

 , Tugba Gurbuz 2, Halime Cali Ozturk 3
, Tugba Gurbuz 2, Halime Cali Ozturk 31 Department of Gynecology and Obstetrics, Memorial Bahçelievler Hospital IVF and Istanbul Arel University, 34180 Istanbul, Turkey
2 Department of Gynecology and Obstetrics Clinic, Medistate Hospital, Istanbul Nişantaşı University, 34381 Istanbul, Turkey
3 Department of Obstetrics and Gynecology, Bezmialem University, 34093 Istanbul, Turkey
Abstract
Unexplained infertility (UI) affects a significant portion of couples worldwide, posing challenges for effective treatment. The prognostic nutritional index (PNI), traditionally used in oncology, has been adapted to evaluate reproductive outcomes, particularly in the context of in vitro fertilization (IVF).
This study analyzed 198 non-obese couples undergoing IVF for UI at a tertiary care center between February 2023 and December 2024. This study assessed the correlation between the PNI, comprehensive hematological profiles, and IVF outcomes, including embryo quality and pregnancy. The PNI was obtained through serum albumin and lymphocyte counts.
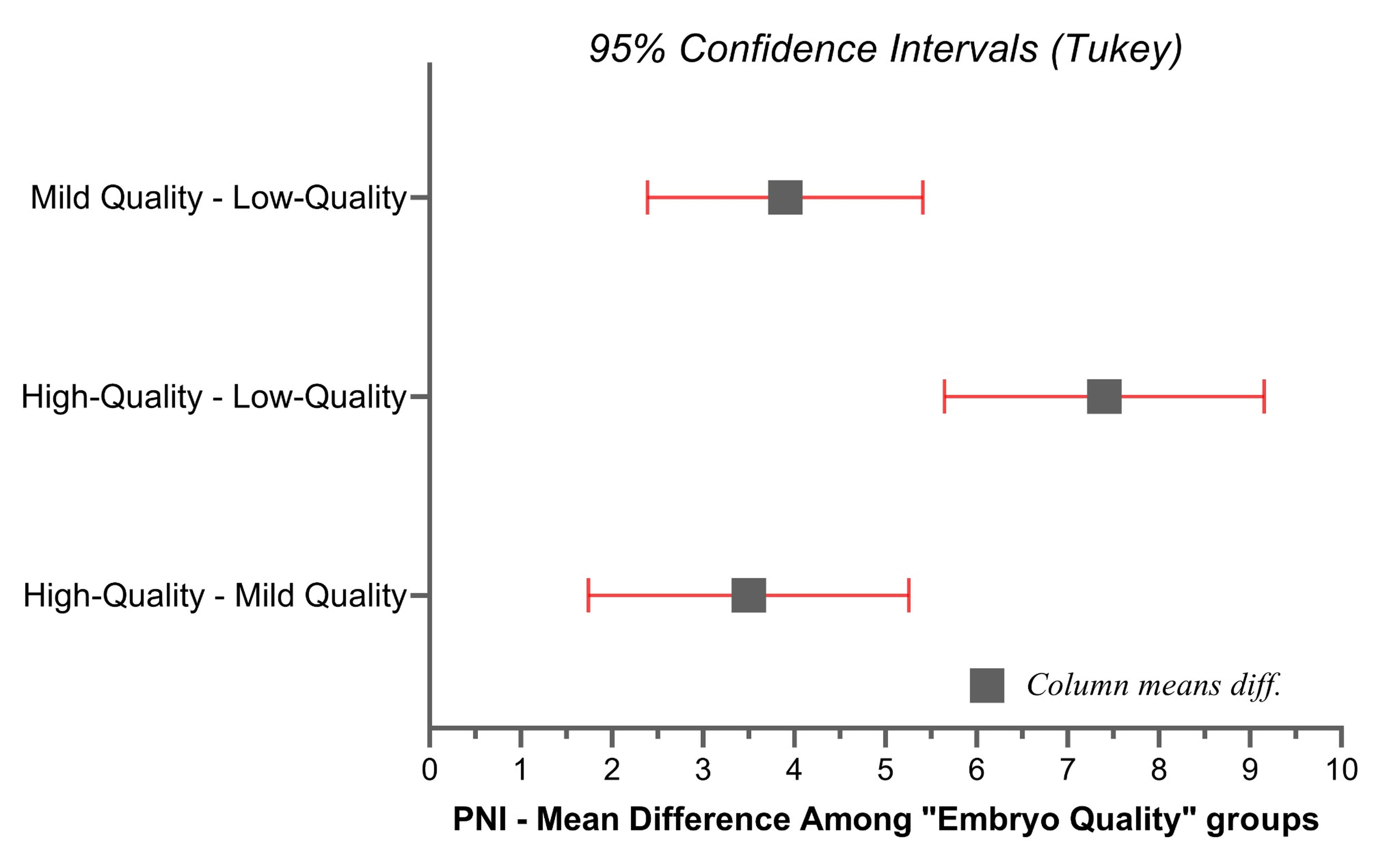
The PNI was elevated in the high-quality embryos (51.65 ± 5.09) compared to those of mild-quality (48.10 ± 2.82) and low-quality (44.20 ± 4.16) (p = 0.0001). A higher PNI was associated with improved embryo quality, with an odds ratio of 11.859 (p = 0.0001) for higher quality embryos. Other inflammatory markers did not demonstrate a predictive value for IVF outcomes (p > 0.05). The PNI yielded an area under the curve (AUC) value of 0.895 (95% confidence interval (CI): 0.85–0.94; p = 0.001), indicating robust discrimination. At a cutoff of 46.5, the PNI demonstrated 81.2% sensitivity and 80.1% specificity, further underscoring the potential of this index as a discriminative marker.
The PNI serves as a strong indicator of IVF outcomes, correlating directly with embryo quality and the success of fertility treatments. Moreover, the predictive potential of the PNI for embryo quality in reproductive medicine highlights the intersection of nutritional and immunological status with reproductive health, offering a framework for enhancing clinical assessments in IVF.
Keywords
- prognostic nutritional index
- unexplained infertility
- in-vitro-fertilization
- embryo quality
- reproductive medicine
Infertility is defined as the inability of a couple to achieve pregnancy after engaging in unprotected regular sexual intercourse for a year or longer, necessitating medical intervention for diagnosis and treatment. It affects around 15–25% of couples worldwide, and a significant portion of cases are classified as unexplained infertility (UI), where standard diagnostic procedures fail to identify clear causes [1, 2]. Despite the availability of advanced diagnostic tools, UI remains a significant challenge, highlighting the need for innovative prognostic tools to predict and improve the outcomes of treatments like in-vitro-fertilization (IVF) [3, 4].
The prognostic nutritional index (PNI), originally evaluates cancer patients’ nutrition and immune condition, has recently been studied for its potential to predict outcomes in various medical fields, including reproductive medicine [5, 6]. It combines serum albumin and lymphocyte measurements, which reflect nutrition status and systemic function, two factors critical to reproductive health [7]. Incorporating systemic markers into IVF outcomes can improve the accuracy of predicting IVF success and personalize treatment approaches, potentially reducing the physical, emotional, and financial burden associated with infertility treatments [8]. In that term, novel researches are expected to explain the interplay between overall health and reproductive success, offering a new framework in reproductive medicine [9, 10]. Ultimately, this could lead to more comprehensive treatment approaches that address the reproductive system and other aspects of patients’ overall health.
This study examined the PNI and inflammatory hematological parameters in non-obese couples undergoing IVF for UI by assessing embryo quality. By focusing on this well-defined group of participants, the research aimed to establish the relationship between these systemic markers and IVF success rates, with the hypothesis that optimal PNI scores and balanced hematological parameters are associated with improved reproductive outcomes.
The prospective observational cohort, including IVF applications, was conducted
at a single care center from February 2023 to December 2024. We analyzed 893
potential candidates for the study’s inclusion criteria and enrolled 198
non-obese couples diagnosed with UI according to the American Society for
Reproductive Medicine guidelines [11]. Couples were eligible for inclusion if
they had a body mass index (BMI) between 18.5 and 24.9 kg/m2 and had
undergone at least one unsuccessful cycle of IVF without a discernible cause. The
inclusion criterion of BMI between 18.5 and 24.9 kg/m2 was based on World Health Organization
(WHO) guidelines defining normal weight, ensuring a homogenous non-obese study
population. Participants were required to demonstrate adequate ovarian reserve,
defined as anti-müllerian hormone (AMH)
Standard IVF protocols were employed. Ovarian stimulation was initiated on the
second menstruation day using recombinant-FSH (r-FSH), with dosages adjusted
based on the ovary’s response analyzed via transvaginal- ultrasonography (USG)
and estradiol levels. Oocyte retrieval was performed 36 hours post-administered
human chorionic gonadotropin (hCG) when at least 2 follicles reached 18 mm in
diameter. Fertilization was conducted via conventional-IVF/intracytoplasmic
injection (ICSI), depending on quality. Controlled ovarian stimulation commenced
with recombinant FSH (150–300 IU/day) on cycle day 2. Dosages were adjusted
based on serial transvaginal ultrasound and estradiol levels. Human chorionic
gonadotropin was administered when two or more follicles reached
Samples were gained on the day of oocyte retrieval to determine hematological
profiles (Complete Blood Count, CBC, inflammatory markers) and reproductive
hormones [FSH, luteinizing hormone (LH), Estradiol, prolactin]. The formula of
PNI: 10
The outcome was the embryo quality, categorized based on morphological criteria [12]. Based on embryo quality, participants were divided into three groups: high-quality, mild, and low-quality. It included the pregnancy rate, implantation rate, take-home baby rate, and abortion rate [13]. Implantation was defined as detecting a gestational sac via ultrasound two weeks after embryo transfer. It was confirmed by fetal heartbeat detection six weeks post-transfer.
All statistical analyses were performed using SPSS version 24.0 (IBM Corp.,
Armonk, NY, USA). Hypothesis testing included independent sample
t-tests, Chi-square tests, and logistic regression models, as
appropriate. Normality assumptions were tested with the Kolmogorov-Smirnov test,
and parameters violating normality (FSH in high-quality embryos, Glucose and PNI
in mild-quality embryos, and platelet distribution width (PDW) in low-quality
embryos) were further verified using non-parametric analyses (Kruskal-Wallis).
Median values for these parameters are explicitly presented alongside mean
Age was broadly similar across the groups, and the majority in each group reported no comorbidities, unlike BMI (Table 1). Fertility outcome measures such as implantation, clinical pregnancy, take-home baby rates, and abortion rates showed no differences between the groups. High-quality embryos slightly outperformed the others in terms of clinical pregnancy and implantation rates. Similarly, the number of oocytes retrieved and the daily dosage of r-FSH used did not differ across groups.
| Variables | High-quality embryos (n = 45) | Mild-quality embryos (n = 76) | Low-quality embryos (n = 77) | p value | |
| Age, years | 31 |
30 |
31 |
0.491 | |
| BMI, kg/m2 | 24.1 |
24.7 |
23.4 |
0.006 | |
| Comorbidities | |||||
| None | 23 (51.1%) | 42 (55.3%) | 44 (57.1%) | 0.811 | |
| Present | 22 (48.9%) | 34 (44.7%) | 33 (42.9%) | ||
| History of gynecological surgery | |||||
| No | 42 (93.3%) | 70 (92.1%) | 76 (98.7%) | 0.151 | |
| Yes | 3 (6.7%) | 6 (7.9%) | 1 (1.3%) | ||
| IVF profile | |||||
| Implantation rate, % | 29.4 | 30.5 | 29.0 | 0.972 | |
| Clinical pregnancy rate, % | 43.2 | 38.6 | 41.6 | 0.877 | |
| Take-home baby rate, % | 24.4 | 25.6 | 23.0 | 0.972 | |
| Biochemical abortion rate, % | 11.9 | 10.4 | 8.8 | 0.927 | |
| Clinical abortion rate, % | 16.0 | 16.0 | 15.1 | 0.991 | |
| Total oocytes retrieved | 13 | 9 | 12 | 0.051 | |
| MII oocyte number | 10 | 7 | 9 | 0.109 | |
| MI oocyte number | 1 | 1 | 2 | 0.848 | |
| GV oocyte number | 3 | 2 | 2 | 0.494 | |
| Duration of infertility, % | 9 | 11 | 9 | 0.456 | |
| Daily r-FSH dosage, % | 232 | 256 | 247 | 0.936 | |
BMI, body mass index; IVF, in-vitro-fertilization; MII,
metaphase II; MI, metaphase I; GV, germinal vesicle; r-FSH, recombinant
follicle-stimulating hormone. Data are presented as mean
The analysis included a range of biochemical and inflammatory parameters, as
shown in Table 2, Figs. 1,2,3. Serum estradiol was lower in the low-quality
embryo group (29.0
| Variables | High-quality embryos (n = 45) | Mild-quality embryos (n = 76) | Low-quality embryos (n = 77) | p value |
| Glc, mg/dL | 102.5 |
101.4 |
94.7 |
0.351 |
| Ure, mg/dL | 30 (25–36) | 32 (25–36) | 29 (25–36) | 0.051 |
| TSH, µIU/mL | 3.36 |
3.19 |
4.14 |
0.068 |
| LH, mIU/mL | 4.8 |
5.6 |
5.2 |
0.100 |
| FSH, mIU/mL | 5.8 |
6.0 |
6.3 |
0.545 |
| E2, pg/mL | 31.0 |
31.0 |
29.0 |
0.004 |
| PRL, ng/mL | 11.6 |
13.1 |
8.6 |
0.211 |
| A-TG, IU/mL | 5.4 (0–10.2) | 5.5 (0–10.2) | 5.8 (0–10.2) | 0.079 |
| A-TPO, IU/mL | 247.5 (0–520) | 240.5 (0–520) | 252.5 (0–520) | 0.0411 |
| PLT, ×109/L | 309.0 |
288.4 |
309.5 |
0.259 |
| MPV, fL | 11.50 |
9.84 |
9.50 |
0.0001 |
| PDW, % | 15.56 |
17.48 |
19.51 |
0.427 |
| NLR, ratio | 1.77 |
1.42 |
1.68 |
0.078 |
| MLR, ratio | 0.18 |
0.19 |
0.21 |
0.326 |
| PLR, ratio | 110.80 |
104.30 |
131.87 |
0.015 |
| MII-1, ratio | 8.01 |
9.33 |
14.14 |
0.001 |
| MII-2, ratio | 539 (180–880) | 510 (180–880) | 524 (180–880) | 0.121 |
| PNI, ratio | 51.65 |
48.10 |
44.20 |
0.0001 |
| SIRI, ratio | 544.1 |
420.4 |
535.1 |
0.053 |
| SII, ratio | 0.85 |
0.75 |
0.87 |
0.455 |
Glc, glucose; Ure, urea; TSH, thyroid stimulating hormone; LH, luteinizing
hormone; FSH, follicle stimulating hormone; E2, estradiol; PRL, prolactin; A-TG,
anti-thyroglobulin; A-TPO, anti-thyroid peroxidase; PLT, platelet count; MPV,
mean platelet volume; PDW, platelet distribution width; NLR,
neutrophil-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; PLR,
platelet-to-lymphocyte ratio; PNI, prognostic nutritional index; SIRI, systemic
inflammation response index; SII, systemic immune-inflammation index. Data
distribution was assessed using the Kolmogorov-Smirnov test. Variables with high
standard deviations relative to their means (suggesting non-normal distribution
or heterogeneity of variance)—including Glucose, Ure, FSH (in high-quality
embryos), MPV, A-TG, A-TPO, PDW, MII-2, PNI (in mild-quality embryos), and
SIRI—are presented as median (interquartile range, IQR). Kruskal-Wallis test
was applied for these variables. For normally distributed variables with unequal
variances, Welch’s ANOVA test was used. Remaining variables were analyzed using
classical one-way ANOVA. A p-value
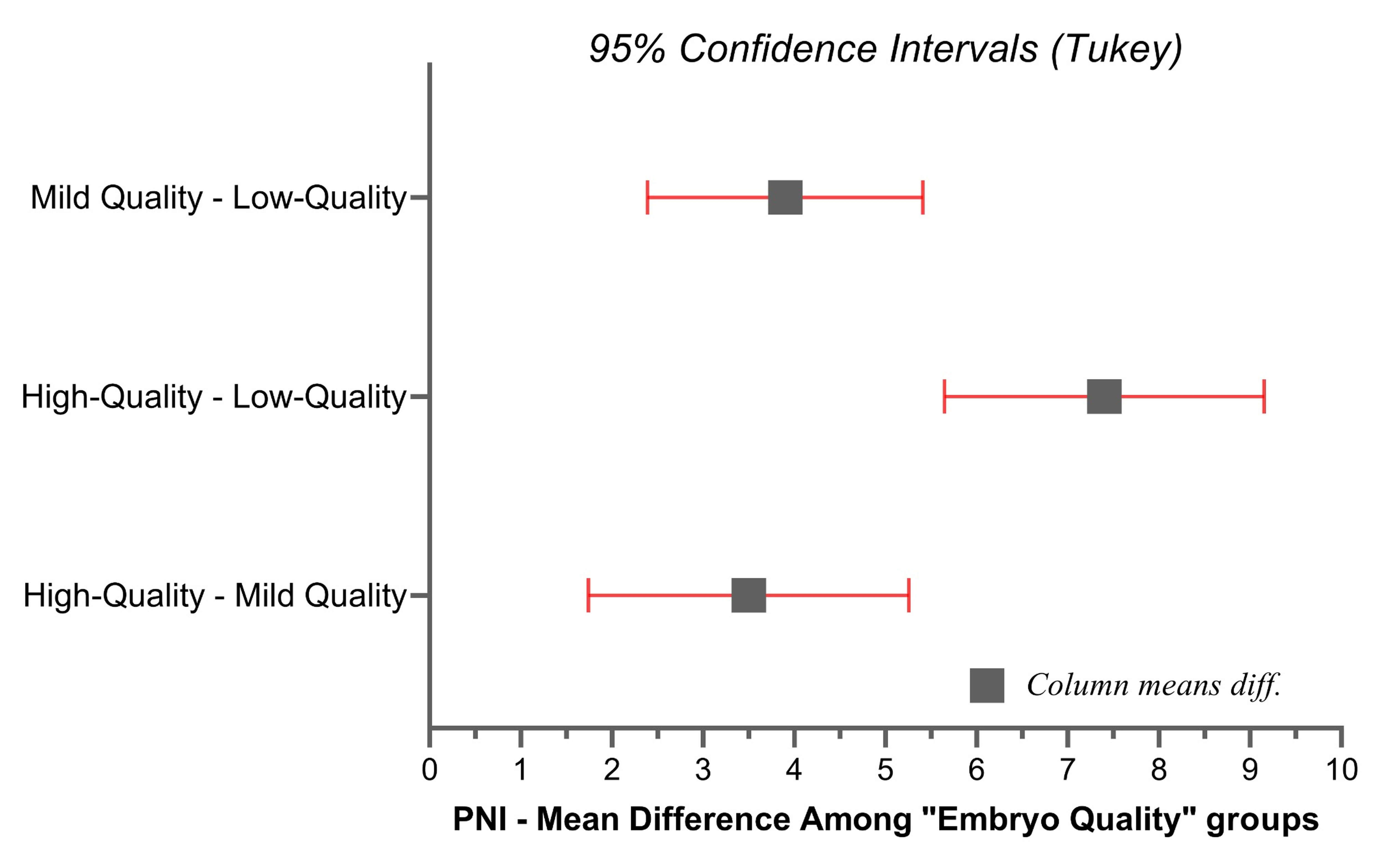 Fig. 1.
Fig. 1.
The mean difference of PNI according to the embryo quality.
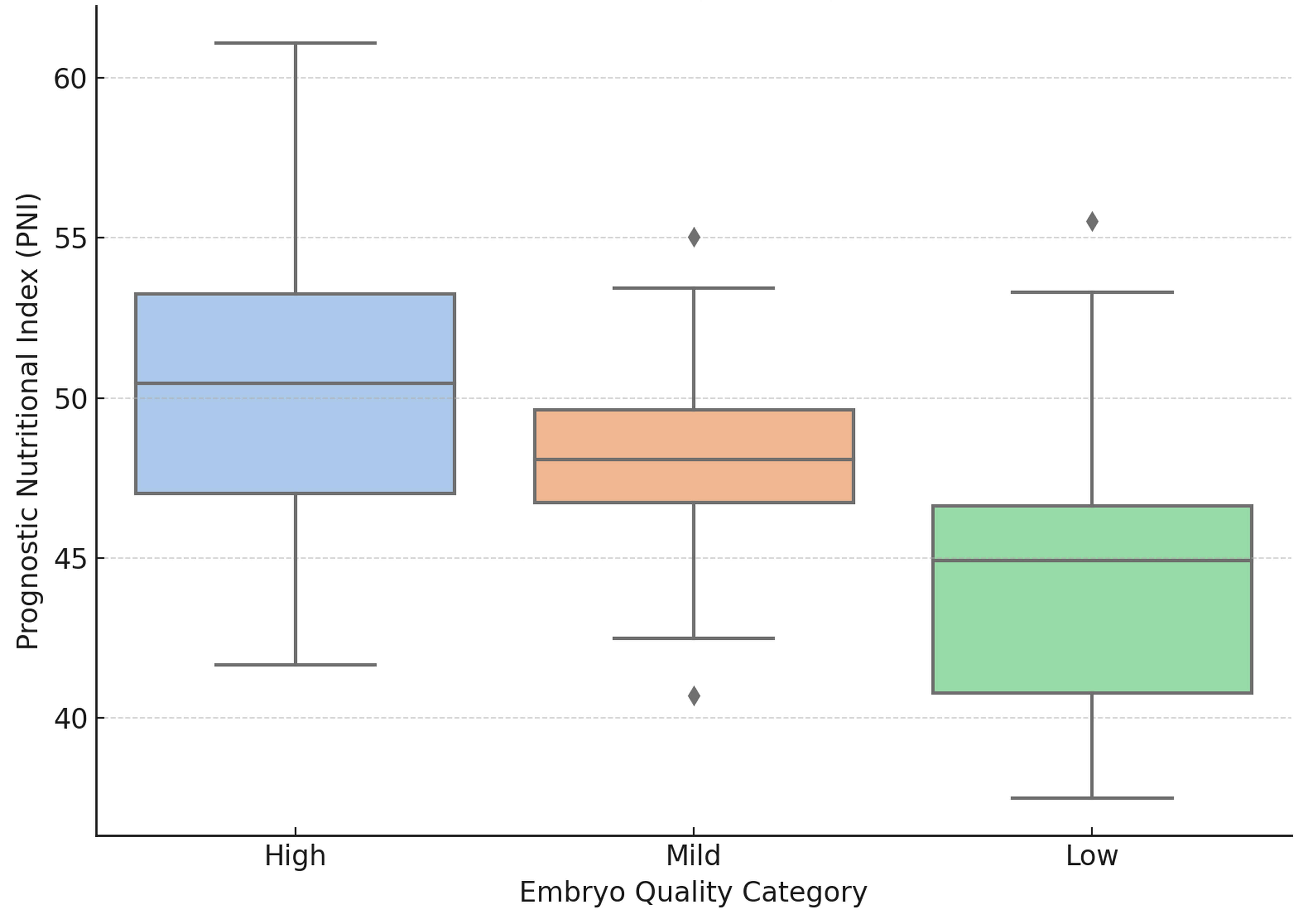
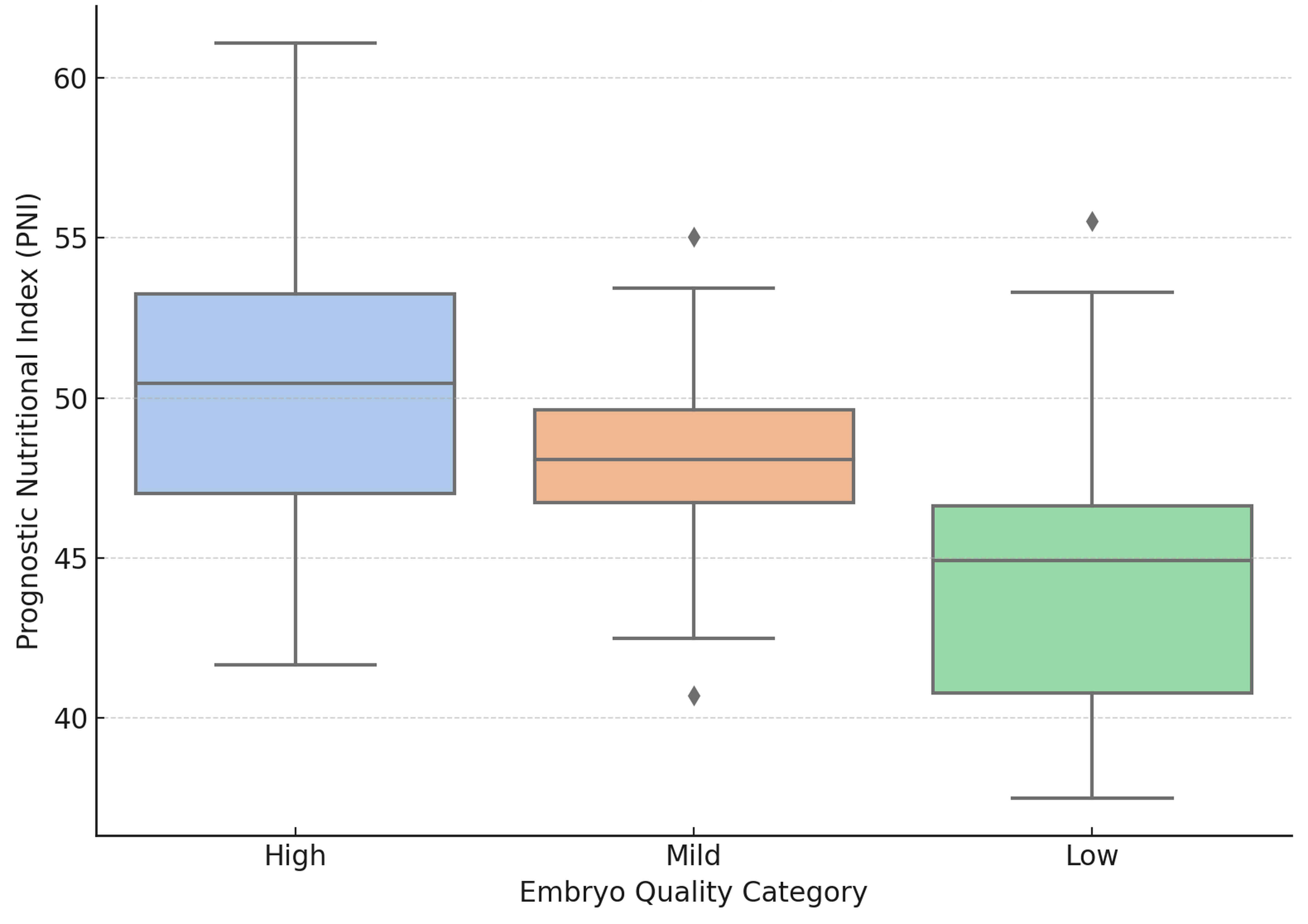 Fig. 2.
Fig. 2.
PNI distribution by embryo quality. Boxplots show the median,
IQR, and overall range. Diamond symbols represent outlier
values outside the 1.5
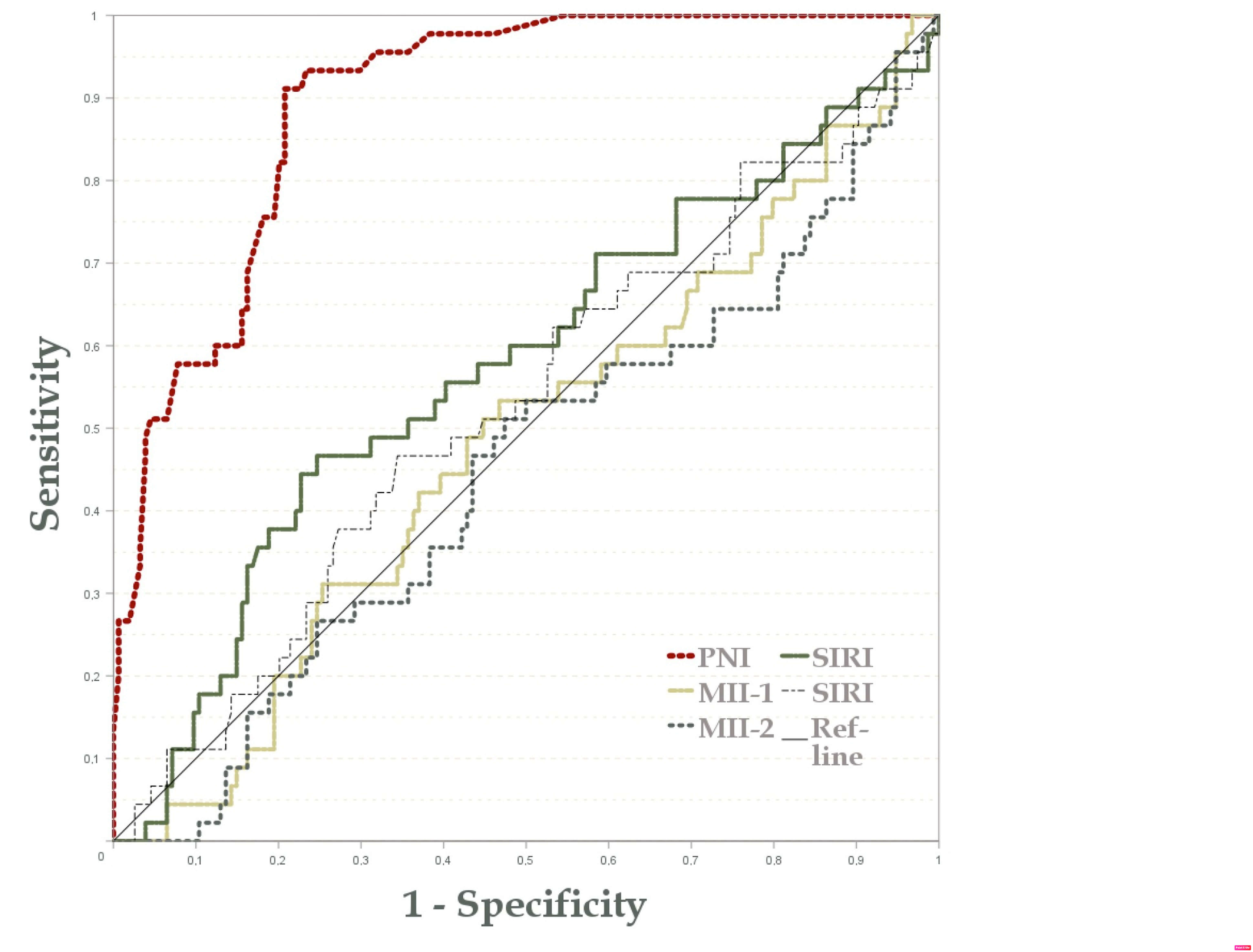
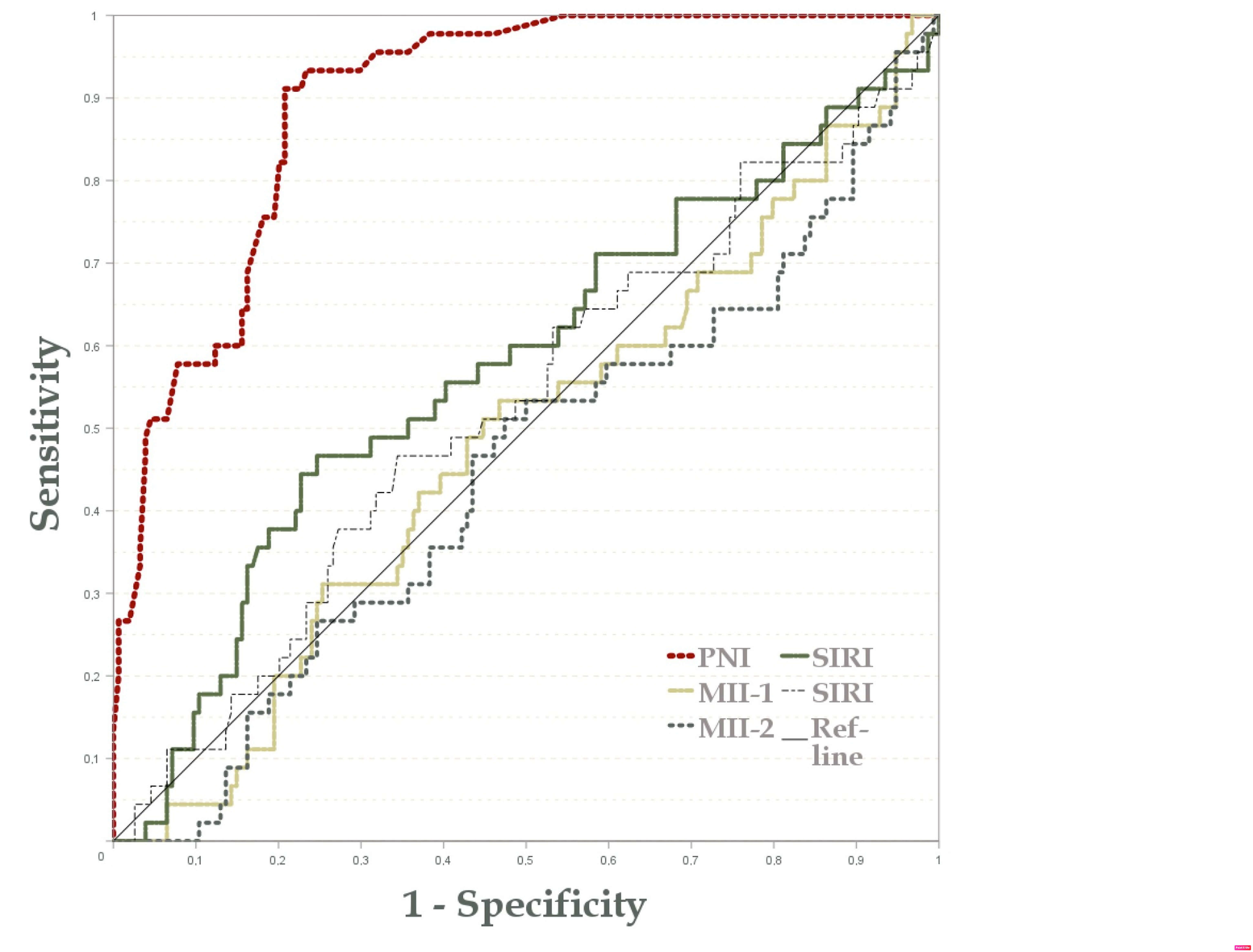 Fig. 3.
Fig. 3.
The ROC analysis of PNI for high quality embryo. ROC, receiver operating characteristic.
In a stepwise regression analysis evaluating factors influencing embryo quality, three models were developed, progressively incorporating the PNI, age, and biochemical abortion rate as predictors. PNI showed a positive impact on embryo quality, with a coefficient of –0.098, a standard error of 0.019, a Beta of –0.560, and a highly significant t-value of –5.132 (p = 0.001). Excluded variables that did not meet the inclusion criteria for the final models included NLR, MLR, PLR, MII-1, MII-2, SII, and SIRI due to their limited additional explanatory power. In the refined logistic regression model, as given in Table 3, the analysis revealed relationships between “Embryo quality”, “Implantation” and PNI classifications (lower or higher than 52 value), particularly useful in clinical settings. Since PNI was measured on the day of oocyte retrieval and precedes embryo assessment, the regression results indicate that a higher PNI significantly increases the likelihood of achieving better embryo quality (OR = 11.859, p = 0.0001), rather than embryo quality influencing PNI. Clinically, good embryo quality was strongly linked to a favorable nutritional status, making it a critical factor for patient assessment. The odds ratio for implantation percentage was 1.077. This finding implied that for each 1% increase in the implantation rate, there was a 7.7% higher chance of the patient falling into the higher PNI (p = 0.0234).
| Variables | Β-Coefficient | S.E. | Wald | Exp (B) | 95% CI | p value |
| Implantation (%) | 0.074 | 0.032 | 5.205 | 1.077 | 1.01 to 1.147 | 0.0234 |
| Embryo quality | 2.473 | 0.572 | 18.721 | 11.859 | 3.868 to 36.35 | 0.0001 |
| Constant | –10.444 | 2.055 | 25.828 | - | - | 0.0001 |
“B” denotes the Beta Coefficient, indicating the effect of predictors on the outcome. “S.E.” represents the Standard Error of this estimate, while “Wald” is a statistic testing the significance of coefficients. “Exp (B)” is the exponential of the Beta Coefficient, showing the multiplicative effect on the outcome. The “95% CI” provides the confidence interval for this effect, and the “p value” indicates the significance of the findings, with values below 0.05 typically considered significant. Variables were entered sequentially in the regression model: Embryo quality at Step 1 and Implantation percentage at Step 2.
The PNI yielded an area under the curve (AUC) of 0.895 (p = 0.001, 95% CI: 0.85–0.94), indicating a robust discriminatory ability (Fig. 3). Conversely, the MII-1 and MII-2 indices exhibited AUCs of 0.482 and 0.449, respectively, failing to reach significance (MII-1: p = 0.72; MII-2: p = 0.303). The SIRI was analyzed using two different measurements, producing AUC values of 0.574 and 0.525, with neither yielding results (p = 0.130 and p = 0.607, respectively). Despite showing moderate AUCs, these values imply limited predictive value for SIRI in this context. In addition to the high AUC observed for the PNI, a cutoff value of 46.5 was determined to yield an optimal balance of sensitivity and specificity. At this threshold, PNI demonstrated a sensitivity of 81.2% and a specificity of 80.1%, further underscoring its potential as a reliable discriminative marker.
The study focused on the significance of PNI and hematological inflammatory profiles in forecasting the outcomes of IVF interventions among non-obese couples who are grappling with unexplained infertility. Optimum nutritional and immunological status, gauged by well-balanced hematological parameters and PNI, is strongly linked to enhanced embryo quality and IVF triumph. These observations corroborate the considerable influence of overall health on reproductive outcomes and suggest that incorporating comprehensive health assessments could fortify patient classification and tailor treatment strategies within reproductive medicine.
In the context of IVF, immune inflammation is critical in the prognosis of multiple cancers and reproductive medicine. A 2024 cohort study of women undergoing IVF with a gonadotropin-releasing hormone (GnRH) antagonist protocol found that elevated SII values were significantly associated with poorer outcomes—including lower biochemical pregnancy, clinical pregnancy, implantation, and live birth rates—even after adjusting for age, BMI, AMH, and stimulation parameters. Notably, women in the highest SII quartile had the worst IVF outcomes, suggesting that a higher pre-IVF inflammatory state may negatively impact implantation and pregnancy success [14]. Indices such as PNI, SIRI, and SII [15]—typically studied within the framework of oncological research—offer information about the immune and nutritional factors that affect IVF. PNI effectively combines albumin with lymphocytes and reflects an individual’s nutrition and immunological status [16]. The immune environment of the endometrium holds considerable sway over the success rate of embryo implantation. Lymphocytes are pivotal in maintaining the immune equilibrium required for successful implantation and early pregnancy [9, 17].
SIRI and SII—a systemic inflammation marker derived from platelet, neutrophil, and lymphocyte counts in peripheral blood—may possess relevant implications for reproductive health assessment [18, 19]. Elevated systemic inflammation levels, denoted by a high SII, can unfavorably impact ovarian function, embryo quality, and endometrial receptivity [19]. In a 2024 retrospective cohort, investigators evaluated various baseline inflammatory markers [including NLR, platelet count, PLR, C-reactive protein (CRP), etc.] in IVF patients [20]. They found that lower NLR was strongly predictive of successful pregnancy outcomes after IVF. In multivariate analysis, NLR emerged as an independent predictor of achieving pregnancy with higher NLR associated with decreased odds of pregnancy, whereas other markers like PLR or CRP did not retain independent. NLR is a robust prognostic indicator for IVF success, reinforcing the idea that a lower systemic inflammatory state lower NLR favors implantation. Another research published on UI provides insight into immune-nutritional indices in IVF. That study reported that higher levels of systemic inflammation indices were associated with poorer oocyte and embryo development in IVF. Women with elevated SII/SIRI had higher rates of embryo arrest and required higher gonadotropin doses, indicating an adverse intra-ovarian environment [21].
As an index, PNI was validated as a prognostic potential in oncology studies [19, 22]. However, their potential role in predicting IVF success brings about an intriguing convergence of nutrition, inflammation, and reproductive medicine. In our analysis, PNI demonstrated noteworthy variations, while most biochemical markers did not exhibit significant differences across groups. The decline in PNI from high to low embryo quality implies a direct association between nutritional and immunological well-being and embryo viability. Our regression analyses supported this inverse relationship between PNI and embryo quality, indicating that a lower PNI, indicative of inferior nutritional and immune status, is linked to diminished embryo quality. This index may be attributed to the pivotal functions of albumin and lymphocytes, components of PNI, in establishing a favorable physiological environment for embryo implantation and development.
Moreover, our stepwise regression models demonstrate the robust predictive capacity of PNI in comparison to other inflammatory indices. The NLR, MLR, SII, SIRI, and PLR failed to meet the inclusion criteria due to limited explanatory power, underscoring the utility of PNI as a comprehensive and predictive index for IVF outcomes. The logistic regression findings further corroborate the significant impact of embryo quality on PNI classifications. Because PNI was measured on the day of oocyte retrieval and therefore precedes embryo assessment, the observed association indicates that lower PNI reflects a less favorable nutritional and immune profile that is subsequently linked with poorer embryo quality—rather than embryo quality exerting any influence on PNI. From a clinical standpoint, monitoring it could be helpful to as a valuable tool for embryo quality and comprehending the overall health status of IVF patients.
The primary strength of this study lies in its systematic approach to investigating the interplay between nutritional and immunological statuses represented by PNI and their influence on IVF outcomes. Our findings underscore the intrinsic connection between systemic health and reproductive success by controlling for confounding and comorbidities. However, it is important to acknowledge several limitations. One limitation of our model is the exclusion of hormone levels measured on the trigger day, such as serum estradiol or LH, which may have potential predictive value. These parameters were not available for all cases, limiting their inclusion in a multivariate framework. Longitudinal studies would better determine the temporal relationship and causal pathways. Additionally, while we controlled for various demographic and clinical variables, other unmeasured confounders may impact nutritional and reproductive outcomes, including lifestyle factors, dietary habits, or genetic predispositions. Given that prolactin levels showed no statistically significant variation among the embryo-quality groups, the current findings do not support any inference about its regulatory or predictive relevance in this context. It is also important to note that the study population may not represent all IVF patients, potentially limiting the generalizability. Future longitudinal studies are necessary to investigate the long-term effects of PNI on pregnancy success, neonatal health, and live birth outcomes, which would broaden the clinical relevance.
The study underscored PNI in monitoring the outcomes of IVF treatments among non-obese couples experiencing unexplained infertility. PNI was directly correlated with embryo quality, and a low PNI, indicative of poor nutritional and immune status, was associated with reduced embryo quality. In contrast, other inflammatory indices such as NLR, MLR, SII, SIRI, and PLR exhibited limited effectiveness compared to the potential of PNI. Clinically, monitoring PNI can serve as a valuable and predictive parameter for analysis of embryo quality and understanding the overall health status of IVF patients.
The data supporting the findings are available from the corresponding author upon reasonable request.
AY, TG and HCO designed and conceptualized the study, as well as conducted data collection and analysis. AY prepared the initial manuscript draft, while TG and HCO reviewed and approved the final version. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
IRB Registration: Reviewed and approved by the Non-Interventional Research Ethics Committee of Bezmialem University. The ethical approval number is E-54022451-050.04-153868, dated 10 June 2022. Informed consent was obtained from all participants included in the study. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
During the preparation of this manuscript, the authors utilized ChatGPT-3.5 solely for grammar and language polishing. The authors thoroughly reviewed, edited, and revised the manuscript and take full responsibility for its content.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.