



 , Nurdan Demirci 3
, Nurdan Demirci 31 Department of Obstetrics and Gynecology Nursing, Division of Obstetrics and Gynecology Nursing, Institute of Health Sciences, Marmara University, 34700 Istanbul, Türkiye
2 Department of Midwifery, Division of Midwifery, Faculty of Health Sciences, Çanakkale Onsekiz Mart University, 17100 Çanakkale, Türkiye
3 Department of Obstetrics and Gynecology Nursing, Division of Nursing, Faculty of Health Sciences, Marmara University, 34700 İstanbul, Türkiye
Abstract
Postoperative ileus after cesarean section prolongs hospital stays and increases perioperative costs. The impact of fennel tea and chewing gum on bowel motility remains unclear. Therefore, this study aimed to evaluate the effects of chewing gum and fennel tea on intestinal motility after cesarean section.
A randomized controlled trial was conducted between January 2018 and April 2018 with 120 participants divided into four groups: chewing gum, fennel tea, chewing gum plus fennel tea, and control (n = 30 per group). Bowel sounds, time to first flatulence, and defecation were recorded. Data were analyzed using statistical tests with p < 0.05 considered statistically significant.
The chewing gum plus fennel tea group exhibited the earliest onset of bowel sounds (6.96 ± 3.41 hours). The fennel tea group demonstrated the shortest time to first flatulence (15.47 ± 7.77 hours) and first defecation (21.02 ± 8.75 hours) compared to the other groups (p < 0.05). Although chewing gum alone promoted enhanced bowel motility, it was less effective than fennel tea alone. No complications or adverse events were reported in any group.
Chewing gum and fennel tea are cost-effective interventions to improve intestinal motility post-cesarean section. Incorporating these remedies into postoperative care may reduce gastrointestinal complications.
This study has been registered on https://classic.clinicaltrials.gov/ (registration number: NCT06403215).
Keywords
- bowel sounds
- cesarean section
- chewing gum
- fennel tea
Postoperative ileus (POI), often referred to as oral diet intolerance after cesarean delivery in the Enhanced Recovery After Surgery (ERAS) protocol, is a significant postoperative complication. POI typically manifests as nausea, vomiting, oral diet intolerance, absence of defecation, and abdominal distension within 24 hours to 4 days [1, 2, 3]. It is a major clinical challenge as it prolongs hospital stays and increases healthcare costs.
Chewing gum has been extensively studied for its potential to prevent POI. Meta-analyses and clinical trials have demonstrated its efficacy in reducing the time to first flatulation and defecation after surgery [4, 5, 6, 7]. For instance, a meta-analysis by Ciardulli et al. [7] reported a 6.5-hour reduction in time to first flatulation among patients who chewed gum postoperatively. Despite these findings, further studies are required to evaluate the safety and broader applicability of chewing gum, particularly after cesarean delivery [8, 9, 10].
Herbal teas, including fennel tea, are also recognized for their ability to enhance intestinal motility [11, 12, 13]. Fennel is widely used for managing gastrointestinal complaints such as bloating, spasms, and flatulence. Experimental studies have demonstrated its efficacy in increasing bowel movements and its antispasmodic properties [14, 15, 16, 17]. Traditional medicine systems, such as Unani and Siddha, have long incorporated fennel in gastrointestinal treatments [18, 19, 20]. However, evidence on its use in postoperative settings, particularly after cesarean sections, remains limited.
Although the effects of chewing gum and fennel tea on intestinal motility have been individually explored, their combined effects, particularly in cesarean sections, remain underexplored. This study addresses this gap by evaluating both independent and combined interventions, providing new insights into their clinical applicability.
This parallel, monocenter, randomised controlled experimental study was carried out at the maternity services of the department of Cerrahpasa Medical Hospital of Istanbul University between January 2018 and April 2018 with the Consolidated Standards of Reporting Trials (CONSORT) guidelines (Fig. 1) [21].
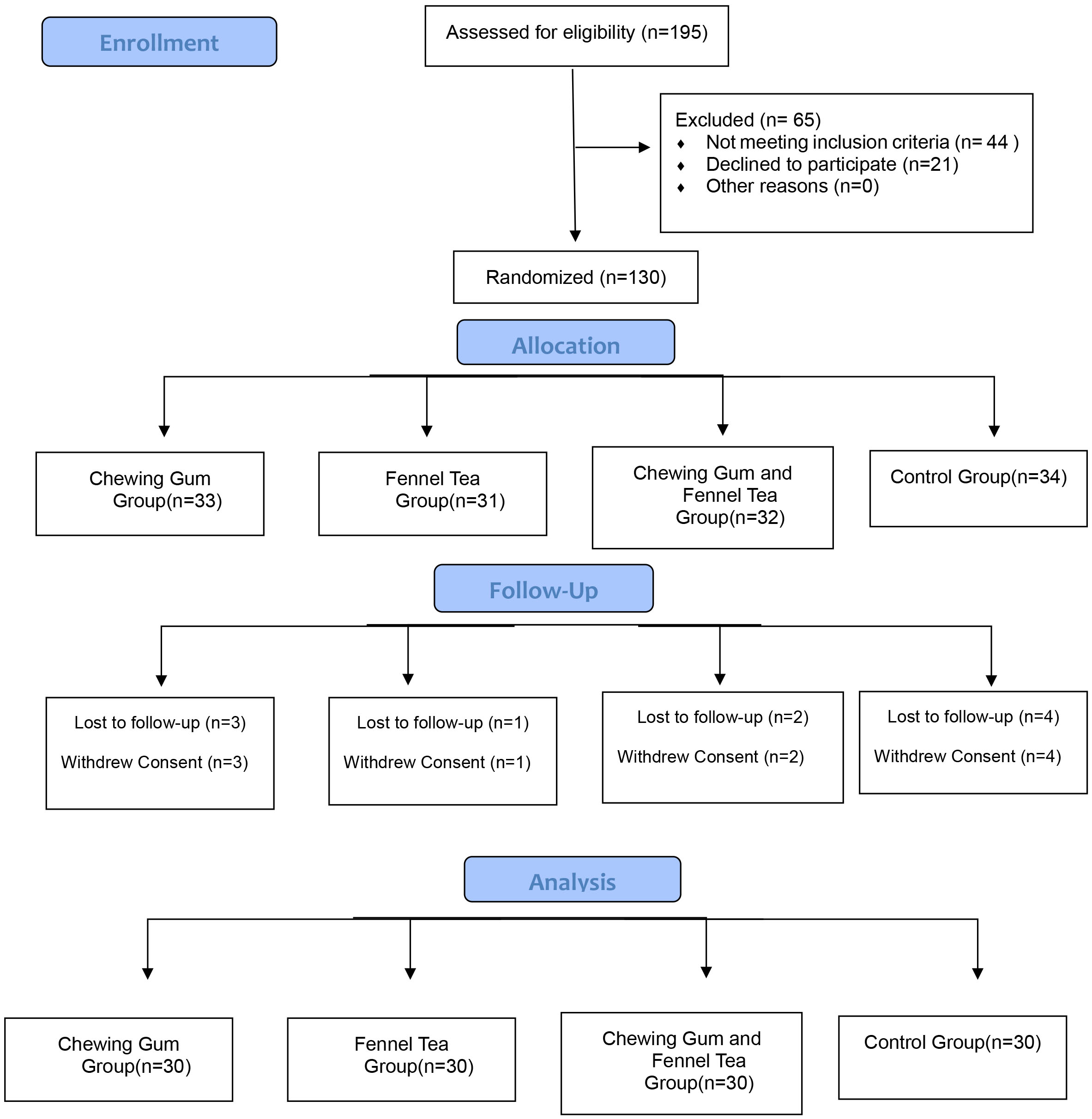 Fig. 1.
Fig. 1.
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
Women were randomly assigned to the gum, fennel tea, gum-fennel tea groups and the control group in a 1:1:1:1 ratio. Women in all groups were followed for 48 hours during cesarean delivery.
Inclusion criteria included healthy women who underwent elective cesarean section under general anesthesia, had at least a primary school education, no chronic systemic diseases, no complications during pregnancy (e.g., preeclampsia, gestational diabetes, or placental abnormalities), no history of allergies, a body mass index (BMI) between 18.50 kg/m2 and 24.99 kg/m2, no prior abdominal surgeries, and no complications during the cesarean procedure. Elective cesarean sections were selected to standardize recovery conditions and reduce variability associated with emergency procedures or complications, such as fetal distress or placenta previa, that might independently affect bowel motility. Women with BMI outside the normal range (18.50–24.99 kg/m2) were excluded to limit variability caused by nutritional and metabolic factors, which could influence intestinal motility.
The exclusion criteria were as follows: age
Using SPSS 24.0 (IBM Corp., Armonk, NY, USA), a random sequence was generated by an independent researcher who was not involved in recruitment, treatment, follow-up, or data processing, ensuring unbiased allocation. The random sequences were sealed in opaque envelopes to maintain allocation concealment. After obtaining informed consent, nurses opened the envelopes to assign participants into four groups in a 1:1:1:1 ratio. The data analysts were blinded to the group assignments to prevent bias in data interpretation. Although the women, environment, and researchers conducting the interventions were not blinded due to the nature of the applications, strict measures were taken to prevent any communication between subjects and data analysts. This ensured that the analysts could not infer group information from the questionnaire findings, maintaining the integrity of the blind evaluation process.
According to the Obstetrics and Gynecology Hospital protocol, 3000 mL of intravenous fluid was administered during the postoperative period. Oral fluid intake commenced six hours after the cesarean operation performed under general anesthesia, regardless of whether intestinal motility had resumed. Following this, the urethral catheter was removed, and mobilization was initiated. Women who experienced flatulation and defecation were discharged 48 hours after surgery as per hospital protocol. However, those who did not exhibit these outcomes were not eligible for discharge until these criteria were met, ensuring early detection and management of potential complications.
During the follow-up process:
-Bowel sounds of the women were listened to by the researcher using the same stethoscope, which was held over the women’s abdomen following the cesarean section. Bowel sounds were listened to every 15 minutes and the first time the bowel sounds could be heard was determined and recorded by the researcher.
-The time of the first flatulation and the time of the first defecation were determined by verbally asking the women and then recorded by the researcher. The researcher stayed at the hospital until the evaluation of bowel sounds after the cesarean section was completed.
The objective of this study was to evaluate the effects of chewing gum and drinking tea on the postoperative recovery process. Both practices are methods used to encourage bowel movements and facilitate the return of the digestive system to its early functional state. The chewing gum protocol (15 minutes every two hours) was adapted from previous randomized controlled trials demonstrating its efficacy in enhancing bowel motility [22]. Similarly, the fennel tea dosage (2 grams per serving) aligns with traditional practices and studies indicating its antispasmodic effects [15]. The incorporation of these methods within the scope of patient education is intended to reduce postoperative complications by enhancing self-care skills. Four different interventionschewing gum and drinking fennel teawere conducted in this study.
Women in this group chewed sugar-free and non-xylite gum for 15 minutes every two hours (2nd, 4th, and 6th) following the cesarean operation. Therefore, in the current study, women chewed gum for 15 minutes every two hours, following two hours after the cesarean operation. The bowel sounds of the women were listened to and their flatulation times were recorded before and after gum chewing for 15 minutes every two hours. When women were allowed oral intake, gum-chewing activity was terminated completely. Data for the first time of flatulation and the first defecation were collected by verbally asking women, and these data were recorded in the follow-up form.
Women in this group started oral intake 6 hours after cesarean delivery and were allowed to drink 2 grams of fennel tea in the 6th, 8th, and 10th hours (a total of 6 grams of fennel tea). Fennel seeds (2 grams) were put into 150 mL water, boiled at a temperature of 100 °C, and left for 20 minutes. Women were then instructed to drink the tea. Bowel sounds were recorded every 2 hours, before and after drinking the fennel tea. The time of the first flatulation and the first defecation were determined by asking the women themselves and this information was then recorded using the study form.
Women in this group chewed sugar-free and xylitol-free gum for 15 minutes every two hours (2nd, 4th and 6th) following the cesarean section. In accordance with the hospital routine and study protocol, women were started on oral feeding 6 hours after cesarean delivery and were allowed to drink 2 grams of fennel tea (6 grams of fennel tea in total) at 6, 8 and 10 hours.
The women’s bowel sounds were listened to and the duration of flatulence was recorded before and after chewing gum for 15 minutes every two hours. Bowel sounds were recorded every 2 hours, before and after drinking the fennel tea.
Data on the time of first flatulation and first defecation were collected by asking the women verbally and these data were recorded on the follow-up form.
Bowel sounds were monitored at 0, 2, 4, 6, 8, and 10 hours in accordance with the hospital’s routine study protocol. Oral feeding was initiated six hours after cesarean delivery. Data on the time of first flatulation and defecation were collected verbally from the participants and recorded on the follow-up form. Laxative medication was not administered. Participants were not discharged from the hospital until flatulation and defecation were observed. Forty-eight hours post-surgery, bowel sounds were re-evaluated to check for any complications, but none were observed.
In the control group, no placebo or additional intervention was provided. Participants in this group followed the hospital’s standard postoperative care protocol, allowing for a comparison against the intervention groups to evaluate the effects of chewing gum and fennel tea. According to hospital protocol, discharge was contingent upon the occurrence of flatulation and defecation, emphasizing the clinical relevance of these outcomes. This protocol ensures early detection and management of potential complications. Consequently, discharge times were included as a secondary outcome to highlight their significance in postoperative recovery. In addition to monitoring bowel sounds, participants were observed for signs of postoperative complications, including, but not limited to, nausea, vomiting and abdominal pain during their hospital stay.
The main objective of this study was to evaluate the effect of chewing gum and fennel tea on bowel motility after cesarean delivery. The primary outcome directly measures the effect of these treatments. Specifically, it will be assessed by examining factors such as the rate of bowel motility and flatus after cesarean delivery. These measurements are critical to determine the effect of the treatments on bowel function. The researcher assessed bowel sounds at 0, 2, 4 and 6 hours after cesarean delivery.
Secondary outcomes include factors the woman’s first flatulation and the first bowel sounds. These measures will be used to understand the impact of treatments and draw clinically meaningful conclusions more comprehensively. The time of the first flatulation and the first defecation were determined by asking the women themselves and this information was then recorded using the study form.
The study was carried out with four different groups determined by 22 factorial trial levels. The sample size was determined as a total of 120 participants at 80% power and 95% confidence interval in consideration of the meta-analysis conducted on the data of the subjects [23].
Adverse events were defined as any unexpected medical occurrences during or after the interventions, including gastrointestinal discomfort (e.g., bloating, nausea, vomiting), allergic reactions, or surgical site complications requiring medical intervention. Participants were closely monitored for adverse events throughout the 48-hour follow-up period. Any observed events were recorded and reported immediately. No adverse events were identified during the study.
The compatibility of the variables with normal distribution was examined using
the Kolmogorov-Smirnov test. For normally distributed (parametric) variables,
one-way analysis of variance (ANOVA) was used to compare differences between
groups. Categorical data were analyzed using Chi-square and Fisher’s exact tests.
The skewness and kurtosis values for these variables were within the acceptable
range (–1 to +1), indicating that the data were normally distributed. Therefore,
the parametric one-way ANOVA is used to evaluate differences among groups.
Statistical analyses were conducted using SPSS Statistics for Windows, Version
24.0 (IBM Corp., Chicago, IL, USA). A p-value
The mean age of the subjects was found to be 29.5
| Chewing gum group (n = 30) | Fennel tea group (n = 30) | Chewing gum and fennel tea group (n = 30) | Control group (n = 30) | p | |||||||
| n | % | n | % | n | % | n | % | ||||
| Age (years) | |||||||||||
| 18–24 | 4 | 13.3 | 9 | 30.0 | 4 | 13.3 | 8 | 26.7 | |||
| 25–34 | 26 | 86.7 | 21 | 70.0 | 26 | 86.7 | 18 | 60.0 | |||
| 35 or over | 0 | 0.0 | 0 | 0 | 0 | 0.0 | 4 | 13.3 | |||
| Education status | |||||||||||
| Primary school | 7 | 23.3 | 9 | 30.0 | 9 | 30.0 | 7 | 23.3 | 15.182 | 0.086 | |
| Second school | 9 | 30.0 | 4 | 13.3 | 5 | 16.7 | 8 | 26.7 | |||
| High school | 6 | 20.0 | 4 | 13.3 | 10 | 33.3 | 12 | 40.0 | |||
| University | 8 | 26.7 | 13 | 43.4 | 6 | 20.0 | 3 | 10.0 | |||
| Smoking status | |||||||||||
| Yes | 26 | 86.7 | 25 | 83.4 | 24 | 80.0 | 21 | 70.0 | 2.917 | 0.405 | |
| No | 4 | 13.3 | 5 | 16.6 | 6 | 20.0 | 9 | 30.0 | |||
| Herbal tea drinking status | |||||||||||
| Yes | 14 | 46.7 | 7 | 23.3 | 7 | 23.3 | 5 | 16.7 | 7.816 | 0.050* | |
| No | 16 | 53.3 | 23 | 76.7 | 23 | 76.7 | 25 | 83.3 | |||
It was found that 53.3% of the chewing gum group, 76.7% of the fennel tea group, 76.7% of the chewing gum and fennel tea group, and 83.3% of the control group did not use herbal tea during pregnancy.
Bowel sounds were heard earliest (6.96
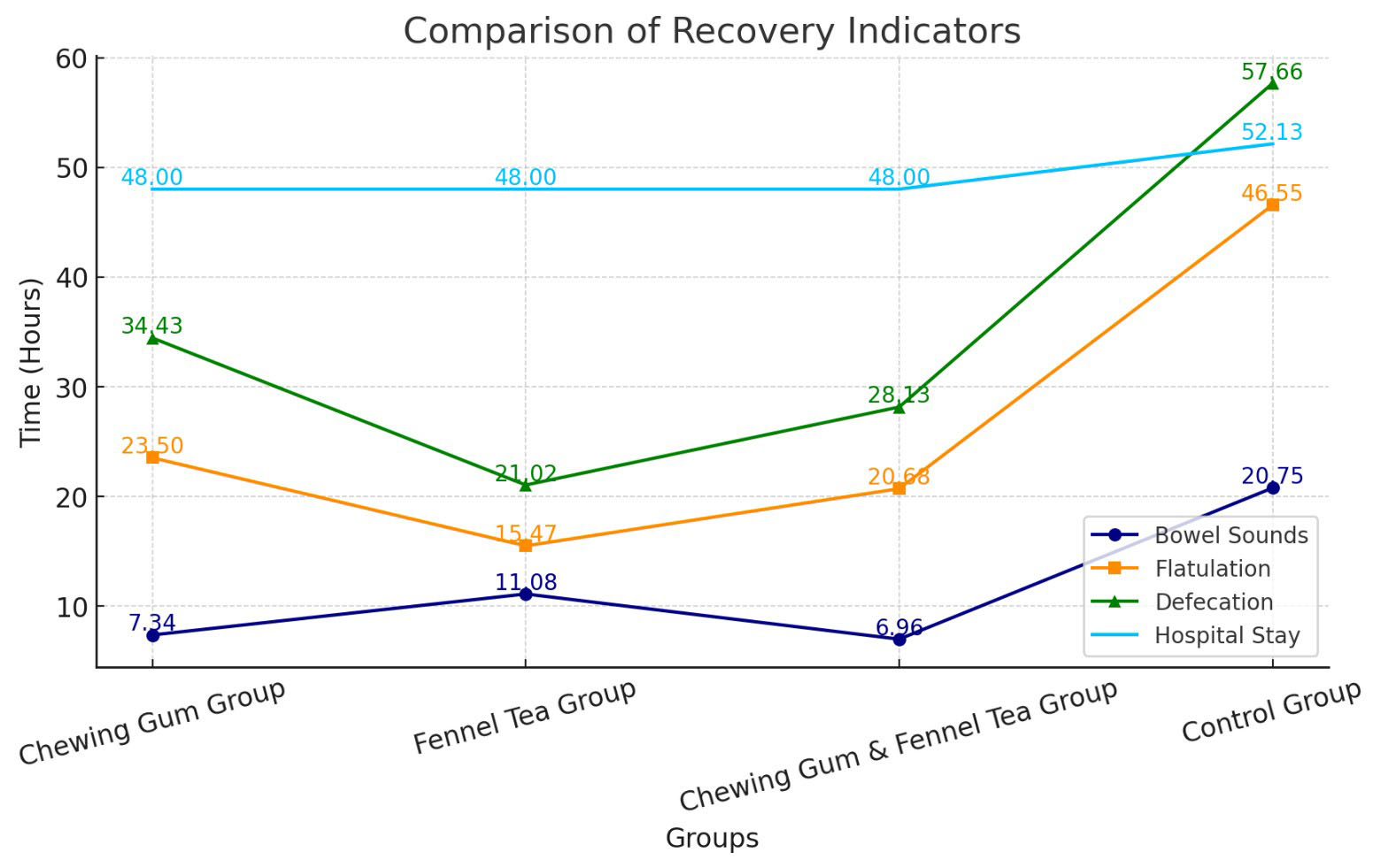 Fig. 2.
Fig. 2.
Distribution of the groups according to intestinal motility after cesarean delivery.
| Time of bowel sounds (hours) | Time of flatulation (hours) | Defecation time (hours) | Hospital stay (hours) | |
| M |
M |
M |
M | |
| Chewing gum group (n = 30) | 7.34 |
23.50 |
34.43 |
48.00 |
| Fennel tea group (n = 30) | 11.08 |
15.47 |
21.02 |
48.00 |
| Chewing gum and fennel tea group (n = 30) | 6.96 |
20.68 |
28.13 |
48.00 |
| Control group (n = 30) | 20.75 |
46.55 |
57.66 |
52.13 |
| Statistical analysis (p), test | 0.001* | 0.001* | 0.001* | |
| F = 85.88 | F = 52.98 | F = 63.06 |
M
The time of the first flatulation was found to be the earliest (15.47
The defecation time after cesarean delivery occurred the earliest (21.02
The duration of hospital stay was found to take a long time for participants in
the control group, which comprised individuals who experienced no application.
While the women in the control group were scheduled for discharge after an
average of 52.13
Our study is the first and valuable study to use fennel tea to improve intestinal motility in the postpartum period. Results show that fennel tea is effective in improving intestinal motility after cesarean section. Consistent with current findings in the literature, gum chewing may play a potential role in accelerating gastrointestinal function in the postoperative period. These results emphasize that the use of fennel tea should be considered a simple and low-cost intervention for early mobilization and improvement of gastrointestinal function in postoperative patients.
Several studies have demonstrated the effectiveness of chewing gum in reducing postoperative ileus by accelerating first flatulation and defecation times [1, 24, 25, 26, 27]. For instance, meta-analyses and randomized trials have consistently reported shorter times for intestinal motility recovery in patients who chewed gum compared to controls [7, 23]. Similarly, fennel tea has been shown to improve gastrointestinal function in animal studies, although human trials remain limited. This study builds on these findings by evaluating the combined effects of chewing gum and fennel tea, contributing novel insights to the field.
For the examination of the time of women’s first defecation according to the
application group, the earliest time was found for the fennel tea group (21.02
The result of this study showed a significant difference in the first time of flatulation of the group that consumed only fennel tea compared with those groups who chewed gum, and those who chewed gum and drank fennel tea. Fennel contains many flavonoids (such as quercetin, isoquercetin, and kaempferol), gallic acid, p-coumaric acid, chlorogenic acid, and phenolic compounds. Accordingly, the fact that the fennel tea group played a more active role in the first time of flatulation than chewing gum groups likely resulted in due to the components in the fennel [23]. Venkataranganna et al. [30] examined the effect of fennel-containing tea on smooth muscles of the gastrointestinal system in guinea pigs, rats, rabbits, and mice and the researchers found that the tea had antispasmodic activity. A recent review Rafieian et al. [31] demonstrated that fennel tea alleviates colic symptoms and exerts a smooth muscle-relaxant effect on the gastrointestinal system. However, future studies in humans with larger samples should confirm the generalizability and clinical applicability of these findings. Furthermore, long-term follow-up studies are needed to assess the long-term effects and possible side effects of fennel tea. Accordingly, this study is expected to make a significant contribution to the literature regarding the clinical use of fennel tea.
Due to the hospital protocol according to which the current study was conducted, women were routinely discharged after 48 hours to prevent any complications and to intervene early. Therefore, the time of discharge occurred regardless of fennel tea and chewing gum applications.
This study encountered four main limitations: (a) there was no quantitative monitoring or recording of postoperative physical activity, preventing examination of any potential impact on recovery from postoperative ileus. (b) Patients were supervised by the same researcher during 15 minutes of gum-chewing, with varying methods and speeds that couldn’t be standardized. The impact of variations in chewing speed on the outcomes was not evaluated. (c) The length of hospital stays, set at 48 hours, without any differences across groups. (d) The research was restricted to patients from a local instructional hospital in Istanbul, restricting the applicability of the conclusions to other regions. Additionally, it is necessary to expand the range of patients included, conduct larger multicenter trials, and employ larger sample sizes to enhance the generalizability of findings.
This study examines the effects of chewing gum and drinking fennel tea on intestinal motility following caesarean section. A primary strength of the study is its novel approach, specifically the addition of fennel tea as a method to enhance intestinal motility in this patient population. However, a potential limitation is that chewing gum is already a well-established method, which may somewhat diminish the study’s novelty. Additionally, the observed differences in age and tea-drinking habits between the groups are unlikely to have influenced the outcomes, as randomization was performed without stratification for these variables. This ensured that potential confounding factors were evenly distributed across the groups, minimizing their impact on the study results.
The combination of chewing gum and fennel tea represents a relatively unexplored approach in cesarean section recovery. Despite individual efficacy, this study contributes novel insights into their potential synergistic effects. However, the combination did not demonstrate a statistically significant improvement compared to the individual interventions. This finding suggests that both chewing gum and fennel tea independently enhance intestinal motility, with their combined use offering no additional benefit. This outcome may be explained by a ceiling effect, where each intervention already provides a substantial benefit, leaving little room for further enhancement. Future studies should focus on larger sample sizes and long-term follow-up to evaluate the broader applicability of these findings. Additionally, while the indications for cesarean delivery may influence postoperative bowel motility, our study minimized this factor by excluding participants with pregnancy complications and focusing on elective cesarean sections. Future research should consider stratifying participants based on cesarean indications to further evaluate their impact.
In this study, no issues were observed regarding the use of gum chewing and fennel tea in women who underwent cesarean section. Postoperative problems, such as difficulty with flatulence, inactivity, hospital infections, and delayed wound healing in the early period, can sometimes delay discharge for cesarean patients; however, the interventions used in this study appeared to be well tolerated and free of complications.
The data supporting the findings of this study are not publicly available and restrictions apply to the availability of these data.
RÖY conceived the study. RÖY and ND searched the literature and collected the data. RÖY and ND performed the statistical analysis. RÖY drafted the manuscript. ND reviewed the manuscript. Both authors contributed to editorial changes in the manuscript. Both authors have read and approved the final paper. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This trial was registered at Clinical Trial Registry: NCT06403215. The study was conducted in accordance with the Declaration of Helsinki and were approved by Marmara University Interventional Clinical Research Ethics Committee (Protocol No: 09.2017.586). All patients signed informed consents.
We would like to express our sincere gratitude to Prof. Emine Akalın, Head of the Department of Pharmaceutical Botany at the Faculty of Pharmacy, Istanbul University, and Assoc. Prof. Gülay Ecevit Genç for their invaluable scientific contributions and academic guidance in this study on fennel tea.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.