

 , Süreyya Sarıdaş Demir 2,*
, Süreyya Sarıdaş Demir 2,* , Lokman Semih Demirkaya 3, Serem Kel Ilgin 4, İbrahim Eren Pek 1, Bülent Demir 1
, Lokman Semih Demirkaya 3, Serem Kel Ilgin 4, İbrahim Eren Pek 1, Bülent Demir 11 Department of Obstetrics and Gynecology, Medical Faculty of Canakkale Onsekiz Mart University, 17020 Canakkale, Turkey
2 Division of Perinatology, Department of Obstetrics and Gynecology, Mehmet Akif Ersoy Hospital, 17020 Canakkale, Turkey
3 Department of Obstetrics and Gynecology, Hassa State Hospital, 31000 Hatay, Turkey
4 Department of Obstetrics and Gynecology, Akcakale State Hospital, 63500 Akcakale, Turkey
Abstract
The presence of increased resistance in uterine artery Doppler measurements is associated with preeclampsia and other adverse pregnancy outcomes. Therefore, this study aimed to evaluate whether a full or empty bladder affects uterine artery Doppler results.
This study included 213 women with singleton pregnancies between 11–13 weeks. The first measurement for bilateral uterine artery Doppler parameters was performed while the patients experienced a full bladder, while the second measurement was conducted immediately following urination.
Uterine artery notching presented statistically significant results when the bladder was evaluated as full and empty. While the mean values calculated for the left uterine artery pulsatility index were 1.82 ± 0.04 before micturition, this value was calculated as 1.74 ± 0.04 after micturition (p = 0.011). The mean value for the right uterine artery while the mean value was 1.85 ± 0.042 before micturition, it was calculated as 1.81 ± 0.041 after micturition (p < 0.001). Uterine artery resistance indices were also statistically different before and after micturition. The mean values calculated for the left uterine artery resistance index were 0.77 ± 0.008 before micturition and 0.74 ± 0.007 after micturition (p = 0.003). For the right uterine artery, it was calculated as 0.76 ± 0.008 before micturition and 0.75 ± 0.01 after micturition (p = 0.047).
Although there are minimal studies on this subject in the literature are limited, physiological principles and the results of the present study show that emptying the bladder before arterial Doppler evaluation of spaces such as the abdominal compartment, will provide more accurate results.
Keywords
- Doppler
- pregnancy
- ultrasonography
- urinary bladder
- uterine artery
Doppler ultrasonographic evaluation of the uterine arteries during the first trimester is a frequently used method for the prediction of uteroplacental pathologies such as preeclampsia and fetal growth restriction [1, 2, 3]. The presence of increased resistance in uterine artery Doppler measurements is associated with preeclampsia and other adverse pregnancy outcomes [4, 5, 6]. This evaluation method, which is considered to provide very valuable information about the uteroplacental unit, is performed with a standardized technique, it is very easy to apply, and little attention is paid as to whether the pregnant patient’s bladder is full or empty [7]. However, theoretically, bladder distension could potentially increase uterine artery resistance indices by stretching the vessels. When the limited number of studies on this subject in the literature were evaluated, it appeared that a full bladder increased uterine artery resistance [8]. We aimed to present the results of our study in which we evaluated the effect of bladder distension on uterine artery flow parameters.
The necessary permissions for the realization of this study were obtained from the Canakkale Onsekiz Mart University Clinical Research Ethics Committee (18920478-050.01.04-E.2000149840; 23.09.2020). The study consisted of pregnant patients who applied to the tertiary healthcare unit of Canakkale Onsekiz Mart University Hospital, Gynecology, and Obstetrics Clinics between January 2022 and June 2022. Informed consent was obtained from all participants before the study and the principles of the Declaration of Helsinki were applied. The inclusion criteria were being between 17–43 years of age, being between 11 w+2 d and 13 w+6 d gestational week, and having a singleton pregnancy. The study was conducted with 213 patients who met the inclusion criteria. Gestational age was calculated from the last menstrual period and was confirmed by a fetal crown-rump length measurement. Ultrasonographic evaluation was performed by 2 specialist physicians using high-resolution probes Voluson® S6 ( © 2016 General Electric Company. Connecticut, ABD). All participants filled out a form containing demographic characteristics such as their last menstrual period, gravity, parity, number of abortions, age, height, and weight. The formula of dividing the body weight in kilograms by the square of the height in meters was used to calculate the Body Mass Index. Those with hypertension, diabetes, vasculopathy, multiple pregnancies, smoking or current use of anticoagulant drugs were not included in the study. The first measurement for bilateral uterine artery Doppler parameters was performed while the patients were experiencing a full bladder, and the second measurements were made just after the patients urinated (empty bladder). To do this, all participants were asked before and after the test whether they felt the urgency to urinate (Fig. 1).
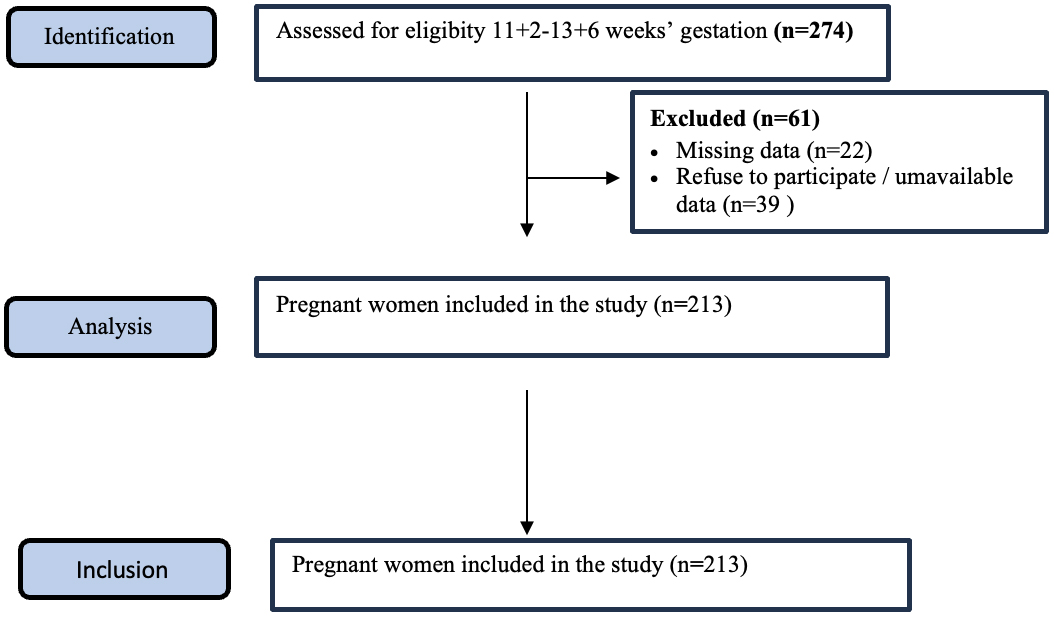 Fig. 1.
Fig. 1.
Flow diagram of patient recruitment.
The uterine arteries were visualized by obtaining an image of the cervical canal
and slowly shifting the ultrasonography probe to the right and left sides. During
the arterial pulsed Doppler sonography, the insonation angle was set to be less
than 30° and the sample spacing was set to 2 mm. In this way, at least 3
wavelengths were recorded. Bladder volume was calculated by measuring 3
orthogonal bladder diameters and applying the volume formula of an ellipsoid
shape (rostrocaudal diameter
All data were recorded on the SPSS 25.0 (SPSS Inc., Chicago, IL, USA). The
suitability of the parameters to the normal distribution was evaluated with the
Kolmogorov-Smirnov Test. Since our parameters were in accordance with the normal
distribution, the paried sample t-test was used and the Chi-Square Test
was used for categorical variables. continuous and categorical variables were
compared in terms of Mean
The study, planned with 274 patients, was completed with 213 patients, 61
patients were excluded from the study because of missing data (n =
22) and refusing to participate/unavailable data (n =
39) (Fig. 1). The quality of the images was considered satisfactory, and
no case was excluded from the analysis. Therefore, all 213 cases were evaluated.
The mean age of the women included in the study was 28.10
| Mean |
Minimum | Maximum | Median | |
| Age (year) | 28.1 |
17.00 | 43.00 | 28.00 |
| BMI (kg/m2) | 25.96 |
15.40 | 51.60 | 24.90 |
| CRL (mm) | 60.10 |
45.90 | 84.00 | 59.00 |
| NT (mm) | 1.34 |
0.80 | 2.20 | 1.32 |
| Bladder volume (before micturition) (mL) | 261.34 |
221.00 | 298.00 | 262.00 |
| Bladder volume (after micturition) | 12.03 |
1.00 | 38.00 | 10.00 |
BMI, Body mass index; CRL, Crown-rump lenght; NT, Nuchal translucency; SD, standard deviation; kg/m2, kilogram/square meter; mm, millimeter; mL, milliliter. Normality of the data was evaluated with skewness and kurtosis.
Uterine artery notching revealed statistically significant results when the
bladder was evaluated as full and empty. While notching was observed in the left
uterine artery in 94 cases before micturition, notching continued in only 39 of
these cases after micturition. The p-value was calculated as
| After micturition yes (n) | After micturition no (n) | Total (n) | p value | |
| Left UtA before micturition yes | 39 | 55 | 94 | |
| Left UtA before micturition no | 17 | 102 | 119 | |
| Right UtA before micturition yes | 33 | 49 | 82 | |
| Right UtA before micturition no | 21 | 110 | 131 |
UtA, uterine artery; n, sample size. Significant difference at p
While the mean values calculated for the left uterine artery pulsatility index
were 1.82
| Before micturition | After micturition | t test | n | p value | |
| Mean |
Mean | ||||
| Left UtA-PI | 1.82 |
1.74 |
2.052 | 213 | 0.011 |
| Right UtA-PI | 1.85 |
1.81 |
0.908 | 213 | |
| Left UtA_RI | 0.77 |
0.74 |
2.598 | 213 | 0.003 |
| Right UtA_RI | 0.76 |
0.75 |
0.581 | 213 | 0.047 |
UtA, uterine artery; PI, Pulsatility index; RI, Resistance index; SD, standard
deviation; n, sample size. Normality of the data was evaluated with skewness and
kurtosis values and significant difference at p
Uterine artery Doppler flow parameters can be affected by hormonal changes in
the menstrual cycle, blood pressure, maternal heart rate, and various drugs. It
is an important factor in determining the flow of uteroplacental vessels during
pregnancy. In our study, apart from the known factors, it was investigated
whether bladder fullness or emptying was also an important factor. The right and
left uterine artery notching values were examined before and after micturition,
and it was found that the notching value decreased at a statistically significant
level. The pulsatility indices of uterine arteries before and after voiding were
examined. It was observed that the change in the left and right uterine artery
pulsatility index was statistically significantly lower. Our results showed that
the state of the bladder affects Uterine Artery Resistance and Pulsatility Index.
Doppler Pulsatility Index (PI) and Resistive Index (RI) are frequently used to
predict preeclampsia [9, 10]. In their study conducted with 51 pregnant patients,
Özel and Şen [11] reported that whether the bladder is full or empty does
not affect the Uterine Artery Pulsatility Index and Uterine Artery Notching. The
mean age of the population studied was 30.3
The main limitation of the present study was that since our hospital is a tertiary advanced healthcare center, the patients who apply generally have additional diseases. These patients were excluded. Another limitation was that the ultrasound measurements were made before and after micturition, which was very time-consuming for each patient. This obstacle was overcome by planning to measure only 4 patients per day.
Although there are not enough studies on this subject in the literature, physiological principles and our study show that emptying the bladder before arterial Doppler evaluations of spaces such as the abdominal compartment may give more accurate results.
The data that support the findings of this manuscript can be provided on request from the first author.
MND: study selection, data extraction, risk of bias assessment and manuscript revision, statistical analysis; SSD: manuscript drafting and revision, study selection, data extraction, risk of bias assessment, manuscript drafting and revision; LSD: conceptualization, supervision and manuscript revision statistical analysis, manuscript drafting and revision; IEP: original draft, conceptualization, data extraction, risk of bias assessment and manuscript revision; SKI: data extraction, statistical analysis, manuscript drafting and revision; BD: study selection, data extraction, risk of bias assessment, statistical analysis, manuscript drafting, and revision. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The necessary permissions for the realization of this study were obtained from the Canakkale Onsekiz Mart University Clinical Research Ethics Committee with the approval numbered: 18920478-050.01.04-E.2000149840, date: 23.09.2020. Informed consent was obtained from all participants before the study and the principles of the Declaration of Helsinki were applied.
We express our gratitude to all the participants who contributed to this study.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.