

 , Masoomeh Kheirkhah 2,*
, Masoomeh Kheirkhah 2,* , Ali Ghobadi 3, Nooshin Eshraghi 4, Shima Haghani 5
, Ali Ghobadi 3, Nooshin Eshraghi 4, Shima Haghani 51 School of Nursing and Midwifery, Iran University of Medical Sciences, 14496-14535 Tehran, Iran
2 Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, 14496-14535 Tehran, Iran
3 School of Persian Medicine, Iran University of Medical Sciences, 11147-33311 Tehran, Iran
4 Shahid Akbarabadi Clinical Research Development Unit (ShACRDU), School of Medicine, Iran University of Medical Sciences (IUMS), 11687-43514 Tehran, Iran
5 Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, 14496-14535 Tehran, Iran
Abstract
Background: Pregnancy striae, a common problem in pregnant women,
create significant concerns about beauty in most women and there are challenges
in preventing and treating them. The current research sought to investigate the
impact of a vitamin “C + D” cream combination on striae distensae in primipara.
Methods: The current research was a clinical study with a control group,
which was carried out in parallel with 60 primipara at 18–20 weeks gestational
age, who presented at Shahid Akbarabadi Hospital in Tehran between 20/07/2022 to
20/01/2023. Sampling was done using a continuous method, and then allocated into
two groups using a random block of 4 and 8 with the Sealed Envelope online
software. One group received vitamin “C + D” cream (30 candidates) while the
other group received a placebo cream (30 candidates). Both sets of candidates
applied the creams to the skin of the abdomen, breasts, thighs, and hips twice
daily for four months. Evaluation of the severity and quantity of stretch marks
was performed with the Atwal’s numerical tool scale. An assessment was conducted
by the investigator at the study center’s prenatal clinic before and at 4, 8, 12,
and 16 weeks following the intervention. Results: There were no notable
disparities in individual and obstetrical characteristics between groups before
the intervention (p
Keywords
- striae distensae
- primiparity
- therapy
- prevention
- ascorbate
- vitamin C
- vitamin D
- cholecalciferol
- vitamin “C + D”
Pregnancy leads to the development of conditions that result in significant physiological, structural, and functional changes in various parts of the body to adapt to this phenomenon. While many of these changes resolve after pregnancy, some may persist permanently, subsequently exerting a significant impact on women’s lives [1]. One of these changes is skin alterations that occur in most women [2]. Skin changes during pregnancy are due to hormonal and metabolic changes, which are categorized into three groups: pre-pregnancy skin diseases, physiological skin changes during pregnancy (including increased skin pigmentation, melasma, changes in hair growth, vascular changes, and striae), and pregnancy-specific skin diseases [3]. Skin changes during pregnancy include increased pigmentation due to melanin deposition in the skin, affecting 90% of pregnant women [4]. This change is more pronounced in women with darker skin tones and is most noticeable in the early stages of pregnancy and in naturally darker areas like the areola, perineum, and navel [5]. Vascular changes in pregnancy, due to increased blood volume and flow and reduced peripheral vascular resistance, include spider angiomas and palmar erythema [6]. Spider angiomas, seen in two-thirds of white women and 10% of black women, are characterized by fine, red protrusions with branching vessels from a central lesion, often observed on the face, neck, and upper chest, and usually resolve after childbirth [7]. Palmar erythema is another change that is clinically insignificant, seen in two-thirds of white women and one-third of black women, and typically diminishes shortly after childbirth [5, 8]. Melasma is a common skin change during pregnancy, affecting 50% of pregnant women, characterized by irregular brown patches on the face, neck, and forehead [3, 9]. The exact cause is uncertain, but it is thought that both environmental and genetic factors may contribute. These patches usually fade after childbirth [5, 9]. Hair growth changes in pregnancy include an increase in the anagen phase compared to the resting phase. Estrogen prolongs the growth phase, while androgens cause follicles to lengthen in androgen-dependent areas like the face and neck [10]. Sudden hair loss during the telogen phase typically starts one to five months after childbirth, with hair growth returning to its pre-pregnancy state within six months to a year after childbirth [7, 10]. Striae are the most common changes in connective tissue that occur during pregnancy, typically appearing in the third trimester and impacting women of any race, whether they are first pregnant women or have had multiple pregnancies [11]. They form on the abdomen, thighs, and breasts, beginning as red or purple streaks that progress into glistening silvery lines, manifesting as creases on the surface of the skin [2, 11]. These pregnancy striae can be several centimeters long and 1–10 millimeter wide [12]. These symptoms can be noticed in 50–90% of pregnant women before 24 weeks and are also prevalent in 50–90% of the general population [13, 14]. In Iran, the prevalence of these skin changes among pregnant women is around 87.7% [15]. Some women consider these symptoms to be normal pregnancy symptoms. The exact cause is still not fully known. It is believed that genetic and hormonal factors, as well as increased mechanical pressure, play an important role in their development [16]. They can also occur as a result of rapid weight gain, specific endocrine disorders, and prolonged use of steroids [1, 17]. Striae are rarer in Asian and African American women, indicating a genetic influence [2, 17, 18]. Hormones such as estrogen and epinephrine are thought to contribute to their development. Estrogen, relaxin, and adrenal gland hormones can decrease collagen fiber connections and increase the extracellular matrix, contributing to striae development in areas under tension [18]. Additionally, there is a notable increase in estrogen, androgen, and glucocorticoid receptors in striae [19]. During pregnancy, estrogen hormone levels increase significantly moreover. The level of epinephrine hormone in pregnant women is higher compared to normal individuals and increases during pregnancy. Also in early pregnancy, the level of relaxin hormone is at its highest. This hormone works to relax the muscles and help facilitate the easier passage of the baby during childbirth [5, 19, 20]. Striae form following sudden weight gain, specific endocrine conditions, and prolonged steroid use [16, 20]. Continuous mechanical pressure on skin tissue alters the elastin fiber network and affects skin elasticity [19, 20]. They result from tension and increased mechanical pressure on the connective tissue, causing skin stretching and inadequate collagen repair disrupted by tension [11, 20]. Changes in the elastin fiber network affect the damaged skin’s viscoelastic properties, leading to firmer skin with reduced elasticity and deformability compared to normal skin [7, 19, 20]. Individuals in this situation are at higher risk of pelvic organ prolapse and tears in the perineal and labial areas during childbirth [19, 20]. Pregnancy striae can be affected by factors such as the age of mother, body mass index (BMI), weight gain, abdominal size, baby weight, family background, and nutrition [21]. While not medically risky, they can impact self-image, confidence, and mental health. This may lead to issues such as negative body image, reduced self-confidence, and even depression [22]. These consequences can result in psychological challenges, poor body image, diminished sexual satisfaction and overall well-being, skin injuries from scratching, formation of itchy papules and plaques, persistent stress and anxiety for the, and potential behavioral issues for the infant [5, 7, 23]. Many primipara or women planning to have a child are seeking information on factors influencing the condition of stretch marks (striae) and how to prevent and treat them [2, 24]. They are ready to spend money on treatment options. Interventions for striae emphasize prevention and management [7, 24]. Actions for preventing and treating stretch marks include engaging in regular physical activity, maintaining a nutritious diet, staying well-hydrated, utilizing skincare goods, and therapeutic approaches such as microdermabrasion and microneedling. Nonetheless, some of these interventions may be costly and not be easily affordable for all individuals [19, 25]. Research conducted in Jiangsu, China, demonstrated that lifestyle choices and dietary habits play a crucial role in the development and intensity of striae on the skin [18, 19, 25]. A study conducted in Lebanon suggested that the topical application of lotion containing cocoa butter may not decrease the chance of developing pregnancy striae [26]. A study has shown a link between the presence of striae and blood levels of vitamin C [27]. Limited evidence suggests that centella and bitter almond oil massage may help prevent and reduce the severity of striae (SG). There is weak evidence supporting the use of hyaluronic acid for preventing SG. Tretinoin may also reduce the severity of new striae, but its use is restricted by its pregnancy category [28]. Some studies have shown the possible effects of certain vitamins, such as vitamin C, on the appearance of stretch marks [29, 30]. Vitamin C, also known as ascorbic acid or ascorbate, is a water-soluble vitamin that acts as an antioxidant and reviving agent in the body and has a chemical structure of a 6-carbon lactone. The deterioration of vitamin C happens quickly when exposed to air [5, 30]. Vitamin C is a crucial component in the diet of humans and many animals, the lack of which can result in scurvy and non-healing wounds [31]. The skin has a significant amount of vitamin C (the concentration of the substance in the tissue ranges from 0.4 to 1 milligram per 100 grams of wet tissue weight), mainly found in the endocellular compartments. It is delivered to the layer of skin through blood vessels [32]. Daily vitamin C intake during pregnancy should be between 80 and 85 mg, which is about 20% higher than when not pregnant. The United States Food and Drug Administration (FDA) classifies vitamin C as category A; consuming more than the recommended amount is considered category C [5, 33, 34]. Humans, in spite of plants and some animals, are incapable of synthesizing it because they do not have the enzyme L-gluconogama lactone oxidase. While high concentrations of vitamin C supplements are found, only a small amount of it is naturally present and active in the skin. It is a potent antioxidant that aids in shielding the skin from aging, ultraviolet (UV) damage, and immune system suppression, as well as helping to prevent carcinogenesis [35]. Vitamin C has anti-aging properties by increasing collagen synthesis and reducing its degradation. It also helps in reducing the development of melanin and pigmentation, and enhances the process of wound repair [21, 30, 35]. This vitamin inhibits the aP-1 (activation protein-1), and decreases the production of matrix metalloproteinase (or matrix metalloproteinase (MMP): an enzyme that breaks down collagen) and hinders the natural production of elastin [5, 21, 35]. There is still limited research on the effects of different types of topical vitamin C formulations on the human skin and more research is needed [21, 30, 35]. Some research has also proposed a potential impact of certain vitamins, such as vitamin D, on the formation of striae distensae. This vitamin is a fat-soluble vitamin that belongs to the tocopherol family. The main compounds within this group are vitamin D₃ and vitamin D₂ [36, 37]. The primary source of vitamin D is sunlight, particularly ultraviolet B rays, which trigger a chemical reaction in the deeper layers of the epidermis, resulting in the production of cholecalciferol or vitamin D₃ [38]. 1,25-dihydroxy vitamin D plays a significant role in calcium homeostasis and bone health. It is biologically active and serves as a stable indicator of the level and status of vitamin D in the body [39]. Additionally, it helps maintain the permeability barrier of the epidermis and stimulates the proliferation and differentiation of keratinocytes in the epidermis, as well as the growth of fibroblasts in the dermis. It is worth noting that fibroblasts are the main cells in the dermis responsible for producing collagen and the extracellular matrix [1, 39]. Therefore, vitamin D deficiency and collagen deficiency are directly related to the occurrence of stretch marks [32, 40]. Collagens, which are produced by dermal fibroblasts in the extracellular matrix, are essential for skin health. Among the various types of collagens, type 1 and type 3 are particularly important and make up 80–90% of the dermis [25, 35]. Considering all the mentioned factors, the contradictory results regarding the efficacy of interventions, limited research on vitamin consumption, high prevalence of this condition as well as expensive costs of cosmetic goods and medical treatments, conducting a study aiming to find out the impact of vitamin “C + D” combination cream on striae in primipara seems essential. This research would not only provide valuable insights into the most effective strategies for preventing and reducing striae but also offer important recommendations to the target population. It would represent a crucial effort in enhancing the well-being of expectant pregnant women and, in turn, benefiting families and society as a whole.
The current study was designed and conducted with the aim of determining the impact of vitamin C + D on pregnancy striae in primipara.
Population, intervention, comparison, and outcome (PICO) question: In primiparous women, does the application of combined vitamin C + D cream compared to placebo or no supplementation reduce or prevent pregnancy striae?
This research was a randomized clinical trial with a control group, which was carried out in parallel with 60 primipara at 18–20 weeks gestational age, who presented at Shahid Akbarabadi Hospital in Tehran between 20/07/2022 to 20/01/2023. After approving the tool and obtaining the code of ethics (IR.IUMS.REC.1401.215), and registering in the clinical trial center of Iran (IRCT20220509054799N1) in adherence to the parameters of the Declaration of Helsinki and Good clinical practice guidelines, after obtaining a letter of recommendation from the Faculty of Nursing and Midwifery at Iran University of Medical Sciences, and submitting it to the authorities at Shahid Akbarabadi Educational and Therapeutic Center in Tehran, which serves as a referral hub for pregnant in the southern part of Tehran, the sampling was carried out. To find out the minimum sample size required at 95% confidence level and 80% test power, and assuming that a 6-unit difference between two groups is considered statistically significant, sample size was calculated using the following formula [41]. Therefore, a sample size of 24 individuals was calculated for each group, and adjusting for a possible 20% dropout rate, the anticipated sample size for each group were 30 individuals.
First, the research samples were selected based on the inclusion criteria of the study. Sampling was conducted using a continuous method by the researcher until reaching the predetermined sample size at Shahid Akbarabadi Hospital. The allocation of samples to groups was performed using the random block allocation method. At first, each of the groups was given the labels A and B. Before the start of the study, a hypothetical list of 60 numbers was prepared through the random block method by the Seal Envelope site, specifying the number of blocks of 4 and 8, for the candidates in two groups of 30 for Cream A and Cream B. Concealing the allocation and maintaining blinding was done using the code provided by the Seal Envelope software (Sealed Envelope Ltd. 2022, London, United Kingdom) on pre-prepared and wax-sealed envelopes. The sampling process continued until the desired sample size was reached. The envelopes were opened in the order in which the candidates entered the research. Candidates were allocated to intervention and placebo groups, each consisting of 30 individuals, according to the list. They were advised to apply the creams topically, gently, and without massaging, using their fingers. The creams should be applied twice daily, at intervals of 12 hours, for a duration of 4 months. The recommended areas for application included the abdominal, thigh, breast, and buttock regions, and it was emphasized to cover these areas with a thin layer of cream. Candidates were advised not to remove the cream until it is completely absorbed. Based on the Fig. 1, in the intervention group, one person experienced abortion, three individuals cited insufficient time and a person reported itching, which led to a reduction in the sample size. Finally, 25 person were present in the vitamin “C + D” group. In the control group, two individuals experienced abortion, three individuals cited insufficient time, and a person reported itching, resulting in a decrease in the sample size. Finally, 24 person were present in the placebo group.
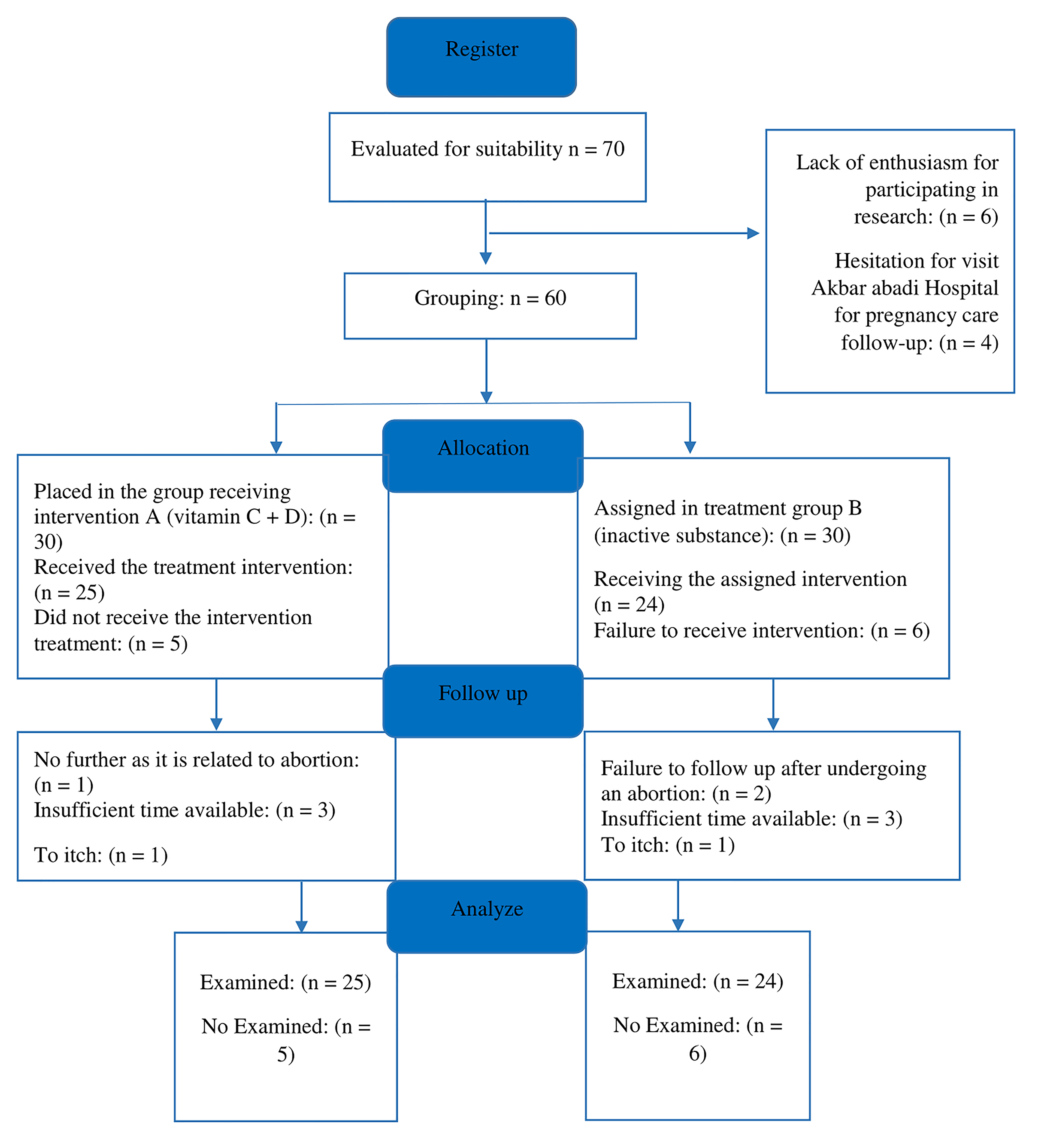 Fig. 1.
Fig. 1.
CONSORT diagram for the study process.
The entrance criteria for the research are as follows: healthy women who are primiparous, aged between 20–40 years, at 18–20 weeks of gestation, with a BMI before the intervention ranging from 18.5 to 25, possessing a minimum level of literacy and willingness to participate in the study, and the exclusion criteria for the research are as follows: suffering from a known systemic or underlying disease (for example gestational diabetes mellitus, pre-eclampsia, adrenal gland disorder, and Cushing’s syndrome), multiple pregnancy, history of skin diseases before striae, history of allergies to vitamin D and C, maternal polyhydramnios and the identification of macrosomia. As well as exit criteria: the use of alternative medications for preventing or treating striae during the research, reluctance to persist in using the medication, experiencing adverse reactions from the medication during the study (itching, burning and redness), failure to use the medicine correctly (failure to observe the amount, number of times and how to use the cream), and concurrent use of medications that may interact with vitamin C and D (for instance corticosteroids that vitamin D may decrease the effectiveness of corticosteroids, and anticoagulants that vitamin C may increase the risk of bleeding when taken with these medications and also may interfere with the effectiveness of them) during the study.
Data collection instruments were a demographic questionnaire, and Atwal striae gravidarum score. The researcher, who was proficiently trained, measured and documented the quantity and intensity of erythematous striae in all stages using Atwal’s numerical scale tool. The highest score for each area (abdomen, breasts, thighs, and buttocks) was capped at 6 (score ranging from 0 to 3 for the number of striae and score ranging from 0 to 3 for erythema severity). If no striae were visible in a given area, a score of 0 was assigned. For less than 5 striae, a rating of 1 was given, for 5 to 10 striae, a rating of 2 was assigned, and for more than 10 striae, a rating of 3 was awarded. For the absence of erythema, a rating of 0 was assigned, for mild erythema (light red or pink), a rating of 1 was given, for marked erythema (dark red), a rating of 2 was assigned, and for intense erythema (purple), a rating of 3 was awarded. The overall score ranged from 0 to 3, denoting either no visible striae or minimal striae, from 4 to 9 indicating slight striae, from 10 to 15 signifying moderate striae, and above 16 suggesting significant striae. The total striae score (TSS) was calculated by adding these two scores together. The TSS ranged from 0 to 24 for all body parts, categorizing women into four groups: those with scores of 0–3 showed no signs of pregnancy striae, scores of 4–9 indicated mild striae, scores of 10–15 indicated moderate striae, and scores above 16 indicated severe striae [42].
In order to evaluate the credibility of the data gathering instrument for the personal traits category, the face and content validity approaches were employed. Firstly, the data collection tool (Atwal striae gravidarum score and demographic survey) was selected based on a comprehensive examination of credible and up-to-date sources articles, alongside advice from experienced professors. Afterwards, in order to collect rectifying feedback, the instrument was distributed to 7 faculty members at Iran University of Medical Sciences. After the ultimate assessment, incorporating guidance from relevant professors, the necessary final modifications were made. The accuracy of this tool (Atwal striae gravidarum score) has been verified by [42]. To assess the reliability of the tool, inter-rater reliability agreement was employed. In this way, the condition, quantity, and degree of pregnancy-induced stretch marks were separately scrutinized and documented by the investigator and a specialist dermatologist in 10 subjects. Due to ethical concerns and the lack of consent from all candidates to have photos taken of the areas under investigation, and out of respect for their beliefs, at the beginning of the study, several cases that did consent to having their photos taken were examined. The images captured by the investigator and skin specialist were assessed utilizing the Atwal method, and the agreement between the findings was established. In the end, an intraclass correlation coefficient (ICC) of 0.98 ~1 was achieved for all regions.
The intervention involved using a combination cream with vitamin C and D. Candidates were enrolled in the study during weeks 18–20 of their pregnancy and were followed for 4 months (at 1, 2, 3, and 4 months after starting the intervention). The data collection for this study was carried out over a span of 6 months, between 20th July 2022 to 20th January 2023. The candidates were given essential information about the conduct of the study, and they were informed that they assigned at random to either the treatment or control groups. The survey regarding individual traits, BMI, and length of pregnancy was finished at the outset of the research. Subsequently, candidates who satisfied the research criteria were assigned to either the treatment or control group according to a pre-established chart, following the completion of the demographic data questionnaire. Creams were concocted at the researcher’s behest with the assistance of the consultant pharmacist from the Department of Traditional Medicine at Iran Medical Sciences. Creams from both classes had similar packaging and the same color and fragrance. Concealment was also carried out according to the guidelines provided by the seal envelope software (Sealed Envelope Ltd. 2022, London, England, United Kingdom), and the creams were divided into two groups: Group A and Group B. The vitamin “C + D” combination cream included 3% topical vitamin C and topical vitamin D 5000 units in 100 grams of Oraand base cream, which included components like alcoacetyl, glycerin, triethanolamine, monostarch acid, white vaseline and purified water. The placebo, conversely, consisted of the Oraand base cream without any active substances.
Both sets of candidates were given thorough instructions on the proper application of the medication. They were instructed to administer the creams externally, softly, and without rubbing, using their fingertips. The creams should be applied twice daily, at intervals of 12 hours, for a duration of 4 months. The recommended areas for application included the abdominal, thigh, breast, and buttock regions, and it was emphasized to cover these areas with a thin layer of cream. Candidates were instructed not to cleanse off the cream until it is completely assimilated. Additionally, the investigator directly gave in-person guidance to females on how to accurately fill out the everyday questionnaires during their initial appointment. The investigator and the candidates were unaware of the contents of the creams. Prior to the intervention, the researcher measured and documented the quantity and intensity of striae erythema using Atwal’s numerical tool scale. Women were requested to document the daily to-do lists on the designated forms following the use of the creams. The Atwal tool was used by the researcher to evaluate the quantity and intensity of striae caused by pregnancy at 1, 2, 3, and 4 months post-treatment initiation. According to this rating system, the intensity of erythema and the quantity of existing striae were evaluated on the abdomen, breast, thighs and buttocks. The study candidates were seen by the investigator at the perinatology clinic during various follow-up appointments. The investigator utilized the Atwal instrument to assess the quantity and severity of striae and documented them. At each appointment, the investigator observed the application of each cream treatment by each candidate. The evaluation times of the study candidates were scheduled to align with their prenatal care appointments. Additionally, the patients’ weight was monitored at each phase due to its impact on the development of stretch marks. The researcher consistently stayed in touch with the study candidates via phone calls or messages to confirm the proper use of the creams and completion of all necessary forms. The researcher also checked for any potential side effects, for instance itching or redness, and asked candidates to notify them in advance if they experienced any. The sampling process persisted until the desired final sample size was achieved. Considering the likelihood of candidates withdrawing or discontinuing their involvement. At the conclusion of the research, the researcher documented the candidates’ body mass index and gestational age, and completed observation sheets noting the occurrence and severity of striae in pregnancy.
The allocation of candidates to categories was performed using the random block allocation method. Researcher was unaware of the group allocation. At the beginning, the two groups were arranged as Group A, Group B. The allocation of candidates to the groups was carried out through the Seal Envelope website, utilizing a pre-prepared list and employing a random block assignment method of 4 and 8. To ensure concealment, ready-to-use envelopes were sealed with a code provided by the Seal Envelope website. Candidates did not know whether they were assigned to the intervention group or placebo. Both groups were given creams. The researchers and candidates were not informed about the content of the creams because their packaging, appearance, smell and colors were the same and there were no variations in theshape and shade of the creams. This research was a triple-blinded randomized clinical trial with a control group. The evaluator, investigator, and candidates were oblivious to the groups.
After gathering the data, the data were analyzed using SPSS version 16 software
(IBM-SPSS Statistics, Chicago, IL, USA) and with descriptive statistics of
relative frequency, average and standard deviation and analytical statistics of
Chi-square, Mann-Whitney U test, Fisher’s exact test, and independent
t-test. Since the Kolmogorov-Smirnov test showed that the distribution
of the data was not normal, the non-parametric Mann-Whitney U test was used to
compare the incidence between groups. The researcher used the Chi-square test to
analyze the education and midwifery characteristics of the two groups, Fisher’s
exact test to compare their economic situations, and the independent
t-test to evaluate differences in age and body mass index between the
groups. The significance level was set at p
The majority of individuals in the vitamin “C + D” group fell within the age
brackets of 25–30 and 35–40 years, whereas in control group, the age range was
30–35 years. After the intervention, their BMI ranged from 25 to 29.9 (Table 1).
The vast majority of the samples in both categories had no prior experience of
abortion and family history of striae in the immediate family members and had
white skin tone (Table 2). Finally, based on Table 1, the findings indicated that
there was no notable distinction among the factors of age, level of education,
financial status, and body mass index following the implementation of the two
groups (p
| Group | Placebo | Vitamin C + D | The significance level |
| Demographic characteristics | (percentage) number | (percentage) number | |
| Age (years) | |||
| 20–25 | (20.83%) 5 | (28%) 7 | Independent t-test |
| 25–30 | (29.17%) 7 | (20%) 5 | p = 0.765 |
| 30–35 | (37.50%) 9 | (24%) 6 | |
| 35–40 | (12.50%) 3 | (28%) 7 | |
| Standard deviation |
28.65 |
29.24 |
|
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| 3.7713 | –2.7913 | ||
| 3.7571 | –2.7771 | ||
| Education | |||
| Elementary | (25.00%) 6 | (16%) 4 | Chi-square test |
| Middle school | (20.83%) 5 | (8%) 2 | p = 2.832 |
| Secondary school | (33.33%) 8 | (44%) 11 | df = 3 |
| Tertiary | (20.83%) 5 | (32%) 8 | |
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| 0.5097 | –0.6297 | ||
| 0.5137 | –0.6337 | ||
| The economic situation | |||
| Enough | (4.17%) 1 | (0%) 0 | Fisher’s test |
| Relatively enough | (75.00%) 18 | (92%) 23 | p = 0.165 |
| Insufficient | (20.83%) 5 | (8%) 2 | |
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| 0.4604 | –0.0371 | ||
| 0.4662 | –0.0428 | ||
| Body mass index after the intervention | |||
| 18.5–24.9 | (8.33%) 2 | (16.66%) 4 | Independent t-test |
| 25.0–29.9 | (91.67%) 22 | (83.33%) 20 | p = 0.395 |
| Standard deviation |
27.48 |
27.03 |
|
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| 0.5983 | –1.4886 | ||
| 0.5941 | –1.4844 | ||
| Group | Placebo | Vitamin “C + D” | Chi-square test result |
| Obstetrics profile | (percentage) number | (percentage) number | |
| History of abortion | |||
| Positive | (45.83%) 11 | (48%) 12 | p = 0.879 |
| df = 1 | |||
| Negative | (57.17%) 13 | (52%) 13 | |
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| 0.3146 | –0.2712 | ||
| 0.3146 | –0.2712 | ||
| History of striae | |||
| Positive | (79.17%) 19 | (56%) 14 | p = 0.084 |
| df = 1 | |||
| Negative | (20.83%) 5 | (44%) 11 | |
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| –0.0439 | –0.5795 | ||
| –0.0448 | –0.5785 | ||
| Skin color | |||
| Olive | (25.00%) 6 | (20%) 5 | |
| White | (41.67%) 10 | (48%) 12 | p = 0.252 |
| df = 2 | |||
| Wheat | (33.33%) 8 | (32%) 8 | |
| Confidence interval of the difference with a 95% level of certainty | |||
| Upper | Lower | ||
| 0.5755 | –0.3488 | ||
| 0.5759 | –0.3492 | ||
Table 3 presents the occurrence of pregnancy striae and their comparison in the
two groups under investigation. Since pregnancy striae did not follow a normal
distribution based on the Kolmogorov-Smirnov test, the non-parametric
Mann-Whitney test was used to compare the two groups. Following the
implementation of the intervention, notable disparities were noted in the
incidence of striae among the two groups at weeks 4 (p
| Group | Placebo | Vitamin “C + D” | The result of the Mann-Whitney test |
| Atwal scale | (percentage) number | (percentage) number | |
| 4 weeks after the start of the intervention | |||
| 0–3 | (50%) 12 | (100%) 25 | p |
| 4–9 | (50%) 12 | (0%) 0 | |
| Average | 3.16 | 0.08 | |
| standard deviation | 2.91 | 0.40 | |
| 8 weeks after the start of the intervention | |||
| 0–3 | (50%) 12 | (100%) 25 | p |
| 4–9 | (50%) 12 | (0%) 0 | |
| Average | 3.66 | 0.24 | |
| standard deviation | 2.74 | 0.87 | |
| 12 weeks after the start of the intervention | |||
| 0–3 | (33.33%) 8 | (84%) 21 | p |
| 4–9 | (50.00%) 12 | (16%) 4 | |
| 10–15 | (16.67%) 4 | (0%) 0 | |
| Average | 4.66 | 0.76 | |
| standard deviation | 3.47 | 1.61 | |
| 16 weeks after the start of the intervention | |||
| 0–3 | (16.67%) 4 | (84%) 21 | p |
| 4–9 | (50.00%) 12 | (16%) 4 | |
| 10–15 | (33.33%) 8 | (0%) 0 | |
| Average | 5.66 | 0.8 | |
| standard deviation | 3.61 | 1.70 | |
The findings suggest that the use of vitamin “C + D” cream could potentially have a positive impact on reducing the development of pregnancy striae in primipara. Further studies are needed to confirm these results and explore the specific mechanisms by which vitamin “C + D” may be beneficial in preventing striae formation during pregnancy, a study by Abdolbaghiyan and colleagues in 2020 titled “Expression changes of collagen І and ІІІ genes in human skin fibroblast cells due to microalgae extract Chlorella vulgaris and its comparison with vitamin C” conducted at the National Institute of Iranian Genetic and Biological Resources, showed that algae extract and vitamin C increased collagen type І expression by 3.14-fold and 1.42-fold, respectively [35]. Chlorella vulgaris algae extract significantly increased the expression of collagen type І gene, while vitamin C significantly increased the expression of collagen type ІІІ gene, increasing the expression to 2.12-fold. They are emerging as promising substitutes to detrimental chemicals in stimulating collagen production [35]. These results support the idea of vitamin C being beneficial for collagen synthesis and its potential role in conditions such as striae in pregnancy.
A 2018 study by Hajhashemi and colleagues [43] evaluated the effectiveness of
aloe vera gel and sweet almond oil on stretch marks in 160 new women. they found
that creams containing aloe vera and sweet almond oil were effective in reducing
striae erythema compared to the base cream. Additionally, these creams alleviated
itchiness and inhibited the advancement of striae (p
Research by Hocaoglu et al. [1] in 2020 aimed at Association between
serum 25-hydroxyvitamin D levels and the presence and severity of striae
gravidarum on 91 primigravid women showed that women with normal levels of serum
25-hydroxyvitamin D (
In 2020, Sadat et al. [44] conducted a research with the aim of
assessing the impact of sesame oil and almond oil on the occurrence of striae in
165 pregnant women. At the end of the 36th week, the findings showed that the
incidence of striae in the almond oil, sesame oil and control groups was 63.60%,
60% and 58.20%, respectively. There was no significant difference in the
incidence of striae gravidarum between the three groups at the 36th week of
pregnancy (p = 0.83). Finally, it was concluded that both sesame oil and
almond oil cannot be effective in preventing the occurrence and severity of
striae gravidarum. Sesame oil and almond oil both contain vitamin D, the finding
of this research does not agree with the results of this study regarding the use
of vitamin D on the occurrence of striae in pregnancy. In this research, blinding
was not done and the control group did not use any placebo, and the samples were
massaged for 5 minutes after applying the oil, which can be effective in creating
bias in the study results and the possible cause of inconsistency in the results
[44]. Taheri et al. [45] conducted a research with the aim of
determining the effect of vitamin C cream on pregnancy striae, showed that use of
Vitamin C cream had a significant effect in reducing number and severity of
pregnancy striae (p
A study by Taavoni et al. [12] in 2011 aimed at assessing the effects of olive oil on striae gravidarum on 70 nulliparous women in the second trimester of pregnancy showed that striae occurred in 40% of women using olive oil, while striae were noted to occur in 50% of the control group. There was no significant difference between the intervention and control groups. The study notes that the use of olive oil until the end of the second trimester of pregnancy was not effective in reducing the occurrence of striae gravidarum (p = 0.11). Olive oil contains vitamin D and C. The finding of this research does not align with the results of study based on the use of topical compounds for the occurrence of pregnancy striae and are not in harmony. However, in this study, blinding was not done, and the control group did not use any placebo. These actions can potentially bias the study results, which may be the reason for the lack of alignment [12]. However, it is important to note that this interaction cannot be fully stated, since vitamin C and vitamin D were not used alone in the research. In the final analysis, studies consistent with the current research suggest that vitamin D performs a crucial task in skin, such as epidermal and fibroblast growth, and the humoral and cellular immune system [39]. Fibroblasts are the main cells in the dermis that produce collagen and the extracellular matrix [1]. In other words, collagen is produced by dermal fibroblasts in the extracellular matrix, and among its various types, type 1 and 3 collagens are very important in the skin and make up 80–90% of the dermis [35]. Moreover, this vitamin reduces cellular apoptosis and excessive proteolytic activity in the epidermis, thereby improving skin hydration [32]. Ultimately, it can be said that a deficiency in this vitamin leads to a deficiency in collagen synthesis, ultimately playing a role in the occurrence and severity of striae [1]. Especially during pregnancy, the need for this vitamin increases. Regarding vitamin C, it can also be said that this vitamin and its derivatives play a significant role in collagen synthesis and skin strengthening [21]. This vitamin plays an important role in maintaining the collagen network of the skin by preventing the inactivation of two enzymes, prolyl and lysyl hydroxylase, which are of great importance in collagen production [32]. This vitamin is an essential component for prolyl and lysyl hydroxylases that catalyze the production of hydroxyproline and hydroxylysine. Also vitamin C has been shown to inhibit the activation of aP-1, which leads to a reduction in MMP production and collagen damage [21]. Vitamin C also directly activates the transcription factors involved in collagen synthesis and stabilizes procollagen messenger RNA (mRNA) that regulates type 1 and 3 collagen synthesis [35]. In addition, vitamin C increases the gene expression of collagen and synthesis of the tissue inhibitor of MMP-1 (matrix metalloproteinase-1), which decreases collagen degradation [32]. In-vitro studies have also shown that vitamin C inhibits the biosynthesis of elastin. in animal studies, application of 5% ascorbic acid two hours prior to UV exposure was found to reduce skin wrinkling. Finally, its anti-aging effect involves increasing the synthesis and stabilization of collagen fibers and reducing their degradation [21]. We can say that the strength of this study was the presence of a placebo group, random candidate assignment to different groups, and blinding and concealing the candidates. Some of the constraints of this research include: it was not possible to accurately regulate the number of times the cream is used by candidates, there was a lack of information about the vitamin C and D serum levels in the samples. Further research is recommended to investigate the benefits of these creams in the treating postpartum striae, as well as their potential applicability to other populations such as persons seeking weight changes and athletes concerned about developing striae. The target groups of this study include primipara, specializing in obstetrics/gynecology, midwives, healthcare professionals, and officials and planners responsible for educational and supportive programs for pregnant. Given that supporting pregnant is a key aspect of midwifery and healthcare, one way to assist them is by preventing and treating pregnancy striae. Considering the high prevalence of striae in pregnancy and the high costs of cosmetic and medical treatments, the use of vitamin supplements can be very beneficial. Providing pregnant with adequate information about striae is essential to reduce their anxiety and worries. In this study, a cream containing vitamins C and D was used, and future studies should also consider the use of other vitamin products, such as a combination of vitamins E and C, to determine their impact on striae. Additionally, the effectiveness of this cream should be investigated, especially in women who have had multiple pregnancies.
In summary, the findings of this study demonstrate that vitamin C and D cream had an impact on diminishing the prevalence and intensity of pregnancy striae and also affected the timing of their appearance.
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
HT and MK designed the model and the computational framework and analyzed the data. HT carried out the implementation. HT and SH performed the calculations. HT and MK wrote the manuscript with input from all authors. HT and AG prepared the creams. HT and NE did the sampling. HT and MK and AG and NE and SH conceived the study and were in charge of overall direction and planning. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the ethics committee of Iran University of Medical Sciences (Approval code: IR.IUMS.REC.1401.215) and with Iran clinical trial site (registration number: IRCT20220509054799N1). Informed consent was obtained from all the candidates. This study was conducted in accordance to relevant guidelines and regulations.
This article is the result of the information obtained from the master’s thesis of midwifery education of Iran University of Medical Sciences and research project 3-1400-3-3-22271 of Iran University of Medical Sciences. The research team expresses its great gratitude to the respected research vice-chancellor of Iran University of Medical Sciences, and the authors also express their gratitude to the Clinical Research Development Unit of Shahid Akbarabadi Hospital, Iran University of Medical Sciences for conducting this research during the study period (IR.IUMS.REC.1401.215).
This work is granted by the Research Deputy of Iran university of Medical Sciences (22271-3-3-1400).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.