
 , Gul Cakmak 2, Ulgen Zengin 3, Bushra M Abdallah 4, Sunullah Soysal 5, Ayten Saracoglu 6,*
, Gul Cakmak 2, Ulgen Zengin 3, Bushra M Abdallah 4, Sunullah Soysal 5, Ayten Saracoglu 6,*
1 Department of Obstetrics and Gynecology, Gazi Yasargil Training and Research Hospital Kayapinar, 21010 Diyarbakir, Turkey
2 Department of Anaesthesiology and Reanimation, Istanbul Training and Research Hospital, 34098 Istanbul, Turkey
3 Department of Anaesthesiology and Reanimation, Marmara Pendik Training and Research Hospital, 34899 Istanbul, Turkey
4 College of Medicine, QU Health, Qatar University, 3050 Doha, Qatar
5 Department of Obstetrics and Gynaecology, University of Marmara Pendik Training and Research Hospital, 34899 Istanbul, Turkey
6 Department of Anesthesiology, University of Florida, UF Health, Jacksonville, FL 32209, USA
Abstract
This study aimed to determine the effect of hypertensive disorders during pregnancy, systolic blood pressure (SBP), and diastolic blood pressure (DBP) on maternal and fetal mortality and morbidity.
This retrospective cohort study included 195 women aged ≥18 years with hypertensive disorders during pregnancy who underwent caesarean section between 2012 and 2017. Patients were divided into groups based on their hypertensive diagnosis (25 with gestational hypertension (GHT), 164 with preeclampsia, 6 with eclampsia) or the recorded SBP or DBP readings at delivery. Logistic regression and linear regression were used to examine associations between hypertensive diagnosis, DBP at delivery, SBP at delivery, and the development of adverse maternal and fetal outcomes after adjusting for confounders.
Multivariable regression analysis revealed a trend toward an increased risk of intrauterine growth restriction (IUGR) (adjusted risk ratio (aRR) = 2.92; p = 0.09) in patients with eclampsia compared to those with GHT, while patients with preeclampsia had a significantly increased risk of IUGR (aRR = 2.77; p = 0.003). Patients with preeclampsia also had a threefold increased risk of premature delivery (aRR = 3.29; p < 0.004), while those with eclampsia had a fourfold increased risk (aRR = 4.09; p = 0.002) compared to patients with GHT. Both groups also had significantly lower fetal birth weights than the GHT group. A DBP of ≥90 mmHg during delivery was associated with significantly reduced fetal birth weight (coefficients (Coef.), –381.5, 95% confidence interval (CI), –739.6 to –23.4; p = 0.04). No significant differences were observed in the outcomes between patients with an SBP value <140 mmHg during delivery and those with a SBP recording ≥140 mmHg.
SBP and DBP are important parameters in the maternal early warning criteria. Strict DBP monitoring may help to increase patient safety, especially in patients with preeclampsia or eclampsia.
Keywords
- diastolic blood pressure
- systolic blood pressure
- hypertensive disorders of pregnancy
- gestational hypertension
- preeclampsia
- eclampsia
Gestational hypertension (GHT) is defined as systolic blood pressure (SBP)
Hypertensive disorders of pregnancy are associated with higher risks for diabetes mellitus, renal disorders, cardiovascular disorders, and premature birth [4]. It has been estimated that one in ten maternal deaths in Asia and Africa is due to hypertensive disorders of pregnancy [2], and that GHT is responsible for 16% of stillbirths worldwide. More detailed analyses have shown that high SBP was associated with increased admission to intensive care in the postpartum period, as well as increases in preterm birth, stillbirth, and kidney damage [5]. Moreover, 10% of early neonatal deaths are known to be accompanied by hypertensive disorders of pregnancy [6]. It has been shown that high SBP values increase fetal mortality and morbidity, as well as maternal mortality and morbidity [7]. For this reason, early diagnosis and treatment of hypertensive disorders are important in order to prevent complications [8].
Changes in the cardiovascular system and volume balance between body compartments in patients with GHT lead to a vicious cycle that involves an uncontrolled increase in blood pressure due to increased cardiac output and intravascular volume, activation of the renin-angiotensin-aldosterone system, sodium retention, and natriuresis [9]. These pathophysiological changes make it difficult to diagnose hypertensive disorders in early pregnancy, resulting in treatment disruption that can lead to serious maternal and fetal complications. One of the most common adverse impacts on the fetus is intrauterine growth restriction (IUGR), resulting from decreased placental blood flow due to increased maternal blood pressure [10].
Changes in SBP and DBP caused by aggressive treatment of hypertension are
explained with the concept of the “J curve”, whereby serious reductions and
elevations in DBP rather than SBP have negative effects on organ perfusion. Bilo
et al. [11] reported variations in the “J curve” according to age and
concomitant diseases. The Systolic Blood Pressure Intervention Trial (SPRINT)
study [12] highlighted that SBP should be kept at
To our knowledge, there are still no studies in the literature on the “J curve” in patients with GHT. In pregnant women with uncontrolled hypertension after 37 weeks gestation, emergency delivery is recommended due to the increased risk of maternal and fetal complications. However, there continue to be poor outcomes in this patient group, possibly due to a lack of research with regard to DBP [10]. Therefore, the primary aim of this study was to investigate the effects of hypertensive disorders of pregnancy on maternal and fetal mortality and morbidity. The secondary aim was to examine the effects of elevated DBP and SBP at delivery on maternal and fetal pregnancy outcomes.
This study was conducted at Marmara University Pendik Training and Research
Hospital, and ethical approval was obtained from the Ethics Committee of Marmara
University (Approval No: 09.2018.162, dated 06 January 2018). The study was
performed in accordance with the ethical standards of the institutional and/or
national research committee and with the 1964 Helsinki Declaration and its
subsequent revisions. This was a retrospective cohort study of adult patients
with hypertensive disorders of pregnancy. We included pregnant women aged
The requirement for patient consent was waived because of the retrospective
nature of this study. Data was entered into a standardised data collection sheet
on Microsoft Excel for Mac, Version 16.83 (Microsoft Corporation, Redmond, WA,
USA). The following information was collected: (1) baseline demographic
characteristics including age, body mass index (BMI), gestational age,
concomitant maternal disorders, and laboratory results for creatinine and
haemoglobin; (2) SBP and DBP readings at admission and delivery; (3) fetal and
neonatal data including fetal birth weight, Appearance, Pulse, Grimace, Activity
and Respiration (APGAR) scores at 1 and 5 minutes, prematurity, and IUGR; and (4)
postpartum and postoperative outcomes including length of hospital stay, presence
of postoperative severe arrhythmia, and pulmonary embolism. The length of
hospital stay was defined as the duration between the first day of patient
admission to the hospital and discharge. Gestational age was recorded as a
continuous variable, but was categorized into the following clinically meaningful
groups: preterm (
Both SBP and DBP values were recorded to evaluate potential relationships between hypo- or hypertension and various outcomes, including length of hospital stay, fetal birth weight, and risks for pulmonary embolism, IUGR, premature delivery, and arrhythmia. Blood pressure was measured using an automated oscillometric device (Model HKD-02, manufactured by Hunkar Ltd. A.S., Denizli, Turkey). Measurements were obtained in the seated position after at least 5 min rest. For each patient, three consecutive readings were taken at one-minute intervals, with the average of the last two readings used for analysis. All measurements were performed by trained personnel using appropriately sized cuffs to ensure consistency and accuracy.
Participants were categorized into three different exposure groups to assess
outcomes across various hypertensive and blood pressure parameters. The first
categorization grouped patients by their specific diagnosis of hypertensive
disorder of pregnancy (GHT, preeclampsia, or eclampsia). The second
categorization grouped participants based on their DBP at delivery (
Preeclampsia was diagnosed based on the presence of new-onset hypertension after
20 weeks of gestation, along with proteinuria
Postoperative severe arrhythmia was defined as any clinically significant disturbance of cardiac rhythm occurring within the first 48 h after surgery and requiring intervention, including pharmacologic therapy or electrical cardioversion, or causing hemodynamic instability. Severe arrhythmias included sustained ventricular tachycardia, ventricular fibrillation, torsades de pointes, new-onset high-grade atrioventricular block, or rapid atrial fibrillation/flutter with hemodynamic compromise. All events were confirmed by continuous electrocardiogram (ECG) monitoring, telemetry, or 12-lead ECG.
Statistical comparisons were performed to evaluate differences across three groups: GHT, preeclampsia, and eclampsia. Numerical data were summarized as the mean and standard deviation if normally distributed, or as the median and interquartile range if they were not normally distributed. The distribution of continuous variables, such as age, birth weight, and BMI, was assessed using the Shapiro-Wilk test. Groups with normally distributed numerical data were compared with the Student’s t test and analysis of variance (ANOVA) test, while groups with skewed data were compared with the Kruskal-Wallis test and the Wilcoxon rank-sum test. Categorical data were presented as frequencies and percentages. Pearson’s Chi-squared test and Fisher’s exact test were used to test hypotheses and compare categorical data.
The relationships between exposures and outcomes of interest were evaluated using three models of multivariable logistic regression and linear regression. The first model examined associations between hypertensive disorders of pregnancy and maternal and fetal outcomes, the second model examined associations between DBP at delivery and the same outcomes, while the third model examined associations between SBP at delivery and the same outcomes. The logistic regression and linear regression models were adjusted for age and gestational diabetes mellitus (GDM). Logistic regression was utilized for categorical outcomes, which included the development of pulmonary embolism, IUGR, premature delivery, and postoperative arrhythmia. Linear regression was employed for continuous outcomes, including fetal birth weight and the length of hospital stay. For categorical outcomes, modified Poisson regression with robust variance estimation was used to calculate adjusted risk ratios (aRR). We chose this approach because several outcomes were common, and estimating aRRs provides a more interpretable measure of relative risk than odds ratios, which can overestimate the effect size in such scenarios.
The 95% confidence interval (95% CI) for aRRs and regression coefficients (Coef.) was also reported. Exact p-values were reported and interpreted as evidence against the null hypothesis. All statistical analyses were carried out using IBM SPSS Statistics 22 (IBM Corp, Armonk, NY, USA) and Stata 18.0 (StataCorp, College Station, TX, USA).
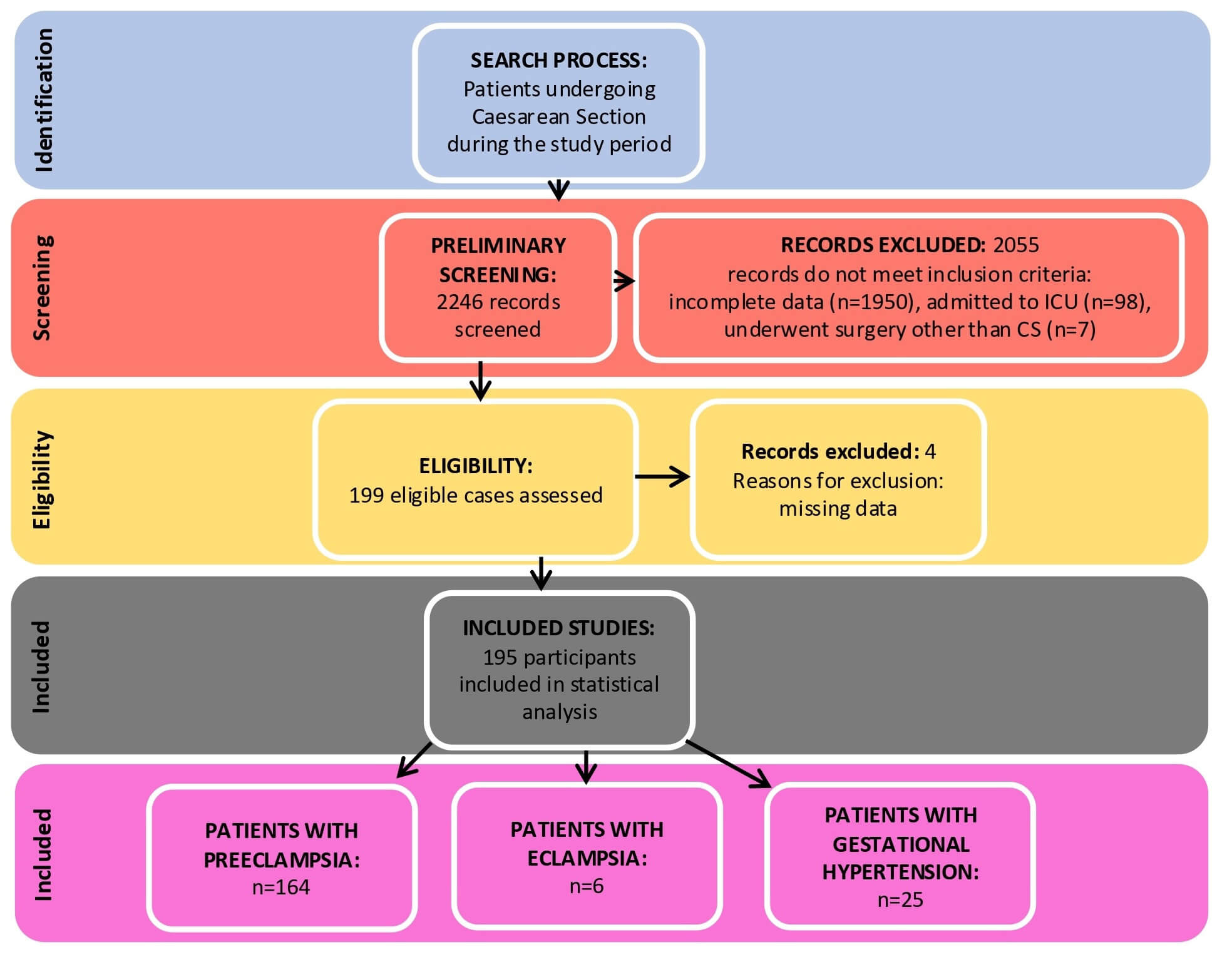
Fig. 1 shows the flow chart for this study and the participant selection process. A total of 2246 patient records underwent preliminary screening for eligibility. After exclusion of ineligible cases, 195 participants were available for inclusion, of which 25 had GHT, 164 had preeclampsia, and 6 had eclampsia. Patients with incomplete data were handled using listwise deletion. Four patients with missing data were excluded from the final analysis.
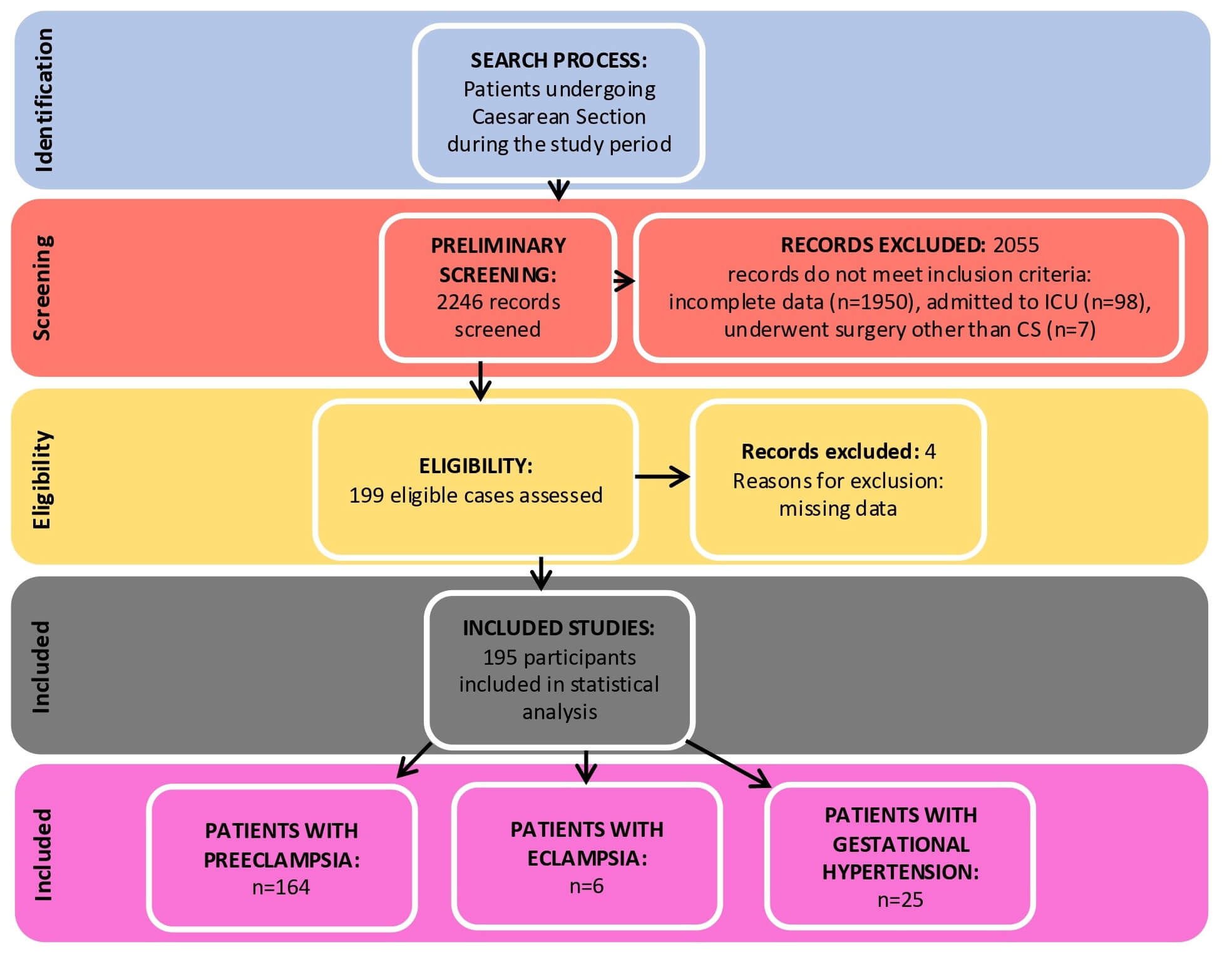 Fig. 1.
Fig. 1.
Flow chart for participant selection. ICU, intensive care unit; CS, cesarean section.
Table 1 presents the baseline characteristics of participants. The eclampsia group was the youngest (mean age 27.0 years), while the GHT group was the oldest (mean age 33.8 years). Patients with GHT had a shorter median hospital stay compared to patients with preeclampsia or eclampsia. The mean fetal birth weight was lowest in the eclampsia group, followed by the preeclampsia and then GHT groups. The majority of participants were multigravida, with 52 (26.7%) being primigravida. The majority of patients with GHT delivered between 37 and 41+6 weeks (76%), whereas most deliveries for preeclampsia patients occurred between 31 and 36+6 weeks (43.9%).
| Parameter | Gestational hypertension (n = 25) | Preeclampsia (n = 164) | Eclampsia (n = 6) | |
| Age, years; mean (SD) | 33.8 (6.0) | 30.5 (6.3) | 27.0 (6.0) | |
| BMI, kg/m2; mean (SD) | 32.7 (2.9) | 31.5 (5.0) | 30.0 (3.8) | |
| Gestational age, weeks | ||||
| 24–30+6 | 0 (0.0%) | 28 (17.1%) | 3 (50.0%) | |
| 31–36+6 | 6 (24.0%) | 72 (43.9%) | 3 (50.0%) | |
| 37–41+6 | 19 (76.0%) | 64 (39.0%) | 0 (0.0%) | |
| Primigravida/Multigravida | ||||
| Primigravida | 2 (8.0%) | 46 (28.0%) | 4 (66.7%) | |
| Multigravida | 23 (92.0%) | 118 (72.0%) | 2 (33.3%) | |
| C-section urgency | ||||
| Elective | 4 (16.0%) | 22 (13.4%) | 0 (0.0%) | |
| Emergency | 21 (84.0%) | 142 (86.6%) | 6 (100.0%) | |
| Anaesthesia type | ||||
| General | 14 (56.0%) | 89 (54.3%) | 6 (100.0%) | |
| Spinal | 11 (44.0%) | 75 (45.7%) | 0 (0.0%) | |
| Birth weight, g; mean (SD) | 3279.6 (866.5) | 2298.6 (1013.6) | 1623.3 (706.9) | |
| APGAR score, 1 min; median (IQR) | 9.0 (8.0–9.0) | 8.0 (6.0–9.0) | 5.0 (5.0–8.0) | |
| APGAR score, 5 min; median (IQR) | 10.0 (10.0–10.0) | 10.0 (8.0–10.0) | 7.5 (7.0–9.0) | |
| Gestational DM | 1 (4.0%) | 11 (6.7%) | 0 (0.0%) | |
| Pre-pregnancy DM | 3 (12.0%) | 8 (4.9%) | 0 (0.0%) | |
| Antihypertensive medication | ||||
| None | 11 (44.0%) | 30 (18.3%) | 1 (16.7%) | |
| Methyldopa | 1 (4.0%) | 23 (14.0%) | 0 (0.0%) | |
| Nifedipine | 10 (40.0%) | 48 (29.3%) | 3 (50.0%) | |
| Methyldopa & Nifedipine | 3 (12.0%) | 61 (37.2%) | 2 (33.3%) | |
| Methyldopa & Doxazosin | 0 (0.0%) | 1 (0.6%) | 0 (0.0%) | |
| Nifedipine & Captopril | 0 (0.0%) | 1 (0.6%) | 0 (0.0%) | |
| Urine protein | ||||
| Negative | 4 (16.0%) | 13 (7.9%) | 1 (16.7%) | |
| Trace | 21 (84.0%) | 18 (11.0%) | 1 (16.7%) | |
| 1+ | 0 (0.0%) | 14 (8.5%) | 0 (0.0%) | |
| 2+ | 0 (0.0%) | 61 (37.2%) | 0 (0.0%) | |
| 3+ | 0 (0.0%) | 52 (31.7%) | 3 (50.0%) | |
| 4+ | 0 (0.0%) | 6 (3.7%) | 1 (16.7%) | |
| 24-h urine protein, g; median (IQR) | 0.0 (0.0–110.0) | 1645.5 (597.5–3294.0) | 3839 (800.0–8632.0) | |
| Hospital LOS, days; median (IQR) | 2.0 (2.0–3.0) | 3.5 (3.0–5.0) | 4.5 (4.0–5.0) | |
BMI, body mass index; C-Section, caesarean section; APGAR, Appearance, Pulse, Grimace, Activity and Respiration; DM, diabetes mellitus; SD, standard deviation; IQR, interquartile range; LOS, length of stay.
A significant difference in patient age was found between groups (p =
0.04). Pairwise analysis revealed that patients with preeclampsia were
significantly younger compared to those with GHT (p = 0.015).
Differences in the level of 24-h urine protein between groups were highly
significant (p
A significant difference was found in the gestational age at delivery
(p
The duration of hospital stay differed significantly across the groups
(p
DBP at delivery demonstrated a significant overall difference between groups (p = 0.036). This was driven by a difference between the preeclampsia and GHT groups (p = 0.016), with no significant difference observed in the other pairwise comparisons. Creatinine levels were significantly different among the groups (p = 0.005). Pairwise comparisons confirmed that both preeclampsia (p = 0.005) and eclampsia patients (p = 0.040) had significantly higher creatinine levels compared to GHT patients.
Table 2 presents the blood pressure measurements, as well as the maternal and
fetal outcomes, in each of the three hypertensive groups. No cases of maternal
mortality occurred in this cohort. All groups had a similarly low incidence of
postoperative arrhythmia and pulmonary embolism. Our analysis also revealed a
significant association between prematurity and the diagnostic group (p
| Factor | Gestational hypertension (n = 25) | Preeclampsia (n = 164) | Eclampsia (n = 6) |
| SBP on admission, mmHg; mean (SD) | 162.0 (14.8) | 163.5 (15.6) | 162.7 (15.5) |
| DBP on admission, mmHg; mean (SD) | 96.4 (10.5) | 99.4 (12.4) | 96.5 (15.3) |
| HR on admission, bpm; mean (SD) | 91.4 (11.5) | 94.3 (14.5) | 82.0 (12.9) |
| SBP before induction, mmHg; mean (SD) | 151.8 (18.0) | 157.6 (23.8) | 172.5 (14.1) |
| DBP before induction, mmHg; mean (SD) | 88.6 (13.0) | 96.2 (16.3) | 102.0 (13.0) |
| HR before induction, bpm; mean (SD) | 103.2 (15.8) | 101.4 (16.8) | 109.8 (14.0) |
| SBP at delivery |
2 (8.0%) | 23 (14.0%) | 0 (0.0%) |
| SBP at delivery |
23 (92.0%) | 141 (86.0%) | 6 (100.0%) |
| DBP at delivery |
8 (32.0%) | 33 (20.1%) | 0 (0.0%) |
| DBP at delivery |
17 (68.0%) | 131 (79.9%) | 6 (100.0%) |
| Pulmonary embolism | 1 (4.0%) | 4 (2.4%) | 0 (0.0%) |
| IUGR | 4 (16.0%) | 72 (43.9%) | 3 (50.0%) |
| Seizure | 0 (0.0%) | 0 (0.0%) | 6 (100.0%) |
| Prematurity | 5 (20.0%) | 108 (65.9%) | 5 (83.3%) |
| Postoperative severe arrhythmia | 1 (4.0%) | 4 (2.4%) | 0 (0.0%) |
SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; IUGR, intrauterine growth restriction.
Further, the majority of patients had elevated SBP and DBP readings at delivery.
The incidence of seizures was very different across the groups (p
We examined the associations between the type of hypertensive disorder including gestational hypertension, preeclampsia, and eclampsia together with maternal and fetal outcomes. Multivariable logistic regression analysis showed that compared to patients with GHT, patients with preeclampsia and eclampsia had 2.77-fold and 2.92-fold higher risks of developing IUGR, respectively (Table 3). Similarly, patients with preeclampsia and eclampsia had 3-fold and 4-fold higher risks of premature delivery, respectively, compared to those with GHT. The risk for postoperative arrhythmia was lower in the preeclampsia group, but this difference did not reach statistical significance. There was no difference in the risk of pulmonary embolism between patients with preeclampsia and GHT. Linear regression showed that both preeclampsia and eclampsia were both associated with significantly lower fetal birth weight compared to GHT. Further, they were both associated with a longer hospital stay compared to GHT. The association between eclampsia and the development of pulmonary embolism or postoperative arrhythmia could not be assessed due to an insufficient number of cases with these outcomes.
| Outcome | Condition | Adjusted effect size* | 95% CI | p-value |
| Birth weight | Preeclampsia | Coef. –992.4 | –1411.6 to –573.3 | |
| Eclampsia | Coef. –1599.0 | –2485.0 to –713.1 | ||
| Hospital LOS | Preeclampsia | Coef. 2.06 | 0.62 to 3.50 | 0.005 |
| Eclampsia | Coef. 1.91 | –1.13 to 4.95 | 0.220 | |
| Pulmonary embolism | Preeclampsia | aRR 0.90 | 0.10 to 8.00 | 0.930 |
| Eclampsia | - | - | - | |
| IUGR | Preeclampsia | aRR 2.77 | 1.11 to 6.93 | 0.003 |
| Eclampsia | aRR 2.92 | 0.85 to 10.01 | 0.090 | |
| Prematurity | Preeclampsia | aRR 3.29 | 1.48 to 7.32 | |
| Eclampsia | aRR 4.09 | 1.69 to 9.90 | 0.002 | |
| Postoperative severe arrhythmia | Preeclampsia | aRR 0.63 | 0.07 to 5.69 | 0.680 |
| Eclampsia | - | - | - |
LOS, length of stay; aRR, adjusted risk ratio; CI, confidence interval; Coef., regression coefficients.
* Adjusted for age and gestational diabetes mellitus.
We evaluated the impact of diastolic blood pressure at delivery, comparing women
with DBP
| Factor | DBP |
DBP |
Adjusted effect size* | 95% CI | p-value |
| Birth weight, mean (SD) | 2658.2 (1037.2) | 2335.8 (1042.3) | Coef. –381.5 | –739.6 to –23.4 | 0.04 |
| Hospital LOS, median (IQR) | 3.0 (2.0, 5.0) | 3.0 (3.0, 5.0) | Coef. 0.38 | –0.81 to 1.57 | 0.53 |
| Pulmonary embolism | 0 (0.0%) | 5 (3.2%) | - | - | - |
| IUGR | 15 (36.6%) | 64 (41.8%) | aRR 1.20 | 0.77 to 1.89 | 0.42 |
| Prematurity | 22 (53.7%) | 96 (62.3%) | aRR 1.21 | 0.88 to 1.66 | 0.25 |
| Postoperative severe arrhythmia | 1 (2.4%) | 4 (2.6%) | aRR 1.06 | 0.12 to 9.45 | 0.96 |
| Seizure | 0 (0.0%) | 6 (3.9%) | - | - | - |
* Adjusted for age and gestational diabetes mellitus.
We analyzed the relationship between systolic blood pressure at delivery as
| Factor | SBP |
SBP |
Adjusted effect size* | 95% CI | p-value |
| Birth weight, mean (SD) | 2269.1 (945.1) | 2423.4 (1062.2) | Coef. 149.7 | –287.3 to 586.8 | 0.50 |
| Hospital LOS, median (IQR) | 3.0 (2.0, 6.0) | 3.0 (3.0, 5.0) | Coef. 0.54 | –0.89 to 1.98 | 0.46 |
| Pulmonary embolism | 0 (0.0%) | 5 (2.9%) | - | - | - |
| IUGR | 11 (44.0%) | 68 (40.2%) | aRR 0.91 | 0.57 to 1.47 | 0.72 |
| Prematurity | 15 (60.0%) | 103 (60.6%) | aRR 1.02 | 0.72 to 1.44 | 0.91 |
| Postoperative severe arrhythmia | 0 (0.0%) | 5 (2.9%) | - | - | - |
| Seizure | 0 (0.0%) | 6 (3.5%) | - | - | - |
* Adjusted for age and gestational diabetes mellitus.
This study of patients with hypertensive disorders of pregnancy found that
preeclampsia and eclampsia increased the risk of developing IUGR by 2.77-fold and
2.92-fold, respectively, compared to GHT. Further, elevated DBP during delivery
(
Prolonged high blood pressure leads to cardiac chamber remodeling, concentric hypertrophy, and diastolic dysfunction, thereby creating conditions that can facilitate arrhythmias, including atrial fibrillation [19]. Various studies have shown that elevated SBP and DBP readings are associated with atrial and ventricular arrhythmia in both obstetric and non-obstetric hypertensive individuals [20, 21]. A meta-analysis in a non-obstetric hypertensive population found that individuals with SBP of 120–130 mmHg and DBP of 60–69 mmHg had a lower incidence of arrhythmia, highlighting the importance of optimal management of hypertension [22].
The tendency toward arrhythmia increases in pregnancy due to hormonal shifts,
reduced autonomic tone, and hemodynamic changes. It often arises in conjunction
with a sudden rise in cardiac output and heart rate triggered by pain during
delivery [23]. Leon et al. [24] identified an association between
elevated blood pressure and postpartum arrhythmia in obstetric patients. However,
to our knowledge, no studies have yet compared DBP and SBP in this context. In the
present study, although we observed that patients with SBP
During early pregnancy, uterine circulation has high-capacity and low resistance
due to trophoblastic invasion and the remodeling of spiral arteries. Severe
preeclampsia is defined as SBP
Studies in the literature have emphasized the importance of managing blood
pressure in severe preeclampsia, with uncontrolled decreases in blood pressure
having negative effects on patient outcomes. Improvements in maternal and fetal
outcomes have been found in patients with SBP
Our findings are consistent with recent evidence highlighting the prognostic importance of maternal DBP in hypertensive disorders of pregnancy. Emerging literature increasingly underscores the nuanced predictive value of both SBP and DBP trajectories in hypertensive disorders of pregnancy. A multicenter retrospective study in women with chronic hypertension found that maintaining SBP below 130 mmHg before 15 weeks reduced the risk of early-onset superimposed preeclampsia and small-for-gestational-age neonates compared with SBP between 140–159 mmHg [29]. Similarly, a Mendelian randomization analysis has provided causal evidence that genetically higher SBP and DBP increase the risk of preeclampsia, preterm birth, and placental abruption [30]. In addition, a large Chinese cohort that examined combined SBP and DBP trajectories showed that higher maternal DBP during both early and late pregnancy was linked to reduced left and right ventricular end-diastolic volumes in offspring, suggesting long-term cardiovascular effects [31]. Taken together, these studies support our observation that DBP may be a more sensitive indicator than SBP for predicting adverse maternal and fetal outcomes in hypertensive pregnancies.
The present study has several strengths. It included all eligible adult patients diagnosed with hypertensive disorders of pregnancy and who underwent caesarean section at our university hospital. Additionally, it investigated the impact of high and low SBP and DBP readings on pregnancy outcomes in a high-risk population. This provides valuable insights into the complications associated with uncontrolled blood pressure, highlighting the importance of proper blood pressure management. Our findings contribute to the development of management algorithms and guidelines for patients with hypertensive disorders of pregnancy.
Nonetheless, certain limitations should be acknowledged. First, this was a single-center study, which may limit the generalizability of our findings to other settings or populations. In particular, the sample size for the eclampsia group was small, and hence the findings for these patients should be interpreted with caution. Second, the retrospective cohort study design is subject to incomplete data and does not permit the establishment of causality. Future multicenter studies with larger sample sizes and longitudinal designs are recommended to further explore this topic, establish causality, and examine long-term effects. Although our regression analyses were adjusted for age and GDM, other important potential confounders such as BMI, parity, use of antihypertensive medication, and severity of proteinuria were not included. These unmeasured factors may have influenced outcomes, particularly since the eclampsia patients in our cohort were younger and more likely to be primigravida, both of which may independently affect maternal and fetal outcomes. The study draws exclusively on data collected 7–9 years ago (2012–2017). Over this extended interval, diagnostic algorithms, therapeutic guidelines, and demographic characteristics have evolved substantially. Contemporary clinical practice now incorporates newer pharmacologic agents, refined monitoring modalities, and earlier intervention strategies that may materially alter patient outcomes.
In conclusion, hypertensive disorders of pregnancy can significantly affect
fetal outcomes. Preeclampsia and eclampsia were associated with markedly
increased risks of IUGR compared to GHT. Elevated DBP (
The data used in this work are available upon reasonable request from the corresponding author.
AS and KCY designed the research study. GC and UZ performed the research. SS and AS contributed to data collection. KCY and BMA analyzed the data. AS and SS drafted the manuscript. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its subsequent revisions. This study received ethics committee approval with protocol number 09.2018.162 from University of Marmara Pendik Training and Research Hospital. Because of the retrospective design, the requirement for informed consent was waived by the Ethics Committee.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG45125.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.