





1 Department of Psychology, Universidad Rey Juan Carlos, 28932 Alcorcón, Madrid, Spain
Abstract
Background: Pregnancy can be a stressful time that affects a woman’s
health, potentially leading to postpartum depression (PPD). Research has
highlighted the importance of certain cognitive variables in coping with
depressive symptoms. Specifically, among mothers, the perception of maternal
competence has been shown to be a protective factor against postpartum
depression. Conversely, other variables such as external locus of control (ELoC),
have been identified as risk factors, although the research in this area is less
abundant. It would be valuable to explore the role of an external locus of
control through integrative models that consider its possible interactions
throughout pregnancy and postpartum. The aim of the present study was to
evaluate the relationship between the external locus of control (at the beginning
of pregnancy) and postpartum depression (four months after childbirth), with
emotional coping as a mediating variable and maternal competence as a moderating
variable. Methods: A prospective cohort study was conducted with 120
pregnant women recruited from a public hospital in Madrid, Spain. External locus
of control was assessed by Rotter’s locus of control scale during the
first-trimester of pregnancy, non-adaptive emotional coping was assessed by
Coping Strategies Questionnaire (CAE) during the third-trimester of pregnancy,
and postpartum depression was assessed by Edinburgh Postnatal Depression scale
and perceptions of maternal competence were evaluated by Mother and Baby Scale,
both during the puerperium. Multivariate regression analyses were conducted using
a moderated mediation model, controlling for anxiety and depression.
Results: Results showed a significant mediating effect of emotional
coping between external locus of control and postpartum depression. The effect of
external locus of control on postpartum depression, considering the effect of
emotional coping, was statistically significant (direct effect:
Keywords
- low risk pregnant women
- maternal competence
- locus of control
- postpartum depression
- coping strategies
- descriptive relationship-seeking design
Pregnancy is a significant life event during which women need to restructure their life goals, behaviors, and responsibilities to achieve the integration of a new self-image [1], thereby making pregnancy and motherhood inherently stressful. From the perspective of interactionist models, this can have varying consequences, positive or negative, for both the mother and the newborn child, depending on the person-environment interaction [1]. Considering this perspective, Lazarus and Folkman’s transactional model of stress and coping has been used as an explanatory model in studies of pregnancy and motherhood [2, 3]. Due to the impact that pregnancy and postpartum have on women’s health, understanding the psychosocial variables influencing pregnancy is a relevant topic in global public health. These models, which consider the person as an active agent in their own health, emphasize two fundamental psychosocial processes: individual’s perception of the stressful stimulus and their coping processes [4]. The present study integrates two perceptual variables (i.e., locus of control (LoC) and maternal competence) and a coping mechanism (non-adaptive emotional coping) into a model that assesses psychological processes from early gestation until four months after delivery. To the best of our knowledge, while the role of the aforementioned variables have been studied independently in the context of pregnancy and motherhood, there are no known studies integrating their combined influence on the outcomes of this stressful situation, such as of postpartum depression (PPD) [5]. Specifically, the changes associated with pregnancy and motherhood require an adjustment process that is challenging for many women [6, 7], potentially leading, in some cases, to the development of PPD [8]. This can lead to feelings of sadness, fatigue, irritability, and a sense of inadequacy in coping with new maternal responsibilities [9], as previous research has indicated a strong association between symptoms of PPD and low perception of maternal competence [10, 11].
Within the interactionist models previously discussed, LoC has received considerable attention as a mediating variable between stressors such as motherhood, perceived stress (cognitive appraisals of the situation), and their consequences [12, 13]. This variable is particularly significant in the present context, as the experience of pregnancy challenges beliefs about control over health and increases perceived stress related to childbearing [14]. According to Rotter’s reformulation [15], LoC reflects a gradient wherein individuals expect varying degrees of control over their own lives. Specifically, individuals with an internal locus of control believe that their outcomes are determined by their own actions and decisions, whereas individuals with an external locus of control (ELoC) attribute their life events to external factors such as luck, chance, or other unspecified forces. Previous research on locus of control during pregnancy has identified associations of external locus of control with higher perceived stress [16, 17], unhealthy behaviors such as smoking or alcohol consumption [18, 19], preterm delivery [17], neonatal death [19], and pain during pregnancy [20]. Moreover, regarding emotional symptoms, ELoC seems to be a predictor of anxiety [21, 22], as well as both prenatal and postpartum depression [23]. The extensive research on this field suggests that prior assessment of control beliefs about pregnancy is considered essential for planning effective interventions to prevent depression during gestation and in the postpartum period [12, 13].
Another cognitive variable of interest in pregnancy and motherhood is maternal competence, recognized as a significant factor that mitigates the impact of perceived stress during pregnancy, allowing for the acquisition of caregiving behaviors, and contributes to the psychosocial development of the infant [24, 25]. Perceived maternal competence refers to an individual’s set of beliefs their ability to meet the demands of parenting and to develop adequate parenting skills [26, 27]. Increased competence promotes persistence in caregiving tasks, thereby mitigating feelings of guilt or frustration, while perceptions of incompetence appear to significantly predict depressive symptoms during initial interactions between the mother has and her baby [28]. Thus, women who feel insecure and perceive their personal resources as insufficient to meet the demands of their baby tend to attribute negative meaning to motherhood and, increasing their susceptibility to experiencing PPD [29]. However, PPD could also impair maternal ability to care for the infant [30], creating a vicious circle that is difficult to break.
From the perspective of the interactionist models of stress discussed earlier, coping strategies play a fundamental role in the perceived outcomes of a stressful situation [4]. The diathesis-stress model defines coping strategies as the cognitive and behavioral efforts individuals employ to manage or minimize the impact of stressful situations, this positioning coping strategies as a fundamental pillar of psychological well-being [4]. Among the different strategies, a distinction is made between emotion-focused and problem-based strategies depending on the objective (e.g., minimizing the unpleasant emotion or solving the problem, respectively). These strategies can be either adaptive or maladaptive, depending on their consequences for the individual. Emotion-focused coping is usually employed when a woman feels significant distress regarding the new circumstances of motherhood [31, 32], which is why it has been associated with a considerable increase in the risk of postpartum depression [33]. Specifically, emotional coping strategies such as denial, guilt, or avoidance stand out as significant predictors of depression during pregnancy [34, 35] and are associated with problems in child development [36, 37], thus being considered as non-adaptive. Conversely, adaptive coping strategies such as positive reappraisal and acceptance are associated with positive emotional states during pregnancy [38].
To the best of our knowledge, no studies have examined the role of non-adaptive emotional coping strategies as mediating variables between external locus of control and PPD, integrating all these variables at different times during pregnancy and the postpartum period. In addition, little information is available on the effect of maternal competence on these associations to guide the appropriate adaptation to motherhood. Recent research highlights the need to delve deeper into variables related to women’s personality [39]. As the previous literature suggests, studying the combined effects of ELoC, coping strategies for managing stress related to childbearing, maternal competence and postpartum depression is essential for understanding and supporting mothers during this critical process. In addition, identifying risk factors associated with gestation and/or postpartum could facilitate the development of programs promoting healthy coping strategies that contribute to the well-being of mothers and their babies. Therefore, the first aim of the current study was to explore the predictive effect of ELoC assessed in the first-trimester of pregnancy, on PPD assessed four months after delivery, and on the mediating role of non-adaptive emotional coping assessed during the third-trimester of pregnancy. Following this model, the second aim was to examine the effect of maternal competence evaluated in the postpartum period on the relationship between non-adaptive emotional coping and PPD, as well as on the relationship between ELoC and PPD.
A prospective cohort design was used for this study. Specifically, three time points were used: during the first-trimester of pregnancy (ELoC), during the third-trimester of pregnancy (non-adaptive emotional coping), and four months after delivery (PPD and maternal competence) (see Fig. 1).
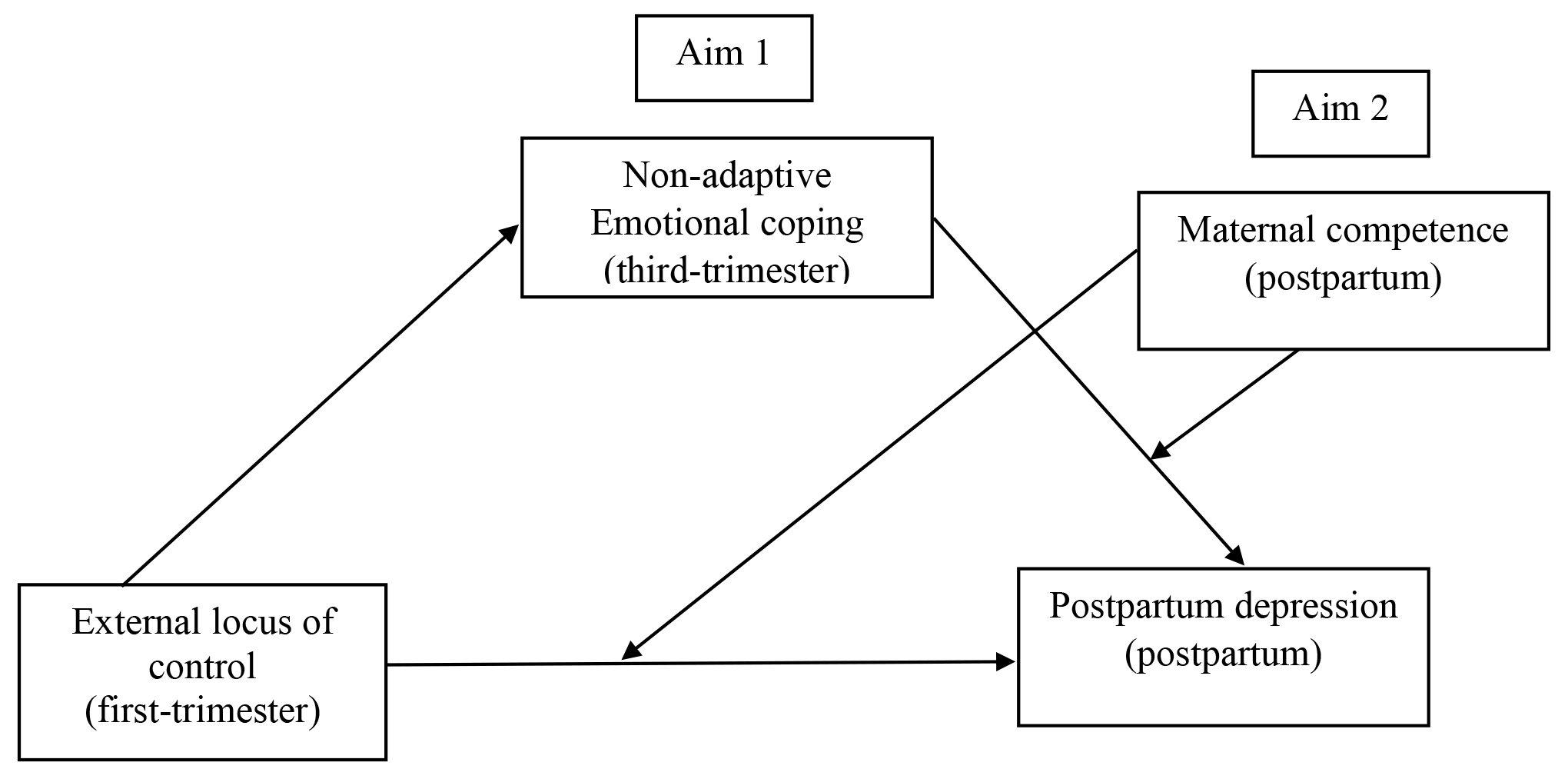 Fig. 1.
Fig. 1.Proposed model of the mediating effect of emotional coping on external locus of control (at three time points) and postpartum depression (Aim 1), considering the moderating role of maternal competence (Aim 2) and the effect of covariates (anxiety and depression symptoms).
Women in the first-trimester of pregnancy were consecutively recruited and evaluated from the Hospital Universitario de Fuenlabrada (Madrid, Spain). Inclusion criteria were as follows: (a) aged 18 years or older; (b) able to independently respond to each questionnaire responses in Spanish; (c) no history of psychiatric diagnosis before or during pregnancy (e.g., schizophrenia, depression, anxiety, personality disorder, or bipolar disorder); (d) completion of all administered questionnaires at each time point. Exclusion criteria were as follows: (a) being underage; (b) having language problems that prevent autonomous completion of the self-reports; (c) presenting severe psychiatric diagnoses; (d) presenting chronic diseases or risk pregnancy; and (e) not signing the informed consent form. Accounting for a typical sampling loss of 30%, in studies with multiple time points, a total of 290 women who completed all questionnaires during the first-trimester of pregnancy were evaluated. However, 5 women experienced miscarriages and were subsequently excluded from the study (n = 285). During third-trimester, 162 completed the questionnaires necessary to test our hypotheses. Ultimately, the total number of women who completed all postpartum evaluations was 120 (see flow diagram in Fig. 2), minimum sample required for mediation analysis [40]. Consistent with previous literature, descriptive relationship-seeking studies conducted with this population tend to experience similar sample losses at each time point [41, 42].
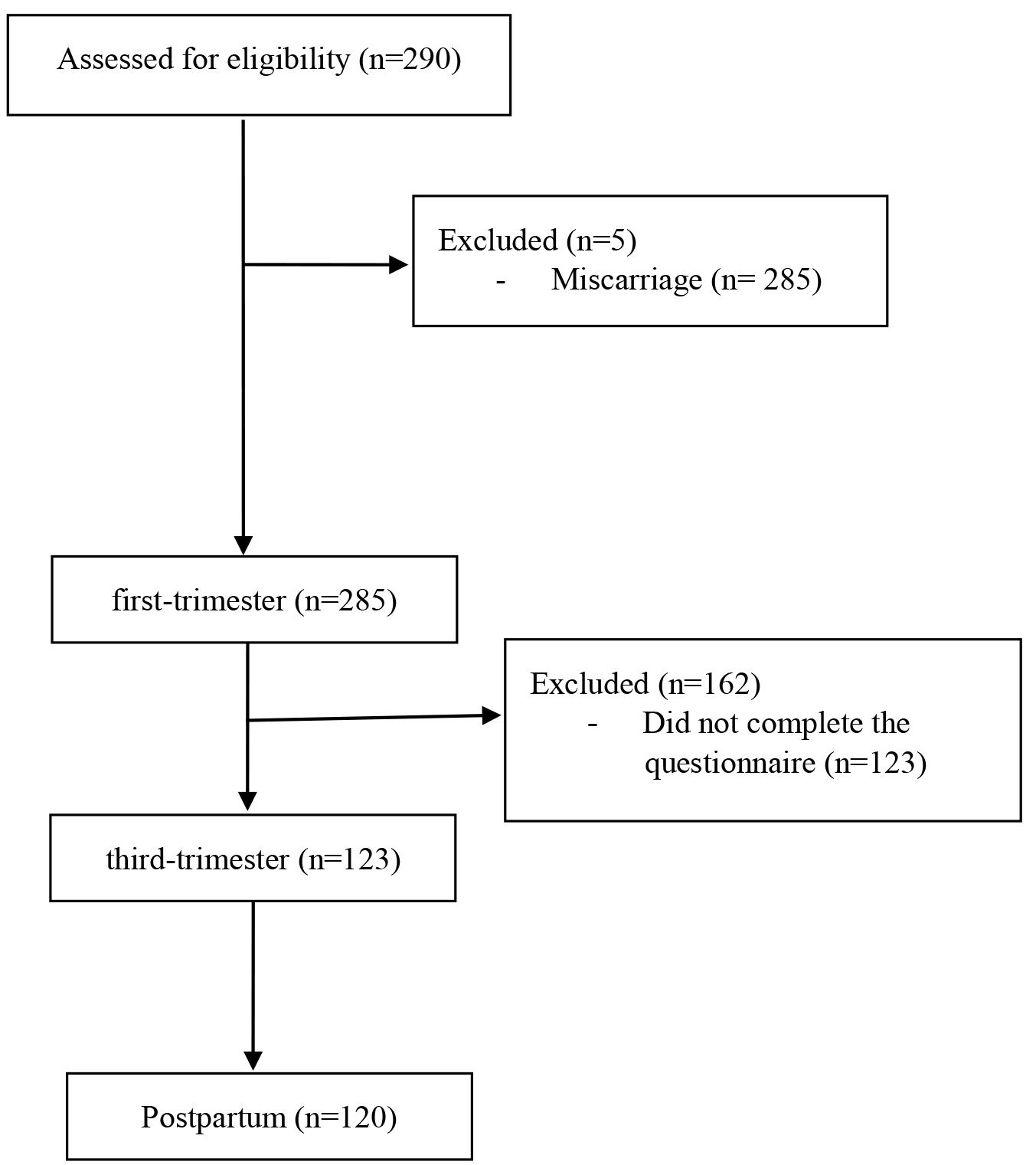 Fig. 2.
Fig. 2.Flow diagram illustrating the cohort at each stage of the study.
An ad-hoc questionnaire was used to collect this data, which included age, educational level, and employment status. Obstetric history was gathered to obtain information about previous pregnancies, type of delivery, and infant feeding practices at four months postpartum (breastfeeding or bottle feeding).
The Spanish validation [43] of Rotter’s Locus of Control Scale [15] was used to
measure external locus of control. The scale consists of 29 items, where
responses are distributed in 2 statements to assess ELoC (1 point) and internal
LoC (0 points), which are finally summed up to provide a final score ranging from
0 to 29. A higher score indicates a stronger ELoC, while lower scores indicate a
stronger internal locus of control, inconsistent with previous research [15], in
our sample, the instrument showed adequate reliability to measure the construct
(Cronbach’s alpha (
The Coping Strategies Questionnaire (CAE) [44] was used to evaluate non-adaptive emotional coping. The instrument contains 42 items that measure two main types of coping strategies: emotion-focused coping (non-adaptive strategies) and problem-focused coping (adaptive strategies), in accordance with the model of Lazarus and Folkman [4]. Responses are distributed on a 4-point Likert-type scale ranging from 0 (never) to 4 (almost always) (score range: 0–168). Higher scores indicate greater use of each of these strategies. For this study, we used the emotion-focused coping factor, which includes negative self-focused coping, overt negative emotional expression, and avoidance as non-adaptive strategies. This instrument has been employed in previous studies and has demonstrated good internal consistency [45, 46]. In our sample, Cronbach’s alpha for non-adaptive emotion-focused coping was 0.82.
Postpartum depression symptoms: postpartum assessment is usually performed
between 4 and 6 months postpartum for various considerations. Assessments at 4
months are crucial for evaluating physical recovery, wound healing, or vaginal
swelling; however, conducting postpartum assessments after 6 months can provide
more comprehensive insights into the mother’s emotional well-being. The Spanish
validation of the Edinburgh Postnatal Depression Scale (EPDS) [47] was used for
the assessment of postpartum depression. It consists of 10 items on a Likert-type
scale with scores ranging from 0 to 3 points (score range: 0–30). The validity
and reliability of the questionnaire have been confirmed in previous research
[48, 49]. Cronbach’s
Maternal competence: The Mother and Baby Scales (MBAS) [50] were used for the assessment of perceptions of maternal competence. The MBAS questionnaire allows the assessment of two types of perceptions: maternal confidence (self-efficacy) and the mother’s perceptions of infant behaviors. Specifically, concerning perceptions related to the confidence of the mother in caring for the baby (24 items), the MBAS distinguishes three dimensions: Global Confidence (3 items), Lack of Confidence in Breastfeeding (8 items), and Lack of Confidence in Caretaking (13 items). The first scale (Global Confidence) has been used in the present study. The scale has a six-point Likert-type response format (0 = not at all to 5 = a lot/very much) with a score range for global confidence of 0–15). In our sample, a Cronbach’s alpha of 0.78 was found for Global Confidence.
As a preventive measure, it was considered appropriate to assess for postpartum depression and perceived maternal competence before 6 months to monitor for potential symptoms [51, 52].
Based on the previous literature, depression and anxiety symptoms during the
third-trimester were considered as potential covariates to control for in the
proposed model. Previous studies suggest that these symptoms are more recurrent
in the third-trimester and have a more significant impact on infant development
[21, 23]. Also, depressive symptoms during this trimester of gestation, if left
untreated, can impact the mother’s health, leading to a lack of adherence to
medical recommendations. For its evaluation, the anxiety and depression subscales
of the Spanish validation of the Symptom Checklist (SCL-90-R) [53] were used.
Each subscale consists of 10 items, using a 5-point Likert-type response format
ranging from 0 (not at all) to 4 (very much). The higher the score, the greater
the symptoms of anxiety and depression. In our study, good reliability was
confirmed for both subscales (
Ethical approval was obtained from the Hospital Universitario de Fuenlabrada. Permission was obtained from the Hospital Ethics Committee, following the principles outlined in the World Medical Association’s Code of Ethics (Declaration of Helsinki). All women provided their informed consent and were guaranteed confidentiality of their data. Participation was voluntary and all participants had the option to withdraw at any time. Additionally, the researchers responsible for the project informed the participants declining to participate or withdrawing from the study would not have any negative consequences for their own health or for the health of their baby.
Data were analyzed with SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for
Windows, Version 27.0. Armonk, NY, USA). First, descriptive statistics (mean,
standard deviation (SD), percentages, and frequencies) were calculated for
demographic, obstetric characteristics, and study variables. Normality of the
data was assessed, confirming that all variables were normally distributed.
Bivariate Pearson correlations were then performed as a precondition for the
mediation analysis [54]. Second, the mediation role of non-adaptive emotional
coping (third-trimester) between ELoC (first-trimester) and PPD were tested using
the SPSS macro-PROCESS (model 4, see Fig. 1). The model tested used regression
and bootstrapping to generate a confidence interval (CI) for the mediation effect
(statistical significance was set at an alpha level of 0.05). Based on these
results, model 15 of SPSS macro-PROCESS was tested to verify the moderated effect
of maternal competence by non-adaptive emotional coping between ELoC and PPD
(Fig. 2). Product terms of non-adaptive emotional coping
Table 1 shows the demographic and obstetric characteristics of mothers. The mean age was 31.28 (SD = 3.96). At the beginning of the pregnancy, the majority of women (68.1%) were working. Regarding obstetric characteristics, half of the women (51.3%) were first-time mothers, and more than half (57.7%) had a vaginal delivery.
| Characteristics | n | % | Mean | SD | Max | Min | |
| Age | 31.28 | 3.96 | 42 | 23 | |||
| Occupation | |||||||
| Employed | 81 | 68.1 | |||||
| Unemployed | 39 | 31.9 | |||||
| Education level |
|||||||
| Primary education (level 1) | 58 | 48.3 | |||||
| Upper secondary education (level 3) | 34 | 28.4 | |||||
| Bachelor’s or equivalent (level 6) | 28 | 23.3 | |||||
| Parity | |||||||
| Primiparous | 62 | 51.3 | |||||
| Multiparous | 58 | 48.7 | |||||
| Mode of birth | |||||||
| Vaginal | 73 | 57.7 | |||||
| Cesarean | 28 | 25.2 | |||||
| Instrumental | 19 | 17.1 | |||||
| Infant feeding pattern (postpartum) | |||||||
| Breastfeeding | 62 | 51.7 | |||||
| Bottle-feeding | 58 | 48.3 | |||||
Table 2 shows means, SDs, and Pearson correlations for the continuous variables.
ELoC was positively correlated with emotional coping (p = 0.001) and
with PPD (p = 0.019), while correlating negatively with maternal
competence (p = 0.029). Emotional coping was positively correlated with
PPD (p = 0.001) and negatively with maternal competence (p =
0.004). PPD was negatively correlated with maternal competence (p
| Mean (SD) | Theorical range | 1 | 2 | 3 | 4 | 5 | |
| 1. External locus of control | 13.24 (3.40) | 1–22 | – | ||||
| 2. Emotional coping | 13.16 (5.06) | 2–27 | 0.323** | – | |||
| 3. Postpartum depression | 11.08 (2.86) | 0–22 | 0.138* | 0.352** | – | ||
| 4. Maternal competence | 15.03 (3.05) | 0–18 | –0.129* | –0.336** | –0.431** | – | |
| Covariates | |||||||
| 5. Anxiety symptoms third-trimester | 0.62 (0.20) | 0–10 | 0.341* | 0.479** | 0.532** | –0.304** | – |
| 6. Depressive symptoms third-trimester | 7.61 (0.48) | 1–10 | 0.182 | 0.542** | 0.465** | –0.351** | 0.373** |
*p
Regarding covariates (symptoms of anxiety and depression in the third-trimester
of pregnancy), ELoC was positively correlated with anxiety symptoms (p = 0.001). Emotional coping was positively correlated with anxiety (p
According to the assumptions raised by Hayes (2017) [54], variables that are significantly associated can be posed in mediation and/or moderation models. Therefore, anxious and depressive symptoms were included as covariates in the proposed model.
In line with the first objective of this study, the mediating role of emotional
coping during the third-trimester pregnancy was explored. Anxiety and depressive
symptoms during the third-trimester were used as covariates. Results showed that
emotional coping significantly mediated the relationship between ELoC and PPD, as
the CI was above zero. The total effect (c = 0.351, t = 2.37, p = 0.020,
[95% CI = 0.057/0.064]) and the direct effect were both statistically
significant (
Regarding covariates, a significant effect of depressive symptoms during
gestation was observed (
Building on the previous mediation model, this study tested the indirect effect
of ELoC (during first-trimester) on PPD through emotional coping (during
third-trimester), moderated by maternal competence (during postpartum).
Similarly, depressive and anxious symptoms during the third-trimester were again
included as covariates. The results show a moderating effect of maternal
competence on the relationship between non-adaptive emotional coping and
postpartum depression (
| B (SE) | t | p-value | [LLCI/ULCI] | ||
| Outcome: Emotional coping (EC) | |||||
| ELoC | 0.461 (0.194) | 2.94 | 0.004 | [0.149/0.771] | |
| Anxiety symptoms third-trimester (covariate) | 2.27 (1.83) | 1.23 | 0.222 | [–1.42/5.96] | |
| Depressive symptoms third-trimester (covariate) | 1.24 (1.06) | 1.63 | 0.530 | [–2.70/5.19] | |
| Outcome: Postpartum depression (PPD) | |||||
| ELoC | 4.76 (1.81) | 2.62 | 0.018 | [–8.37/–1.28] | |
| Emotional coping (EC) | 2.14 (0.815) | 2.17 | 0.009 | [1.63/2.82] | |
| Moderator: maternal competence (MC) | –4.90 (1.61) | –3.03 | 0.004 | [–8.15/–1.64] | |
| Interaction 1: EloC |
–0.301 (0.112) | –2.66 | 0.010 | [–0.525/–0.073] | |
| Interaction 2: EC |
–0.412 (0.051) | –2.06 | 0.009 | [–0.105/–0.099] | |
| Anxiety symptoms third-trimester (covariate) | 2.14 (1.91) | 1.12 | 0.268 | [–1.70/6.00] | |
| Depressive symptoms third-trimester (covariate) | 0.447 (2.26) | 0.197 | 0.844 | [–4.11/5.00] | |
| Conditional effect of MC on the relationship between EC and PPD | |||||
| Low: 13.25 | 0.832 (0.382) | 2.176 | 0.035 | [1.60/0.062] | |
| Medium: 15.03 | –0.119 (0.203) | –0.551 | 0.584 | [–0.584/0.297] | |
| High: 17.90 | –0.608 (0.287) | –2.117 | 0.039 | [–0.300/–1.18] | |
| Global model: Conditional effect of MC on the relationship between ELoC and PPD through the mediation of EC | |||||
| Low: 13.25 | 0.132 (0.068) | 1.92 | 0.055 | [–0.003/0.266] | |
| Medium: 15.03 | –0.195 (0.052) | –3.74 | [–0.297/–0.092] | ||
| High: 17.90 | –0.258 (0.066) | –3.86 | [–0.391/–0.127] | ||
| Indirect effects | |||||
| Direct effects | |||||
| Total effect | |||||
B, unstandardized beta; SE, standard error for the unstandardized beta; LLCI/ULCI, lower level confidence interval/upper level confidence interval; ELoC, external locus of control; EC, emotional coping; PPD, postpartum depression; MC, maternal competence; CI, confidence interval.
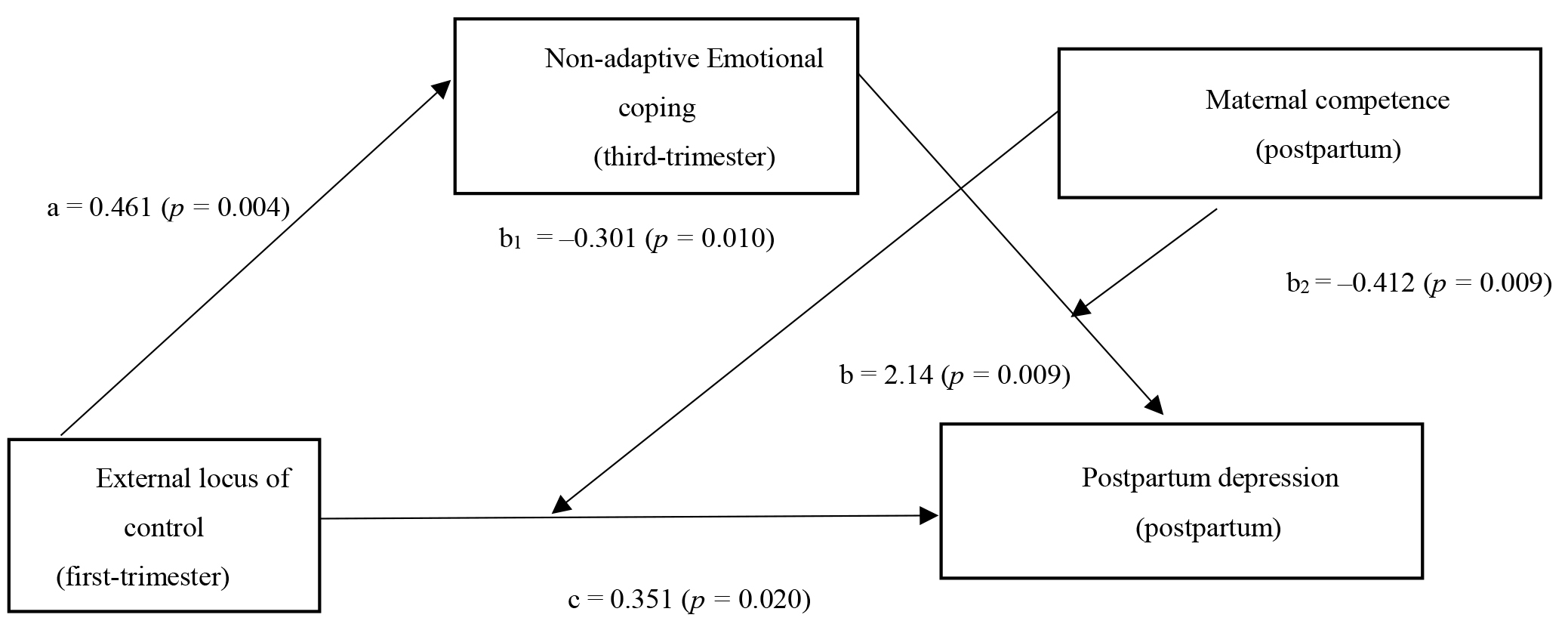 Fig. 3.
Fig. 3.Coefficients of the proposed model of the mediation effect of
emotional coping in the relationship between external locus of control and
postpartum depression, moderated by maternal competence. a, b, b
The present study aims to explore, from an interactionist perspective, the mediating role of maladaptive emotional coping strategies in the relationship between external locus of control and PPD, while considering the possible moderating role of maternal competence. Our results suggest that external locus of control is associated with increased use of non-adaptive emotional coping strategies, which in turn contributes to greater symptoms of postpartum depression. Interestingly, these associations may weaken in the presence of moderate and high levels of perceived maternal competence.
In relation to the first aim of the present study, ELoC predicted the occurrence of PPD through the mediating effect of non-adaptive emotional coping strategies. This type of coping can manifest in specific behaviors, such as maladjusted and uncontrollable expressions of negative emotions, including confrontation and anger towards other people. Previous studies have shown that this type of coping can lead women to adopt strategies based on guilt and resignation, thereby potentially exacerbating depressive symptoms [55]. Similarly, previous research has identified a relationship between external locus of control and PPD [22]. These results align with studies suggesting that mothers with an external locus of control exhibit less persistence in addressing parenting challenges, take less responsibility for the infant’s health status, refrain from seeking information, have lower tolerance for delays in the neonatal development, and consequently, may experience less success in effective parenting [56]. This shows the importance of examining the perceived lack of control during pregnancy, as it may hinder the adjustment to motherhood and prevent emotional disorders during pregnancy or postpartum [23]. Similarly, previous research conducted with low-risk pregnant women suggested that coping styles varies throughout pregnancy, with (non-adaptive) emotional coping being the style most associated to depressive states [38, 57, 58]. Our results show that the longitudinal assessment of prenatal coping is particularly relevant in highlighting effective strategies that reduce maternal postpartum depression and contribute, in turn, to maternal-infant well-being.
The prenatal period presents an opportunity for early identification of risk
factors to help prevent PPD, supported by previous studies indicating that
depression during pregnancy is one of the most significant predictors [59, 60].
Indeed, our data corroborate the role of prenatal emotional symptoms in
predicting postpartum depression within the simple mediation model considered
(external locus of control
In our opinion, our results have important clinical implications for low-risk pregnant women. This study examined the influence of external locus of control and emotional coping on the occurrence of PPD in a longitudinal descriptive relationship-seeking study, from the beginning of pregnancy until four months after delivery. External locus of control combined with non-adaptive emotional coping are shown to be clear risk factors for PPD. According to the transactional model of stress and the cognitive diathesis-stress model of depression, psychological vulnerability factors such as perception and coping interact with stressful events to increase the likelihood and/or occurrence of depression [62, 63].
Of special relevance is the buffering role of the maternal competence against the negative effects of the aforementioned variables (e.g., ELoC, emotional coping). In clinical contexts, studies with pregnant women suggest that maternal identity integration is a protective factor for PPD. This is due to the observed relationship between depression and feelings of being a “bad mother”, stemming from perceptions of neglect and inadequate care toward their children [10]. One personal resource that may enable women to negotiate motherhood competently and adaptively is acquiring a repertoire of behaviors to regulate emotions such as guilt or frustration, and addressing cognitive factors that might interfere with infant care. From the theoretical framework of maternal role attainment [64, 65] our study underscores the importance of working on maternal competence through behavioral modification to mitigate the effects of PPD. From this perspective, various psychological interventions have focused on improving competency beliefs through techniques aimed at reducing maladaptive behaviors and promoting healthy ones [66, 67]. Therefore, implementing programs aimed at improving self-efficacy during pregnancy seem particularly relevant, with further research needed to explore optimal interventions and associated contextual variables, given insufficient results regarding the long-term efficacy of interventions for pregnant women predisposed to PPD [66, 67, 68]. In this regard, prenatal education programs can be useful in providing the knowledge on skills and risk factors that can help pregnant women prevent PPD. Bringing together midwives, nurses, and other health providers can facilitate the establishment of consistent procedures for assessing past and present psychosocial stressors that may affect women’s health from the first-trimester of pregnancy through the postpartum period.
The present study has certain limitations to be considered. Firstly, the small sample size and recruitment from a single hospital limit the generalization of the results obtained. Nevertheless, our research design, which incorporates measurements at three different points in time, allows us to explore various predictors of PPD across different stages of the perinatal period, although future research should incorporate additional variables. Secondly, the data obtained relies on self-report measures, which are subject to well-known limitations such as response biases influenced by the participants’ desire to present themselves favorably. Regardless, the measures used in our study demonstrate good psychometric properties. Lastly, the perception of maternal competence may be influenced by socio-demographic, ethnic, and cultural variables that were not included in this study. Regarding the sample size, the observed attrition may introduce bias in interpreting consistent results over time, although similar studies using the same methodology also reported similar sample losses [41, 42].
Despite the previous limitations, our results support the mediating effect of the use of non-adaptive coping strategies, in this case emotional, between the external locus of control and postpartum depression. Previous literature points out the relationship between external locus of control and depression, but research on the influential mechanisms is less abundant, especially in the case of maternal mental health. Thus, the detection and intervention of non-adaptive strategies during stressful situations such as pregnancy and motherhood appears to be a proactive approach in the promoting of maternal health. On the other hand, regarding protective factors, beliefs of competence as a mother play a clearly buffer the effects of external locus of control on postpartum depression through maladaptive coping. These results are of special relevance considering the prospective nature of the research and the finding that prenatal anxious-depressive symptoms (covariates) did not significantly influence the proposed moderated mediation model. Therefore, promoting maternal competence can serve as a positive resource for reducing postpartum depression and supports the transition to the maternal role as an integrated part of one’s own identity.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
LGH participated in conceptualization, data curation, investigation, methodology, resources writing—original draft, supervision and validation. PCM participated in conceptualization, methodology, resources, data curation; writing—original draft preparation. CÉG participated in conceptualization, methodology, resources, data curation; writing—original draft preparation. CPP participated in conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, writing review and editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethics Committee of Fuenlabrada University Hospital in Madrid, Spain. Written informed consent was obtained from all participants.
The authors gratefully acknowledge all the participants for their collaboration and enthusiasm. We thank Dr. Dolores Marín for her invaluable collaboration in the initiation of this research.
This work was supported by the Health Research Fund (Fondo de Investigaciones Sanitarias, FIS), Instituto de Salud Carlos III (Spain) (Reference PI07/0571).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.