


 , Patricia Catala 1, Lorena Gutierrez 1, Cecilia Peñacoba-Puente 1,*
, Patricia Catala 1, Lorena Gutierrez 1, Cecilia Peñacoba-Puente 1,*
1 Department of Psychology, Rey Juan Carlos University, 28932 Madrid, Spain
Abstract
It is estimated that around 20% of women experience mental health problems during the perinatal period, including depression and anxiety, which negatively affect both the mother and the baby’s development. Although previous mental health problems have been identified as important predictors, it is relevant to further explore the role of other psychosocial variables of interest such as coping with worries or maternal confidence in caring for the baby, in order to design effective preventive actions to promote perinatal mental health. This study analyzed the effect of maternal lack of confidence in caring for her infant and depressive symptoms on pregnancy worries (PW) and postpartum depression (PPD) using a multifactorial and prospective approach.
A prospective cohort study (with three points in time) was conducted with 120 pregnant women recruited from a public hospital in Madrid, Spain. Women were evaluated for pregnancy worries in the first trimester of pregnancy, for depressive symptoms in the third trimester, and for PPD and mothers’ lack of confidence 4 months after childbirth. Parallel and serial mediation analyses were conducted using PROCESS (SPSS tool for estimating regression models with mediation and/or moderation effects). According to the Enhancing the Quality and Transparency Of health Research (EQUATOR) checklist, the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement was chosen for this study.
A parallel multiple model showed that while depressive symptoms significantly mediated the relationship between pregnancy worries and postpartum depression (a1b1 = 1.4733, [95% confidence interval (95% CI) = 0.7105, 2.2309]), mothers’ lack of confidence did not (a2b2 = 0.2404, [95% CI = –0.0569, 0.5826]). However, when both mediators were analyzed together, a significant indirect effect of depressive symptoms on postpartum depression was found through the effect of depressive symptoms on mothers’ lack of confidence (d21 = 0.2144, [95% CI = 0.0595, 0.4562]).
It is necessary to analyze factors related to postpartum depression from a multifactorial approach focused on the analysis of depression during pregnancy, but also including other variables such as mothers’ lack of confidence as possible risk factors of postpartum depression. The associations found between worries, depressive symptoms, and maternal insecurity with postpartum depression could allow professionals to develop preventive interventions of postpartum depression.
Keywords
- pregnancy worries
- depressive symptoms
- mothers’ lack of confidence
- postpartum depression
Pregnancy can be defined as a life event that could lead to negative consequences on maternal wellbeing [1], becoming a mother is certainly a stressful situation that might be moderated by variables regarding childcare that require the implementation of strategies to help to cope with this new experience [2]. Maternal competence refers to a woman’s perceived ability to care for her child and the impact this perception has on her sense of self as a mother and on the quality of care she provides to her child [3].
Depression has been found to be a common mental health problem experienced not only during pregnancy, but also postnatally [4], with substantial and long-term consequences for both the mothers and the infants [5, 6, 7]. However, although a promising integrative conceptual framework exists and personalized treatments have increased, the condition is underdiagnosed, and screening is still lacking [7, 8]. Specifically, the guidelines of the American College of Obstetricians and Gynecologists (ACOG) recommend that clinicians screen for depressive symptoms (DS), but it only recommends at least one screen during the perinatal period, without specifying an ideal time for depressive screening [9]. The psychological wellbeing of new mothers is essential to their ability to navigate and adjust to their new situation therefore, the role of healthcare professionals is essential to screening when, throughout the perinatal period, women need more attention related to depressive symptoms, due to the transitions that take place during this time.
One of the variables suggested to play a role in psychological adjustment during the perinatal window is perseverative thinking about negative content, and women frequently report difficulty disengaging from their pregnancy and maternal worries [10]. Worries are defined by an endless chain of defeatist thoughts about difficult situations to be faced in the future. In pregnant women, worries usually originate during gestation and their content is related to childbirth or possible complications in the development of the fetus [11], and have been associated consistently with depression throughout the perinatal period [12, 13, 14], and with postpartum depression (PPD) [15]. Additionally, worries have been found to be a mediator between maternal psychopathology and parenting difficulties [16], and could compromise a mother’s capacity to process and respond to her infant’s cues in a timely manner [10, 17].
In this context, maternal competence [18, 19], has been considered as a dynamic emotional state that brings well-being to the newborn [19], and helps it to develop correctly at the cognitive and motor level [20]. However, depression can affect the mother’s capacity to bond with her new-born and it has shown that depressed mothers may react negatively towards the child [21, 22]. According to this, recent studies suggest that low maternal self-confidence creates a vulnerability mechanism where women perceive themselves as less capable of managing motherhood challenges, directly increasing PPD risk [23], and that diminished maternal self-confidence triggers negative cognitive schemas related to negative self-evaluation of maternal capabilities [24]. These cognitive patterns significantly predict PPD symptoms, creating a psychological pathway from low self-confidence to depressive symptoms [3, 24, 25, 26, 27, 28]. Thus, it seems that bonding depends on the emotional stability of mothers during gestation [29], hence it would be necessary to adopt a multifactorial and prospective approach to study the associations between variables that could confer vulnerability to mothers during gestation, but also during the postpartum period. To the best of our knowledge, no studies have yet been conducted in which pregnancy worries (PW) and postpartum depression have been associated with mothers’ lack of confidence (MLC) in caring for her infant and depressive symptoms during pregnancy.
Despite the lack of conclusions from previous studies, it is believed that worries originating during pregnancy continue to develop immediately after birth and during the first few months of the baby’s life [18, 19]. However, what remains unclear is, specifically, whether the combination of depressive symptoms and mothers’ lack of confidence may exacerbate the negative impact of worries on postpartum depression. Thus, the knowledge about worries and their influence on pregnancy and postpartum depression over time, mediated by the effect of depressive symptoms and mothers’ lack of confidence as contextual factors, may be an interesting point of study [30].
Specifically, the aim of this study has been to analyze whether depressive symptoms throughout pregnancy (third trimester) and mothers’ lack of confidence in caring for her infant (4 months after delivery) have a mediating effect in the relationship between pregnancy worries (in early pregnancy; first trimester) and postpartum depression (4 months after delivery) after controlling for sociodemographic data [15]. We expect that depressive symptoms during the third trimester mediate the effect of worries on postpartum depression [31, 32]. Moreover, we also expect that mothers’ lack of confidence in caring for her infant will share variance with depressive symptoms in the prediction of postpartum depression through pregnancy worries.
This study used a longitudinal prospective design that included three time points (first and third trimester of pregnancy, and 4 months postpartum). The study adhered to the most stringent ethical guidelines governing human participant research. Specifically, all experimental procedures were meticulously designed and implemented in full compliance with the 1964 Helsinki Declaration and its subsequent amendments, which represent the international gold standard for ethical medical research. It received comprehensive ethical review and obtained formal approval from Fuenlabrada University Hospital Ethics Committee (approval reference: CPMP/ICH/135/95). All women signed a consent form to declare a voluntary agreement with all procedures implicated in this project. According to the Enhancing the Quality and Transparency Of health Research (EQUATOR) checklist, the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement was chosen for this study.
This study is part of a larger study that aims to analyze the evolution of maternal psychosocial variables during pregnancy and postpartum. The study was carried out in Fuenlabrada University Hospital in Madrid (Spain), with an allocated population of 216,803, which provides care to about 3000 obstetric patients per year. Women were considered eligible for the study if they were of legal age (over 18 years), had a low-risk pregnancy with a maximum gestational age of 14 weeks, and were mentally and physically healthy without a psychiatric diagnosis during pregnancy. Out of 290 Spanish women evaluated during first-trimester, 120 (41.37%) met the inclusion criteria for the present study, which included being followed up in the third-trimester, immediately postpartum, and 4 months postpartum. Health status was defined by the absence of depression or any other psychiatric disorders. Additionally, the study exclusively included naturally conceived pregnancies, explicitly excluding in vitro fertilization-embryo transfer (IVF-ET) pregnancies.
In the first trimester of pregnancy (1–13 weeks of pregnancy), and according to the established inclusion criteria, a total of 290 pregnant women agreed to participate in this study. All women received their obstetric clinical care at the hospital where the study was carried out. During the first obstetric clinical appointment, coinciding with the first ultrasound (about 12–14 weeks of pregnancy), the midwife, and a member of the research team, informed the women about the study that was being carried out, and if they agreed, they signed the corresponding informed consent and filled out the evaluation protocol (see variables and instrument section), in the presence of the midwife in case any doubts arose. Sociodemographic and clinical data of interest were extracted from the clinical history. Of the total 290 women who completed the questionnaires five were excluded because of a miscarriage (n = 285). In the third trimester (around weeks 30), a new evaluation protocol (see variables and instrument section) was mailed to the women with a prepaid envelope for returning the completed questionnaire to the research team, 122 participants completed this phase. These women were evaluated again in the immediate postpartum period, during their hospital stay (although this measurement is not part of the present study) (n = 122). Finally, 4 months after delivery, the last evaluation protocol (see variables and instrument section) was sent in the post, obtaining a response from 120 women. To understand the sample loss, which is common in prospective studies, we should highlight that, in addition to there being different evaluation modalities used (in person, via mail), around 35% of the pregnant women treated at the hospital where we carried out the study did not end up giving birth there. There were no significant differences in sociodemographic, clinical or pregnancy variables between the first, third trimester, and 4 months after birth. Moreover, when main analyses were conducted no significant results were found in sociodemographic variables.
Pregnancy worries. We used the total score of the Spanish version of the Cambridge Worry Scale (CWS) [33]. It includes 16 items rated on a 6-point Likert-type scale ranging from 0 (not a worry) to 5 (major worry). The CWS is a specialized psychometric instrument designed to assess pregnancy-related concerns and anxieties among expectant mothers. Developed to provide a nuanced understanding of maternal psychological experiences, the scale offers critical insights into the complex emotional landscape of pregnancy. It was specifically created to capture the multidimensional nature of pregnancy-related worries. Unlike generic anxiety measures, it focuses explicitly on concerns unique to the maternal experience, providing a targeted approach to understanding psychological well-being during pregnancy. The global measure of pregnancy worries (average score of the 16 items; range 0 to 5) was used for this study. Cronbach’s alpha was 0.81 for this study.
Depression symptoms. The Spanish version of the Symptom Checklist-90-R (SCL-90-R) was used [34]. The SCL-90-R includes 90 items, rated on a 5-point Likert-type scale. This instrument has been widely used, translated, and validated into different languages, having shown good psychometric properties [35]. Despite it measuring 9 dimensions, the depression dimension (13 items; average score; range 0 to 4) was the one used in this study (Cronbach’s alpha of 0.87).
Postpartum depression. The Spanish version of the Edinburg Postnatal Depression Scale (EPDS) was used [36]. This scale includes 10 multiple choice items (4 options each), in which higher scores indicate higher postpartum depression. The total score can range from 0 to 30. An alpha value of 0.87, sensitivity of 85%, specificity of 77%, and a positive predictive value of 83% has been found in previous research [37]. In our sample, Cronbach’s alpha value was 0.82.
Lack of confidence in caring for the baby. Mothers’ perceptions were assessed using the Mother and Baby Scales (MABS) [38]. This scale represents a critical instrument in perinatal mental health assessment, designed to provide a comprehensive and nuanced evaluation of maternal psychological functioning during the postpartum period. It is a multidimensional assessment tool specifically developed to capture the complex psychological experiences of new mothers, evaluate both maternal mental health and mother-infant interactions, and to provide a holistic approach to postpartum psychological assessment. The questionnaire is made up of 63 items that assess two types of maternal perceptions: maternal confidence and self-efficacy and mothers’ perceptions of infant behaviors. The aim of this study focuses on the first. The Lack of confidence in caring for the baby scale consists of 13 items on a 6-point Likert-type response scale (0 = not at all to 5 = a lot/very much). The total score of the scale is obtained from the sum of the items (range 0 to 65). In our sample, the subscale showed a Cronbach’s alpha of 0.79.
Data were processed using SPSS version 23 (IBM, Chicago, IL, USA), with a
predetermined significance level of p
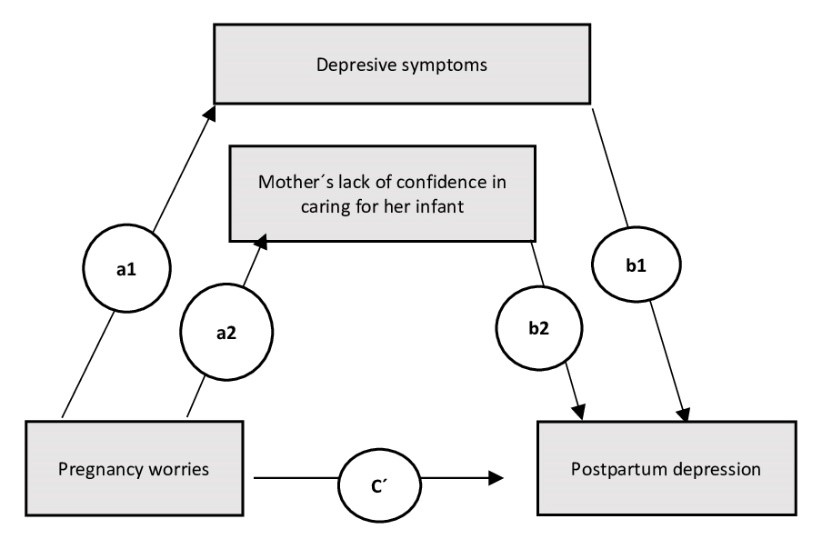 Fig. 1.
Fig. 1.
Hypothesized multiple model of the interrelationships between pregnancy worries, depressive symptoms (mediator 1), a mothers’ confidence in caring for her infant (mediator 2) and postpartum depression (dependent variable) a1-b1 (indirect effect of mediator 1); a2-b2 (indirect effect of mediator 2); C´: direct effect.
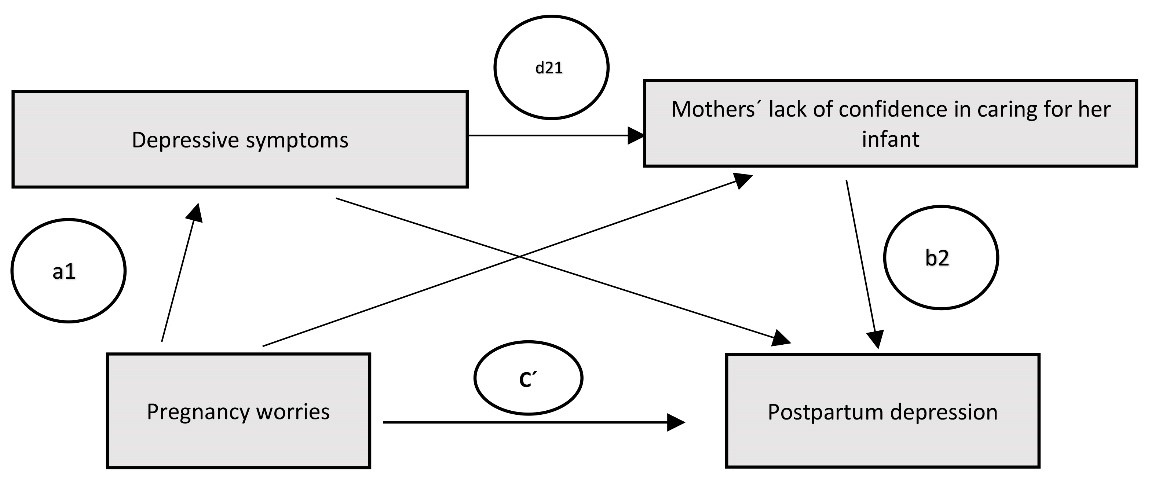 Fig. 2.
Fig. 2.
Hypothesized serial model of the interrelationships between pregnancy worries, depressive symptoms, a mothers’ confidence in caring for her infant and postpartum depression (dependent variable) a1-b2 (indirect effect of both mediators working in serial; d21 (effect of depressive symptoms on mothers’ lack of confidence); C´: direct effect.
Focusing on theoretical and methodological justification for both integrated mediation models, the integration of serial and parallel mediation models represents a sophisticated approach to understanding complex psychological mechanisms, offering a more comprehensive and nuanced analysis of variable interactions. To explain the rationale for this integrated mediation modeling, psychological phenomena rarely follow linear, single-pathway mechanisms. The integrated approach allows for the comprehensive exploration of multiple mediational pathways, simultaneous examination of direct and indirect effects, and capturing complex interrelationships between variables. The methodological advantages of serial mediation model characteristics are to examine sequential mediational processes, capturing cascading psychological mechanisms and tracing variable influences through multiple intermediary stages. In relation to parallel mediation model characteristics, they look for simultaneous mediational pathways, identifying competing or complementary mediational mechanisms, and provide a comprehensive viewpoint of variable interactions [40].
The mean of age of women included in this study was 31.28 (standard deviation (SD) = 3.96) years ranging between 23 and 42 years old. Descriptive data related to pregnancies planned, multiparous women, previous miscarriage, working status when women got pregnant, educational level, type of delivery, type of anesthesia and breastfeeding are presented in Table 1.
| Characteristics | n | % | Mean | SD | Max | Min | |
| Age (years) | 31.28 | 3.96 | 42 | 23 | |||
| Occupation | |||||||
| Employed | 81 | 67.5 | |||||
| Unemployed | 39 | 32.5 | |||||
| Educational level1 | |||||||
| Primary education (level 1) | 58 | 48.33 | |||||
| Upper secondary education (level 3) | 34 | 28.33 | |||||
| Bachelor’s or equivalent (level 6) | 28 | 23.33 | |||||
| Parity | |||||||
| Primiparous | 62 | 51.66 | |||||
| Multiparous | 58 | 48.33 | |||||
| Mode of birth | |||||||
| Vaginal | 73 | 60.83 | |||||
| Cesarean | 28 | 23.33 | |||||
| Instrumental | 19 | 15.83 | |||||
| Infant feeding pattern (postpartum) | |||||||
| Breastfeeding | 62 | 51.66 | |||||
| Bottle-feeding | 58 | 48.33 | |||||
1Information on education was organized according to The International Standard Classification of Education (ISCED, 2011) https://uis.unesco.org/en/topic/international-standard-classification-education-isced, accessed on 27 December 2024. SD, standard deviation; Max, maximum; Min, minimum.
The correlation analysis showed (Table 2) that pregnancy worries were positively
associated to depressive symptoms (p
| Mean (SD) | Median | Maximum | Minimum | 2 | 3 | 4 | |
| 1. Pregnancy worries (PW) (first trimester) | 1.91 (0.85) | 1.81 | 4.56 | 0 | 0.40** | 0.28** | 0.26** |
| 2. Depression symptoms (DS) (third trimester) | 0.76 (0.48) | 0.76 | 2.38 | 0 | 0.28** | 0.46** | |
| 3. Mother’s lack of confidence (MLC) (puerperium) | 14.73 (9.6) | 13 | 47 | 0 | 0.50** | ||
| 4. Postpartum depression (PPD) (puerperium) | 6.08 (4.86) | 5 | 22 | 0 |
** p
In relation to sociodemographic and clinical variables, age, planned pregnancy, previous pregnancies, previous abortions, type of delivery, birth weight and anesthesia were analyzed in relation to the variables of interest. Only age correlated negatively with mothers’ lack of confidence in caring for her infant (p = 0.008). Likewise, in relation to the characteristics of pregnancies, while pregnancy planning did not show significant associations with any variable under study, previous pregnancies did show significant differences on a mothers’ lack of confidence in caring for her infant and on pregnancy worries (Table 3). Finally, previous abortions, type of delivery, birth weight and anesthesia also showed no significant differences with any of the variables analyzed.
| Primiparous women (n = 62) | Multiparous women (n = 58) | M-W | Z | p | |
| Median (IQR) | Median (IQR) | ||||
| Mothers’ lack of confidence | 16 (10–24) | 10 (6–17) | 1074.00 | –3.237 | 0.001 |
| Pregnancy worries | 2.06 (1.37–2.71) | 1.68 (1.25–2.25) | 7915.00 | –2.958 | 0.003 |
IQR, interquartile range; M-W, Mann-Whitney U test.
Firstly, a parallel multiple model was tested (Fig. 1). This model included
PW as the independent variable, DS at
third trimester and mother’s lack of confidence in caring for her infant as
mediator variables, and PPD as the dependent variable, considering the previously
described covariates (age, previous pregnancies). The results showed that, the
predictive effect of pregnancy worries on depressive symptoms was significant (a1
= 0.29, t = 4.08, p
| Path | Effect | Boot LLCI | Boot ULCI | SE | t | p | R2 | F | p | |
| Predictive effect on depressive symptoms | ||||||||||
| Pregnancy worries | 0.29 | 0.1507 | 0.4346 | 0.0716 | 4.08 | p |
||||
| Predictive effect on mother’s lack of confidence | ||||||||||
| Depressive symptoms | 5.11 | 2.5521 | 7.6763 | 1.2928 | 3.95 | p |
||||
| Pregnancy worries | 1.67 | –0.3959 | 3.7525 | 1.0467 | 1.60 | p |
||||
| Previous pregnancies | –6.008 | –9.1141 | –2.9028 | 1.5671 | –3.83 | p |
||||
| Multiple and serial Mediation Modelsa of postpartum depression (PPD) | ||||||||||
| Total effect c | 1.6438 | 0.5318 | 2.7558 | 0.5612 | 2.9293 | 0.004 | 63% | F = 46.85 | p | |
| Direct effect (pregnancy worries) c´ | –0.2843 | –1.0509 | 0.4822 | 0.3868 | –0.7352 | 0.4638 | ||||
| a1 (depressive symptoms) | 5.0312 | 4.0345 | 6.0352 | 0.5047 | 9.9753 | |||||
| a2 (mothers’ lack of confidence) | 0.1432 | 0.0742 | 0.2123 | 0.0348 | 4.1132 | |||||
| Previous pregnancies | 0.7158 | –0.4922 | 1.9238 | 0.6095 | 1.1745 | 0.2428 | ||||
| Indirect effects: | ||||||||||
| Indirect effect 1 | 1.4733 | 0.7105 | 2.2309 | 0.3889 | ||||||
| Indirect effect 2 | 0.2404 | –0.0569 | 0.5826 | 0.1623 | ||||||
| *Indirect effect 3 | 0.2144 | 0.0595 | 0.4562 | 0.1025 | ||||||
| Contrast | ||||||||||
| c1 | 1.2329 | 0.4004 | 2.0903 | 0.4351 | ||||||
| c2 | 1.2590 | 0.5658 | 1.9826 | 0.3619 | ||||||
| c3 | 0.0260 | –0.4118 | 0.4314 | 0.4088 | ||||||
Notes: aModels include controls for age and previous pregnancies. a1, a2, = regression coefficients of X1, X2, respectively. *Indirect effect 3 corresponds to serial model results.
Abbreviations: Boot LLCI, bootstrapping lower limit confidence interval; Boot ULCI, bootstrapping upper limit confidence interval; SE, standard error. Model 6 from PROCESS.
Looking to test if there was a possible serial effect between variables, a
serial model was tested (Fig. 2). This model included PW as an independent
variable, DS as a first mediator, and mother’s lack of confidence in caring for
her infant as a second mediator (MLC). PPD was included as the dependent
variable. In this model, covariates (i.e., age, previous pregnancies) were also
added. As Table 4 shows, indirect effects of pregnancy worries on postpartum
depression via depressive symptoms on mothers’ lack of confidence in caring for
her infant (indirect effect 3) were significant (d21 (PW by MLC on PPD)
= 0.2144, [95% CI = 0.0595, 0.4562]. However, when contrast effects were
analyzed, results showed that the mediation effect of depressive symptoms at
third trimester between pregnancy worries and postpartum depression (indirect
effect 1) was higher than the mediated effect of a mothers’ lack of confidence in
caring for her infant (indirect effect 2), and showed also larger effects
compared to the serial mediation path, as indicated by bootstrap CI that were
entirely above zero for both contrast effects (contrast 1: indirect effect 1
In the current study our aim was to analyze whether depressive symptoms throughout pregnancy (third trimester) and a mothers’ lack of confidence in caring for her infant (4 months after delivery) have a mediating effect on the relationship between pregnancy worries (in early pregnancy; first trimester) and postpartum depression (four months after delivery). Based on the results presented, our first hypothesis has been confirmed: there seems to be a prospective effect of pregnancy worries on postpartum depression which is mediated by depressive symptoms experienced during pregnancy. This result is congruent with cross-sectional and longitudinal studies providing evidence of the effect of pregnancy worries on depressive symptoms [11, 12, 13, 41] that highlight the influence of depressive symptoms on postpartum depression [15]. According to recent studies, the incidence of depressive symptoms is particularly high during the second and third trimesters [42], our mediated effect of depressive symptoms in the third trimester (analysis that were not significant in the first trimester) implying a possible increase of symptoms over the course of the pregnancy [43]. Moreover, our result may be corroborated by studies that argued that progressive hormonal changes, particularly increased cortisol levels and altered neuroplasticity, contribute to heightened vulnerability to depressive symptoms in later trimesters [26]. Finally, related to postpartum depression, our results may also be congruent with the fact that more than three quarters of women with depressive symptoms during pregnancy tend to develop postpartum depression [44].
Related to our second hypothesis and based on studies that have shown that depressive symptoms have a negative impact on both mother and child [30, 31], the serial model tested showed that mothers’ lack of confidence has an indirect effect between worries and postpartum depression, influenced by depressive symptoms experienced during the third trimester. In concordance with our results, a recent study supports the fact that maternal self-confidence has an influence on PPD by suggesting that low maternal self-confidence creates a vulnerability mechanism where women perceive themselves as less capable of managing motherhood challenges, a fact that directly increases PPD risk [23]. Therefore, increased physical limitations and discomfort in later pregnancy stages correlate with higher depressive symptom scores, challenging women’s perceived competence and self-efficacy. According to the Cognitive Vulnerability Model [24], researchers have identified that diminished maternal self-confidence triggers negative cognitive schemas, characterized by increased self-doubt, heightened performance anxiety, and negative self-evaluation of maternal capabilities. These cognitive patterns significantly predict PPD symptoms, creating a psychological pathway from low self-confidence to depressive symptoms [24]. Along this line, pregnancy worries include the anticipation of childcare responsibilities that significantly increase psychological distress (particularly in the second and third trimesters) [28], a fact that is supported by neurobiological correlates emerging from neuroscientific research that indicate that low maternal self-confidence is associated with altered hypothalamic-pituitary-adrenal (HPA) axis functioning, increased cortisol reactivity, and reduced stress-coping mechanisms. These neurobiological markers suggest a complex interplay between psychological confidence and physiological stress responses, which are both contextual variables related to depressive symptoms as well [25].
Regarding the predictive capacity of worries in the early stages of pregnancy on postpartum depression, only two studies have examined whether initial pregnancy worries predicted psychological symptoms later in pregnancy [11, 45]. Although some studies have tracked the course of worries across the perinatal period [45], the interrelation of pregnancy worries and depression over time, more specifically in the third trimester, have been less analyzed [46, 47]. Our results can be considered relatively novel as they also incorporate the role of maternal lack of confidence in newborn care as a mediator for pregnancy worries and postpartum depression. However, when comparing both mediators, depressive symptoms have a greater impact that lack of confidence. According to our results and based on contradictory results found in previous studies about pregnancy worries and postnatal depression, the mediation role of lack of confidence on depressive symptoms could be due to the fact that pregnancy worries may influence postnatal depression via its interaction with contextual variables [48]. According to these results, researchers have highlighted that as the pregnancy progresses, women’s perception of their caregiving capabilities become more pronounced, directly influencing their psychological resilience and potential depressive symptoms [23]. Thus, our results may be key regarding preventive interventions on postpartum depression by focusing on training women to cope with worries, negative emotions, and perceptions about their capacity to care related to their new experience. Given the prospective nature of our study, we would like to highlight the importance of working with worries and depressive symptoms in pregnancy as a preventive intervention, but also the importance of working specifically with the mother’s perception of her ability to care for her baby as an essential factor in the development of postpartum depression. These results are congruent with studies that show that low efficacy regarding both birth and bonding, may be related to a generally underconfident thinking style and negative self-appraisal, which could be identified and addressed early in pregnancy [45].
Another result of interest is that, despite worries predicting postpartum depression, when the overall model is analyzed, worries do not have a direct effect on postpartum depression. It appears that worries do not directly influence postpartum depression, and it is, through depressive symptoms during pregnancy, and influenced by mothers’ perceived insecurity of care, how worries influence postpartum depression. These results are in line with a recent study that showed that worries were associated with maternal perception of impaired bonding, but not with observed mother-infant interactions, even after controlling for sociodemographic factors, concurrent depression, and the presence of anxiety disorders [14]. The possible reasons behind this result may be related to the fact that the concept of worries includes several components including fears relating to the infant as well as fears specifically around childbirth [49]. Thus, as Challacombe et al. [14] pointed out, the self-efficacy component of worries may be most strongly associated with lower reported bonding, but not with observed mother-infant interactions. Because mother-infant interaction quality was not affected in the study of Challacombe et al. [14], it could be hypothesized that the results found are due to low self-efficacy and would impact psychological adjustment during pregnancy and, specifically, would be higher in women with depressive symptoms during pregnancy. Target interventions during pregnancy focusing on treatment of both childbirth and bonding worries could help women adjust earlier. Moreover, considering our results, such interventions should also focus on the regulation of depressive emotional states, which, influenced by pregnancy worries, may have an impact on insecurity and on postpartum depression. In line with this, a recent study has suggested mindfulness interventions as an alternative to be considered in diminishing the effect of worries during pregnancy, improving affective dysregulation of the mother, and mother-baby attachment itself [50]. Research has shown that pregnant women who attended mindfulness training develop the ability to notice their worries, therefore being better able to tolerate and cope with them [51, 52, 53, 54].
Finally, regarding the covariates included in the study, previous literature has shown that most of the women who experience postpartum depression were primiparous (vs. multiparous) women [55]. In our results, its predictive value as a covariate is significant on mothers’ lack of confidence in caring for her infant but not on the total model. Likewise, in relation to age, our results show that the older the mother the less the insecurity. However, when this variable is introduced into the models, its role becomes non-significant.
Based on our results, we can conclude the importance of considering these variables as possible risk factors not only for postpartum depression [44, 56], but also for mothers’ security in caring for their babies. Over time, the mother will judge herself as a failed mother or a woman who cannot be a perfect mother [57]. Research has shown that the condition of a mother who is not able to answer the needs of her baby properly can cause stress to the baby, and postpartum depression can inhibit the growth and development of infants along with impacting the mother’s ability to understand the baby’s emotional expression [57, 58].
This study has some limitations that should be highlighted. First, the interpretation and extrapolation of the results must be linked to some limitations because the sample was taken from a single hospital and from women with low obstetric risk. Based on the literature reviewed where there is a higher percentage of depressive symptomatology in women with pregnancy complications, the fact that one of the inclusion criteria was low obstetric risk opens the opportunity to generalize our results (specifically in relation to postpartum depression) to a larger number of women. Moreover, the loss of participants in the different phases of the study could be another bias to the interpretation of the results. Thirdly, self-reported measures used to assess variables included may be subject to the usual bias found in these types of assessment tools. Nevertheless, demographic, and clinical variables associated with postpartum depression in pregnancy were considered, but the effects of other physical symptoms such as anxiety related to postpartum depression should also be controlled. Fourthly, we have confirmed the importance of depressive symptoms as significant mediators between pregnancy worries in the prenatal stage and their implication in bonding in the postnatal stage, however, within a broader family context, it would be interesting to consider other variables, such as the role of the father figure in the bond [59], that may influence the possibility of developing an adequate bond with the baby [60]. The father’s role emerges as a critical psychological mediator in maternal mental health and perceived childcare competence, extending far beyond traditional conceptualizations of parental support. The contemporary understanding transcends traditional support conceptualizations, positioning fathers as active, transformative agents in maternal psychological adaptation. For example, researchers have shown that paternal emotional responsiveness significantly modulates maternal self-perception by enhancing maternal resilience, increasing perception of caregiving competence, and reducing vulnerability to postpartum depressive symptoms [59, 60]. Moreover, practical co-parenting engagement impacts maternal psychological adaptation by sharing responsibilities that also reinforces maternal self-efficacy [61]. The fathers’ role should be integrated into future studies as a contextual role trying to understand how it impacts maternal self-efficacy.
The apparent contradiction in the research finding—where worries predict postpartum depression at an individual level but not at a global model level—can be explained through several nuanced psychological and methodological perspectives. First, the lack of direct effects in the global model suggests that worries operate through intermediary psychological processes rather than having a straightforward, linear relationship with postpartum depression. Potential mediating factors might include worries that may activate underlying cognitive schemas and negative thought patterns that indirectly contribute to depressive symptoms. These mechanisms might be more pronounced at an individual level but become diluted when examining broader population dynamics. Furthermore, individual differences in coping mechanisms, social support, and personal resilience can modulate how worries translate into depressive symptoms. This heterogeneity could explain why a direct relationship disappears in aggregate models. Moreover, related to methodological considerations, in complex psychological models, some variables can suppress or mask the direct effects of other variables when additional factors are introduced. Worries might have a statistically suppressed effect when controlling for other psychological and environmental variables.
Future studies should consider these variables to gain in-depth knowledge of all the factors that may influence the mother-baby bond. As we know, psychological phenomena rarely follow simple linear patterns. The global model might reveal more complex, non-linear interactions that obscure the direct relationship visible at the individual level. The research reveals that the relationship of worries with postpartum depression is intricate and context-dependent. While predictive at an individual level, these effects become more complex when examined through broader statistical lenses, reflecting the sophisticated nature of psychological processes.
This study provides critical insights into the complex psychological landscape of maternal mental health, offering valuable perspectives on PPD prevention strategies. Specifically, our results have shown that there seems to be a prospective effect of pregnancy worries on postpartum depression which is mediated by depressive symptoms experienced during pregnancy, and that mothers’ lack of confidence has an indirect effect between worries and postpartum depression, influenced by depressive symptoms experienced during the third trimester.
Focusing on clinical contributions, the identification of depressive symptoms (at third trimester) and mothers’ lack of confidence as mediational variables offer unprecedented insights into the complex interactions between psychological variables during the perinatal period. By identifying key psychological mechanisms and risk factors as depressive symptoms and lack of confidence healthcare professionals can implement more precise and effective screening and support strategies.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request
CE participated in conceptualization, data curation, investigation, methodology, resources writing—original draft, supervision and validation. PC and LG participated in conceptualization, methodology, resources, data curation; writing—original draft preparation. CPP participated in conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, writing review and editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All procedures involving human participants in this study were conducted in strict adherence to the ethical guidelines established by the 1964 Helsinki Declaration and its subsequent amendments. The research protocol underwent comprehensive ethical review and received formal approval from Fuenlabrada University Hospital Ethics Committee (approval reference: CPMP/ICH/135/95). These approvals ensure that the study met rigorous ethical standards for human subject research, protecting the rights, safety, and well-being of all participants throughout the investigation. All women signed a consent form to declare a voluntary agreement with all procedures implicated in this project.
The authors gratefully acknowledge all the participants for their collaboration and enthusiasm. We thank Dr. Dolores Marín Morales for her invaluable collaboration in the initiation of this research.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.