
 , Yao Chen 2, Bairong Xia 3, Wulin Shan 3, Tingwei Xing 1, Weiwei Wei 1, Bin Tang 1, Yu Du 1, Hong Zheng 1
, Yao Chen 2, Bairong Xia 3, Wulin Shan 3, Tingwei Xing 1, Weiwei Wei 1, Bin Tang 1, Yu Du 1, Hong Zheng 11 Department of Gynecology and Obstetrics, The Affiliated Changzhou No.2 People's Hospital of Nanjing Medical University, 213003 Changzhou, Jiangsu, China
2 Department of Gynecology and Obstetrics Graduate School, Bengbu Medical College, 233030 Bengbu, Anhui, China
3 Department of Gynecology, The First Affiliated Hospital of the University of Science and Technology of China, Division of Life Sciences and Medicine, University of Science and Technology of China, 230031 Hefei, Anhui, China
Abstract
Objective: Myomas of the uterus are the most common benign tumors of the female reproductive system. This article presents a detailed review of the suturing methods and ancillary techniques for uterine incision used in transumbilical single-port laparoscopic myomectomy in order to provide a reference for beginners and a research direction for the future development of this surgery. Mechanism: The authors reviewed credible search engines and literature databases (such as PubMed) for the period 2000–2023, extracted published data and content, and summarized the collected information. This was combined with the authors own surgical experience to provide a detailed description of the suture methods and ancillary techniques for uterine incision used in transumbilical single-port laparoscopic myomectomy. Findings in Brief: This review provides a comprehensive understanding of the suture methods and ancillary techniques for uterine incision commonly used in transumbilical single-port laparoscopic myomectomy. The advantages and limitations of different methods are also recognized. Conclusions: Suture methods for uterine incision in transumbilical single-port laparoscopic myomectomy include: simple interrupted suture, figure-of-eight suture, interrupted mattress suture, simple continuous suture and baseball type suture. Ancillary techniques for uterine incision in transumbilical single-port laparoscopic myomectomy include: needle hook assisted method, suspended line method, one-handed operation method and the modified operative method.
Keywords
- laparoendoscopic single-port surgery
- trans-umbilical
- myoma of uterus
- suture methods
- ancillary techniques
Uterine fibroids are the most common benign tumors of the female reproductive system, with a prevalence of up to 75% in women of childbearing age, while the incidence of uterine fibroids in post-menopausal women being significantly lower [1]. With the development of minimally invasive surgery, laparoscopic techniques have matured with the pursuit of minimally invasive procedures increasing. Natural orifice transluminal endoscopic surgery (NOTES) has begun to be developed and is being used in clinical practice [2].
Trans-umbilical laparoscopic-endoscopic single port surgery (TU-LESS) perfectly interprets the persistent pursuit of cosmetic results in minimally invasive surgery. Single-port laparoscopic techniques were initially utilized in gastrointestinal and urological surgery, and have been slow to develop due to their relatively long learning cycle [3]. In the field of gynecology, the technique was first used for tubal sterilization. With the surgeon’s continuous surgical experience and improvement of the technique, Semm [4] in 1979 reported the first single-port laparoscopic myomectomy, pioneering the use of single-port laparoscopic techniques in the field of uterine fibroid surgery.
In recent years, TU-LESS has grown rapidly in the field of gynecologic uterine fibroid surgery. Because of the obvious limitations of the single-port laparoscopic technique, such as the “chopstick effect” and the “bucket view” [5], it is more difficult to suture the uterine muscle during the procedure. Suture methods have evolved in pursuit of better results and improved patient prognosis. From the early days of simple interrupted sutures to today’s popular baseball sutures, a variety of suture methods are available, each with their own advantages. In this article, we will review the commonly used uterine muscle sutures and ancillary techniques used in transumbilical single-port laparoscopic myomectomy.
Intraoperative bleeding is almost unavoidable during myomectomy due to the specificity of uterine tissue. Suture closure of the uterine wound is a critical step in surgery, which directly affects the surgical outcome and the patient’s prognosis [6]. In recent years, the following methods of suturing uterine wounds under TU-LESS have been utilized.
The interrupted suture technique is a commonly used in surgery and is widely used in almost all types of surgery. In the field of gynecology, interrupted sutures used in single-port laparoscopic myomectomy are used as simple interrupted suture, figure-of-eight suture or interrupted mattress suture.
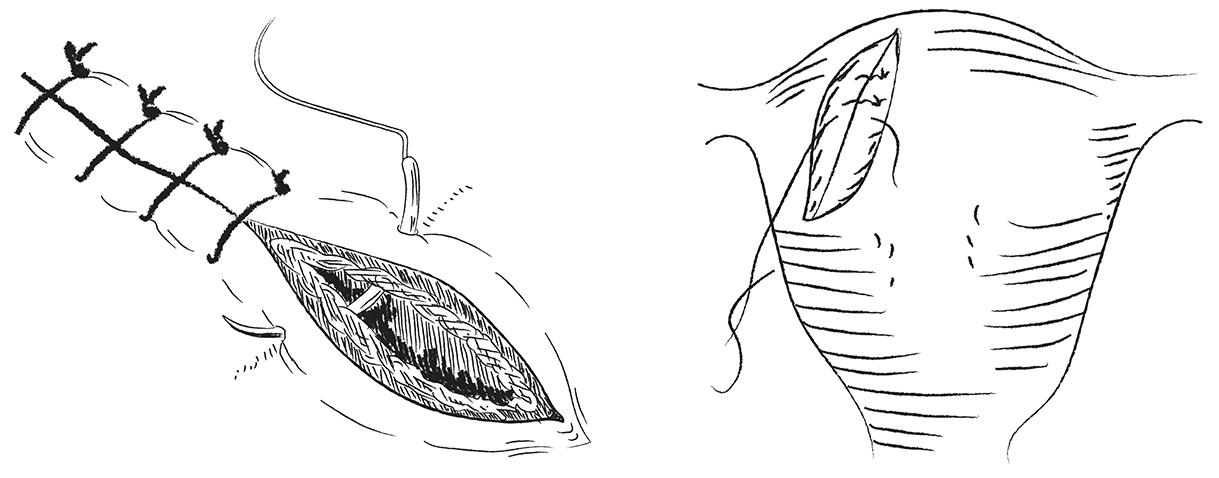
The suture method involves interrupted suturing of the muscular layer, serous layer, or all layers with absorbable sutures to close the tumor cavity and the uterine incision (Fig. 1). As the use of this method is prone to longer operating times, the appearance of dead space [7], and increased intraoperative bleeding when suturing the myometrium near the uterine vascular area, it is difficult to achieve the desired results [8]. In recent years, there have been fewer reports on the use of this suture in open myomectomy, multi-port laparoscopic myomectomy, or single-port laparoscopic myomectomy. This suture is only mentioned in the context of supplemental uterine suturing for hemostasis, and is often presented as a control group when used as the primary intraoperative suture.
 Fig. 1.
Fig. 1.Simple interrupted suture.
The authors concluded from more than 30 single-port laparoscopic myomectomies performed in the past year that when supplemental hemostasis is required, bleeding which can be stopped by simple interrupted sutures can be easily resolved by electrocoagulation devices. Occasionally, it is used in supplemental suturing of the deeper part of the tumor cavity.
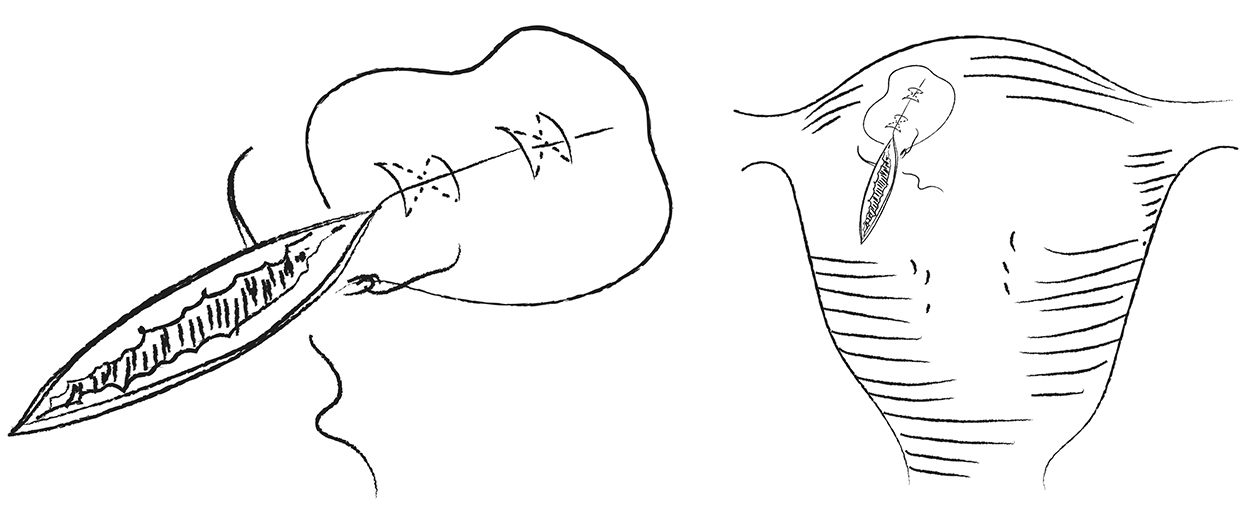
A figure-of-eight suture is used to stop bleeding. It is performed by entering the needle from the upper right corner of the incision or bleeding site and exiting the needle at the lower left corner, then entering the needle from the lower right corner and exiting the needle at the upper left corner, and finally tightening the suture and completing the knot (Fig. 2). The hemostasis principle of this suture is to promote the closure of the blood sinus at the bleeding site by applying pressure [9].
 Fig. 2.
Fig. 2.Figure-of-eight suture.
Although the figure-of-eight suture has good hemostasis, it is relatively difficult to operate under single-port laparoscopy due to the need for frequent pulling, reversing, looping, and tying of knots during the operation. When using a figure-of-eight suture under single-port laparoscopy, the operator needs to wind the thread 2–3 turns (preferably 3) to tighten the knot to ensure that there is enough tension on the knot to keep it from unraveling due to the lack of an assistant. This knotting and winding operation is relatively difficult and time-consuming in single-port laparoscopy, and is not recommended for beginners. It can be used at the discretion of those who are skilled in single-port laparoscopic operation.
The authors have used this suture in supplemental hemostasis during single-port laparoscopic myomectomies in the last two years and concluded that when supplemental hemostasis is required secondary to the hemostasis of the electrocoagulation device being poor, supplemental figure-of-eight sutures followed by localized precision electrocoagulation can achieve satisfactory hemostasis.
Interrupted mattress sutures are used for uterine fibroid surgery, both being interrupted horizontal mattress or interrupted vertical mattress sutures. Both can effectively close the tumor cavity and provide effective compression of the uterine incision to stop bleeding.
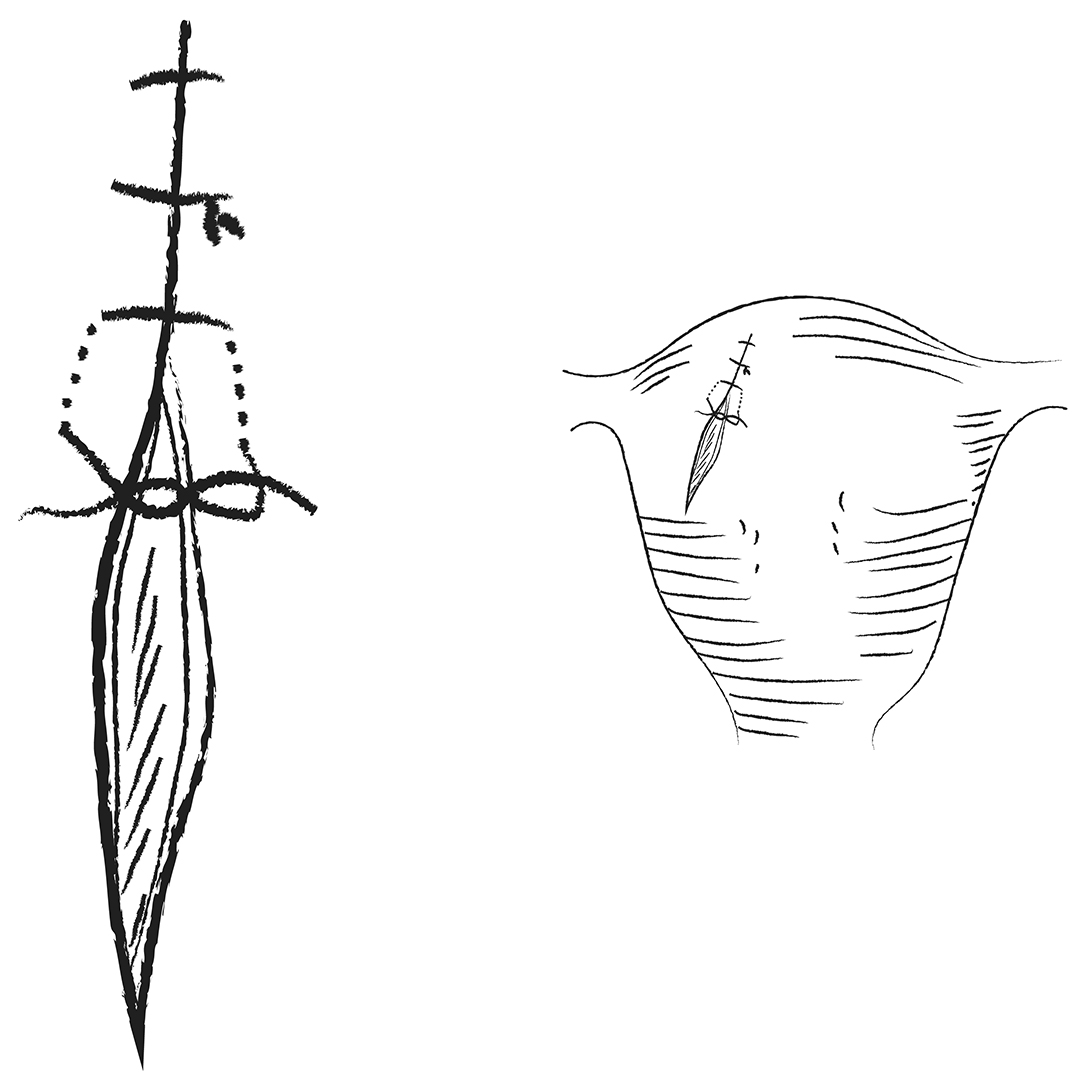
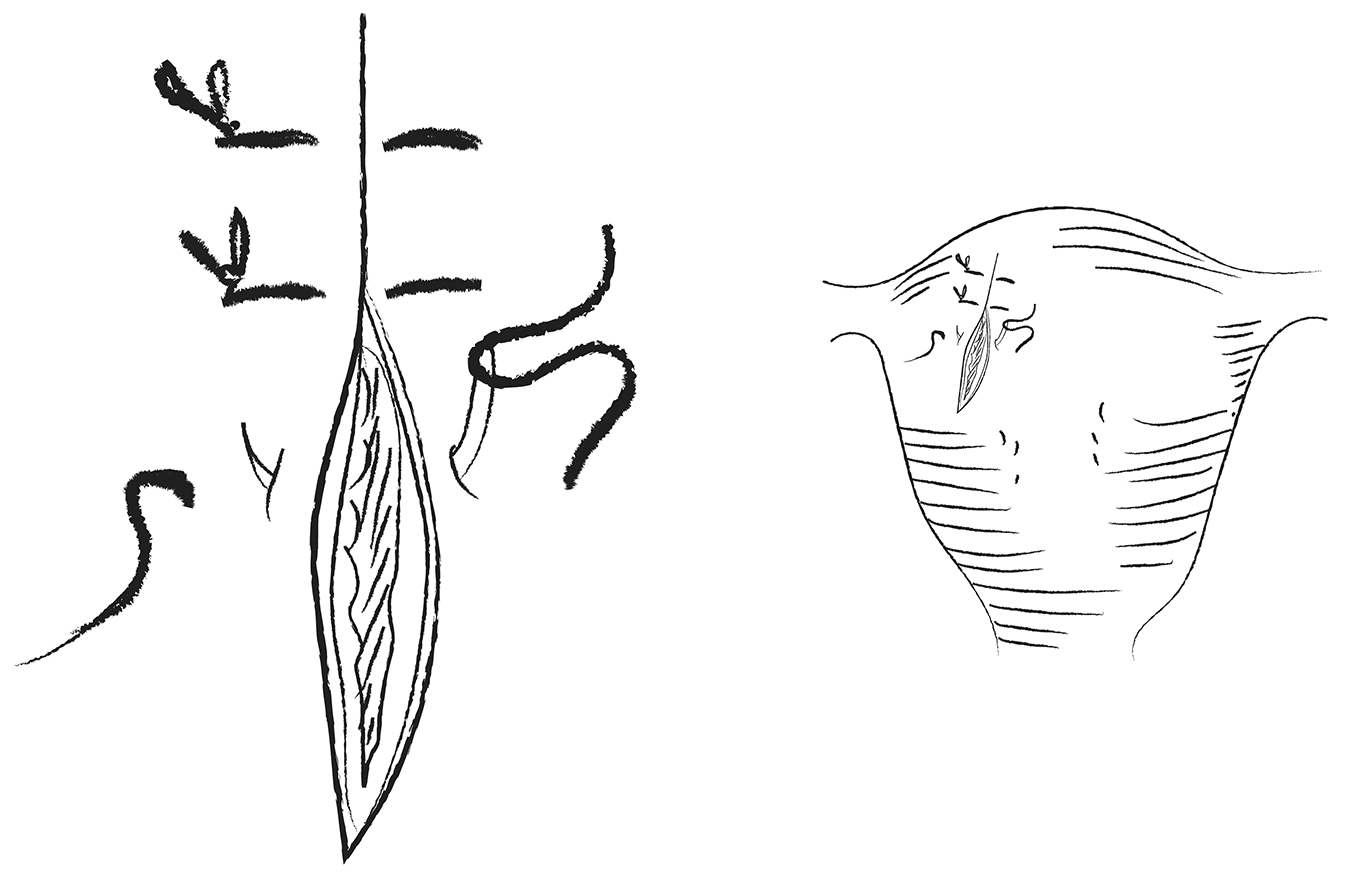
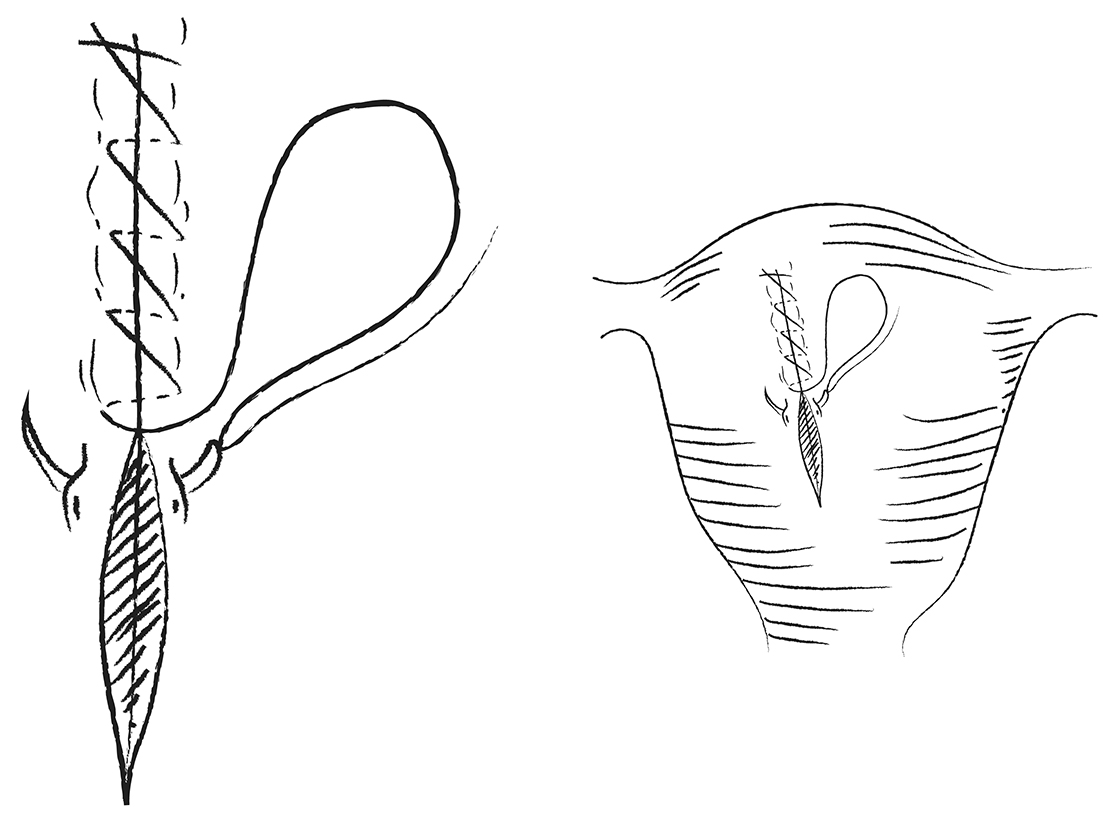
Interrupted horizontal mattress sutures are used for uterine fibroid surgery with an interrupted horizontal mattress inversion suture (Halsted suture). This suture method requires that the needle be inserted at a distance of about 0.5 to 1.0 cm from the incision, the needle is discharged at a distance of 0.5 to 1.0 cm from the entry point on the ipsilateral side, and then the needle is inserted at a distance of about 0.5 to 1.0 cm from the incision on the contralateral side, so that the line connecting this entry point with the exit point on the opposite side is perpendicular to the incision. The needle is discharged at a distance of 0.5 to 1.0 cm from the entry point on the same side, so that the line connecting this exit point and the entry point on the opposite side is perpendicular to the incision and the line connecting this entry point with the exit point on the same side is parallel with the incision edge (Fig. 3). The interrupted vertical mattress suture is performed by inserting the needle at a distance of about 0.5 to 1.0 cm from the incision, passing it out at a symmetrical point on the opposite side of the incision at a distance of about 0.5 to 1.0 cm from the incisional edge, then inserting the needle at a distance of about 0.1 to 0.2 cm from the incisional edge on that side, and then exiting the needle at a distance of about 0.1 to 0.2 cm from the incisional edge on the opposite side, and then tying a knot to close the cavity of the tumor (Fig. 4).
 Fig. 3.
Fig. 3.Interrupted horizontal mattress suture.
 Fig. 4.
Fig. 4.Interrupted vertical mattress suture.
This suture plays an effective role of compression hemostasis, and at the same time can align the uterine incision, so that the uterine wound appearance is flatter and smoother, while reducing the occurrence of postoperative pelvic tissue adhesions. Compared with a simple interrupted suture, this suture has more advantages in terms of hemostasis and operative time, and reduces surgical trauma [10]. Based on the field of single-port laparoscopic surgery, some studies have analyzed the efficacy of a baseball suture and interrupted mattress sutures in single-port laparoscopic uterine fibroid debulking surgery, and concluded that the use of this method in single-port laparoscopic surgery is difficult to perform [11, 12].
The authors have used this suture in single-port laparoscopic myomectomies in the last 2 years, but the frequency of its use has gradually decreased. We concluded that interrupted mattress sutures have similar hemostasis to the figure-of-eight suture and provide better alignment of the uterine muscle, but are more difficult to perform under a single port than using a figure-of-eight suture.
Continuous sutures are widely used in gynecologic surgery, demonstrating a clear superiority in operative time over various interrupted sutures. In recent years, simple continuous sutures and baseball sutures have been commonly used in the field of single-port laparoscopic uterine fibroid surgery.
This suture is a more traditional suture in the development of uterine fibroid surgery, and its operation is as follows: start from the tip of the incision edge with absorbable thread, from deep to shallow, successive suture layer by layer, and finally embedded suture in the serous layer of the uterus (Fig. 5). In the field of single-port laparoscopic surgery, Koo et al. [13] concluded that this suture method has advantages in terms of total operative time, intraoperative bleeding, postoperative drainage, and average hospitalization stay. In recent years, the emergence of barbed sutures has led to a resurgence in the use of this simple continuous suture. Zhang et al. [14] concluded that continuous suturing with barbed sutures has certain advantages in reducing intraoperative bleeding, shortening operative time, and reducing operation difficulty. The hemostasis and the difficulty of the operation were no less than that of the baseball suture when using barbed suture.
 Fig. 5.
Fig. 5.Simple continuous suture.
This suture has been our primary method of suturing uterine muscle in recent years. The advent of the barbed suture further reduces the difficulty of using this method and while improving its hematostatic effect.
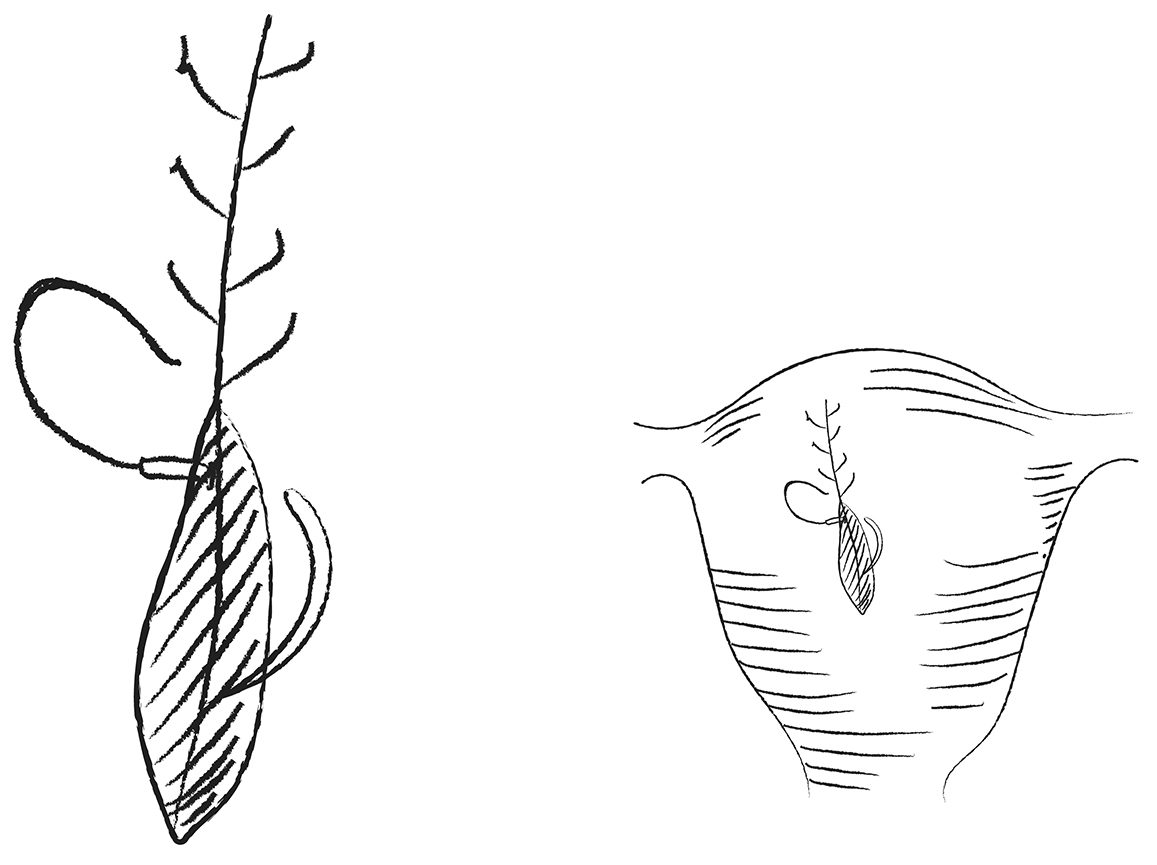
In recent years, the baseball suture is a commonly used method in uterine fibroid wound closure, both in the open and laparoscopic approach. Baseball sutures are used to close fibroid wounds with tighter incisional junctions for better hemostatic effect [15]. The baseball suture is performed as follows: on one side of the incision, the needle is inserted from the bottom of the tumor cavity from the inside, and exited from the serous layer of the uterus on the same side at a distance of about 1.0–1.5 cm from the incision. Then the needle is inserted from the bottom of the contralateral side of the tumor cavity, and exited from the serous layer of the uterus on that side at a distance of about 1.0–1.5 cm from the incision. The distance between the needles is kept at 1.0–1.5 cm for consecutive suturing (Fig. 6).
 Fig. 6.
Fig. 6.Baseball suture.
The use of the baseball suture in single-port laparoscopic uterine fibroid surgery has certain advantages in terms of surgical time and hemostasis when compared with the use of other sutures. Xie et al. [12] applied the baseball suture method to single-port laparoscopic and multi-port laparoscopic myomectomy and found that the use of the baseball suture method was satisfactory in terms of operative time, intraoperative bleeding, and postoperative drainage. Fernandes et al. [16] concluded that the inside-out needle travel characteristic of the baseball suture method makes the pressure toward the direction of the uterine smooth muscle after pulling the suture tight, when a barbed suture is used, it is more capable of forming a uniform and strong hemostatic force, reducing the probability of blood seepage from the eye of the needle. It has a shorter operative time and decreases the likelihood of the occurrence of myometrial tearing.
We have used this suture more commonly in single-port laparoscopic myomectomies and have concluded that although this method is slightly more difficult to use than the simple continuous suture, when the uterine trauma is large and bleeding is high, the use of this method for uterine muscle closure can obtain better hemostasis while reducing the need for supplemental hemostatic procedures.
With the gradual expansion of the indications for single-port laparoscopic myomectomy, the limitations on the location, number, and size of fibroids have been gradually liberalized, with ensuing problems increasing [17]. Increased intraoperative bleeding adds to the difficulty of the surgery, and visual field exposure is affected, especially for fibroids in the posterior wall of the uterus. The suture is prone to loosening, which further increases intraoperative bleeding, affects surgical results, and increases the incidence of postoperative complications [18]. In order to minimize intraoperative bleeding and reduce the difficulty of suturing, the choice of suture is important under the premise of having a good suturing technique and method. Currently, the main sutures used in multi-port laparoscopic or single-port laparoscopic myomectomy are ordinary absorbable sutures and barbed sutures.
Suturing of the tumor cavity in uterine fibroid surgery is often performed with ordinary (barbless) absorbable sutures, and a large number of reports have concluded that it is feasible to perform tumor cavity suturing with ordinary absorbable sutures [19]. Tight suturing of the fibroid tumor cavity is required. Because of the smooth surface texture of ordinary absorbable sutures and the high tension of the incision in the tumor cavity, it is easy to loosen the previous suture without the aid of an assistant to pull it during suturing. In continuous suturing, to achieve a tight suture effect, it is necessary for the assistant to pull repeatedly and work closely with the primary surgeon. This leads to longer operative time, a certain error rate, increased intraoperative bleeding, and multiple cuts to the tissue increase the probability of intraoperative bleeding at the eye of the needle [20]. Further difficulties during single-port laparoscopic surgery may mandate a switch to multi-port laparoscopic surgery to complete the procedure.
The barbed suture has a precise and rational design, with tiny barbs distributed on its surface, which are closely and evenly arranged to form a “serrated” structure. This special design ensures a tight alignment of the incision even when the suture is not pulled by an assistant and is not tied with a knot during surgery. Greenberg and Einarsson [21] first used barbed sutures in gynecologic surgery. Aoki et al. [22] concluded that the use of barbed sutures for tumor cavity closure reduces surgical time by 25% and reduces the burden on the surgeon relative to closure with ordinary absorbable sutures. Angioli et al. [23] concluded that the use of barbed sutures for closure significantly reduced intraoperative bleeding. Lee et al. [24] used barbed wire to suture uterine fibroid wounds under single-port and multi-port laparoscopy, and concluded that the use of barbed wire for tumor closure under single-port laparoscopy is safe, effective, and feasible, with obvious advantages in reducing intraoperative bleeding and shortening the operative time. This reduces the energetic damage to the uterine tissues and the adjacent tissues or organs caused by the use of bipolar coagulation for hemostasis. A certain level of confidence in the surgeon’s ability to learn single-port laparoscopic suturing procedures has been enhanced and the learning curve has been shortened.
Because of the operational limitations of single-port laparoscopic surgery, the selection of the appropriate suture method as well as the choice of suture plays an important role. As far as interrupted suture is concerned, it is now rarely used as a main suturing method because of the difficulty of operating under single-port laparoscopy. Occasionally, it is used for supplemental hemostasis in the deeper part of the tumor cavity. Continuous suture is often used as the primary suture for uterine fibroid wounds, as it has advantages over interrupted suture in terms of operative difficulty, operative time, and hemostasis. Compared with simple continuous suture, the baseball suture is more advantageous in reducing intraoperative bleeding and improving the patient outcomes. The use of barbed suture in gynecological surgery allows the incision to be tightly aligned and hemostatic without the need to pull the thread. The use of barbed sutures for uterine fibroid wound closure reduces the requirement for the operator’s suturing technique, which in turn shortens the operative time and reduces the incidence of intraoperative and postoperative bleeding. We have concluded that it is beneficial to use barbed suture for continuous suture or baseball suture when performing the operation under single-port laparoscopy. When operating, it is necessary to pay attention to the tightening of the thread knot, and when unassisted tightening of the thread is operated by a single person under single-port laparoscopy, the manipulation of the left hand of the operator is more difficult.
Due to the specificity of the uterine tissue, the suturing of uterine wounds is extremely demanding. The lack of assisting surgeon in single-port laparoscopic surgery makes it difficult to provide effective fixation of the tissue during suturing, and this aspect has become a technical difficulty in single-port laparoscopic surgery. A variety of ancillary techniques have been explored and the following is a list of several ancillary suturing techniques that have been suggested.
The post needle hook assisted approach to single-port laparoscopic surgery appeared first in pediatric surgery [25]. In the field of single-port laparoscopic gynecologic surgery, the small operating space and the difficulty of the procedure are the problems that must be faced in order to learn the technique. The needle hook assisted method used in single-port laparoscopic surgery is like “invisible hands”, so that the technical difficulty of single-port laparoscopic surgery is greatly reduced [26].
The needle hook assisted method is used in single-hole laparoscopic uterine fibroid surgery. The main method of operation is in the middle of the anterior axillary line and the midclavicular line. From the upper edge of the pubic symphysis at the level of about 5 cm, using a straight needle with a line, a puncture is made into the abdominal cavity, that allows the straight needles on both sides of to be curved into a V-shaped or U-shaped fishhook shape. Hooking, fixing, and pulling the fibroid or the myometrium surrounding the fibroid to expose the gap between the tumor and the surrounding myometrium aids in fibroid removal. Subsequent immobilization and lifting of the fibroid or traumatized myometrium by means of a needle hook can assist in bagging and removing the fibroid, as well as assisting in the suturing of the uterine surface. At the end of the procedure, the needle hook can be removed through the umbilical incision, reducing damage to the skin and achieving a scarless result.
One study has opted for needle hook versus non-needle hook approach to perform transumbilical single port laparoscopic myomectomy [27]. The results demonstrated that the needle hook method plays a good role in lifting and fixation assistance in the exposure of the operative field, intraoperative bagging and removal of the fibroid, along with suturing of the uterine wound. However, excessive pulling may cause local tissue damage and increase the chance of further bleeding. There are few reports on the efficacy of this method for single-port laparoscopic myomectomy, and its safety and efficacy need to be further explored.
The suspended line method, originally derived from studies of gasless laparoscopic surgery [28], is now more common in single-port ovarian cyst surgery. This method can effectively fix the organs and expose the lesion, thus further solving the problems of difficult operation and long operative time during the application of single-port laparoscopic surgery.
When the suspended line method is used in single-port laparoscopic myomectomy, its operation method is as follows. After the fibroid is removed during the operation, in the left or right lower abdomen corresponding to the starting location of the fibroid, the pelvis is punctured with an ordinary suture under the direct vision of the single-port laparoscopic lens, and the appropriate length of suture is determined. The vascular forceps fix the part of suture left at the outer end of the body, and the abdominal cavity with the needle side suture is sutured with a continuous suture to close the defect. The length of the suture at the outer end of the body is adjusted in order to maintain tension, maintain the lifting and fixing effect, and facilitate the intra-abdominal tissue suture. After the suture is completed, the knot is made by using the feeding method to tighten the two ends of the suture at the same time.
Some scientific studies have examined the use of this method in single-port laparoscopic ovarian cyst surgery [29] and tubal sterilization [30]. The authors concluded that in single-port laparoscopic myomectomy, the suspended line method can be used to select the position of the needle from the abdominal wall according to the needs of the intraoperative situation. By adjusting the length and tightness of the suture line left outside of the body, the position of the uterus in the pelvic cavity is suspended or fixed, so as to make the surface of the fibroid removal clearly exposed. This assists the operator in closing the uterine wound under single-port laparoscopy. In the population of patients with fibroids without a history of sexual activity that prohibits the placement of a uterus lifting cup, the use of the suspended line method solves the problem of uterine immobilization in the absence of a uterus lifting cup. Knotting is difficult in single-port laparoscopy and is simplified and made easier by the combined external and internal knotting of the suspended line method. The use of this method for single-port laparoscopic ovarian cyst debulking has been reported, but the efficacy analysis for single-port laparoscopic myomectomy has been reported in few cases, and there is value in further research on its safety and efficacy.
In single-port laparoscopic surgery, the laparoscopic lens and various surgical instruments enter the abdominal cavity through a single incision in the umbilicus. This may cause mutual interference between instruments, inability to form an operating triangle, and potentially reduces the surgical safety [31]. In addition, single-port laparoscopic surgery is mainly operated by a single person without the help of an assistant, which tends to affect the exposure of the scope of the surgical field of view, which in turn leads to an increase in the difficulty of the operation and an increase in the failure rate of the operation [32].
Numerous studies have shown that it is feasible to use single-port laparoscopic surgery for myomectomy [24, 33]. However, compared with the multi-port laparoscopic approach, single-port surgery still has some operational limitations due to the “bucket view” and “chopstick effect” created by the single-port surgical approach [34]. Reducing interference between instruments or lenses and minimizing the effects of the chopstick effect is a key factor in the success of single-port laparoscopic suturing. In single-port laparoscopic myomectomy, knot-free barbed sutures are used, and the assistant lifts the uterus to manipulate the direction of the uterus to allow suturing. The use of one hand for suturing and thread pulling reduces the number of instruments entering the operative field, thus freeing up more operating space, and effectively reducing the impact of the “chopstick effect” and facilitates the closure of the fibroid wound.
The single-port laparoscopic technique is more demanding for beginners. The modified operation is mostly used in the stage of beginner’s single-port laparoscopic surgery as well as supplementary operations when the progress of the operation is difficult. Based on the transumbilical single-port laparoscopic surgery, a 0.5-cm operation hole is added in the left or lower abdomen, allowing the difficulty of the operation to be reduced. Myomectomy mostly requires the placement of drainage tubes, and this operation hole can be used as the passage site of drainage tubes, avoiding the risks of infection and umbilical hernia (especially for obese patients) associated with placing drainage tubes at the umbilical orifice [35].
Kang et al. [36] studied the long-term efficacy of transumbilical single-port laparoscopic myomectomy and concluded that modified transumbilical single-port laparoscopic myomectomy has no limitation on the number and size of fibroids, which allows the indications for the operation to be expanded. If difficulties are encountered during single-port surgery and the operation is difficult to be performed, the modified operation can be chosen. The position of the additional operative hole is not set, and can be chosen according to the intraoperative situation and the aesthetics of the abdominal wall. Choi et al. [37] concluded that the modified transumbilical single-port laparoscopic myomectomy is advantageous in terms of operative time, intraoperative and postoperative bleeding, and reduces the difficulty of myoma debulking as well as suturing of the wound compared to multi-port laparoscopic surgery. By analyzing the efficacy of single-port, double-port, and triple-port laparoscopic myomectomy, Kim et al. [38] concluded that the double-port modified operation is more advantageous than the single-port operation in terms of reducing the operative time, decreasing the difficulty of the operation, and shortening the learning time as compared to the triple-port operation.
The gradual maturation of single-port laparoscopic surgery is an inevitable trend in the development of minimally invasive surgery. Single-port laparoscopic surgery has obvious minimally invasive advantages, but the chopstick effect produced by single-port laparoscopic surgery greatly increases the difficulty of the procedure. Safe, effective, rapid and aesthetic suturing of the lesion in single-port laparoscopic myomectomy is a difficult point to focus on in this procedure. There is a lack of data related to the hemostasis of different sutures on uterine muscle in single-port laparoscopic myomectomy.
As far as suturing is concerned, the use of interrupted sutures for uterine trauma has been significantly less recommended than continuous sutures. Clinical studies have shown that the use of barbed suture for baseball suture or simple continuous suture is recommended, which is more advantageous than other suture methods in terms of reducing intraoperative and postoperative hemorrhage, shortening operative time, decreasing the probability of additional suture for bleeding from the eye of the needle, and decreasing the patient’s tissue damage. Interrupted sutures may be used when supplemental local sutures are used to stop bleeding (Table 1). In order to reduce the difficulty of suturing in single-port laparoscopic myomectomy, studies have introduced a variety of ancillary suturing techniques, such as needle-hook-assisted method, suspended line method, one-handed operation method, and the modified operative method. Needle-hook-assisted and suspended line methods have been proven to be effective in their respective areas of expertise, and have been used in single-port laparoscopic myomectomy, but their safety and efficacy need to be further explored and studied. The one-handed operation method can free up more operating space and reduce the influence of the “chopstick effect”, but it requires the operator to have a certain degree of basic experience with single-port surgery. The modified operative method has obvious advantages in reducing the operative time, lowering the difficulty of the operation, and shortening the learning time, but it is slightly insufficient in the concept of being minimally invasive (Table 2). At this stage, the methods and techniques for suturing the surgical wounds of uterine fibroids under single-port laparoscopy are still in the exploratory stage. It is worthwhile to consider whether there are more minimally invasive, safe and feasible ancillary techniques to reduce the difficulty of single-port laparoscopic uterine fibroid wound closure. Optimization of surgical instruments to improve the efficiency of single-port laparoscopic suturing while further improving surgical skills is also a research direction in this field. Whether there are more appropriate suture methods, more intelligent instrumentation and equipment, and more efficient and minimally invasive ancillary suture techniques under single-port laparoscopic operation are worthy of further exploration and research.
| Advantages | Limitation | Application | ||
| Interrupted suture | Simple interrupted suture | Relatively easy to operate | Poor hemostasis effect | Used when supplementing local hemostasis |
| Figure-of-eight suture | Good hemostasis effect | Somewhat difficult to operate | ||
| Interrupted mattress suture | Good hemostasis effect and better closure of uterine incision | Difficult to operate | ||
| Continuous suture | Simple continuous suture | Relatively easy to perform, with no significant difference in hemostasis effect from baseball sutures when using barbed sutures | For ideal hemostasis effect, rely on barbed sutures | Primary suture method when suturing uterine fibroid wounds |
| Baseball suture | Good hemostasis, more effective when using barbed sutures | Increased number of intraoperative needle adjustments, slightly more difficult to operate than simple continuous suturing |
| Advantages | Limitation | Aesthetics | |
| Needle hook assisted method | Effective lifting and immobilization of the uterine wound to facilitate suturing | If there is excessive stretching, there is a possibility of local bleeding, increasing the chance of additional sutures to stop bleeding | No operation holes other than the umbilical hole, interpreting the concept of minimally invasive surgery |
| Suspended line method | |||
| One-handed operation method | Reducing the impact of the “chopstick effect” | Requires the operator to have some basic experience in single-port laparoscopic surgery | |
| The modified operative method | Reduces the “chopstick effect” and prevents adverse reactions caused by placing the drain in the umbilicus | Additional operating holes, slightly inadequate at the minimally invasive level | |
YW, MM and JC—designed the research study. YW, YC, BX, WS and TX—wrote and revised manuscripts, proposed methodology and conceptualization. YW, HZ, WW, BT and YD—conducted the selection of relevant studies. YW, JC and HZ—drafted the paper. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This work was supported by grants from Top Talent of Changzhou “The 14th Five-Year Plan” High-Level Health Talents Training Project (2022CZBJ074), the maternal and child health key talent project of Jiangsu Province (RC202101), the maternal and child health research project of Jiangsu Province (F202138), the Scientific Research Support Program for Postdoctoral of Jiangsu Province (2019K064), and the Scientific Research Support Program for “333 Project” of Jiangsu Province (BRA2019161).
The authors declare no conflict of interest. Jiming Chen is serving as one of the Guest editors of this journal. We declare that Jiming Chen had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Michael H. Dahan.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.