


 , Jie Shen 1, Bing Han 1, Qin Huang 1, Youguo Chen 1
, Jie Shen 1, Bing Han 1, Qin Huang 1, Youguo Chen 11 Department of Obstetrics and Gynecology, The First Affiliated Hospital of Soochow University, 215006 Suzhou, Jiangsu, China
Abstract
Background: Nausea and vomiting are common and unpleasant symptoms for pregnant women during cesarean section, which can lead to aspiration, a serious complication that can cause pneumonia. This study aimed to evaluate the effects of oral multi-vitamin carbohydrate beverage on maternal intraoperative nausea and vomiting by gastric ultrasound. Methods: This was a single-center, randomized controlled trial. According to their diet, pregnant women who were converted from vaginal delivery to cesarean section were divided into two groups: the observation group (multi-vitamin carbohydrate beverage) or the control group (semi-solid food). The cross-sectional area (CSA) of the gastric antrum was measured by ultrasound before cesarean section, and the occurrence of intraoperative nausea, vomiting, and aspiration was recorded in both groups. Results: The CSA of the gastric antrum at 1 h, 2 h, after eating, and before cesarean section in the observation group was significantly smaller than that in the control group. This suggests that an oral multi-vitamin carbohydrate beverage needs less gastric emptying time. The incidence of vomiting in the observation group was significantly lower than that in the control group. Moreover, the pH of the vomited fluid in the observation group was higher than that in the control group, indicating that oral multi-vitamin carbohydrate beverage may reduce the acidity of stomach contents, which can further reduce the risk and severity of vomiting. Conclusions: Oral multi-vitamin carbohydrate beverage can promote gastric emptying and reduce the incidence and harm of vomiting during urgent cesarean section. This dietary intervention may be a simple and effective way to improve maternal outcomes during cesarean section. Clinical Trial Registration: The study has been registered on https://classic.clinicaltrials.gov/ (registration number: NCT06333626).
Keywords
- multi-vitamin carbohydrate
- cesarean section
- nausea and vomiting
- gastric ultrasound
Nausea and vomiting are common and unpleasant symptoms for pregnant women during cesarean section and can be caused by anesthesia, vagal hyperactivity, opioid drugs, and numerous other factors [1, 2]. Nausea and vomiting can further increase the risk of aspiration pneumonia, a serious complication that can lead to respiratory problems and even death [3, 4, 5, 6].
Traditionally, pregnant women were advised to fasting during labor to minimize the risk of aspiration during cesarean section. However, recent studies have shown that fasting is not only unnecessary but can also be harmful [7, 8]. Importantly, fasting during labor may cause ketosis, and the acidic stomach juice is dangerous to pregnant women if aspiration occurs [9, 10].
According to a study of more than 1200 hospitals in China, most hospitals allow pregnant people to drink water or eat easily digestible food as desired during labor [11]. The Chinese Society of Anesthesiologists encourages pregnant women to consume a multi-vitamin carbohydrate beverage to meet the increased energy requirement during labor [12]. Studies have shown that oral carbohydrate ingestion does not affect the outcome of labor [13, 14, 15]. However, studies of oral carbohydrates on maternal vomiting and the risk of aspiration during urgent cesarean section are still lacking.
Gastric ultrasound is a very simple and non-invasive bedside diagnostic tool for assessing gastric content qualitatively and quantitatively [16, 17]. In this study, we used gastric ultrasound to evaluate the gastric emptying of an oral multi-vitamin carbohydrate beverage on pregnant women.
This was a single-center, randomized controlled trial conducted from January to December 2021 which compared the cross-sectional area (CSA) of pregnant women converted from vaginal delivery to cesarean section who received either a multi-vitamin carbohydrate beverage or semi-solid food.
The inclusion criteria were as follows: (1) 18–40 years old; (2) at least 37 weeks pregnant; (3) had not eaten for at least 4 h before entering the delivery room; (4) converted from vaginal delivery to cesarean section. The exclusion criteria were as follows: (1) gestational diabetes mellitus or gastroesophageal reflux disease; (2) cesarean section performed under general anesthesia.
The PLAN procedure of the SAS 9.4 software (SAS Institute, Cary, NC, USA) was used to create a random sequence. The pregnant people would be in the observation group if the random number was between 1 and 45. The pregnant people would be in the control group if the random number was between 46 and 90. According to the diet, the pregnant patients converted from vaginal delivery to cesarean section were included and divided into the observation group (multi-vitamin carbohydrate beverage) or the control group (semi-solid food). The Clinical Nutrition Center of our hospital provided the multi-vitamin carbohydrate beverage (energy 840 kJ, carbohydrates 50 g, sodium 157.5 g, vitamin B1 0.84 mg, vitamin B6 0.45 mg, vitamin B12 0.5 µg, zinc 5.2 mg, taurine 175 mg, 350 mL). The semi-solid food was soft noodles provided by the canteen in the hospital (350 g).
The gastric content was quantitatively assessed by measuring the CSA of the stomach antrum using gastric ultrasound. The gastric ultrasound was performed by an experienced obstetrician with more than three years of obstetric ultrasound experience, who was blinded to the group assignment. The upper abdomen of the pregnant woman was scanned in the semi-recumbent position using a parasagittal section to obtain a clear CSA standard section image of the antrum (Convex probe, 2–5 MHz; Edge II, SonoSite, Bothell, WA, USA). The ring tool of the ultrasound instrument was utilized three times for each measurement to obtain an average value for the CSA area (Fig. 1).
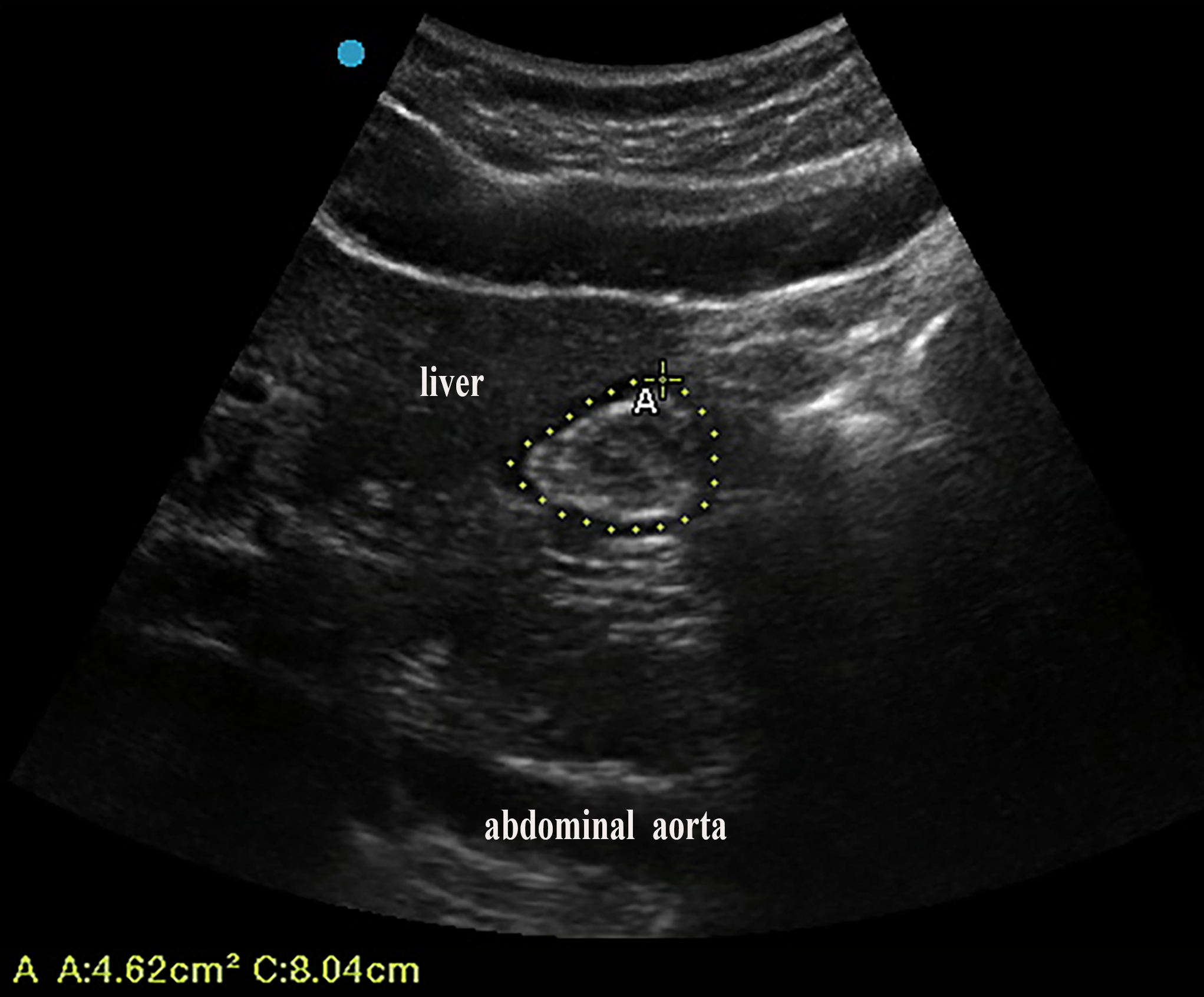 Fig. 1.
Fig. 1.A maternal standard ultrasonic image of the CSA of the gastric antrum. CSA, cross-sectional area; A, area.
The midwives blinded to the group assignment asked for the thirst and hunger scores (score 0–3, 0 for no thirst or hunger, 1 for mild thirst or hunger, 2 for tolerable thirst or hunger, and 3 for intolerable thirst or hunger) of the two groups before entering the operating room. They recorded the occurrence of nausea, vomiting, and aspiration during urgent cesarean section. A pen pH meter (PHB3, Sanxin, Shanghai, China) was used to record the pH value of the vomited fluid when it was present.
The primary outcome of this study was to compare the CSA of the gastric antrum before urgent cesarean section in the two groups. The secondary outcomes included: the CSA of gastric antrum before and at 1 h and 2 h after eating, the thirst and hunger scores before entering the operating room, and the occurrence of nausea, vomiting, and aspiration during urgent cesarean section.
The sample size calculation was based on previous studies about the maternal CSA
of the gastric antrum after eating [18, 19]. We determined that 45 participants in
each group were required, including a 10% dropout rate. SPSS 26.0 statistical
software (IBM Corporation, Armonk, NY, USA) was used for statistical analyses.
Quantitative data were expressed as the mean
A total of 90 pregnant women were eligible for analysis. They were randomized
equally between the observation and control groups. As shown in Fig. 2, 2 women
in the observation group and 3 women in the control group were excluded due to
the use of general anesthesia during urgent cesarean section; 3 pregnant women in
the observation group and 1 pregnant woman in the control group were excluded due
to incomplete data. Forty women in the observation group and 41 women in the
control group were finally included. There was no statistical difference in age,
body mass index (BMI), weeks of gestation, proportion of primipara, and labor
analgesia between the two groups (p
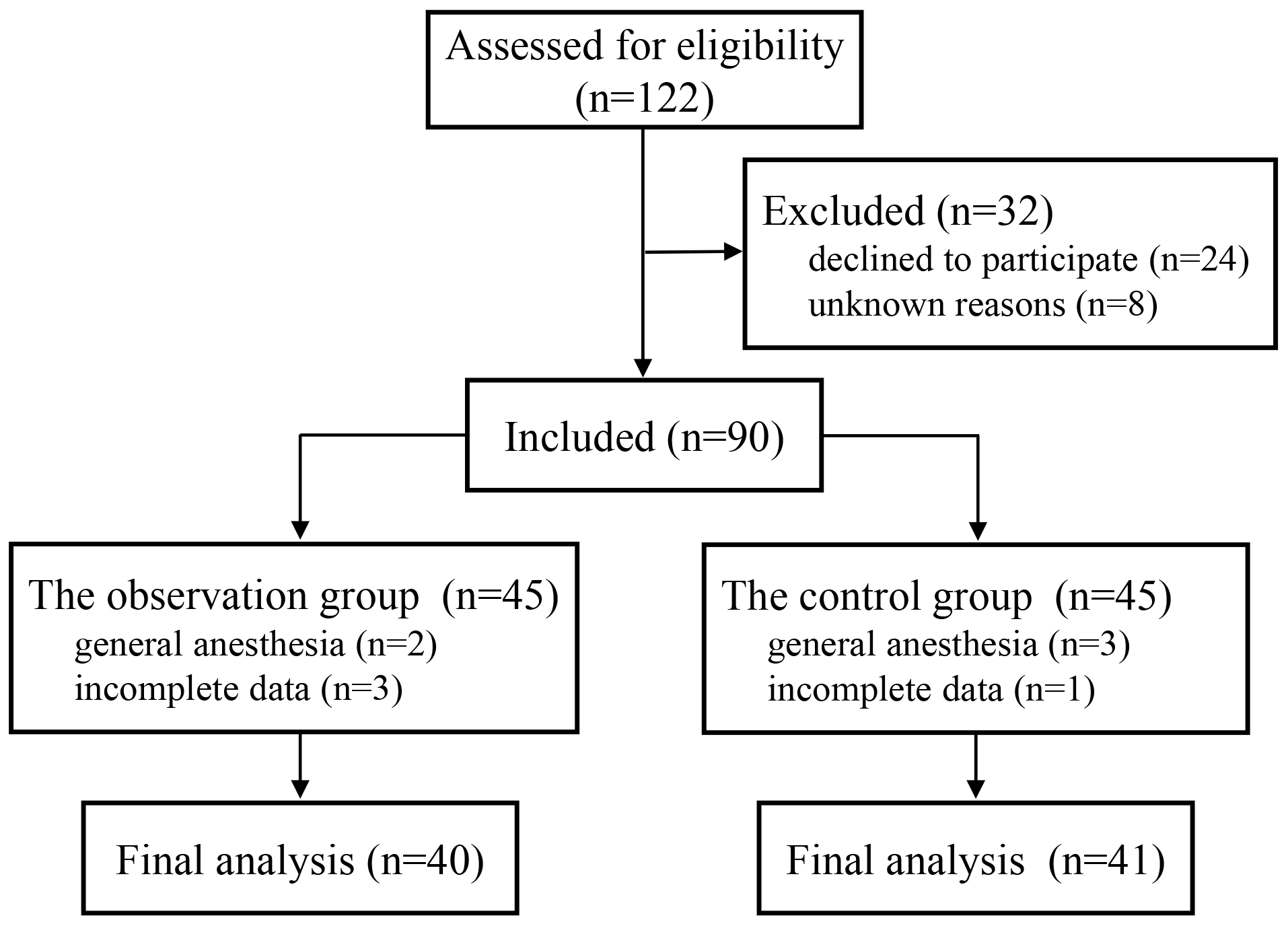 Fig. 2.
Fig. 2.Participant flow.
| Observation (n = 40) | Control (n = 41) | p value | |
| Age (years) | 29.0 |
29.6 |
0.457 |
| BMI (kg/m |
26.2 |
25.7 |
0.407 |
| Gestation weeks | 39.1 |
39.4 |
0.145 |
| Primipara (n) | 37 | 38 | |
| Labor analgesia (n) | 31 | 35 | 0.362 |
BMI, body mass index.
As shown in Table 2, there was no statistical difference in the CSA of the
gastric antrum before and immediately after eating between the two groups
(p
| Observation (n = 40) | Control (n = 41) | p value | |
| Before eating | 5.6 |
5.8 |
0.496 |
| After eating | 12.3 |
12.4 |
0.766 |
| 1 h | 7.8 |
11.1 |
|
| 2 h | 6.1 |
8.8 |
CSA, cross-sectional area.
The differences in thirst and hunger scores and the time after eating before
entering the operating room were not statistically significant between the two
groups (p
| Observation (n = 40) | Control (n = 41) | p value | |
| Thirst (n) 0/1/2/3 | 10/25/5/0 | 12/24/5/0 | 0.779 |
| Hunger (n) 0/1/2/3 | 9/24/7/0 | 13/24/4/0 | 0.267 |
| Time after eating (min) | 70.2 |
66.6 |
0.259 |
| CSA (cm |
4.7 |
6.9 |
Score 0–3: 0 for no thirst or hunger, 1 for mild thirst or hunger, 2 for tolerable thirst or hunger, and 3 for intolerable thirst or hunger.
There was no statistically significant difference in the incidence of
intraoperative nausea between the two groups (p
| Observation (n = 40) | Control (n = 41) | p value | |
| Nausea (n) | 33 | 32 | 0.615 |
| Vomiting (n) | 11 | 25 | 0.002 |
| pH | 4.7 |
3.4 |
|
| Aspiration (n) | 0 | 0 | - |
Pregnant women require a significant amount of energy during labor, with an average vaginal delivery length of approximately 9 hours demanding over 3000 kJ of energy [20]. Therefore, before entering the delivery room, pregnant women need to consume food to obtain sufficient energy. Maternal gluconeogenesis and fat mobilization can increase the generation of ketone bodies if energy intake is insufficient [21]. In addition to water and clear drinks, most medical institutions in China usually recommend semi-solid food such as soft noodles and congee, considering that solid food is not easily digestible and can cause a prolonged full stomachs [11]. However, it was found that maternal gastric emptying time remained significantly slower compared to the non-pregnant controls due to factors such as painful uterine contractions after eating semi-solid food [19]. The delayed gastric emptying can increase the risk of aspiration when pregnant women need to transition from vaginal delivery to urgent cesarean section. Aspiration, though rare, can lead to severe consequences, including aspiration pneumonia and potential cardiac arrest [22]. Therefore, evaluating the effectiveness of an oral multi-vitamin carbohydrate beverage consumed during labor is of great clinical significance.
Gastric ultrasound techniques can visually provide information on gastric contents and gastric volume. Gastric ultrasound techniques can assist in determining the risk of aspiration by using a stomach volume assessment based on the CSA in the sinus area at standard views. Previous studies have demonstrated that even inexperienced sonographers can reliably obtain the CSA of the gastric antrum using a simple standard view [23, 24, 25]. In this study, we employed gastric ultrasound to examine maternal gastric emptying before and after consuming different diets. We determined that the CSA of the gastric antrum was significantly reduced at 1 h and 2 h after eating in pregnant women on an oral multi-vitamins carbohydrate beverage compared with women consuming semi-solid food. The CSA of pregnant women on an oral multi-vitamin carbohydrate beverage before entering the operating room was significantly smaller than that of the women on semi-solid food. This may occur because a multi-vitamin carbohydrate beverage is a clear liquid that can be quickly emptied, and it presents no difference in thirst and hunger sensation.
Nausea and vomiting during cesarean section are commonly associated with factors such as hypotension, full stomach, surgical traction, and opioid drugs [26]. While our study found no significant difference in intraoperative nausea between the two groups, the incidence of intraoperative vomiting was significantly lower in pregnant women who consumed an oral multi-vitamin carbohydrate beverage compared to those who consumed semi-solid food. Additionally, the pH of the vomited fluid in the oral multi-vitamin carbohydrate beverage group was significantly higher than that of the semi-solid food group. This suggests that the dilution effect of a multi-vitamin carbohydrate beverage may reduce gastric acid secretion, contributing to the lower vomiting incidence. Although aspiration was not observed in either group, its potential severity highlights the importance of interventions that can minimize the risk of this complication. Studies have shown that a lower pH of aspirated fluid is associated with a poorer prognosis, emphasizing the potential benefit of an oral multi-vitamin carbohydrate beverage in reducing the harm of intraoperative aspiration [22, 27, 28].
There are some limitations of this study. First, pregnant women who ate semi-solid food required a longer time than those who drank a multi-vitamin carbohydrate beverage, resulting in a delay in measuring CSA. Second, this study only included urgent cesarean sections with intraspinal anesthesia and did not consider urgent cesarean sections with general anesthesia. Finally, our study employed a single-blind design, with pregnant women aware of the intervention they received. This lack of blinding could have introduced bias into the study outcomes.
Our study demonstrates that an oral multi-vitamin carbohydrate beverage can significantly expedite maternal gastric emptying, thereby reducing the incidence and harm of intraoperative vomiting during urgent cesarean delivery. This finding holds considerable clinical significance, particularly in the context of urgent cesarean sections, where rapid gastric emptying can potentially minimize the risk of aspiration and its associated complications.
All data generated or analyzed during this study are included in this published article.
MS and JX designed the study. JX, JS, and MS performed the research, collected data. MS and BH analyzed the data, advised on writing manuscript and revised manuscript. JX wrote manuscript. JX and MS analyzed the data. QH and YC analyzed and interpreted the data and revised manuscript. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University (approval number: 2020-281). The study has been registered on https://classic.clinicaltrials.gov/ (registration number: NCT06333626).
We thank Dr. Jing Yang of the Department of Nutrition and Dr. Qianru Sun of the Department of Ultrasonography at the First Affiliated Hospital of Soochow University for their assistance and Dr. Wei Guo from the Department of Epidemiology and Statistics, Soochow University, for her guidance in statistics.
This study was supported by the Medical Research Project of the Jiangsu Commission of Health (grant no. H2019010).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.