furthermore, although the difference in the number of uterine surgeries approached statistical significance (p = 0.079), this observation requires further validation in studies with larger sample sizes. Detailed information is provided in Table 4.
| Characteristic | Classification of UR | Neonatal outcome | |||||
| Incomplete UR group (n = 45) | Complete UR (n = 17) | p-value | Unfavorable neonatal outcomes (n = 8) | Favorable neonatal outcomes (n = 54) | p-value | ||
| Age | 1.000 | 1.000 | |||||
| Advanced maternal age | 12 (26.67%) | 5 (29.41%) | 2 (25.00%) | 15 (27.78%) | |||
| Non-advanced maternal age | 33 (73.33%) | 12 (70.59%) | 6 (75.00%) | 39 (72.22%) | |||
| Number of prior pregnancies | 3.44 |
4.24 |
0.058# | 4.25 |
3.57 |
0.228# | |
| Number of previously given birth | 1.11 |
1.24 |
0.549# | 1.25 |
1.13 |
0.783# | |
| History of cesarean section | 0.178 | 0.365 | |||||
| Yes | 37 (82.22%) | 11 (64.71%) | 5 (62.50%) | 43 (79.63%) | |||
| No | 8 (17.78%) | 6 (35.29%) | 3 (37.50%) | 11 (20.37%) | |||
| Number of uterine surgeries | 2.64 |
3.47 |
0.079# | 3.38 |
2.80 |
0.360# | |
| Gestational age at UR | 0.024 | 0.002 | |||||
| 1 (2.22%) | 2 (11.76%) | 3 (37.50%) | 0 (0.00%) | ||||
| 26–36 weeks | 6 (13.33%) | 7 (41.18%) | 1 (12.50%) | 12 (22.22%) | |||
| 37–38 weeks | 19 (42.22%) | 3 (17.65%) | 1 (12.50%) | 21 (38.89%) | |||
| 19 (42.22%) | 5 (29.41%) | 3 (37.50%) | 21 (38.89%) | ||||
| Duration in years from uterine surgeries to conception | 5.80 |
5.41 |
0.743# | 4.75 |
5.83 |
0.491# | |
Note: UR, uterine rupture; Apgar score
Regarding neonatal outcomes, an analysis of the Apgar scores for neonates
post-UR was conducted to investigate the potential determinants of neonatal
outcomes. Participants were divided into two groups: the group with unfavorable
neonatal outcomes (Apgar score
These findings indicate that these maternal characteristics are unlikely to be determining factors for neonatal Apgar scores. Future studies should explore additional potential factors for a more comprehensive understanding of UR’s complexities and its implications on maternal and neonatal health. Detailed information is provided in Table 4.
UR is a rare yet severe obstetric complication during pregnancy, frequently leading to significant health risks for mothers and neonates [30]. Although medical research has identified certain risk factors for UR, many studies have not controlled for potential confounding variables [5, 14, 15]. This study utilized PSM to systematically evaluate the risk factors associated with UR, focusing on the correlation between multiple uterine surgeries and the risk of UR. This study aimed to develop more precise perinatal management strategies to reduce the incidence of UR.
This study demonstrated that the UR rate was 0.024% (72/306,336), lower than previously documented rates (range, 0.13%–0.31%) [3, 5]. We speculate that this discrepancy could be due to differences across distinct geographical regions or normative prenatal examinations. The prevalence of UR during pregnancy continues to increase in China, consistent with the finding reported by Zhou et al. [5]. This study observed UR rates from 2019 to 2023 recorded at 0.0092% (2019), 0.0087% (2020), 0.0349% (2021), 0.0332% (2022), and 0.0368% (2023), respectively.
After PSM matching, this study identified that pregnant women with a history of cesarean section exhibited a significantly increased risk of UR compared to those without such a history. However, multivariate analysis indicated no statistically significant difference between the UR and non-UR groups in cesarean section history. This finding may be due to the inclusion of cesarean section counts in the number of uterine surgeries, which was controlled for in the multivariable model, potentially suggesting that a history of cesarean section could serve as a protective factor. This correlation is particularly relevant, as CSP rates will continue to increase with the rising incidence of cesarean sections [31]. Furthermore, a previous study has demonstrated that women with a previous cesarean section who undergo labor induction with uterotonic drugs are at an elevated risk of UR and subsequent complications [32]. Our study corroborates these findings, revealing that a history of cesarean section significantly increases the risk of UR and estimated blood loss during delivery. Specifically, we found that a history of cesarean section significantly increased the risk of UR and estimated blood loss during delivery. However, CSP presents with nonspecific clinical symptoms in early pregnancy or only resembles signs of threatened miscarriage, such as slight vaginal bleeding and mild lower abdominal pain [33]. Critically, the diagnosis of CSP relies on identifying the gestational sac within the uterine scar, as detected by ultrasound or magnetic resonance imaging (MRI) [34]. Nonetheless, owing to the relatively low sensitivity of imaging examinations, many CSP patients may be misdiagnosed. Consequently, such misdiagnosis may result in dilation and curettage procedures for suspected pregnancy failure, leading to severe complications [33].
This study revealed that the incidence of uterine surgeries was significantly
higher in the UR group (2.87
Indeed, the extent of uterine surgery and the surgical modality utilized can affect our findings. However, it is undeniable that less-invasive procedures would likely decrease this risk. Hurst et al. [36] suggested that the existence of any difference, such as surgical technique, instruments, energy devices, or laparotomy, might result in myometrium wound healing difficulties. These include myometrial defects not being fully sutured, hematoma formation, and excessive unipolar or bipolar electrocautery severing blood vessels within the myometrium. These factors are thought to interfere with the healing of myometrial wounds and increase the risk of rupture. Prior studies have been inconsistent, with one finding no relation [37] and several others showing that the hysterectomy rate after UR is associated with scar pregnancy [38, 39, 40]. Researchers have speculated that treatment tends to be delayed because of a low suspicion index in patients without a history of uterine surgery [22]. In addition, unscarred UR most often occurs in the uterine body and outside the uterus. Therefore, surgical repair is a far more significant challenge than scarred UR. It is probably one of the reasons leading to the increase in severe maternal outcomes [37, 38]. Therefore, not following an antenatal care plan may increase hysterectomy rates. Colmorn et al. [41] expressed a similar view that certain hysterectomies can be avoided if UR is adequately repaired early.
In this study, a statistically significant difference was observed between the complete and incomplete UR groups in the distribution of gestational age (p = 0.024). Notably, between 26 and 36 weeks, the incidence of complete UR was markedly higher in the complete rupture group than in the incomplete rupture group (41.18% vs. 13.33%, respectively). This finding indicates a potentially substantial increase in the risk of complete UR during the gestational period. The elevated risk during this gestational period could be attributed to multiple factors. During this phase, uterine growth and fetal development reach a critical peak, and the tension in the uterine wall is markedly heightened, potentially elevating the risk of UR [7]. Moreover, the increase in fetal weight and amniotic fluid volume could impose additional stress on the uterine wall, which may explain the higher prevalence of complete UR observed at this stage of gestation [32, 42]. Therefore, clinicians should conduct more rigorous surveillance and management of these high-risk pregnancies during the 26–36-week gestational period to promptly detect and address potential UR risks.
Our study is subject to several limitations. Firstly, the data were obtained from a relatively small patient sample, and we lacked comprehensive pregnant women’s information regarding the location, quantity, onset, symptoms, and outcomes of the ruptures. These diverse rupture characteristics could substantially impact both fetal and maternal outcomes. Secondly, we could not collect sufficient data on the extent of uterine surgery and the surgical modalities employed in patients with a history of uterine surgery. Thirdly, the study was conducted in a region characterized by advanced economic development in China, with participating hospitals of higher rank (comprising seven third-level hospitals and four second-level hospitals), which may have influenced the study outcomes. Fourthly, although PSM effectively reduced certain biases, several unaddressed confounding factors, such as the socioeconomic status of pregnant women, access to prenatal care, and the experience and qualifications of the surgical team, may affect the incidence of UR. Fifthly, concerning neonatal outcomes, our data collection remains incomplete, with specific complications arising from UR necessitating further data collection and statistical analysis to achieve a comprehensive assessment. Therefore, the UR rates in this study should be analyzed cautiously.
In future research endeavors, we aim to broaden the scope of our study by incorporating additional regions, larger datasets, and comprehensive data collection methodologies. We will employ advanced statistical techniques to account for confounding variables. Our analysis will include detailed information on variables such as location, frequency, onset characteristics, symptoms, rupture outcomes, administration of uterotonics, presence of fetal macrosomia, and types of uterine surgeries. Special emphasis will be placed on examining the impact of the type and frequency of uterine surgeries on the risk of UR.
The study found that multiple uterine surgeries significantly increased the risk of UR during pregnancy, highlighting the need for a thorough obstetric history. It emphasizes the importance of targeted perinatal management, especially in areas with increasing cesarean rates. Health authorities should work to prevent UR by ensuring proper use of partographs and avoiding unnecessary cesareans.
The data used or analyzed during the current study are available from the corresponding author upon reasonable request.
XX, YX, and WS were involved in protocol development, data analysis, and manuscript writing. XX and WS were involved in data management and analysis. XX, YX, YS, and WS were involved in protocol development and responsible for reviewing the data. XX and YX were involved in project development, data collection, and manuscript editing. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All procedures followed the ethical standards of the responsible committee on human experimentation (institutional and national) and the 1975 Helsinki Declaration (in its most recently amended version). The study was approved by the Ethical Committee of the Wuxi Maternity and Child Health Hospital (reference number: 2020-01-07-0731-23). As this was a retrospective study, the requirement for informed consent was waived by the ethics committee.
We thank the ultrasonologist Jinxiao Sun in the ultrasound department, Taihu Sanatorium of Jiangsu Province, for reviewing the uterine ultrasound images.
This study was supported by a grant from the Jiangsu Provincial Key Discipline of Maternal and Child Health (No. SFY3-JS2021), and Scientific Research Project of the Health and Family Planning Commission of Wuxi City (No. M202057), Scientific Research Project of Wuxi Health and Family Planning Commission (No. FYKY202303).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.