

 , Huihui Sun 1, Lihong Zhang 1, Xiang Li 1
, Huihui Sun 1, Lihong Zhang 1, Xiang Li 11 Department of Anesthesiology, Fuxing Hospital, Capital Medical University, 100038 Beijing, China
Abstract
Background: This study aimed to evaluate whether dexmedetomidine (DEX) can relieve postoperative pain and reduce stress reaction after laparoscopic uterine fibroids (UF) surgery. Methods: This randomized controlled study included 100 patients age range of 40–60 years, American Society of Anesthesiologists (ASA) 1–2 grade, admitted for laparoscopic UF surgery from January 2020 to October 2023. The patients were randomly allocated to the DEX group (n = 50) and non-DEX group (n = 50). The visual analogue scale (VAS), Richmond Agitation-Sedation Scale (RASS) score, anesthesia time, spontaneous breathing recovery time, consciousness recovery time, extubation time, and recovery room time were recorded. Results: The VAS of the DEX group was smaller than that of the non-DEX group at half an hour, but there was no significant difference in VAS at 1 h, 12 h and 24 h. Dex group has a RASS value closer to zero than non-DEX group at half an hour. There was no significant difference in RASS at 1 h, 12 h, or 24 h. There were differences in spontaneous breathing recovery time, consciousness recovery time, extubation time, recovery room time, chills and nausea between the two groups. Conclusion: Application of DEX in perioperative period can relieve postoperative pain, reduce stress reaction after laparoscopic UF surgery. Clinical Trial Registration: The study has been registered on https://classic.clinicaltrials.gov/ (registration number: NCT03524950).
Keywords
- dexmedetomidine
- laparoscopy
- uterine fibroids
- VAS
- RASS
Uterine fibroids are common benign tumors in women. Laparoscopic uterine fibroids (UF) surgery is currently the first choice for the treatment of uterine fibroids. However, abdominal pain and discomfort are common complications after UF surgery [1, 2].
Dexmedetomidine (DEX) is a selective
In our study, 100 patients undergoing laparoscopic UF surgery were selected. The purpose of this study was to investigate whether dexmedetomidine can promote the recovery of patients with laparoscopic UF surgery and reduce the incidence of postoperative pain and complications.
This was a pilot prospective interventional study from January 2020 to October
2023. This study was approved by the ethics review committee of Fuxing Hospital,
Capital Medical University (Ethics approval number: 2020FXHEC-KY036). Trial
registration number: NCT03524950. All patients signed the informed consent form.
This study occurred 100 patients (The power of 0.9 and Alpha of 0.05 were
calculated by PASS15 (NCSS Corp., Kaysville, UT, USA), and the sample size was 76, with 38
cases in each group. Considering a 10% increase in sample, a total of 100
patients were included. The two studies were divided into two groups with 50
cases in each group by random number table method). The inclusion criteria:
patients aged 40–60 years, American Society of Anesthesiologists (ASA) class
1–2, and undergoing laparoscopic UF surgery under general anesthesia. The
exclusion criteria: (1) hypertension; (2) thyroid disease; (3) adrenal disease;
(4) acute or chronic renal disease; (5) impaired liver function; (6) obesity
(body mass index (BMI)
One hundred patients were randomly assigned to two groups by computer random number table method: dexmedetomidine group and non-dexmedetomidine group. Random numbers were sealed in envelopes. Prior to the operation, the nurse who did not participate in the study opened the envelope and prepared the experimental drugs according to the grouping assignment in the envelope.
Dexmedetomidine group: study medication was: 0.2 mg of dexmedetomidine (Yangzijiang Pharmaceutical Company, Taizhou, Jiangsu, China) diluted with normal saline to 50 mL. The injection rate was 1 µg/kg/h of dexmedetomidine and the injection time was 10 minutes before anesthesia induction. The injection rate was 0.7 µg/kg/h of dexmedetomidine during the maintenance phase with discontinuation occurring 30 minutes before the end of the operation.
Non-dexmedetomidine group: study drug was: normal saline 50 mL. The dosage was calculated according to dexmedetomidine group.
Prior to induction of anesthesia, the experimental drugs were injected into both groups by an intravenous infusion pump for 10 minutes (pump speed: 1.0 µg/kg/h calculated according to dexmedetomidine). Patients in both groups received the experimental drug at a pump rate of 0.7 µg/kg/h and the infusion was continued until half an hour before the end of surgery. Other induction drugs used in both groups were: sufentanil 0.5 µg/kg (IDTBiologikaGmbH, Beijing, China), propofol initiated at 6 µg/mL via target-controlled infusion (TCI), and rocuronium 0.6 mg/kg.
During the maintenance phase of anesthesia, both groups received remifentanil (0.1–0.3 µg/kg/min; Yichang Renfu Pharmaceutical Co., Ltd., Yichang, Hubei, China) and propofol (AstraZeneca, S.P.A, Milano, Lombardia, Italy) continuously. The injection speed of the propofol pump was adjusted according to the bispectral index (BIS) value, with BIS value maintained between 45–55. When blood pressure rises to 30% of baseline, 10–30 mg of urapidil hydrochloride is injected intravenously. When blood pressure is reduced by 30% from baseline, 6–10 mg of ephedrine hydrochloride (Northeast Pharmaceutical Group Company Shenyang first pharmaceutical factory, Shenyang, Liaoning, China) is injected intravenously Vasoactive drugs could be reused after 10 minutes. There was no reduction in blood pressure in this study, therefore ephedrine hydrochloride was not used. After surgery: an intravenous analgesia pump was utilized (100 mL). Tropisetron Hydrochloride injection 5 mg and Flurbiprofen Axetil injection 50 mg were administered intravenously half an hour before the end of surgery to prevent postoperative nausea, vomiting and pain. When the postoperative visual analogue scale (VAS) of the patient was more than 5, Flurbiprofen Axetil injection 50 mg was injected intravenously.
The surgeon performs the operation through three small puncture sites made in the patient’s abdomen. The surgeons were senior gynecologists who have performed more than 500 laparoscopic UF surgeries.
(1) General information of the patient, included: age, height, weight, uterine fibroids diameter, number of fibroids, anesthesia time, spontaneous breathing recovery time, consciousness recovery time, extubation time, and recovery room time.
(2) Post‑operative pain: visual simulation scoring method (visual analogue scale, VAS) scores were recorded at 0.5 h, 1 h, 12 h and 24 h postoperatively. The VAS score was graded on a scale of 0–10. The score 0 was no pain and 10 was unbearable pain. The higher the score, the higher the pain level.
(3) Post operative stress response: Richmond Agitation-Sedation Scale (RASS) was recorded at 0.5 h, 1 h, 12 h and 24 h after the operation. The sedation score is on a 10-point scale, from –5 to 4.
A scale of –5 to 0 indicates coma to wakefulness, and the higher the score, the better the wakefulness. On a scale of 0 to 4, it ranges from wakefulness to agitation and violent behavior. The closer the score is to zero, the better the level of wakefulness.
(4) Postoperative chills (involuntary shaking of the whole body or part of the muscles occurs after surgery), nausea, and vomiting were recorded.
SPSS 26.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The
continuous variables conforming to the normal distribution (Kolmogorov-Smirnov
test) were presented as means
There were 50 patients in each group (Fig. 1). Their baseline characteristics are shown in Table 1. There were no significant differences in age, height, weight, diameter, or number of uterine fibroids between the two groups (Table 1).
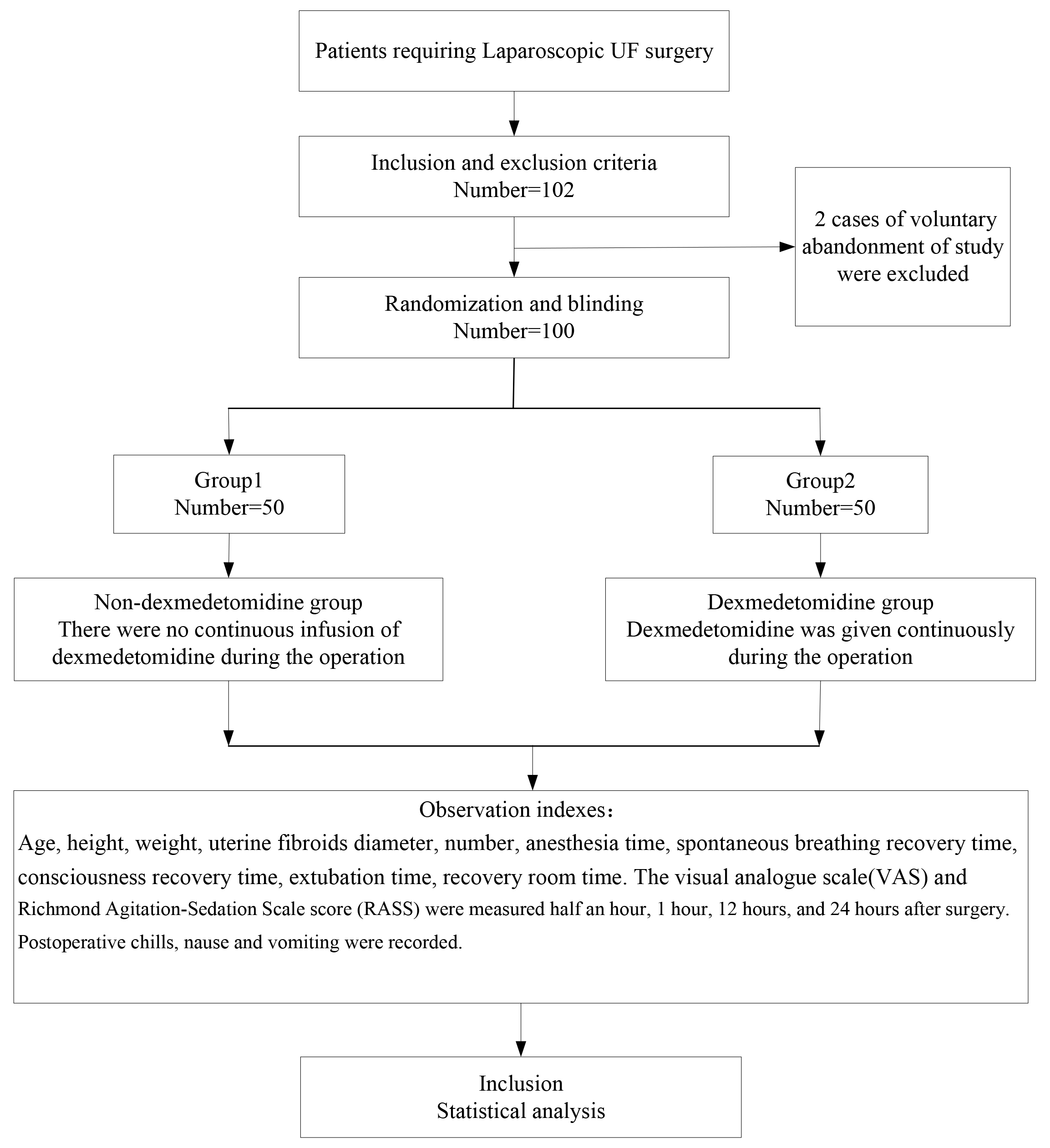 Fig. 1.
Fig. 1.Flow chart. UF, uterine fibroids.
| Characteristics | Group 1 (n = 50) | Group 2 (n = 50) | t/Z | p |
| Age (years) | 40.12 |
40.06 |
0.046 | 0.964 |
| Height (cm) | 162.64 |
162.06 |
0.584 | 0.561 |
| Weight (kg) | 59.88 |
59.60 |
0.167 | 0.868 |
| The number of uterine fibroids | 1 (1, 2) | 1 (1, 2) | 0.373 | 0.709 |
| The size of uterine fibroids (cm) | 6.26 |
6.24 |
0.059 | 0.953 |
SD, standard deviation. The number of uterine fibroids expressd as: p50 (p25, p75).
There was no difference in anesthesia time. There were differences in spontaneous breathing recovery time, consciousness recovery time, extubation time, recovery room time (Table 2), chills and nausea between the two groups (Table 3).
| Characteristics (min) | Group 1 (n = 50) | Group 2 (n = 50) | t | p |
|---|---|---|---|---|
| Anesthesia time | 115.26 |
112.44 |
0.774 | 0.441 |
| Spontaneous breathing recovery time | 6.48 |
4.10 |
7.320 | 0.000 |
| Consciousness recovery time | 16.98 |
12.00 |
6.052 | 0.000 |
| Extubation time | 18.98 |
13.88 |
6.017 | 0.000 |
| Recovery room time | 29.70 |
26.06 |
4.075 | 0.000 |
| Characteristics n (%) | Group 1 (n = 50) | Group 2 (n = 50) | p | |
|---|---|---|---|---|
| Chills | 10 (20.0%) | 1 (2.0%) | 8.274 | 0.004 |
| Nausea | 8 (16.0%) | 1 (2.0%) | 4.396 | 0.036 |
| Vomiting | 2 (4.0%) | 1 (2.0%) | 0.000 | 1.000 |
Dex group has a RASS value closer to zero than non-DEX group. There was no significant difference in RASS at 1 h, 12 h, 24 h (Table 4). The VAS of the DEX group was smaller than that of the non-DEX group at half an hour, but there was no significant difference in VAS at 1 h, 12 h and 24 h (Table 5).
| Group | RASS | |||
| 30 min | 1 hour | 12 hours | 24 hours | |
| Group 1 | –1 (–3, 0) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) |
| Group 2 | –1 (–1, 0) | 0 (–1, 0) | 0 (0, 0) | 0 (0, 0) |
| F | 2.132 | 0.522 | 0.022 | 0.010 |
| p | 0.033 | 0.602 | 0.982 | 0.992 |
RASS, Richmond Agitation-Sedation Scale.
| Group | VAS | |||
| 30 min | 1 hour | 12 hours | 24 hours | |
| Group 1 | 3 (2, 4) | 2 (1, 3) | 1 (1, 1) | 0 (0, 0) |
| Group 2 | 3 (2, 3) | 2 (1, 2) | 1 (0, 1) | 0 (0, 0) |
| F | 2.471 | 0.451 | 1.283 | 0.348 |
| p | 0.013 | 0.652 | 0.199 | 0.728 |
VAS, visual analogue scale.
The incidence of uterine fibroids is common, and large fibroids are often accompanied by various symptoms [7, 8, 9]; which can reduce the quality of life of patients. Symptoms include: excessive abnormal uterine bleeding, pain, intestinal dysfunction and bladder irritation.
Laparoscopic UF surgery is the first choice for the treatment of uterine fibroids. Because a large number of experimental studies have shown that laparoscopic UF surgery has less blood loss during the operation, shorter operative time and shorter postoperative recovery time, and it results in a lower probability of intrauterine adhesions after surgery [7, 8, 10].
However, laparoscopic UF surgery can stimulate the neuroendocrine system due to artificial pneumoperitoneum, special posture, and the use of pituitrin during the operation, which increase the secretion level of catecholamines in the body, stimulating the systemic stress response. This leads to increased conduction of the body’s nervous system [11], and increases the level of inflammatory cytokines and transmitters. For example, the increased secretion of dopamine, vasopressin, epinephrine, norepinephrine, angiotensin and cortisol [12, 13, 14, 15] leads to the enhancement of the body’s stress response. The enhancement of the stress response can cause circulation instability and a series of complications in the perioperative period.
Dexmedetomidine is a selective
In this study, spontaneous breathing recovery time, consciousness recovery time, extubation time, and recovery room time of patients in the dexmedetomidine group were lower than those in the non-dexmedetomidine group. Portelli et al. [19] study showed that the use of dexmedetomidine could shorten extubation time and reduced mechanical ventilation time. This may occur because dexmedetomidine provides analgesia, reduces the use of opioids during surgery and simulates natural sleep with maintenance of spontaneous breathing and upper airway tone [20]. This is conducive to the recovery of patients’ spontaneous breathing and consciousness after surgery.
In our study, postoperative VAS score at half an hour after surgery in the
dexmedetomidine group were lower than that in the non-dexmedetomidine group. The
dexmedetomidine group recovered better at half an hour after surgery (RASS score
was closer to zero). This may occur because dexmedetomidine reduces the release
of tumor necrosis factor-
During laparoscopic UF surgery, the use of lithotomy, pneumoperitoneum, and pituitrin can greatly cause the body stress response [24]. Therefore, we selected patients for laparoscopic UF surgery. Our study is consistent with the results of the Wu et al. [23] study. In conclusion, dexmedetomidine can relieve postoperative pain and reduce stress reaction after laparoscopic UF surgery.
This study has limitations as it was a single center study. Additional studies are necessary with expansion of sample size and utilization of other surgical centers.
Application of DEX in perioperative period can relieve postoperative pain, reduce stress reaction after laparoscopic UF surgery.
The data sets used in this article are available through the corresponding author upon reasonable request.
XC—data collection, extraction, drafting of the manuscript, analysis of data, manuscript revision; XD—data collection; HHS—data collection; LHZ—data collection; XL—analysis of data. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. This study was approved by the ethics review committee of Fu Xing Hospital, Capital Medical University. Ethics approval number: 2020FXHEC-KY036. Trial registration: NCT03524950.
We would like to express my gratitude to all those who helped me during the writing of this manuscript.
This project was supported by Fuxing Hospital, Capital Medical University PhD project started.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.