





1 Department of Gynaecology and Obstetrics, The Second Hospital of Hebei Medical University, 050005 Shijiazhuang, Hebei, China
Abstract
A hypoplastic uterus is a rare anomaly often considered incompatible with successful pregnancy due to inadequate uterine size, thin myometrium, and poor vascularization.
This case reports on a 29-year-old primigravida with a hypoplastic uterus who achieved a full-term pregnancy complicated by central placenta previa and placenta increta. At 37 + 4 weeks of gestation, a cesarean delivery yielded a healthy neonate; however, the patient required an emergent hysterectomy due to extensive uterine rupture and uncontrolled hemorrhage.
This case highlights the importance of meticulous prenatal surveillance in patients with uterine anomalies and underscores the potential necessity for timely intervention to avert life-threatening complications.
Keywords
- hypoplastic uterus
- placenta increta
- uterine rupture
- hysterectomy
The hypoplastic uterus is generally considered incompatible with successful pregnancy due to its compromised ability to sustain normal gestation, characterized by inadequate uterine size, thin myometrium, and poor vascularization [1]. Despite advances in reproductive medicine, natural conception and the attainment of term gestation in patients with a hypoplastic uterus remain exceptionally rare. Most reported cases involve early pregnancy loss or severe complications, such as uterine rupture or abnormal placentation [2]. This report presents a rare case of a hypoplastic uterus that successfully supported a pregnancy to term, complicated by central placenta previa and placenta increta, which ultimately necessitated hysterectomy. Because the patient was referred to our center only at term, this report emphasizes the necessity of early prenatal identification of uterine hypoplasia and timely referral to tertiary care facilities. Furthermore, in situations where maternal health is severely compromised, consideration of elective termination of pregnancy may be warranted.
A 29-year-old primigravida at 37 + 4 weeks of gestation was admitted to the hospital with a diagnosis of placenta previa centralis. Following six years of marriage without contraception, the patient naturally conceived her first pregnancy, which progressed uneventfully until hospitalization. During pregnancy, no progesterone supplementation was administered. The patient did not undergo routine antenatal care at our hospital. At 22 weeks of gestation, fetal ultrasound at an external hospital suggested placenta previa with the placental margin covering the cervical os. At 37 + 4 weeks, upon admission to our hospital, placenta increta was diagnosed with a score of eight based on the placenta accreta scoring system [3]. A cesarean section was performed the following day. Intraoperatively, the placenta occupied almost the entire anterior uterine wall, precluding a corporal or fundal incision that would avoid placental disruption. The uterine muscle wall appeared thin with a purplish-red discoloration, and extensive, prominent blood vessels were observed (Fig. 1). The placenta, located beneath the incision site, was perforated during surgery, resulting in the rupture of the fetal membranes and the delivery of a healthy neonate weighing approximately 2600 g. The uterus exhibited complete atony and appeared sac-like.
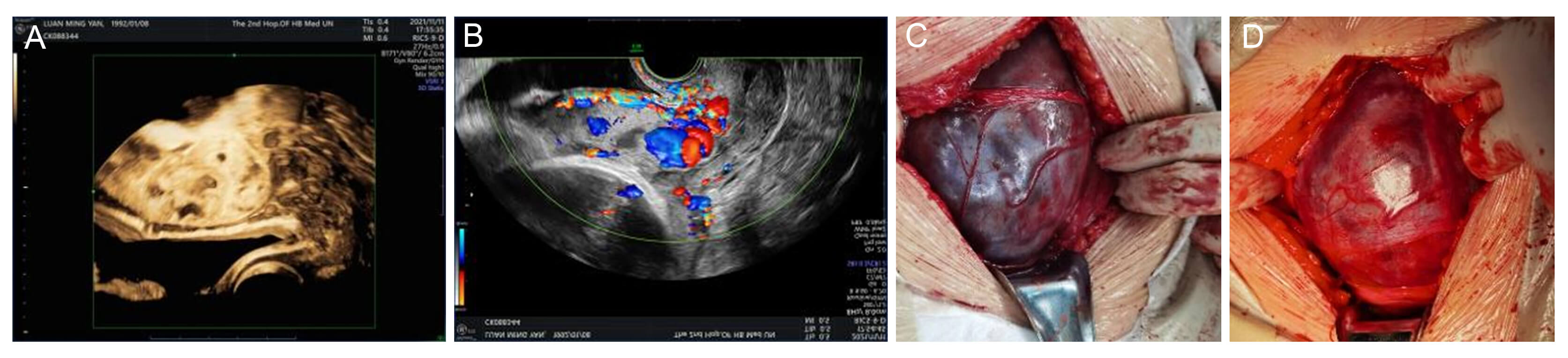 Fig. 1.
Fig. 1.
Ultrasonographic findings and direct vision of the uterine muscle wall. (A,B) Preoperative ultrasonographic examination. (C,D) Intraoperative views of the uterine muscle wall.
To control hemorrhage, a tourniquet was applied to the lower uterine segment. The uterine surface appeared smooth and intact, and bilateral ovaries and fallopian tubes were normal. However, placental attachment was noted on nearly all four walls of the uterine cavity above the internal cervical orifice, sparing the uterine floor. Because of congenital uterine hypoplasia, with diffusely damaged myometrium and loss of contractile function, selective occlusion of the iliac arteries, uterine artery embolization, or leaving the placenta in situ were not considered viable hemostatic strategies. The myometrium demonstrated irregular ruptures attributable to inadequate development, and the uterine wall was unresponsive to uterotonic agents, including oxytocin and carboprost tromethamine. Consequently, the placenta could not detach spontaneously and required manual removal. The placenta was notably large, with a thin, uneven thickness ranging from 1–5 mm. The uterine muscle wall exhibited varying thicknesses of 1–3 mm and was translucent (Fig. 2). Upon release of the tourniquet, substantial intrauterine bleeding ensued. Due to extensive rupture of the uterine wall, predominantly involving the uterine fundus and the adjacent anterior and posterior wall, and the inability to achieve adequate repair, a hysterectomy was performed to save the patient’s life, following informed consent from the mother and her family despite their initial reluctance.
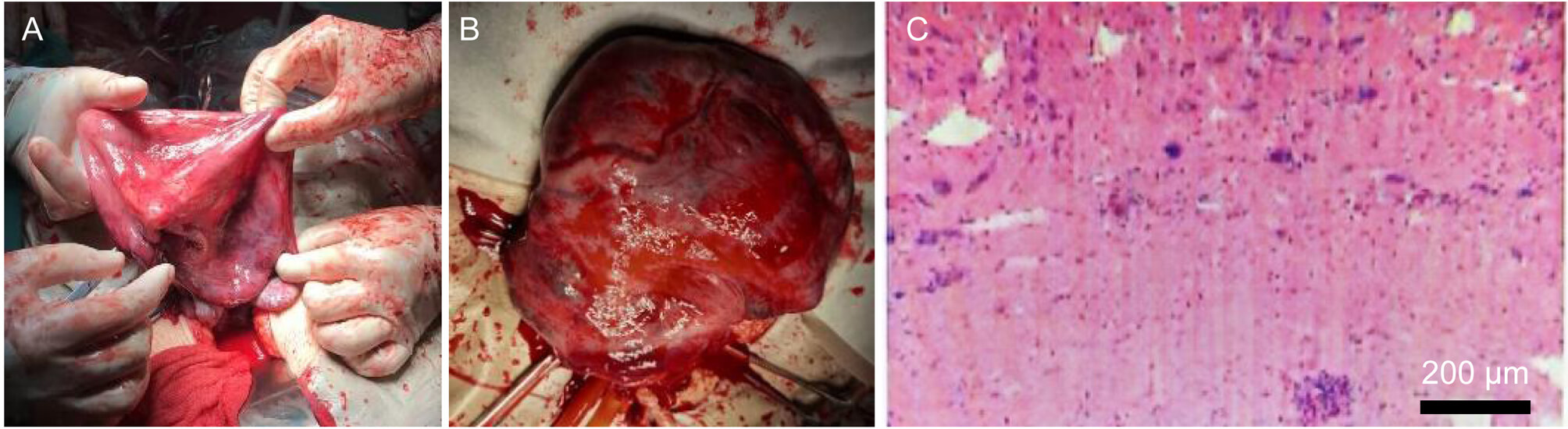 Fig. 2.
Fig. 2.
The uterine muscle wall after delivery of the fetus. (A) The uterine muscle wall exhibiting a translucent appearance under direct vision. (B) The uterine muscle wall after removal. (C) Histopathological examination of the subtotal hysterectomy specimen. Scale bar: 200 μm.
Postoperative review of her medical history revealed light menstrual flow since
menarche at age 12, with no history of dysmenorrhea. A pre-pregnancy ultrasound
at the age of 27 indicated a uterine size of approximately 3.81
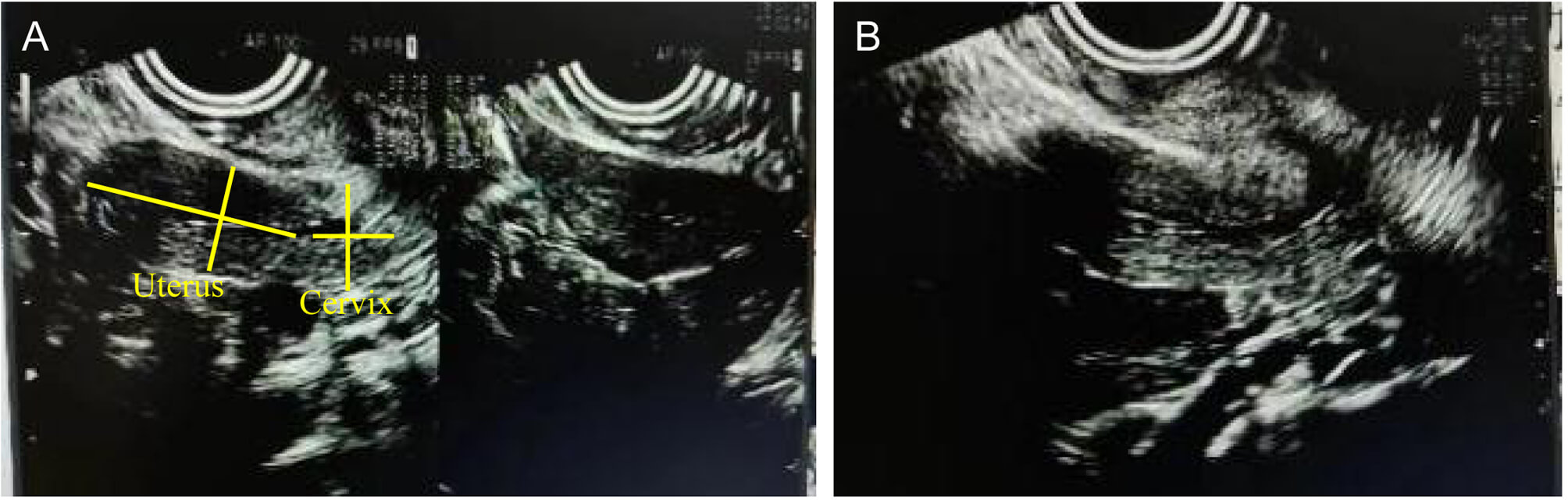 Fig. 3.
Fig. 3.
The sonographic findings of uterus before pregnancy. (A)
Pre-pregnancy uterine ultrasonography (longitudinal and transverse views),
showing a uterine size of approximately 3.81
Hypoplastic uterus is characterized by a normally shaped but undersized uterine corpus, often accompanied by oligomenorrhea and infertility [1]. Transvaginal ultrasound and magnetic resonance imaging (MRI) serve as valuable diagnostic modalities [4, 5]. Despite these challenges, some patients with hypoplastic uterus are able to conceive either spontaneously or through assisted reproductive technologies, although they are at heightened risk for miscarriage, preterm delivery, and uterine rupture [6, 7]. Term pregnancy, as in this case, is exceptionally rare. In this case, pre-pregnancy ultrasonography demonstrated a small uterus with normal but diminutive bilateral ovaries and a uterine body-to-cervix ratio approaching 2:1. The patient also reported scant menstrual flow and difficulty conceiving, consistent with a diagnosis of uterine hypoplasia [2].
Uterine rupture in patients with uterine dysplasia is attributed to increased uterine cavity pressure during pregnancy combined with reduced myometrial muscle mass. This impairs the uterus’s ability to contract spontaneously, leading to cervical dilation and non-responsiveness to uterotonic agents, rendering vaginal delivery unfeasible. Nevertheless, postpartum hemorrhage often necessitates surgical removal of the uterus. Reduced uterine muscle mass is a known contributor to adverse pregnancy outcomes. In patients with a hypoplastic uterus, myometrial dysplasia and abnormal uterine artery blood flow result in diminished spiral artery distribution and reduced or absent decidua basalis. This predisposes to placental villi attachment to the basal decidual layer with partial or complete myometrial invasion [8]. This markedly increases the risk of uterine rupture, and the occurrence of abdominal pain in such patients should raise strong clinical suspicion. Systematic monitoring of myometrial thickness and placental invasion is essential for evaluating rupture risk in pregnancies complicated by uterine hypoplasia. Although MRI offers superior assessment of villous invasion and placental coverage, we opted for an economical and practical ultrasound scoring system. The patient’s score of 8 predicted a moderate risk of intraoperative hemorrhage, providing valuable guidance for clinical management [3]. Histopathological examination of the hysterectomy specimen revealed marked thinning of the myometrium with cystic dilatation and placenta increta, which is consistent with the diagnosis of uterine hypoplasia and confirms the structural abnormality. However, the case still lacked further etiological assessment, such as endocrine, genetic, or Müllerian duct anomaly evaluation, which remains a limitation of this report.
In conclusion, the eligibility of patients with uterine dysplasia for pregnancy requires comprehensive evaluation. Continuous monitoring of the myometrium and placenta throughout gestation is imperative, with meticulous assessment of both the timing and mode of delivery to minimize the risk of uterine rupture. Cesarean section remains the preferred delivery approach in such cases. In instances of extensive placental invasion, immediate hysterectomy may be warranted to safeguard maternal and neonatal health, thereby optimizing pregnancy outcomes.
All data reported in this paper will also be shared by the corresponding author upon request.
QL and CW designed the research study. RP performed the research. WJ analyzed the data. QL and CW wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the Ethics Committee of the Second Hospital of Hebei Medical University (Ethic Approval Number: 2024-P039), and the participant provided signed informed consent.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work, the authors used ChatGPT-3.5 in order to check spelling and grammar. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG45041.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.