








 , Sorana Muresan 1
, Sorana Muresan 11 Promama Center Association, Lactation Institute, and Breastfeeding Center, 400910 Cluj-Napoca, Cluj, Romania
Abstract
Forceful milk ejection reflex in mothers and tongue-tie in infants often cause breastfeeding difficulties. Our purpose was to observe the breastfeeding behavior of tongue-tied neonates, in the presence of forceful milk ejection of their mother versus tongue-tied infants without forceful milk ejection or in the presence of forceful milk ejection in non-tongue-tied infants.
This is an observational, prospective, cohort study. The study was undertaken at the Lactation Institute, in Cluj-Napoca, Romania, between 2012 and 2018. We studied the breastfeeding behavior of neonates attending the Institute. The study includes 80 tongue-tied new-borns of mothers with forceful milk ejection (Group I), compared with the breastfeeding behavior of 40 tongue-tied neonates of mothers with normal let-down (Group II) and 29 neonates without tongue-tie in the presence of forceful let-down (Group III). Descriptive statistics, including numbers and percentages, and SAS software were utilized. Categorical data are presented as counts and percentages and analyzed with chi-square tests, utilizing R and Python software. Statistical significance was set at p-value ≤ 0.001, in some cases at p-value ≤ 0.05 using a chi-square test, sometimes validating the results with Fisher’s Exact Test. Proportional Analysis and Post-Hoc Analysis (pairwise Z-tests for proportions) were also carried out to demonstrate the frequency of cases.
From Group I, the majority (92.50%) were breastfed effectively in the first week, significantly different from infants in Group II (20%), where frenotomy was more frequent (92.50%) and performed mainly for suckling difficulties (86.48%). The difficult latch had a higher percentage in infants in Group II (92.50%). “Reflux-like syndrome” (93.10%), breast refusal (24.13%), and, choking (93.10%) were more frequent in infants in Group III.
The majority of tongue-tied infants, whose mothers had early forceful milk ejection, were able to effectively breastfeed after birth. In this cohort, frenotomy might not be necessary or could be postponed. The presence of tongue-tie only, without fast milk flow, led to suckling difficulties and the need for frenotomy. Reflux-like syndrome, choking, and breast refusal were more present in infants without tongue-tie but with fast milk flow.
Keywords
- neonates
- forceful milk ejection
- tongue-tie
- breastfeeding
- suckling difficulties
Forceful milk ejection and tongue-tie often contribute to breastfeeding difficulties [1]. The association of these has not been studied. Lingual frenotomy is widely indicated by healthcare professionals, in case of tongue-tie often without clear evidence of serious breastfeeding problems [2]. Our purpose was to observe the breastfeeding behavior of tongue-tied neonates in the presence of forceful milk ejection of their mother versus tongue-tied neonates without forceful milk ejection, or in the presence of forceful milk ejection in non-tongue-tied neonates.
Forceful Milk Ejection Reflex (MER) involves a forceful release of milk during infant suckling, a fast ejection, resulting in spraying [1] of the milk from the mother’s nipple. While common among primiparas [1], the exact cause of forceful MER, possibly linked to an unusually strong reaction to oxytocin [3], remains unknown. Overactivity of MER is normal in early lactation but tends to diminish [1] over time. Some authors have stated that it normally slows somewhere between 3 weeks to 3 months [4]. However, for some mothers, fast flow persists [5], potentially leading to issues such as breast refusal and weaning [4, 5]. During nursing, fast milk flow causes rapid swallowing [5], incoordination of suck-swallow-breath [3, 6], choking, and apnea [7]. Babies ma y attempt to control the flow by gently compressing the nipple, leading to nipple pain [3, 8] and a shallow latch [3]. The spraying of milk can result in the baby swallowing air [9], leading to choking, coughs [1], “reflux-like syndrome” [4], and, short [6], frequent suckling episodes. In such cases, feeding at the breast is stressful, and often the baby is struggling [9] with the high flow. Forceful MER is often associated with oversupply [9].
Ankyloglossia (Tongue-tie) is characterized by a tight lingual frenulum that restricts tongue mobility [10]. Recent anatomy research suggests that a tight fascia may be responsible for this restriction [11, 12] and the diagnosis of tongue-tie is based on clinical examination [13]. Considering that the neonatal oral structure is variable in appearance [14], there is a lack of a consistent classification system for clinically significant ankyloglossia [6]. Most classifications are based on appearance [15], while only a few take into account functionality [8, 16].
Over the last decade, the literature has distinguished between “anterior” and “posterior” tongue-ties [17]. Anterior tongue-tie (type 1 and type 2) [15] is characterized by insertion at the tip of the tongue (type 1) or slightly behind (type 2) [18]; posterior tongue-tie is characterized by a thickened frenulum (type 3), attached at mid-tongue but most authors refer to “posterior tongue-tie” as a submucosal frenulum (type 4), attached to the floor of the mouth at the base of the tongue [2], appreciated by palpation [17]. “Posterior tongue-tie” may be more difficult to diagnose [6, 15, 19, 20].
Some authors consider that in many children, ankyloglossia is asymptomatic or symptoms may resolve spontaneously, as babies learn to compensate for decreased lingual mobility [21]. In others, tongue-tie may lead to breastfeeding difficulties [6, 22, 23], maternal nipple pain [2, 24, 25], and early weaning [2, 24]. The nature of tongue-tie-associated breastfeeding difficulties is poorly defined [18] and controversy exists about when sublingual tissue is the actual cause of clinical dysfunction [20].
The restrictive lingual frenulum has been described to produce restricted tongue mobility [2, 6, 26], causing shallow latch [24]. Ultrasound studies observed two different sucking dynamics: some infants pinched the tip of the nipple, having difficulty maintaining a seal to the breast and some infants pinched the nipple at the base, biting and strongly latching, both causing nipple trauma [23]. Poor latch results in aerophagia [27], “reflux-like syndrome”, problems in coordination of swallowing [2, 6, 26, 28], choking, and fussy babies [26].
In the case of restrictive tongue-tie, some healthcare professionals refer the infant for surgery. Others indicate conservative management, consisting of modifying the latch and position, the temporary use of nipple shields and, expressed breast milk for supplementation when necessary [11], exercises to help improve tongue motion, and maintaining a full milk supply [17]. However, there are limited studies regarding the efficacy of nonsurgical strategies [11]. Surgical interventions include frenotomy, frenulectomy, and frenuloplasty.
Frenotomy is a non-invasive release of the frenulum with scissors [18], with few adverse effects and minimal aftercare. It can be performed with laser surgery, which, in the opinion of some authors, has unintended outcomes but is recommended in cases of thickened and vascularized frenulum [18]. However, several studies have documented breastfeeding difficulty, questioning the effectiveness of frenotomy [13, 22]. A systematic review conducted by the Cochrane Collaboration shows weak evidence that frenotomies benefit breastfeeding babies [29].
Other surgical procedures, in addition to frenotomy, include frenuloplasty and frenectomy. Frenuloplasty involves plastic surgery of the frenulum. Frenectomy is the complete surgical removal of the frenum.
Lip–tie is a tight superior labial frenum and, according to some authors, it may be an unusual source of sucking problems [30]. For the diagnosis of Lip-tie, Kotlow [30] made a classification in newborns. According to Mohan et al. [31], the upper lip frenums from Kotlow’s classification are all normal maxillary labial frenums. The role of the upper lip during breastfeeding is limited, as during suckling the upper lip needs only be in a neutral position [17].
This is an observational, prospective, cohort study. The protocol to study human subjects was approved by the Local Ethics Committee (approval No. 2/C.E./10.04.2011). Informed consent was signed by all mothers participating in the study. The study was undertaken at the Lactation Institute in Cluj-Napoca, Romania, between 2012 and 2018.
We examined the breastfeeding behavior of 149, healthy, exclusively breastfed, term neonates and their mothers. Infants were referred to the Institute in the first week after birth, by an International Board Certified Lactation Consultant (IBCLC) for breastfeeding difficulties. We recruited primipara, secundipara, and multipara mothers with forceful MER, having infants with or without tongue-ties, and mothers with normal MER having tongue-tied neonates. Subjects were categorized into three groups: Group I, 80 tongue-tied neonates and their mothers with forceful MER; Group II, 40 tongue-tie newborns with mothers with normal MER, and Group III, 29 newborns without tongue-ties but with mothers with forceful MER. Exclusion criteria included neonates with perinatal complications (asphyxia, birth trauma, sepsis), visible genetic syndrome, craniofacial anomalies, muscular or neurologic deficits, and mothers with breast or nipple anomalies.
Our Protocol consisted of:
(1) Consultation of our subjects, in the first week after birth:
(a) Completion of a questionnaire (Appendix 1) covering perinatal history, infant and mother’s health, and breastfeeding-related questions.
(b) Global assessment and visual and digital oral examination of the infant by a Pediatrician.
(c) Assessment of the mother’s breast and the MER by an IBCLC.
(d) Assessment of suckling and milk intake by an IBCLC.
(2) Follow-up:
(a) Phone call, 24 hours after the visit to record daily milk intake.
(b) Weekly calls during the first month for breastfeeding-related questions.
(c) Follow-up visits at the request of mothers.
Forceful MER was considered after ruling out other causes when: the milk was spraying far from the breast (Fig. 1); fussy suckling, choking, shallow latch, and frequent feeding interruptions. Hyperlactation was not specifically considered.
 Fig. 1.
Fig. 1.
Forceful milk ejection.
Tongue-tie was defined as a tight lingual frenulum. Identification involved visual and digital examination, including the “Murphy maneuver” for assessing posterior ankyloglossia [32]. Descriptive classification followed Corryllos’ criteria [19].
Tongue Function Assessment: Evaluated using the first three items (lateralization, lift, and extension of the tongue) from the Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF) [16]. A cutoff of less than or equal to 4 was used based on Amir et al.’s [13] recommendation for frenotomy, which has high sensitivity and specificity.
We evaluated other studies [22, 33] recommending frenotomy in case of inadequate milk transfer, severe maternal nipple pain, difficult latch, excessive crying, and parental request. Frenotomy was conducted by a qualified provider in specialized ambulatory settings using scissors or, in some cases, laser surgery. No complications occurred apart from a case of sublingual abscess after scissor division, with Streptococcus Agalactie from the skin of the mother’s breast, and a case of mouth aversion after laser treatment. Frenotomy’s impact on breastfeeding problems was not specifically observed.
Superior Lip Frenulum: The superior lip frenulum was also examined in the neonates included in the study. This was assessed using L. Kotlow’s Classification: Class 1 lip attachment requires no treatment, Class 2, attaching at the junction free and attached gingival tissue, Class 3, attaching just in front of the anterior papilla; Class 4 attachment into the anterior papilla, extending into the hard palate [30]. Classes 2, 3, or 4 may contribute to breastfeeding problems and should be evaluated for revision [30]. Considering that classes 3 and 4 are of higher severity, we counted only the anterior insert upper lip frenulum. According to several authors [31, 34] what Kotlow refers to as a “lip-tie” in newborns, is a normal superior lip frenulum. Therefore, we considered that it did not require treatment.
Breastfeeding Behavior Assessment: Recorded parameters included effective breastfeeding, difficult latch, shallow latch, reflux-like syndrome, breast refusal, choking, suckling difficulties, and mother’s nipple pain.
Effective Breastfeeding was defined as adequate milk intake measured by test-weighing the baby for 24 hours. Adequate daily milk intake thresholds were established at various infant ages: a minimum of 230 mL at 4 days [35], 350 mL at 5 days [35], 550 mL at 6 days [35], and 600 mL at 7 days of age [22].
The difficult latch was defined as a failure to stay attached to the nipple and shallow latch as a narrow gape.
The “reflux-like syndrome” consisted of frequently spitting up.
We identified suckling difficulties, including ineffective suckling and latching issues.
We documented follow-up visits.
A comparative analysis was conducted of the results among the three groups and a separate analysis of all tongue-tied infants from Groups I and II.
Data was collected adhering to Directive (EU) 2016/680 and Romanian Law 190/2018, with informed consent from participants, during visits to the Institute and subsequent phone calls by the study author and co-author. Participants’ confidentiality is maintained for ten years at the Institute’s archive.
Descriptive statistics, including numbers and percentages, and SAS 9.4 software,
SAS Institute Inc., Cary, North Carolina, USA were utilized. Categorical data are
presented as counts and percentages and analyzed with chi-square tests, utilizing
R, 4.2.0, R Foundation for Statistical Computing, Vienna, Austria and Python 3.8,
(SciPy 1.7.1/Stats models 0.12.2) software, Python Software Foundation,
Wilmington, Delaware, USA. Statistical significance was set at p-value
In Groups I and II, the majority of infants had anterior tongue-tie (78.33%), potentially due to difficulties in identifying tongue-tie type 3 and type 4 (Fig. 2). Of 120 tongue-tied neonates, almost half (45%) underwent lingual frenotomy (Table 1), 72.22% in the first week after birth, and 27.78% after 7 days postpartum (Fig. 3). Of infants who underwent frenotomy, the majority had anterior tongue-tie (90.74%), and only a few (9.25%) presented with tongue-tie type 3 and none with tongue-tie type 4 (Table 1).
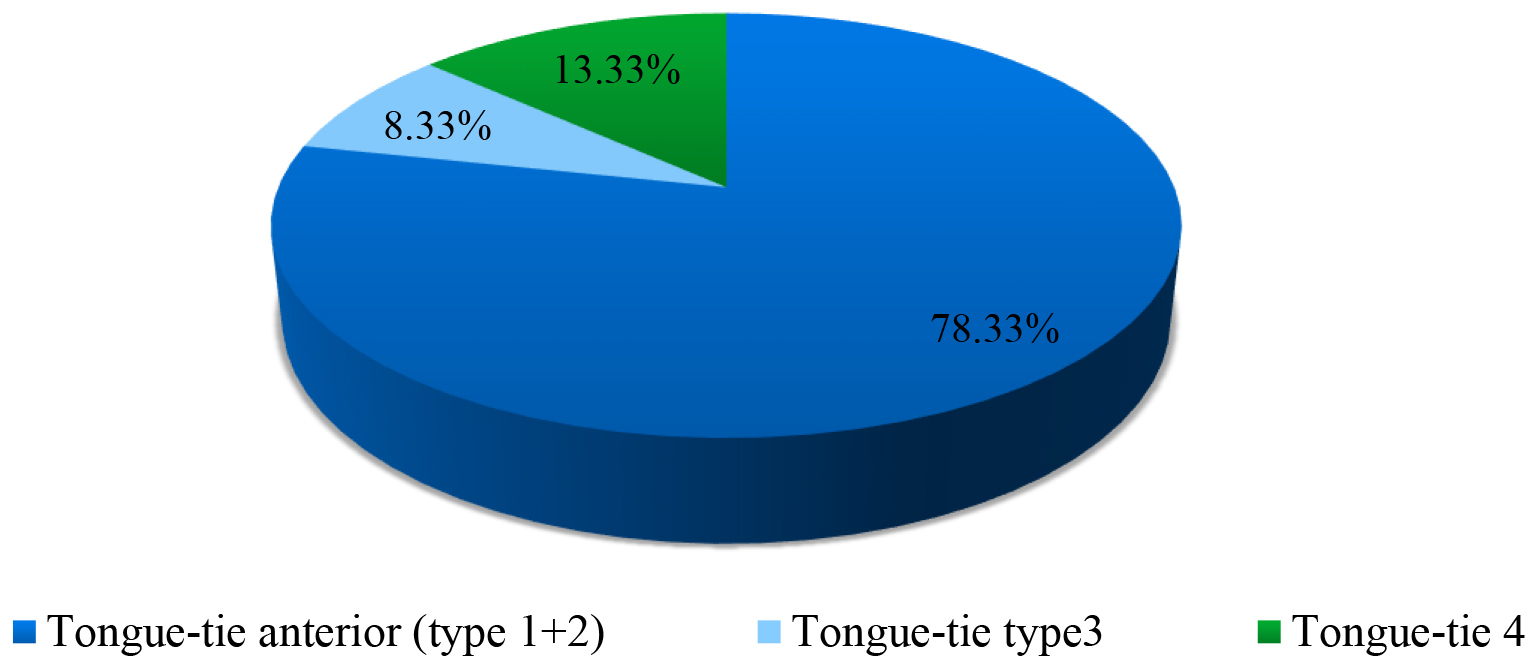 Fig. 2.
Fig. 2.
Total tongue-tied neonates.
| Frenotomy | Effective breastfed | Difficult latch | Shallow latch | Reflux like syndrome | Breast refusal | Choking | Nipple pain | |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |
| Total Tongue-tied Infants N:120 | 54 (45) | 82 68.33) | 43 (35.83) | 57 (47.50) | 8 (6.66) | 8 (6.66) | 3 (2.50) | 33 (27.5) |
| Tongue-tie anterior (Type 1+2) | 49 (90.74) | 41 (95.34) | 27 (81.81) | |||||
| Tongue-tie Type 3 | 5 (9.25) | 2 (4.65) | 3 (9.09) | |||||
| Tongue-tie Type 4 | 0 | 0 | 3 (9.09) | |||||
| χ2 | 15.12 | 12.50 | 0.716 | |||||
| p |
0.00052* | 0.00193 | 0.699 |
Note: *, statistically significant; χ2, chi-square.
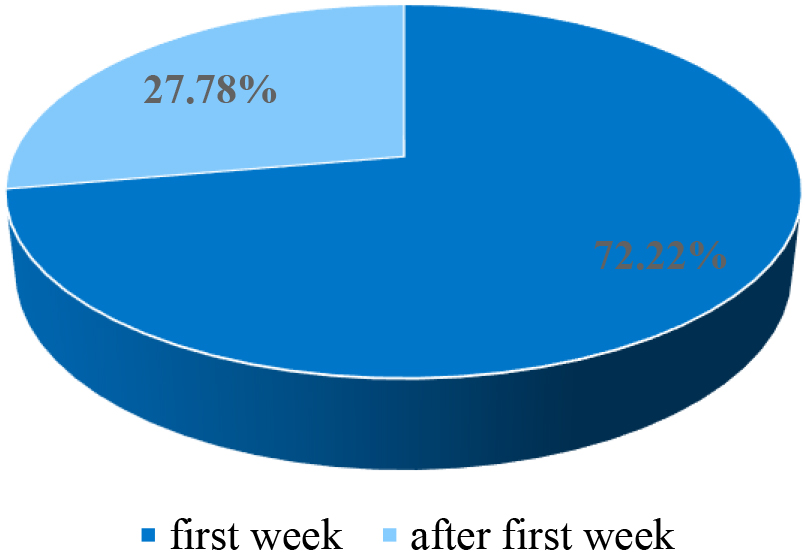 Fig. 3.
Fig. 3.
Timing of fretonomy.
In Group I, frenotomy was less frequent (21.25%) than in infants from Group II
(92.50%), with differences being significant for p
| Frenotomy | Frenotomy at follow-up visit |
Frenotomy for nipple pain | For suckling difficulties | |
| N (%) | N (%) | N (%) | N (%) | |
| Total Tongue-tied Cases N:120 | 54 (45) | 15 (27.77) | 16 (29.62) | 38 (70.37) |
| Group I Tongue-tie + forceful MER N:80 | 17 (21.25) | 9 (52.94) | 11 (64.70) | 6 (35.29) |
| Group II Tongue-tie N:40 | 37 (92.50) | 6 (16.21) | 5 (13.51) | 32 (86.48) |
| χ2 | 51.856 | 0.0086 | 12.28 | 12.29 |
| p |
5.97 |
0.770 | 0.000456* | 0.00046* |
Note: *, statistically significant; χ2, chi-square; MER, Milk Ejection Reflex.
Of all neonates studied, the majority (97.99%) had a Superior lip frenulum inserted anteriorly (Fig. 4).
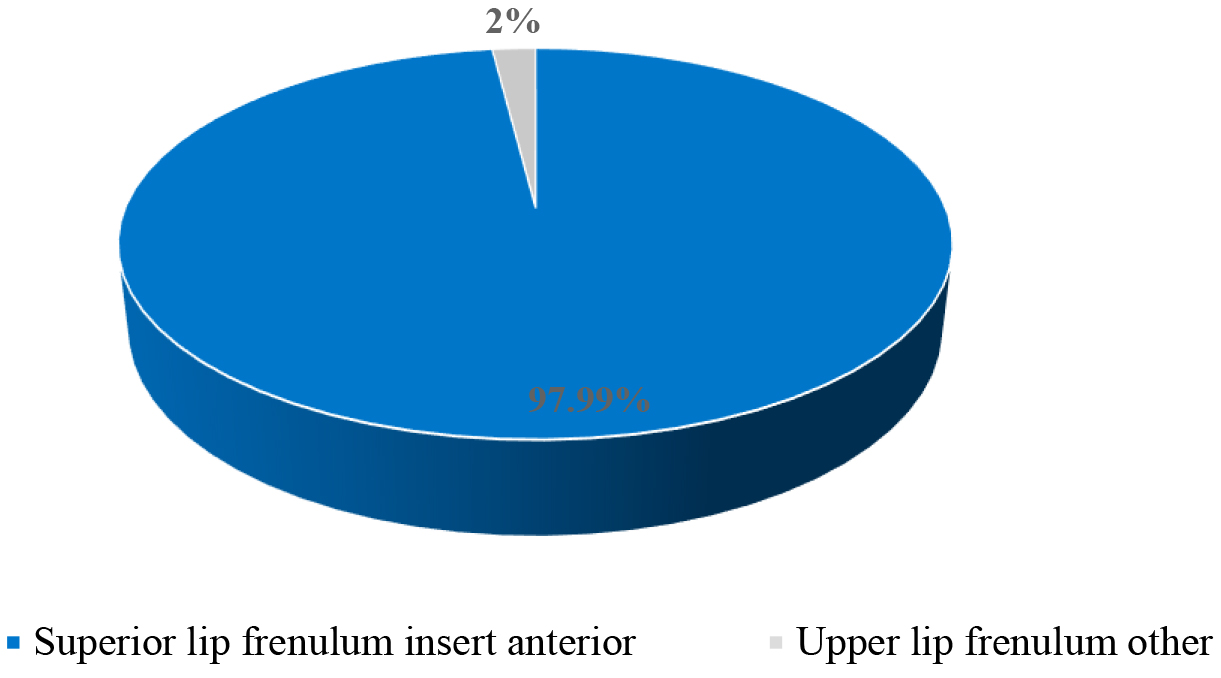 Fig. 4.
Fig. 4.
Superior lip frenulum per groups.
In our study, the Hazelbaker functional score modified by Amir et al.’s [13]
revealed that from the total number of tongue-tied infants (N = 120), 49.16% had
a score
| H. Score |
H. Score = 4 | Sum H. Score |
H. Score | |
| N (%) | N (%) | N (%) | N (%) | |
| Total Tongue-tie (Group I + Group II) N = 120 (100%) | 52 (43.33) | 7 (5.83) | 59 (49.16) | 61 (50.83) |
| Group I Tongue-tie + forceful MER | 20 (38.46) | 5 (71.42) | 25 (42.37) | 55 (90.16) |
| Group II Tongue-tie | 32 (61.53) | 2 (28.57) | 34 (57.62) | 6 (9.83) |
| χ2 | 28.71 | 28.71 | ||
| p |
8.40 |
8.40 | ||
| Frenotomy (Group I + Group II) | 38 (73.07) | 4 (57.14) | 42 (71.18)** | 12 (19.67) |
| Frenotomy Group I | 9 (21.42) | 8 (66.66) | ||
| Frenotomy Group II | 33 (78.57) | 4 (33.33) | ||
| χ2 | 23.29 | 6.29 | ||
| p |
1.39 |
0.0121 | ||
| Frenotomy in the first week | 36 (85.71) | 3 (25) | ||
| Frenotomy after the first week | 6 (14.28) | 9 (75) |
Note: H. Score, Hazelbaker Score; *, statistically significant; χ2,
chi-square; **, p significant for
 Fig. 5.
Fig. 5.
Sum Hazelbaker Score
Of total tongue-tied infants, 50.83% presented with scores
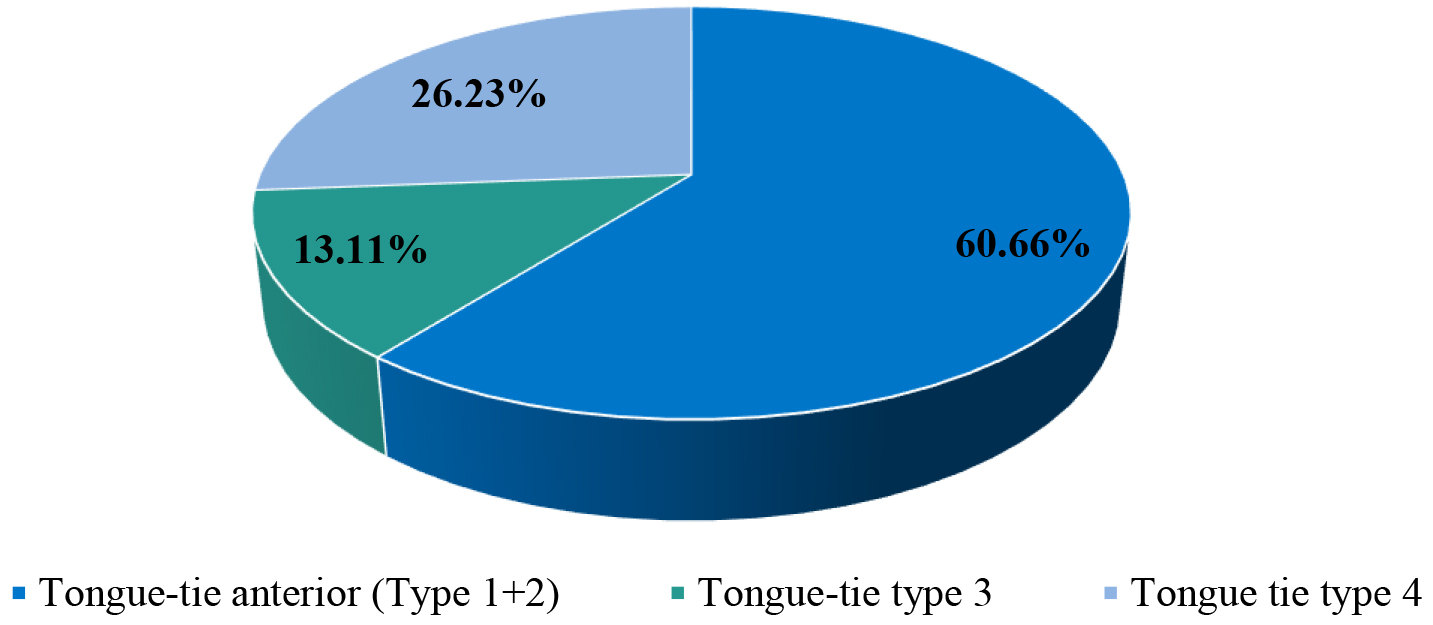 Fig. 6.
Fig. 6.
Hazelbaker Score
Regarding frenotomy, 71.18% of all infants with scores
From the category of infants with a score
Effective breastfeeding in the first week of life was present in 73.82% of all
infants studied (149), and 74.54% of this category were tongue-tied infants
(Table 4). We found that the majority of tongue-tied neonates in the case of
forceful MER (Group I), were breastfeeding effectively (92.50%) and also a high
percentage (96.55%) from Group III. Differences were statistically significant
(p
| Effective breastfed | Difficult latch | Shallow latch | Reflux like syndrome | Breast refusal | Choking | Nipple pain | |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |
| Total cases N = 149 | 110 (73.82) | 58 (38.92) | 81 (54.36) | 35 (23.48) | 15 (10.06) | 30 (20.13) | 42 (28.18) |
| Tongue-tie | 82 (74.54) | 43 (74.13) | 57 (70.37) | 8 (22.85) | 8 (53.33) | 3 (10) | 33 (78.57) |
| Group I Tongue-tie + forceful MER N = 80 | 74 (92.50) | 6 (7.50) | 27 (33.75) | 6 ** (7.50) | 6 *** (7.50) | 2 (2.50) | 21 (26.25) |
| Group II Tongue-tie N = 40 | 8 (20) | 37 (92.50) | 30 (75) | 2 (5) | 2 (5) | 1 (2.50) | 12 (30) |
| Group III forceful MER N = 29 | 28 (96.55) | 15 (51.72) | 24 (82.75) | 27 (93.10) | 7**** (24.13) | 27 (93.10) | 9 (31.03) |
| χ2 | 82.16 | 83.52 | 29.99 | 97.19 | 8.06 | 119.23 | 0.33 |
| p |
1.44 |
7.30 |
3.07 |
7.88 |
0.018 | 1.29 |
0.848 |
| p |
0.018* |
Note: MER, Milk Ejection Reflex; *, Statistically significant; **, 4
(66.66%) at follow-up visit
The difficult latch was present in 38.92% of all infants studied, and 74.13%
of this category were tongue-tied infants (Table 4). Difficult latch was
significantly (p
The shallow latch was present in 54.36% of all infants studied. It was less
frequent in infants from Group I (33.75%) compared with infants from Group III
(82.75%) and in infants from Group II (75%), with differences being significant
for p
“Reflux-like syndrome” was present in 23.48% of all infants studied (Table 4). It was less frequent (7.50%) in Group I (the majority of cases 66.66%, appeared later) and in Group II (5%). However, it was more present in infants in Group III (93.10%) (Table 4). Analyzing all tongue-tied infants, 6.66% of them had relevant symptoms of this syndrome (Table 1).
Breast refusal was 10.06% of all infants studied. It was rare in Group I
(7.50%) with the majority, 83.30%, occurring at the follow-up visit. It was
most frequent in Group III (24.13%), statistically at a higher rate than in
Groups I and II, significant at p
Choking was present in 20.13% of all infants studied, with only 10% having
tongue-tie. It was less frequent in Group I (2.50%) but significantly more
frequent in infants in Group III (93.10%), with a significant difference
(p
Nipple pain in mothers occurred in ~1/3 (28.18%) of all cases. The majority (78.57%) had tongue-tied infants (Table 4) and, of them 81.81% were with anterior tongue-tie, and only a few (18.18%) with tongue-tie type 3 and 4 (Table 1). Within the groups, the frequency of nipple pain was almost the same with no significant differences between the three groups (Table 4).
For all infants studied, 24.83% (Table 5) returned for a follow-up visit after the first week of life. Return was more frequent in the first month (35.13%) and within Group III (48.27%), with a higher proportion of patients returning compared to Groups I and II.
| In the first month |
2 Month | 3 Month | 4 Month | 5 Month | ||
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |
| Total Follow-up Cases | 37 (24.83) | 13 (35.13) | 7 (18.91) | 5 (13.51) | 11 (29.72) | 1 (2.70) |
| TT. | 23 (62) | |||||
| Group I Tongue-tie + forceful MER | 17 (21.25) | 4 (23.52) | 6 (35.29) | 2 (11.76) | 4 (23.5) | 1 (5.88) |
| Group II Tongue-tie | 6 (15) | 6 (100) | 0 | 0 | 0 | 0 |
| Group III forceful MER | 14 (48.27) | 3 (21.42) | 1 (7.14) | 3 (21.42) | 7 (50) | 0 |
| Z statistic Gr. I versus II | 0.82 | |||||
| p |
0.412 | |||||
| Z statistic Gr. I versus III | –2.76 | |||||
| p |
0.0057* | |||||
| Z statistic Gr. II versus III | –3.01 | |||||
| p |
0.0026* |
Note: TT., Tongue-tie; Gr., Group; *, Statistically significant; Z, pairwise z-tests for proportions.
Regarding the parity of mothers studied, the majority of primiparas were in Group II, having normal MER and the majority of the second para was in Group I, having forceful MER (Fig. 7). The total number of mothers with forceful MER was 109 (73.15%). The differences in proportions were statistically significant across all pairwise comparisons, demonstrating that forceful milk ejection (MER) is more frequent in second para women (Table 6).
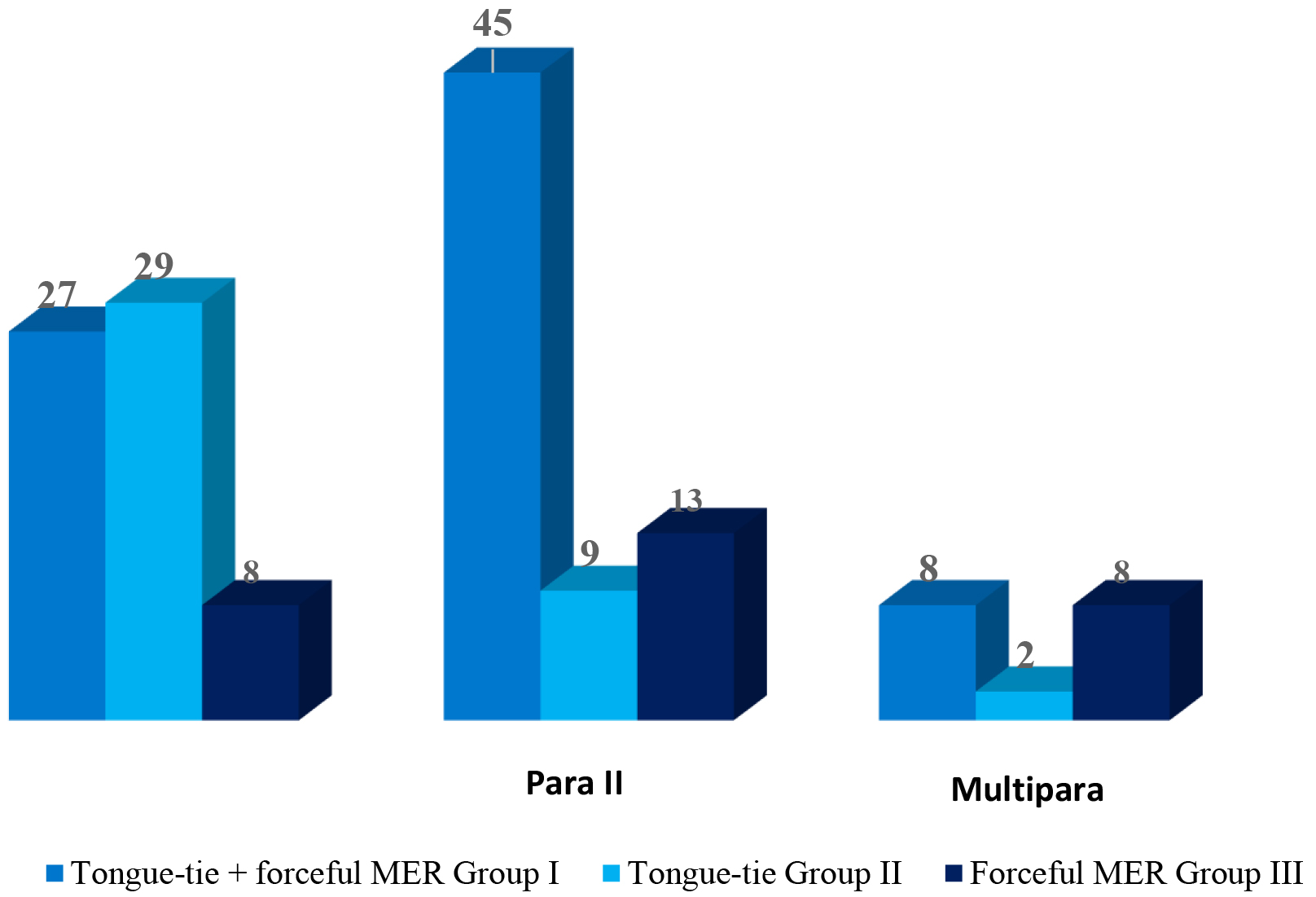 Fig. 7.
Fig. 7.
Mothers’ parity.
| Tongue-tie + forceful MER Group I | Tongue-tie Group II | forceful MER Group III | Total number of forceful MER | |
| N = 80 | N = 40 | N = 29 | N = 109** | |
| Para I N (%) | 27 (33.75) | 29 (72.50) | 8 (27.58) | 35 (32.11) |
| Para II N (%) | 45 (56.25) | 9 (22.5) | 13 (44.82) | 58 (53.21) |
| Multipara N (%) | 8 (10) | 2 (5) | 8 (27.58) | 16 (14.67) |
| Z statistic P.I versus P.II | –3.15 | |||
| p |
0.0016* | |||
| Z statistic P.I versus Mult. | 3.04 | |||
| p |
0.0024* | |||
| Z statistic P.II versus Mult. | 6.01 | |||
| p |
1.89 |
Note: MER, Milk Ejection Reflex; P.I, Para I; P.II, Para II; Mult., Multipara; *, Statistically significant; Z statistic, pairwise z-tests for proportions; **, 73.15% from all mothers participated in the study.
Analyzing all tongue-tied infants (Group I + Group II), more than half were suckling effectively, probably because the majority of them had mothers with forceful MER. This study supports the statement of Geddes et al. [36] (2010), that “the majority of infants with ankyloglossia can breastfeed successfully”.
In tongue-tied infants, the latch is shallow and US studies demonstrated that the nipple is compressed into the hard palate [28], which slows milk flow. If it is associated with a superior lip tight frenulum, this helps to stop the fast flow, compressing the breast and collapsing some ducts. It seems that in some cases of early forceful MER, some neonates adjust to cope with the mother’s fast milk flow. This supports ultrasound results that suggest that some mothers may have particular MER characteristics that contribute to the successful breastfeeding of infants with ankyloglossia [36]. Another explanation could be that the negative pressure of intra-oral vacuum is most effective when combined with a positive pressure of maternal milk ejection [37].
Although Lawrence RA and Lawrence RM [1] (2016) stated that forceful MER is more frequent in primipara mothers, in our study it was more frequent in second-para mothers.
We found a high incidence of anterior tongue-tie (types 1 and 2), comparable to Coryllos et al.’s [19] (2004) report. Regarding “posterior tongue-tie”, we found fewer cases perhaps because it is more difficult to diagnose [15, 19].
Although Amir et al. [13] (2006) found that the cut-off of
“less than or equal to 4” score, at HATLFF modified functional score, indicates
a recommendation for frenotomy, we report an ~71% percentage of
frenotomy in this category. The majority had mothers with normal MER. We also
found some cases needing frenotomy in infants with a score
Frenotomy of tongue-tied infants was more frequent in the absence of fast milk flow and the majority had anterior tongue-tie. The high percentage of difficult latch, mainly having anterior tongue-tie, shallow latch, and ineffective breastfeeding in the first week after birth, explains the need for urgent frenotomy in this group [20].
We found that the incidence of nipple pain was almost equal in the three groups, approaching Kent et al.’s [40] (2015) findings. The relatively low percentage of mother’s nipple pain of tongue-tied neonates in the absence of forceful MER (Group II) could be explained by the early frenotomy in this group. Although in Group I nipple pain frequency was almost similar, it represented the primary cause of frenotomy, but it was not an emergency. In half of these cases, mothers returned for division later, the majority after 2 months postpartum, and a small number at 4 and 5 months.
The primary cause of the mother’s nipple pain was anterior tongue tie, as described in the literature [23], and presents in a high percentage of cases of a difficult latch. Anterior tongue-tie represented the majority of cases that underwent frenotomy, supporting the opinion of other authors [19] about the necessity of urgent treatment. Our study also demonstrated that frenotomy cannot be recommended for all infants with ankyloglossia [36], because only 45% of total tongue-tied infants underwent frenotomy.
Our study, analyzing all tongue-tied infants, found that “reflux-like syndrome”, occurred in a very low percentage, a fact also demonstrated by ultrasound studies [23, 41], as compared with infants without tongue-tied but forceful MER. Choking was present in very few cases of tongue-tied infants, demonstrating that there is no evidence to suggest that dyscoordination of suck-swallow-breath indicates oral connective tissue problems [26]. Choking had a high percentage of infants without tongue-tie, fighting with forceful milk ejection. Air-induced reflux and choking in this group could be the reason for the frequent follow-up visits.
We observed the superior lip frenulum normally present [11, 42] and found that a high percentage of neonates have a lip frenulum inserted anteriorly. According to Kotlow [30], these are tight frenulum cases, which in his opinion may be a source of sucking problems. Our findings support other studies [31, 34] that this short upper lip frenulum is normal in neonates.
The present study explored the association between forceful MER and infant tongue-tie, offering guidance for professionals considering frenotomy in tongue-tie cases with a mother experiencing forceful milk ejection reflex.
The difficulty in the follow-up of cases, after they visit our Institute, is a limitation to the present study. A future study is needed with the possibility of a randomized control trial.
The majority of tongue-tied infants, whose mothers had early forceful milk ejection, were able to effectively breastfeed after birth. The present study suggests that frenotomy might not be necessary or could be postponed. The presence of tongue-tie only, without fast milk flow, led to suckling difficulties and the need for frenotomy. Reflux-like syndrome, choking, and breast refusal were more frequent in infants without tongue-tie but with fast milk flow.
All data points generated or analyzed during this study are included in this article and there are no further underlying data necessary to reproduce the results.
MM—contributed to conception and design, acquisition, analysis, and interpretation, drafted the manuscript, gave final approval, agreed to be accountable for all aspects of work ensuring integrity and accuracy. SM—contributed to acquisition, analysis, and interpretation, critically revised the manuscript, agrees to be accountable for all aspects of work ensuring integrity and accuracy. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki. The protocol to study human subjects was approved by the Institute’s Ethics Committee (approval No. 2/C.E./10.04.2011). Informed consent was signed by all mothers participating in the study.
We would like to express our gratitude to all the students from ProMAMA Lactation Institute who voluntarily helped us with data collection for this study. We thank all the peer reviewers for their constructive opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
Appendix 1. Questioner
1. Feeding method of the infant
Suckling from the breast:
-How often?: ___________________________
- Day: ___________________________
- Night: ___________________________
- Duration of a breastfeeding session?: ___________________________
- The longest interval between meals: ___________________________
- One or both breasts at a time: ___________________________
- How long does it take for the first breast to suck from both?: ___________________________
- Do you test weighing her sucking (weighed before and after sucking)?: ___________________________
- How many times?: ___________________________
- In what position are you breastfeeding?
- Sitting: ___________________________
- Lying down: ___________________________
- Football: ___________________________
- How tall is the baby’s head when you are breastfeeding? (in the breast, lower or higher?) : ___________________________
-When he sucks in a supine position, is the baby sitting on his back with his head turned towards the breast, or is he lying in a line parallel to you, his belly touching your belly?
___________________________
- When he is attached to the breast, does he catch a part of the areola or only the nipple?
___________________________
- Does your nipple hurt when you suck? ___________________________
- He is sucking noisy? ___________________________
- Does his cheek clog when he sucks? ___________________________
- Is his tongue under the nipple? ___________________________
- Can you hear him swallowing when he sucks? ___________________________
- Does he leave the breast or do you take your breast out of your mouth? He is taking frequent breaks during a suck?
___________________________
- Is he satisfied immediately after sucking? fall asleep? ___________________________
- Does milk come out after sucking? ___________________________
- After he attached to the breast, does he happen to get rid of it? ___________________________
Completion:
- Do you give him the pacifier:
- Yes ___________________________
- No ___________________________
- Is he sucking his finger? ___________________________
- Do you give him extra water, tea or milk powder, or other foods?
___________________________
- When was the first time completed? ___________________________
- How was given the completion (with the bottle, teaspoon, glass, others)?: ___________________________
2. The child’s health
- Birth weight: ___________________________
- The weight at the discharge from the hospital and the age of the baby when you left?: ___________________________
- Current weight: ___________________________
- Gestational age (was he premature?): ___________________________
- Twin: ___________________________
- Did he have problems immediately after birth? what?: ___________________________
- Did he have jaundice? had to be put on the lamp (phototherapy)?: ___________________________
- Does the child take any medication?: ___________________________
- How often does he urinate? (frecvently/rare- normal 6
- Stool:
- Soft: ___________________________
- Yellowish: ___________________________
- Brown: ___________________________
- Hard or green: ___________________________
- How many times/day?: ___________________________
- After each suck?: ___________________________
- He has an appetite?: ___________________________
- Is he vomiting?: ___________________________
- How is he sleeping?
-A lot: ___________________________
-Little bit: ___________________________
- Does he have a trush in his mouth?: ___________________________
- Does he have colic? if so what medications do you give him?: ___________________________
- Does he have any disease or malformations?: ___________________________
3. Pregnancy, birth, first feeding
- How did the pregnancy go?: ___________________________
- How was the birth (vaginal, cesarean)?: ___________________________
- How long after birth did they bring him to the breast ?: ___________________________
- Did you sleep with the child in the rooming-in?: ___________________________
4. Mother’s condition
- Your age: ___________________________
- How is the breast?: ___________________________
- Normal nipple: ___________________________
- Flat: ___________________________
- Umbilicate: ___________________________
- Cracked with a wound: ___________________________
- Nipple rash: ___________________________
- Have you ever had mastitis, blocked duct, or engorgement? (symptoms, have you been treated?)
___________________________
- Do you feel your breasts full and tense?: ___________________________
- Do you feel them soft after sucking?: ___________________________
- Do you wash your breast before or after breastfeeding? (do not have to!!): ___________________________
- If you are expressing milk how (by hand, regular pump, electric)?: ___________________________
- You are healthy, have hormonal disorders, thyroid problems, diabetes, or other:
___________________________
- Are you taking any medication?: ___________________________
- Are you allergic?: ___________________________
- Do you smoke? if yes how many/day: ___________________________
- Do you drink more than one cup of coffee, cola or black tea, Lipton Ice tea?
___________________________
- How much do you eat/day, how many liquids do you drink, and do you rest?
___________________________
- Do you have help from your family? Does it support you in breastfeeding?
___________________________
5. Previous experience with feeding young children
- Number of other children if you still have: ___________________________
- How many did you breastfeed?: ___________________________
- If yes it was a positive or negative experience: ___________________________
Describe any information you find useful that may help resolve the issue
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.