






 , Jiayin Wu 3,4,†, Shujiao Lin 1,2, Hongli Liu 2,5, Yanqiu Zhong 1,2, Maoqi Wu 1,2, Xiaohong Zhong 1,2,*
, Jiayin Wu 3,4,†, Shujiao Lin 1,2, Hongli Liu 2,5, Yanqiu Zhong 1,2, Maoqi Wu 1,2, Xiaohong Zhong 1,2,*1 Department of Ultrasound, Women and Children’s Hospital, School of Medicine, Xiamen University, 361102 Xiamen, Fujian, China
2 Department of Obstetrics and Gynecology, Women and Children’s Hospital, School of Medicine, Xiamen University, 361102 Xiamen, Fujian, China
3 Department of Laboratory Medicine, Women and Children’s Hospital, School of Medicine, Xiamen University, 361102 Xiamen, Fujian, China
4 Fujian Key Clinical Specialty of Laboratory Medicine, Women and Children’s Hospital, School of Medicine, Xiamen University, 361102 Xiamen, Fujian, China
5 Department of Gynecology, Women and Children’s Hospital, School of Medicine, Xiamen University, 361102 Xiamen, Fujian, China
†These authors contributed equally.
Abstract
Endometriosis affects an estimated 10% of women of reproductive age and is characterized by chronic pelvic pain, infertility, and an increased risk of ovarian cancer. Laparoscopy remains the diagnostic gold standard for endometriosis; however, this technique is an invasive procedure. Therefore, non-invasive alternatives, such as serum biomarkers (e.g., carbohydrate antigen 125 (CA125), carbohydrate antigen 199 (CA199), and human epididymis protein 4 (HE4)) and ultrasound, represent promising techniques but currently lack consistent accuracy. Thus, this study aimed to evaluate the diagnostic efficacy of CA125, HE4, and ultrasound, individually and in combination, for detecting endometriosis.
A retrospective analysis was conducted involving 51 patients with endometriosis and 52 healthy controls. Serum levels of CA125 and HE4 were measured by chemiluminescence, and ultrasound examinations were performed. Diagnostic performance was evaluated using sensitivity, specificity, accuracy, and receiver operating characteristic (ROC) curves.
CA125 levels were significantly elevated in patients with endometriosis (1.90 ± 0.39, log10) compared to controls (1.06 ± 0.22, log10; p < 0.001), yielding an area under the curve (AUC) of 0.97 (95% confidence interval (CI): 0.94–1.00), with a sensitivity of 94.23% (95% CI: 0.87–1.01), specificity of 92.16% (95% CI: 0.85–1.00), positive predictive value (PPV) of 92.18% (95% CI: 0.85–1.00), negative predictive value (NPV) of 94.21% (95% CI: 0.87–1.01), and accuracy of 93.20% (95% CI: 0.88–0.98). In contrast, HE4 did not exhibit a significant difference (p = 0.156). Ultrasound demonstrated a sensitivity of 72.55% (95% CI: 0.60–0.85), a specificity of 100.00% (95% CI: 1.00–1.00), PPV of 100.00% (95% CI: 1.00–1.00), NPV of 78.79% (95% CI: 0.69–0.89), and an accuracy of 86.41% (95% CI: 0.80–0.93). Combining CA125 and ultrasound enhanced the diagnostic accuracy to 95.15% (95% CI: 0.91–1.00), achieving a sensitivity of 92.16% (95% CI: 0.85–1.00), PPV of 97.92% (95% CI: 0.94–1.02), NPV of 92.73% (95% CI: 0.86–1.00), and specificity of 98.08% (95% CI: 0.94–1.01) (AUC: 0.96, 95% CI: 0.92–1.00).
Combining CA125 and ultrasound significantly improves the non-invasive diagnosis of endometriosis, providing high sensitivity and specificity. This approach may reduce the reliance on laparoscopy, thereby facilitating earlier intervention. However, as this is a small-scale retrospective cohort study, larger sample cohorts are required for future validation to confirm these findings.
Keywords
- biomarkers
- CA125
- diagnostic
- endometriosis
- HE4
- ultrasound
Endometriosis is a prevalent gynecological disorder characterized by the ectopic implantation of functional endometrial tissue outside the uterine cavity, predominantly in the ovaries, pelvic peritoneum, and rectovaginal septum [1]. Under hormonal influence, these ectopic lesions undergo cyclic bleeding, eliciting chronic inflammatory responses, fibrosis, and adhesion formation, which lead to clinical symptoms such as chronic pelvic pain, dysmenorrhea, dyspareunia, and infertility [2, 3]. Globally, endometriosis affects approximately 10% of reproductive-aged women [4], with its prevalence rising to 30%–50% among infertile women. Endometriosis not only severely impacts the quality of life of patients but also increases the risk of ovarian cancer [5]. The chronic pain and infertility associated with this condition impose significant economic and psychological burdens on families and society [6]. Therefore, early diagnosis and intervention are crucial for delaying disease progression, improving reproductive outcomes, and reducing the risk of malignant transformation.
Currently, laparoscopy combined with pathological biopsy is considered the gold standard for diagnosing endometriosis, enabling direct visualization of lesions and staging [7]. However, this technique is invasive, costly, requires general anesthesia, and carries the risk of surgical complications, which makes it difficult to promote it as a screening method. In recent years, serum biomarker testing and imaging techniques have garnered widespread attention due to their convenience. Carbohydrate antigen 125 (CA125) is one of the earliest studied markers, with elevated levels associated with pelvic inflammation and peritoneal irritation [8]. Multiple studies have reported that the sensitivity of CA125 for diagnosing endometriosis ranges from 24% to 94%, while its specificity ranges from 83% to 93% [9, 10]. However, CA125 is susceptible to interference from the menstrual cycle, ovarian cysts, and other gynecological conditions [11]. A decrease in hemoglobin (HGB) is commonly observed in patients with endometriosis who experience excessive menstrual bleeding or the deep infiltrating type [12], but this marker lacks specificity. Carbohydrate antigen 199 (CA199) may be elevated in some endometriosis patients [13], but its sensitivity is low. Human epididymis protein 4 (HE4) is a novel biomarker; in recent years, HE4 has been introduced into endometriosis research as an ovarian cancer marker [14], with the advantage of being unaffected by the menstrual cycle [15]. Studies have shown that HE4 is significantly elevated in endometriosis patients, with a sensitivity of about 66% [16, 17], but its diagnostic efficacy is limited when used alone. In imaging techniques, transvaginal ultrasound (TVUS) demonstrates a high diagnostic value for ovarian endometriosis, particularly for chocolate cysts [18], with a sensitivity ranging from 70% to 92% [19, 20]. However, its sensitivity for superficial endometriosis is relatively low, and this sensitivity is highly dependent on the operator’s experience, which may introduce diagnostic bias. Previous studies have indicated that the combination of multiple markers can enhance diagnostic accuracy. For instance, the AUC for endometriosis diagnosis can reach 0.90 when CA125 is combined with HE4, HGB, and CA199 [16], although this still requires validation with larger sample sizes.
In this study, we conducted a retrospective analysis of serum tumor marker levels and ultrasound findings in both patients with endometriosis and healthy controls. The diagnostic performance of CA125, HE4, ultrasound, and their combinations was assessed to identify an optimal combined indicator for the detection of endometriosis.
Between July 2021 and July 2024, 51 patients with endometriosis who received
treatment at Xiamen Maternal and Child Health Care Hospital were selected for the
observation group. The ages of the patients ranged from 26 to 54 years, with all
cases confirmed by histopathological examination. Inclusion criteria required
that patients who had laparoscopic surgery and were pathologically confirmed to
have endometriosis. Exclusion criteria comprised patients with missing clinical
data, those with hormone-dependent diseases (such as adenomyosis and uterine
fibroids), individuals taking any hormonal medications, those with a history of
pregnancy within the past six months, patients with other endocrine, immune, or
metabolic diseases, and those with severe liver and kidney dysfunction,
hematological disorders, or malignant tumors (Fig. 1). Furthermore, 52 healthy
women who underwent physical examinations at the same hospital during the same
period were selected as the control group (Fig. 1), aged between 25 and 60 years.
There was no statistically significant difference in age between the two groups
(p
 Fig. 1.
Fig. 1.
Flowchart of study population inclusion and exclusion criteria. n, number of samples.
For serum tumor marker testing, 4 mL of peripheral venous blood was drawn from patients in the observation group preoperatively during non-menstrual periods and under fasting conditions in the morning. Similarly, the control group had 4 mL of peripheral venous blood drawn on the morning of the physical examination, also while fasting. After standing at room temperature for 30 minutes, the samples were centrifuged at 3000 rpm for 10 minutes. The serum was collected and stored in sterile EP tubes, which were then stored at –80 °C until testing. The serum (20153401967, Innovax, Xiamen, Fujian, China) and HE4 (20163400698, Innovax, Xiamen, Fujian, China) expression levels of both groups were measured using a chemiluminescence analyzer (I2000, Abbott, Lake Forest, IL, USA), with all testing procedures strictly adhering to the kit instructions.
The ultrasound examination was performed by multiple operators using the Philips (IU22, Amsterdam, NH, Netherlands), Aloka (ProSound Alpha 5, Hitachi Aloka, Tokyo, Japan) and GE (Voluson E8, Boston, MA, USA) color Doppler ultrasound diagnostic system, with meticulous observation of the patient’s pelvic area, including the uterine and ovarian spaces. Key aspects assessed include the thickness of the endometrium, uterine size, internal echo, and the position of the uterus. Additionally, detailed observations and recordings were made regarding the lesion’s location, marginal morphology, diameter, and whether a capsule was present. The blood flow signal distribution in the targeted lesion was also examined. The diagnosis of endometriosis at various sites was made using established clinical diagnostic criteria.
This study aims to evaluate the positive outcomes associated with endometriosis diagnosed through ultrasound using statistical methods. We compared and analyzed the serum levels of CA125 and HE4 between two groups of subjects. Additionally, we considered the histopathological examination results from surgery as the gold standard for diagnosing endometriosis. The diagnostic efficacy of ultrasound, CA125, and HE4 was statistically analyzed and compared both individually and in combination. Specificity was defined as the proportion of true negative cases to the sum of true negative and false positive cases, expressed as a percentage. Sensitivity was calculated as the ratio of true positive cases to the sum of true positive and false negative cases, also expressed as a percentage. Accuracy was calculated by dividing the sum of true positive and true negative cases by the total number of cases, then multiplying by 100%.
The sample size requirement was determined using PASS (version 2021, NCSS,
Kaysville, UT, USA), specify the test direction, report power = 90%, anticipated
AUC of 0.9, null AUC of 0.7, allocation ratio was set at 1:1, the lower limit of
the false positive rate was 0.0, and the upper limit of the false positive rate
was 1.0, resulting in a need for a minimum of 24 patients with endometriosis and
24 healthy controls. Ultimately, the study included a total of 51 patients with
endometriosis and 52 controls. All statistical analyses were conducted using SPSS
27.0 software (IBM Corp., Armonk, NY, USA). The Shapiro-Wilk test was employed to
analyze the type of data distribution, and the parameters distributed with normal
distribution were explained as Mean
A total of 51 patients with histologically and pathologically confirmed
endometriosis and 52 age-matched controls were enrolled for analysis. Comparative
analysis of baseline characteristics demonstrated that the mean age of the
endometriosis group was slightly higher than that of the control group (38.20
| Parameters | Control group (n = 52) | Endometriosis group (n = 51) | Differential analysis |
| Age (years, mean |
35.60 |
38.20 |
t = 1.75, p = 0.080 |
| Menopause | 11.54% | 1.96% | Z = 2.14, p |
| Dysmenorrhea | 7.69% | 76.47% | Z = 18.43, p |
| CA125 (log10, mean |
1.06 |
1.90 |
t = 1.85, p |
| HE4 (log10, mean |
1.67 |
1.62 |
t = 13.79, p = 0.070 |
SD, standard deviation; CA125, cancer antigen 125; HE4, human epididymis protein 4.
Analysis of endometriotic lesion distribution revealed that the most common isolated lesion type was ovarian endometriosis (25 cases, 49.02%), followed by ovarian combined with pelvic endometriosis (11 cases, 21.57%). Other isolated lesion types included pelvic endometriosis (2 cases, 3.92%), abdominal wall endometriosis (1 case, 1.96%), and fallopian tube endometriosis (1 case, 1.96%). Additionally, several multifocal lesion combinations were observed: ovarian with fallopian tube involvement (2 cases, 3.92%), ovarian with uterosacral ligament involvement (1 case, 1.96%), and ovarian with rectal involvement (1 case, 1.96%). Furthermore, seven cases (13.72%) exhibited triple-site involvement, including combinations of ovarian-cervical-pelvic, ovarian-vaginal wall-pelvic, ovarian-fallopian tube-pelvic, ovarian-fallopian tube-vaginal wall, ovarian-rectal-abdominal wall, ovarian-rectal-vaginal, and ovarian-pelvic-intestinal endometriosis (Table 2).
| Lesion sites | Cases | Proportion (%) |
| Ovary | 25 | 49.02% |
| Ovary and pelvic cavity | 11 | 21.57% |
| Ovary and fallopian tube | 2 | 3.92% |
| Pelvic cavity | 2 | 3.92% |
| Abdominal wall | 1 | 1.96% |
| Fallopian tube | 1 | 1.96% |
| Ovary and intrinsic ligament | 1 | 1.96% |
| Ovary and rectum | 1 | 1.96% |
| Ovary, cervix, and pelvic cavity | 1 | 1.96% |
| Ovary, pelvic cavity, and vaginal wall | 1 | 1.96% |
| Ovary, fallopian tube, and pelvic cavity | 1 | 1.96% |
| Ovary, fallopian tube, and vaginal wall | 1 | 1.96% |
| Ovary, rectum, and abdominal wall | 1 | 1.96% |
| Ovary, rectum, and vagina | 1 | 1.96% |
| Ovary, pelvic cavity, and intestine | 1 | 1.96% |
We analyzed the serum tumor marker expression levels between the endometriosis
group and the control group. The results showed that the CA125 expression level
in the endometriosis group (1.90
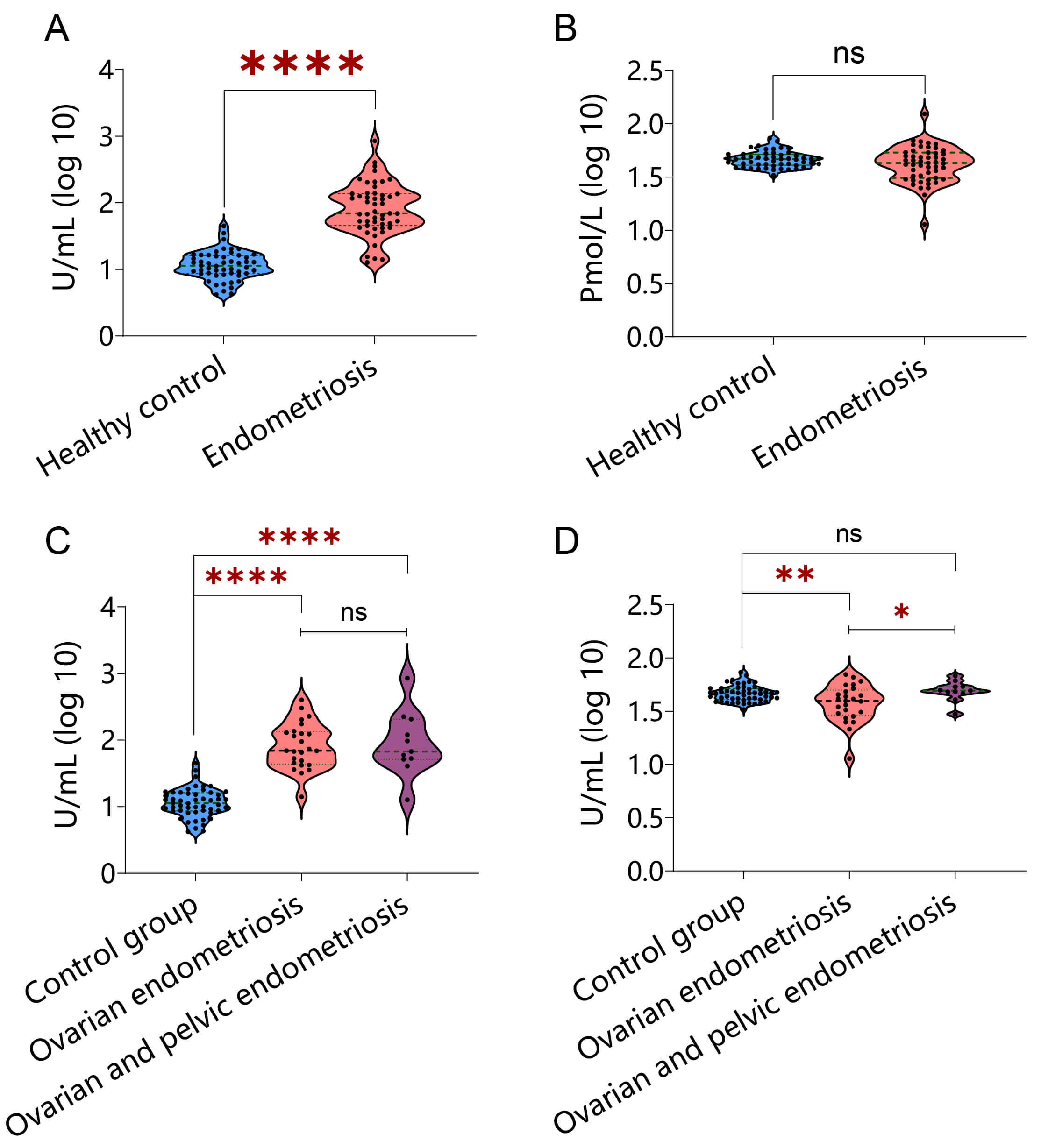 Fig. 2.
Fig. 2.
Comparative analysis of serum tumor marker levels
between endometriosis patients and healthy controls. (A) Carbohydrate antigen
125 (CA125) levels in controls versus endometriosis patients. (B) HE4 levels in
controls versus endometriosis patients. (C) CA125 levels across study groups:
controls, isolated ovarian endometriosis, and ovarian endometriosis with pelvic
involvement. (D) HE4 levels across study groups: controls, isolated ovarian
endometriosis, and ovarian endometriosis with pelvic involvement. * represents
p
| Serum tumor marker | Group (number) | Quantitative level (log10, mean |
p-value | |||
| CA125 | Healthy people (n = 52) (1) | 1.06 |
1 vs. 2: t = 1.85, p |
1 vs. 3: t = 13.36, p |
1 vs. 4: t = 9.75, p |
3 vs. 4: t = 0.27, p = 0.7900 |
| Endometriosis (n = 51) (2) | 1.90 | |||||
| Ovarian endometriosis (n = 25) (3) | 1.91 | |||||
| Ovarian and pelvic endometriosis (n = 11) (4) | 1.95 | |||||
| HE4 | Healthy (n = 52) (1) | 1.67 |
1 vs. 2: t = 13.79, p = 0.0700 | 1 vs. 3: t = 3.22, p = 0.0019** | 1 vs. 4: t = 0.94, p = 0.3500 | 3 vs. 4: t = 2.05, p = 0.0480* |
| Endometriosis (n = 51) (2) | 1.62 | |||||
| Ovarian endometriosis (n = 25) (3) | 1.57 | |||||
| Ovarian and pelvic endometriosis (n = 11) (4) | 1.69 | |||||
* represents p
To further elucidate the characteristics of endometriosis based on different sites of disease onset, this study classified patients according to their disease location and focused on comparing the levels of CA125 and HE4 in the two most common subtypes—ovarian endometriosis and ovarian endometriosis combined with pelvic endometriosis—with those of the control group. The results showed that the CA125 levels in the control group were statistically different from those in both the ovarian endometriosis group and the ovarian endometriosis combined with pelvic endometriosis group. However, there was no statistically significant difference in CA125 levels between the ovarian endometriosis group and the ovarian endometriosis combined with pelvic endometriosis group (Fig. 2C, Table 3). Additionally, the HE4 levels in the control group were statistically different from those in the ovarian endometriosis group, but not from those in the ovarian endometriosis combined with pelvic endometriosis group. Notably, there was a statistically significant difference in HE4 levels between the ovarian endometriosis group and the ovarian endometriosis combined with pelvic endometriosis group (Fig. 2D, Table 3).
We further analyzed the individual diagnostic efficacy of CA125 and HE4 serum
markers in the diagnosis of endometriosis. To this end, we used a healthy control
group as a reference and drew ROC curves to evaluate the diagnostic accuracy of
these two markers. The results showed that the AUC value of the CA125 diagnostic
model was 0.97 (p
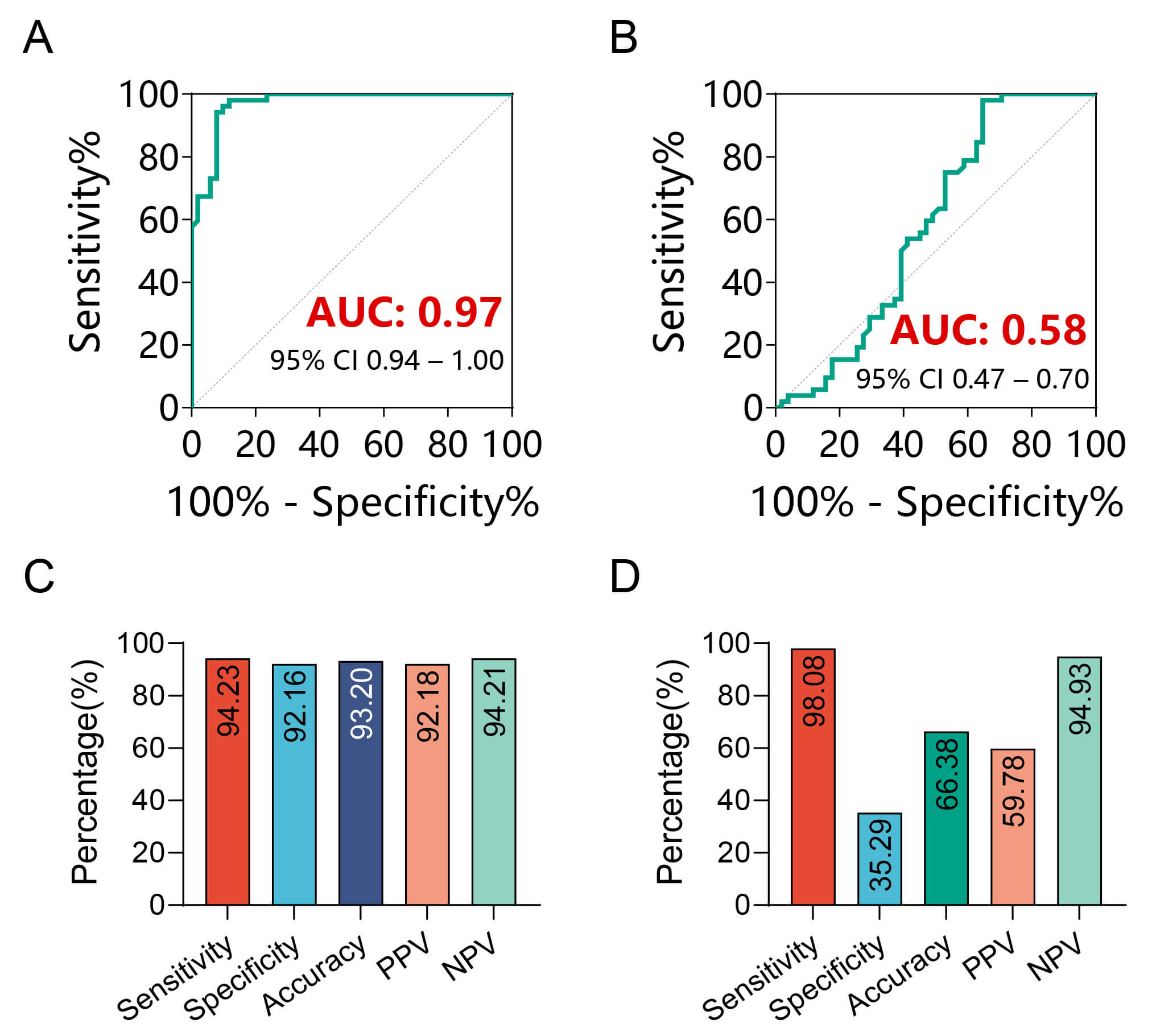 Fig. 3.
Fig. 3.
Analysis of the diagnostic value of CA125 and HE4 for endometriosis. (A) ROC curve analysis of the diagnostic performance of CA125 for endometriosis. (B) ROC curve analysis of the diagnostic performance of HE4 for endometriosis. (C) Sensitivity, specificity, and accuracy of diagnosing endometriosis through CA125. (D) Sensitivity, specificity, and accuracy of diagnosing endometriosis through HE4. AUC, area under the curve; 95% CI, 95% confidence interval; PPV, positive predictive value; NPV, negative predictive value; ROC, receiver operating characteristic.
| Serum tumor marker | Indicator | Result (95% CI) |
| CA125 | AUC | 0.97 (0.94–1.00) |
| Sensitivity | 94.23% (0.87–1.01) | |
| Specificity | 92.16% (0.85–1.00) | |
| Accuracy | 93.20% (0.88–0.98) | |
| PPV | 92.18% (0.85–1.00) | |
| NPV | 94.21% (0.87–1.01) | |
| HE4 | AUC | 0.58 (0.47–0.70) |
| Sensitivity | 98.08% (0.94–1.02) | |
| Specificity | 35.29% (0.21–0.48) | |
| Accuracy | 66.38% (0.57–0.75) | |
| PPV | 59.78% (0.49–0.70) | |
| NPV | 94.93% (0.84–1.06) |
Furthermore, through the maximum Youden index, we calculated the sensitivity, specificity, and accuracy of CA125 and HE4 in the diagnosis of endometriosis. CA125 had a sensitivity of 94.23% (95% CI: 0.87–1.01), specificity of 92.16% (95% CI: 0.85–1.00), accuracy of 93.20% (95% CI: 0.88–0.98), positive predictive value (PPV) of 92.18% (95% CI: 0.85–1.00), and negative predictive value (NPV) of 94.21% (95% CI: 0.87–1.01) (Fig. 3C, Table 4). This means that CA125 can effectively identify the vast majority of actual patients and accurately exclude non-patients, with high overall diagnostic accuracy. HE4 had a sensitivity of 98.08% (95% CI: 0.94–1.02), specificity of 35.29% (95% CI: 0.21–0.48), accuracy of 66.38% (95% CI: 0.57–0.75), PPV of 59.78% (95% CI: 0.49–0.70), and NPV of 94.93% (95% CI: 0.84–1.06) (Fig. 3D, Table 4). Although HE4 has high sensitivity, meaning that it can detect most actual patients, its low specificity indicates that there may be more false-positive results, i.e., misdiagnosing some non-patients as patients. This could lead to unnecessary further examinations and treatments. Therefore, based on the AUC values and various diagnostic indicators, CA125 performs better than HE4 in the diagnosis of endometriosis.
We used pathological diagnosis as the gold standard to evaluate the diagnostic value of ultrasound in endometriosis. A total of 51 patients diagnosed with endometriosis and 52 controls were included in the study. Ultrasound examination results showed that among the 51 patients, 14 were missed (ultrasound did not detect the disease), while in the 52 controls, ultrasound did not detect any abnormalities.
To explore the diagnostic value of ultrasound in endometriosis, we used the
Chi-Square test to analyze the association between ultrasound results and disease
status. The results showed that ultrasound could significantly distinguish
patients with endometriosis from controls (Chi-Square test;
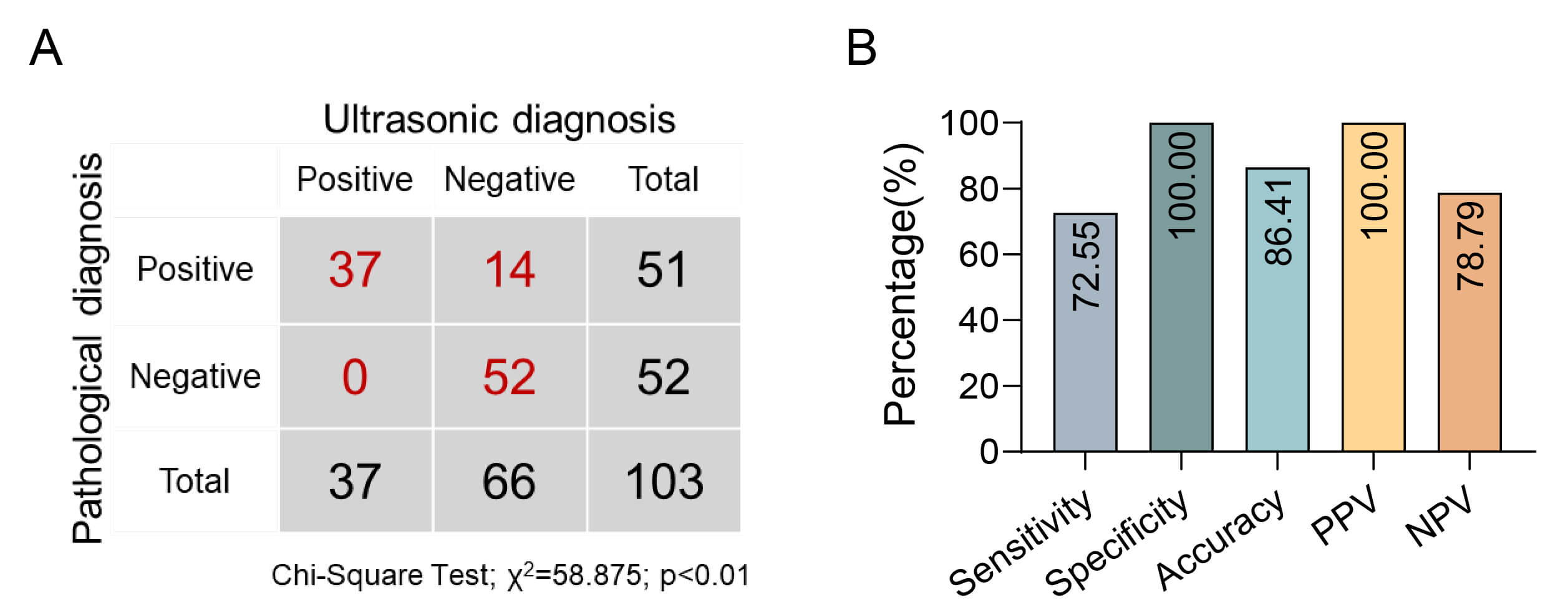 Fig. 4.
Fig. 4.
Analysis of the diagnostic value of ultrasound for endometriosis. (A) Pearson’s Chi-Square test analysis of whether ultrasound can differentiate between patients with endometriosis and controls. (B) Sensitivity, specificity, and accuracy of ultrasound in diagnosing endometriosis.
Furthermore, through the maximum Youden index, we calculated the sensitivity, specificity, accuracy, PPV, and NPV of ultrasound detection to be 72.55% (95% CI: 0.60–0.85), 100.00% (95% CI: 1.00–1.00), 86.41% (95% CI: 0.80–0.93), 100.00% (95% CI: 1.00–1.00), and 78.79% (95% CI: 0.69–0.89), respectively (Fig. 4B, Table 5). These metrics indicate that ultrasound detection has high specificity and accuracy in the diagnosis of endometriosis, although the sensitivity is slightly lower, meaning that a certain proportion of patients may be missed. However, the 100% specificity means that ultrasound can very reliably exclude those without the disease, which helps reduce unnecessary further examinations. In conclusion, ultrasound detection has important clinical value in the diagnosis of endometriosis.
| Detection method | Indicator | Result (95% CI) |
| Ultrasound | Sensitivity | 72.55% (0.60–0.85) |
| Specificity | 100.00% (1.00–1.00) | |
| Accuracy | 86.41% (0.80–0.93) | |
| PPV | 100.00% (1.00–1.00) | |
| NPV | 78.79% (0.69–0.89) |
Previous studies have shown that serum tumor marker CA125 and ultrasound imaging have certain diagnostic value in the diagnosis of endometriosis. However, the diagnostic accuracy of these single-detection methods still requires improvement. Therefore, this part of the study aims to explore whether the combination of CA125 and ultrasound detection can improve the diagnostic accuracy.
To achieve this goal, we used logistic regression model to combine the numerical values of CA125 and ultrasound detection results to establish a combined diagnostic model and evaluated its diagnostic performance by drawing ROC curves (Fig. 5A, Table 6). The results showed that the AUC of the ROC curve for the combined diagnostic model was 0.96 (95% CI: 0.92–1.00), indicating that it has high accuracy in distinguishing patients with endometriosis from non-patients. Further analysis through the maximum Youden index showed that the sensitivity, specificity, accuracy, PPV, and NPV of the combined diagnostic model were 92.16% (95% CI: 0.85–1.00), 98.08% (95% CI: 0.94–1.01), 95.15% (95% CI: 0.91–1.00), 97.92% (95% CI: 0.94–1.02), and 92.73% (95% CI: 0.86–1.00), respectively. These metrics indicate that the model can not only effectively identify true patients (high sensitivity) but also accurately exclude non-patients (high specificity), with high overall diagnostic accuracy.
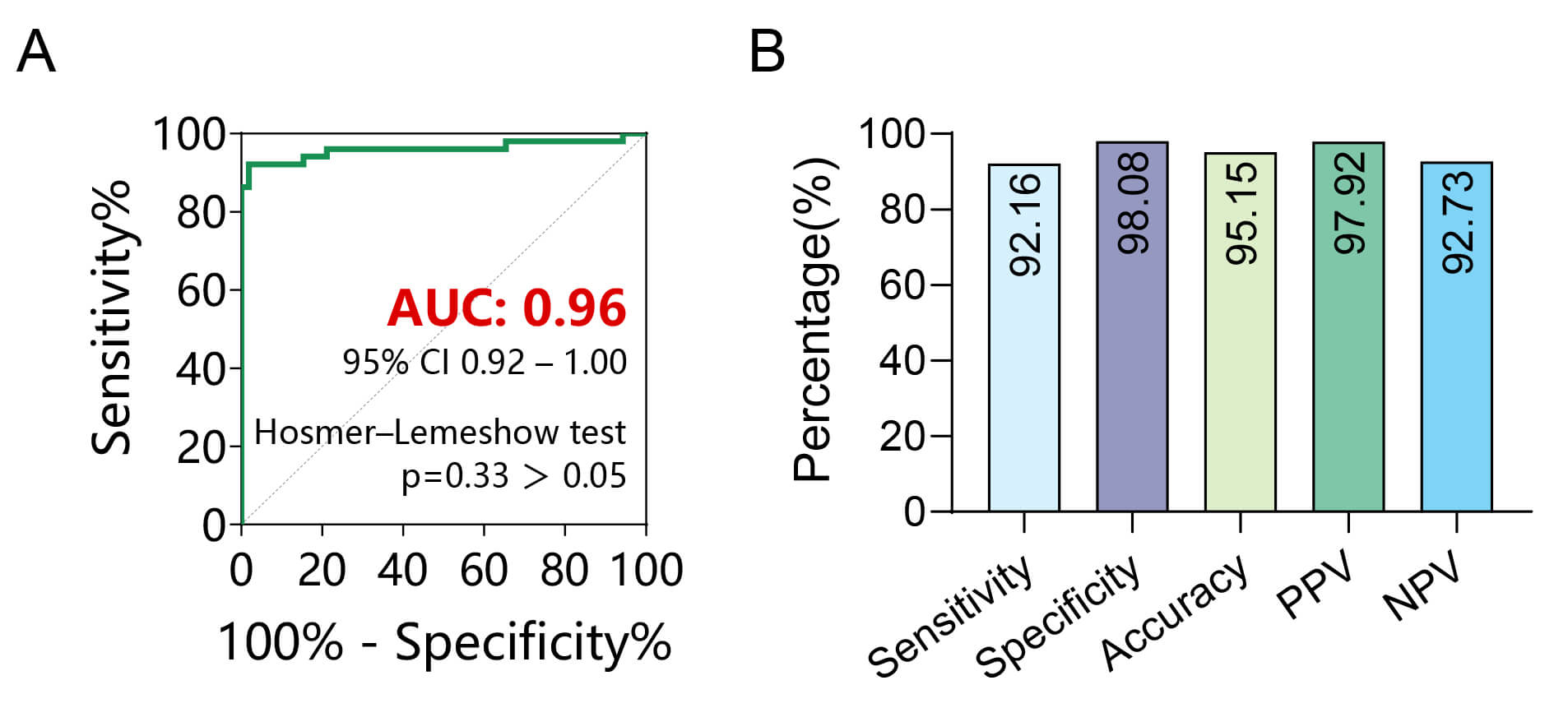 Fig. 5.
Fig. 5.
Analysis of the diagnostic value of combined CA125 and ultrasound for endometriosis. (A) ROC curve analysis of the diagnostic performance of combined CA125 and ultrasound for endometriosis. (B) Sensitivity, specificity, and accuracy of combined CA125 and ultrasound in diagnosing endometriosis.
| Combined detection | Indicator | Result (95% CI) |
| CA125 and ultrasound | AUC | 0.96 (0.92–1.00) |
| Sensitivity | 92.16% (0.85–1.00) | |
| Specificity | 98.08% (0.94–1.01) | |
| Accuracy | 95.15% (0.91–1.00) | |
| PPV | 97.92% (0.94–1.02) | |
| NPV | 92.73% (0.86–1.00) |
Notably, compared with the single use of CA125 or ultrasound detection, the accuracy of the combined diagnostic model increased by 2.05% and 8.84%, respectively (Fig. 5B, Table 6). These results indicate that the combined application of CA125 and ultrasound detection outperforms single detection methods in the diagnosis of endometriosis. This may provide an effective approach for earlier and more accurate diagnosis of endometriosis in clinical practice.
Endometriosis is an estrogen-dependent chronic inflammatory disease characterized by the ectopic implantation of endometrial stromal cells outside the uterine cavity [21]. This condition affects approximately 10% of women of reproductive age and manifests as severe pelvic pain, dysmenorrhea, and infertility, which significantly impairing quality of life [2, 3, 22]. Additionally, endometriosis is linked to the formation of adhesions and potential ovarian malignancies, highlighting its long-term health risks and contributing to a substantial socioeconomic burden due to delayed diagnosis and repeated interventions [5, 6]. Traditional diagnostic methods for endometriosis have significant limitations. Currently, the gold standard for diagnosis is laparoscopic examination combined with histopathological confirmation [7]. However, this invasive procedure, poses a risk of surgical complications and is expensive, limiting its practicality for early screening. Non-invasive imaging techniques, such as TVUS and magnetic resonance imaging (MRI), exhibit limited sensitivity in detecting early-stage diseases [23]. Meanwhile, serum biomarkers like CA199 lack specificity, as their elevated levels are frequently observed in other gynecological conditions, leading to diagnostic ambiguity. Therefore, identifying reliable diagnostic indicators is crucial to bridging these clinical gaps. A combination of biomarkers with high sensitivity and specificity can enable timely diagnosis, reduce reliance on surgical confirmation, and facilitate the implementation of personalized treatment strategies.
In this study, we performed a retrospective analysis of serum inflammatory markers (including CA125, HE4) and ultrasound indicators in patients with endometriosis. We aimed to evaluate the differences between patients with endometriosis and healthy controls, as well as to assess the diagnostic efficacy of these markers to identify an optimal combined diagnostic indicator for precise diagnosis of endometriosis.
Based on the theory that immune system dysfunction plays a role in the pathogenesis of endometriosis [24], immune molecules and inflammatory cytokines have been extensively studied as potential biomarkers for this condition [25]. However, most results remain controversial. Despite the conflicting evidence regarding the efficacy of CA125 as a biomarker for endometriosis, meta-analyses indicate that CA125 remains one of the most used markers for this condition [10]. Our study found that CA125 levels in patients with endometriosis are higher than those in healthy individuals. This increase is associated with the inflammatory response and fibrotic processes, where ectopic endometrial tissue induces chronic localized inflammation, leading to increased production and release of CA125 [26]. Additionally, angiogenesis and cellular proliferation in ectopic lesions may also promote the expression of CA125, resulting in a significant increase in its concentration in the blood. HE4 has been reported to be associated with endometriosis, suggesting it’s a hematological marker for diagnosing [14]. In this study, we explored the diagnostic potential of HE4; however, we found no statistically significant difference in HE4 levels between patients with endometriosis and healthy individuals. This lack of significance may be attributed to variations in sample population used in the study as well as the relatively small sample size. Therefore, additional research involving a larger sample size is necessary to assess the diagnostic efficiency of the HE4 as a biomarker for endometriosis.
Ultrasound, due to its high resolution, real-time imaging capability, and non-invasive nature, offers substantial advantages in the diagnosis of endometriosis, particularly in identifying ovarian endometriosis [18, 19, 20, 27]. In this study, the sensitivity of ultrasound for diagnosing endometriosis was found to be 72.55%, with a specificity of 100%. These findings are consistent with previous reports, suggesting that the lower resolution of ultrasound in detecting small cysts and early lesions largely accounts for the reduced sensitivity observed [28]. Notably, the combined use of ultrasound and CA125 in diagnosing endometriosis can increase sensitivity to 92.16% while maintaining high specificity, thereby improving diagnostic accuracy. Furthermore, our findings revealed a superior AUC when compared to prior studies utilizing multiple diagnostic indicators for endometriosis detection [24]. This enhancement may be attributed to the complexity of endometriosis, which presents with varied symptoms and affects multiple organs. A collaborative diagnostic approach can facilitate a comprehensive assessment, further enhancing diagnostic efficacy.
This study has several limitations that should be considered. The modest sample size (n = 103) restricted in-depth subgroup analyses, particularly for rare lesion subtypes, and may have increased the risk of selection bias. Furthermore, although healthy controls were included, the absence of pathological confirmation means that asymptomatic endometriosis cannot be definitively ruled out in the control group. Future studies with larger, prospectively recruited cohorts and gold-standard verification for all participants are needed to validate these findings and facilitate the translation of this combined diagnostic strategy into routine clinical practice.
In summary, this study developed a combined diagnostic model integrating CA125 and ultrasound detection, offering a novel method for the precise non-invasive diagnosis of endometriosis. To strengthen clinical applicability, future efforts should focus on multi-center validation using larger, prospective cohorts. Further refinement of diagnostic accuracy could also be achieved by incorporating additional novel biomarkers alongside advanced ultrasound characteristics.
This study demonstrates that the combined use of CA125 and ultrasound shows a trend toward improvement of the non-invasive diagnosis of endometriosis, achieving a sensitivity of 92.16%, specificity of 98.08%, and an overall diagnostic accuracy of 95.15%. While CA125 alone exhibited high diagnostic performance (AUC: 0.97, 95% CI: 0.94–1.00), its integration with ultrasound further improved sensitivity, particularly in detecting early or atypical lesions that may evade detection by either method alone. The non-invasive nature of this combined approach offers a promising alternative to laparoscopy, potentially reducing surgical risks and enabling earlier intervention for symptom management and fertility preservation. However, the retrospective design and limited sample size underscore the need for validation in larger, prospective cohorts. These findings advocate for the adoption of CA125 and ultrasound as a first-line diagnostic strategy, bridging the gap between clinical suspicion and definitive diagnosis in endometriosis care.
All the original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
YHZ and XZ designed the research study. YQZ, SL and JW performed the research. HL, YQZ and MW analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki. This study has been approved by the Ethics Committee of Women and Children’s Hospital, School of Medicine, Xiamen University (KY-2025-104-K01). All patients meet the criteria for waiver of informed consent.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work the authors used DeepSeek in order to check spell and grammar. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.