

1 Department of Pediatrics, Key Laboratory of Birth Defects and Related Diseases of Women and Children of the Ministry of Education, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Key Laboratory of Obstetrics & Gynecologic and Pediatric Diseases and Birth Defects of the Ministry of Education, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
Abstract
Background: The correlation among Glucokinase (GCK) rs1799884 polymorphism and the risk of gestational diabetes mellitus (GDM) remains controversial, as previous studies have reported inconsistent findings. The potential relationship among the GCK rs1799884 polymorphism and GDM risk was examined by a meta-analysis. Methods: In order to find relevant studies for our investigation, we performed an extensive search across multiple databases, such as Ovid, PubMed, China National Knowledge Infrastructure, and Web of Science. Afterward, the link among the GDM risk and GCK rs1799884 polymorphism was evaluated by employing either random-effects models or fixed-effects to compute 95% confidence intervals (CIs) and pooled odds ratios (ORs). Results: This meta-analysis comprised a total of 11 studies. The findings revealed that the GCK rs1799884 polymorphism was linked to a decreased risk of GDM across all examined models. The pooled analysis demonstrated a substantial link, with the corresponding 95% CIs and the following ORs: Allele contrast: 0.80 (0.73–0.88), recessive model 0.81 (0.76–0.88), homozygote 0.60, (0.49–0.73), heterozygote 0.84, (0.78–0.91), dominant model 0.59, (0.48–0.72). Conclusions: The GCK rs1799884 variant, according to the current meta-analysis, may act as a genetic biomarker of GDM. The investigation was registered on PROSPERO (https://www.crd.york.ac.uk/prospero/) under registration number CRD42023492185.
Keywords
- gestational diabetes mellitus
- GCK
- polymorphisms
- meta-analysis
Gestational diabetes mellitus (GDM) is characterised by hyperglycemia and glucose intolerance during pregnancy [1]. It is projected that about 14% of pregnant women worldwide are glucose intolerant [2]. GDM is associated with adverse pregnancy outcomes and foetal chronic metabolic diseases. The mechanism as well as the aetiology of GDM is yet to be fully known. Nevertheless, published evidences suggests that GDM is a clinical illness caused by environmental and genetic determinants [3, 4]. For GDM, genetic susceptibility is an important risk factor [5].
Glucokinase (GCK) is a crucial enzyme in glycolysis due to its ability to
promote glucose metabolism and regulate insulin release [6]. At present, a large
number of studies have demonstrated that GCK gene mutations are associated with
abnormal glucose metabolism [7, 8, 9]. Weedon et al. [10] reported a
significant correlation between the GCK rs1799884 polymorphism and
fasting blood glucose levels in the general population. A study by Holmkvist
et al. [8] found that GCK gene
Numerous investigations conducted over the previous 20 years have assessed the possible correlation among the GCK rs1799884 polymorphism and the risk of GDM in various national races; nonetheless, the ultimate outcomes have been non-uniform and ambiguous [11, 12, 13, 14, 15]. Consequently, the correlation among the GDM risk and GCK rs1799884 mutation was examined by a meta-analysis utilising existing case-control studies.
All articles on the association between GDM risk and GCK rs1799884 polymorphism were extracted from Ovid, Pubmed, CNKI, and Web of Science using the keywords such as “GCK rs1799884”, “polymorphism” and “GDM”, and the latest search was updated on 10 December 2022. This study was previously registered with PROSPERO (CRD42023492185) and followed PRISMA guidelines (Supplementary Material).
Regardless of sample size, all studies needed to meet the following requirements to be considered: (i) to assess the association GCK rs1799884 polymorphism and the risk of GDM, (ii) for case-control research, and (iii) to have sufficient data to obtain a 95% confidence interval (95% CI) for the odds ratio (OR). Studies that fit within this scope have not been included: (i) abstracts, reviews, overviews, or editorials, (ii) studies with insufficient data.
According to the inclusion criteria mentioned above, two reviewers (Y. Hu and A. Wang) have independently extracted the information from all eligible and qualified publications. After consulting with the arbitrators, the discrepancies were resolved (K. Yi).
The next available information was captured from all eligible publications: first author’s last name, date of publication, participants’ country, case- and control-sample size, races, genotyping methods, and minor allele frequencies (MAF). The ethnic groupings have been categorised as Asian, Caucasian, or African.
We used the Cochran Q statistic and the I
Publishing bias was explored by visual examination of funnel diagrams using
Egger’s power-weighted regression method and Begg’s hierarchy correlation method
(p value
We used trial sequential analysis (TSA) to assess the required information size
(RIS) and the reliability of the results. The RIS was calculated based on a 5%
risk of type I error (
After conducting a meticulous literature retrieval, we eventually limited our scope to 42 publications that might merit in-depth confirmation. After further eliminating 29 articles based on their headings and abstracts, we searched the 13 articles’ full text. Finally, we went ahead and removed 1 article because it focused on a literature review [21], and another because it had nothing to do with GCK rs1799884 polymorphism [22]. A total of twelve case-control studies, derived from eleven publications, were identified for inclusion in this meta-analysis. These studies investigated the potential relationship between GDM risk and GCK rs1799884 polymorphism [11, 12, 13, 14, 15, 23, 24, 25, 26, 27, 28]. The Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guiding principle were followed in the selection of these studies [29]. The documentation searching and research selection proceedings are shown in Fig. 1.
 Fig. 1.
Fig. 1.Study selection and literature search process utilised for a meta-analysis of GDM and GCK rs1799884 genetic polymorphism. GCK, Glucokinase; GDM, gestational diabetes mellitus.
Table 1 (Ref. [11, 12, 13, 14, 15, 23, 24, 25, 26, 27, 28]) presents the unique attributes of the chosen studies. Seven studies included participants of Caucasian descent, four studies involved individuals of Asian descent, and one study encompassed people of African descent. Researches were conducted in Brazil, China, Poland, Russia, Sweden, Thailand, the UK, and the USA.
| Author | Year | Country | Ethnicity | Sample | Genotyping Methods | MAF in Controls | HWE |
| Chiu et al. [11] | 1994 | USA | African | 94/99 | PCR-SSCP | 0.19 | 0.28 |
| Zaidi et al. [23] | 1997 | UK | Caucasian | 47/92 | PCR-SSCP | 0.27 | 0.08 |
| Shaat et al. [12] | 2006 | Sweden | Caucasian | 642/1229 | Taqman | 0.15 | 0.50 |
| Freathy et al. [13] | 2010 | UK | Caucasian | 614/3811 | Illumina | 0.18 | 0.91 |
| Thailand | Asian | 384/1706 | 0.10 | 0.61 | |||
| Santos et al. [24] | 2010 | Brazil | Caucasian | 150/600 | PCR-RFLP | 0.19 | 0.11 |
| Li et al. [25] | 2011 | China | Asian | 1023/907 | Taqman | 0.21 | 0.55 |
| Han et al. [26] | 2015 | China | Asian | 948/975 | PCR-RFLP | 0.10 | 0.98 |
| Popova et al. [14] | 2017 | Russia | Caucasian | 278/179 | PCR-RFLP | 0.10 | 0.12 |
| Tarnowski et al. [27] | 2017 | Poland | Caucasian | 204/207 | Taqman | 0.11 | 0.87 |
| Popova et al. [28] | 2021 | Russia | Caucasian | 688/454 | PCR-RFLP | 0.13 | 0.14 |
| She et al. [15] | 2022 | China | Asian | 835/870 | Taqman | 0.19 | 0.24 |
Abbreviations: PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; PCR-SSCP, polymerase chain reaction–single strand conformation polymorphism; MAF, minor allele frequency; HWE, Hardy-Weinberg equilibrium.
Twelve case-control studies were included, comprising 11,129 controls and 5907 patients. The meta-analysis outcomes are displayed in Table 2. Fig. 2 shows the forest diagrams for assessing the correlation among the GDM risk and GCK rs1799884 polymorphism.
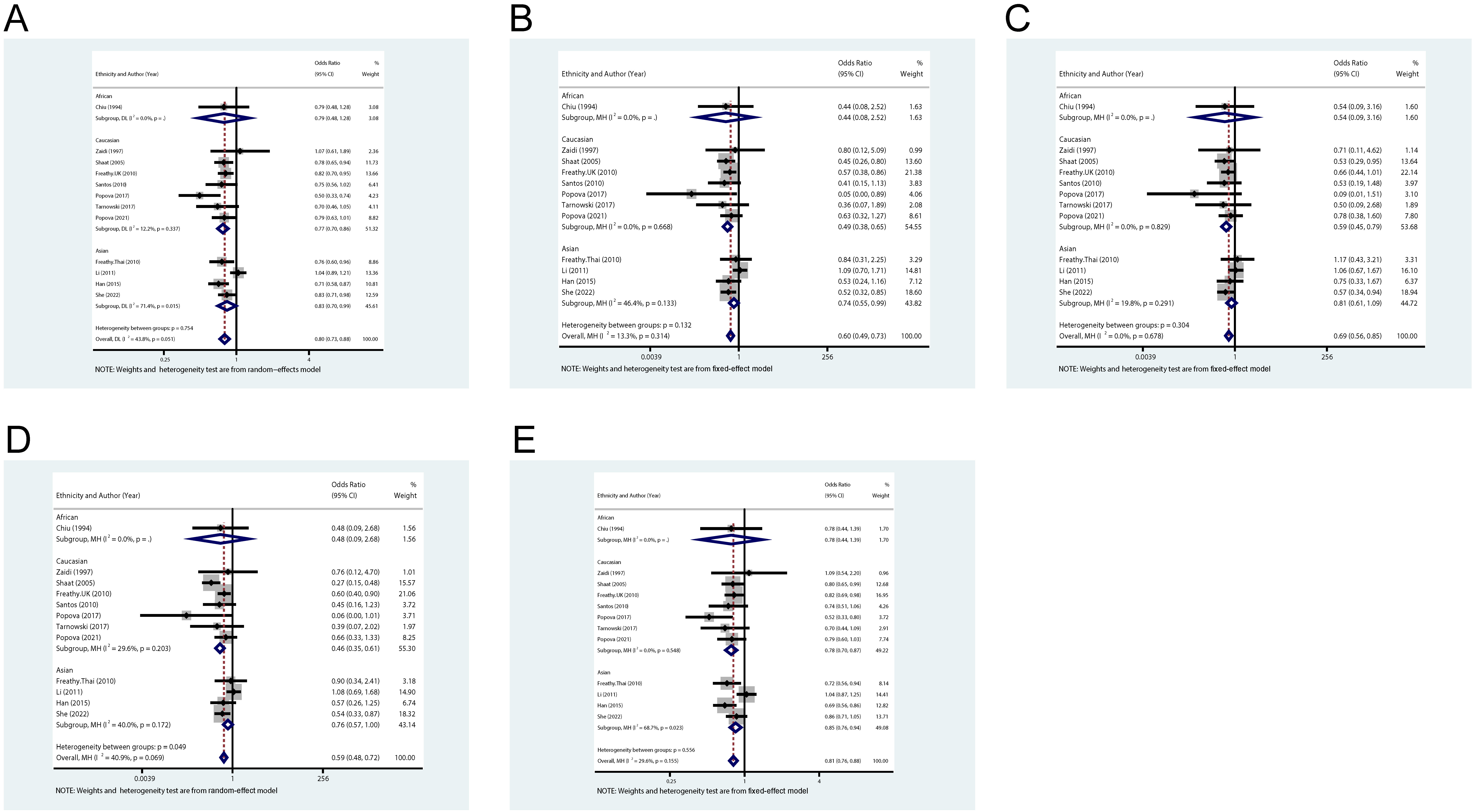 Fig. 2.
Fig. 2.GDM risk and GCK rs1799884 polymorphism forest plots of ORs with 95% CIs. (A–E) displays the allelic, homozygous, heterozygous, dominant model, and recessive models, respectively. OR, odd ratio; CI, confidence interval.
| Genetic model | Allele contrast | Homozygote | Heterozygote | Dominant Model | Recessive Model | |||||||
| Variables | Sample size | G vs. A | GG vs. AA | GA vs. AA | GG + GA vs. AA | GG vs. GA + AA | ||||||
| N |
Case/control | OR (95% CI) | p value |
OR (95% CI) | p value |
OR (95% CI) | p value |
OR (95% CI) | p value |
OR (95% CI) | p value | |
| Total | 12 | 5907/11129 | 0.80 (0.73, 0.88) | 0.051 | 0.60 (0.49, 0.73) | 0.314 | 0.69 (0.56, 0.85) | 0.678 | 0.59 (0.48, 0.72) | 0.069 | 0.81 (0.76, 0.88) | 0.155 |
| Caucasian | 7 | 2623/6572 | 0.77 (0.70, 0.86) | 0.337 | 0.49 (0.38, 0.65) | 0.668 | 0.59 (0.45, 0.79) | 0.829 | 0.46 (0.35, 0.61) | 0.203 | 0.78 (0.70, 0.87) | 0.548 |
| Asia | 4 | 3190/4458 | 0.83 (0.70, 0.99) | 0.015 | 0.74 (0.55, 0.99) | 0.321 | 0.81 (0.61, 1.09) | 0.291 | 0.76 (0.57, 1.00) | 0.172 | 0.85 (0.76, 0.94) | 0.023 |
| African | 1 | 94/99 | 0.79 (0.48, 1.28) | NA |
0.44 (0.08, 2.52) | NA |
0.54 (0.09, 3.16) | NA |
0.48 (0.09, 2.68) | NA |
0.78 (0.44, 1.39) | NA |
Overall, our analysis revealed that, in all of the models we tested, the GCK rs1799884 polymorphism was significantly associated with a reduced risk of gestational diabetes mellitus. Specifically, the homozygote model (GG vs. AA) yielded an OR of 0.60 and a 95% CI of 0.49–0.73; the allele contrast model (G vs. A) yielded an odds ratio (OR) of 0.80 and a 95% confidence interval (CI) of 0.73–0.88; the dominant model (GG + GA vs. AA) yielded an OR of 0.59 and a 95% CI of 0.48–0.72; the heterozygote model (GA vs. AA) yielded an OR of 0.84 and a 95% CI of 0.78–0.91; and the recessive model (GG vs. GA + AA) yielded an OR of 0.81 and a 95% CI of 0.76–0.88.
The evaluations of the dominant model and allele model revealed significant
heterogeneity (dominant model, p
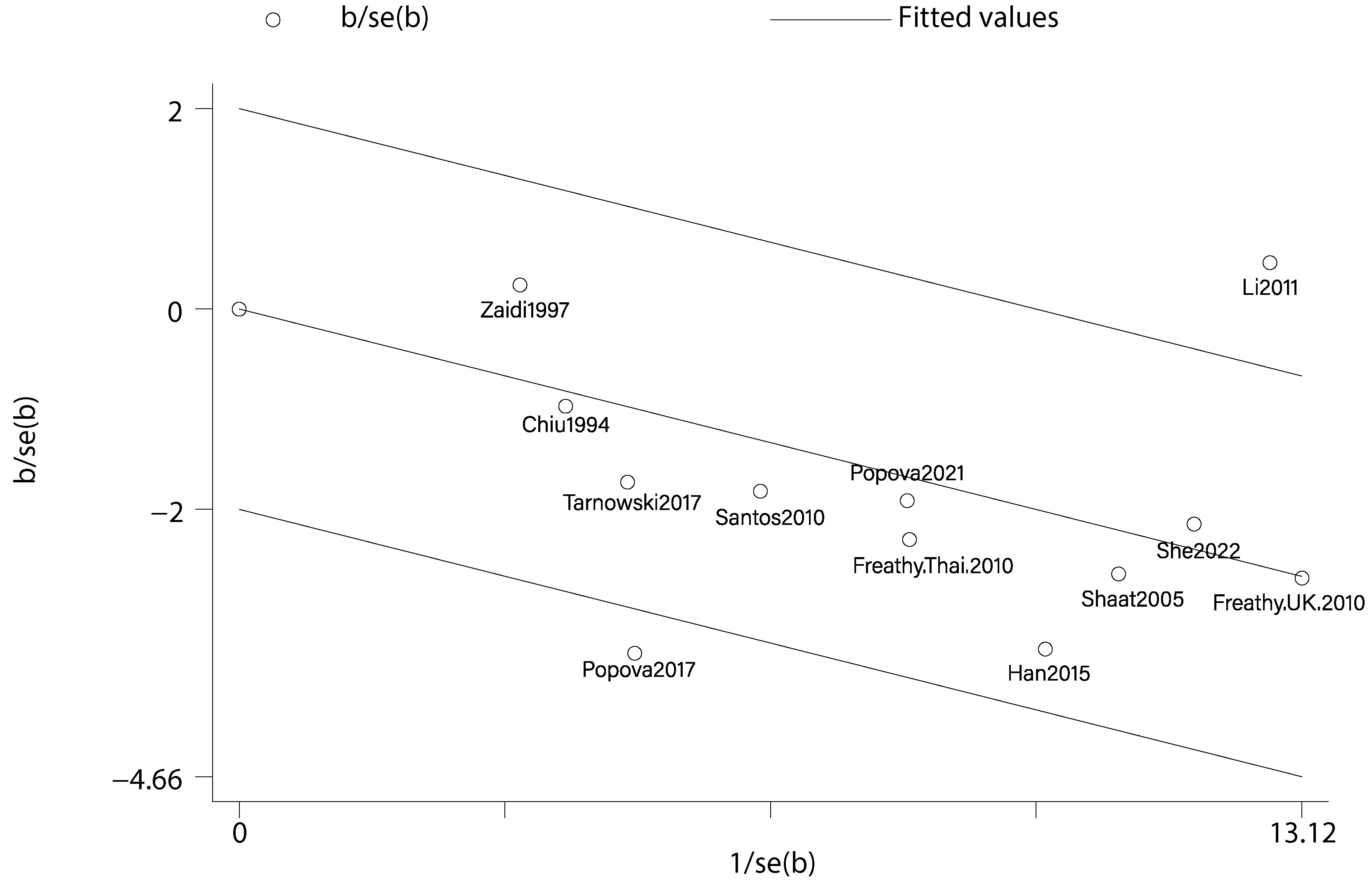 Fig. 3.
Fig. 3.Galbraith plots utilised for assessing heterogeneity concerning GCK rs1799884 polymorphism.
The outcomes are stable, as shown by the sensitivity analyses (Fig. 4) and cumulative meta-analysis (Fig. 5).
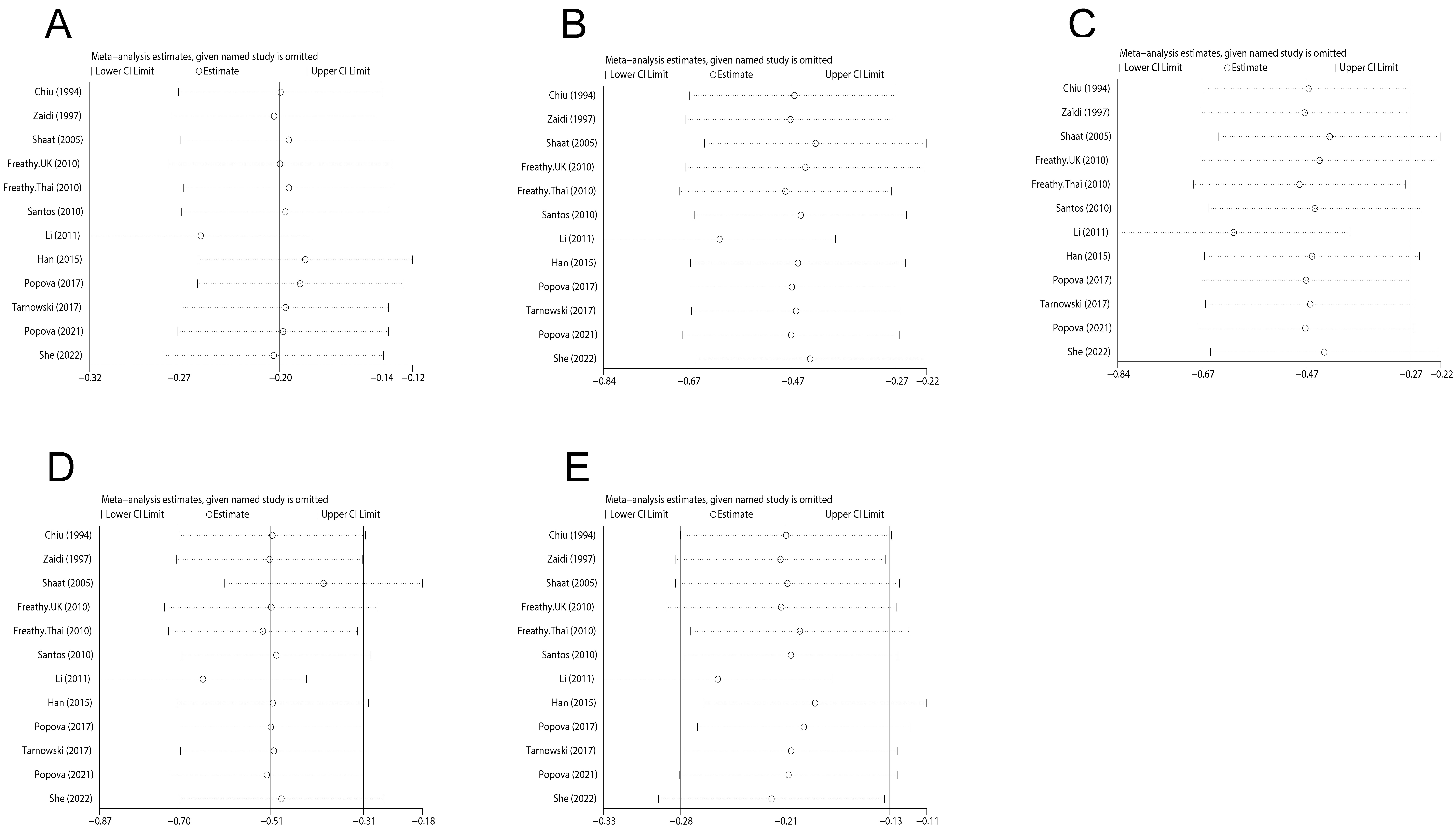 Fig. 4.
Fig. 4.Sensitivity analysis of correlation among GDM risk and GCK rs1799884 polymorphism. (A–E) displays the allelic, homozygous, heterozygous, dominant model, and recessive models, respectively.
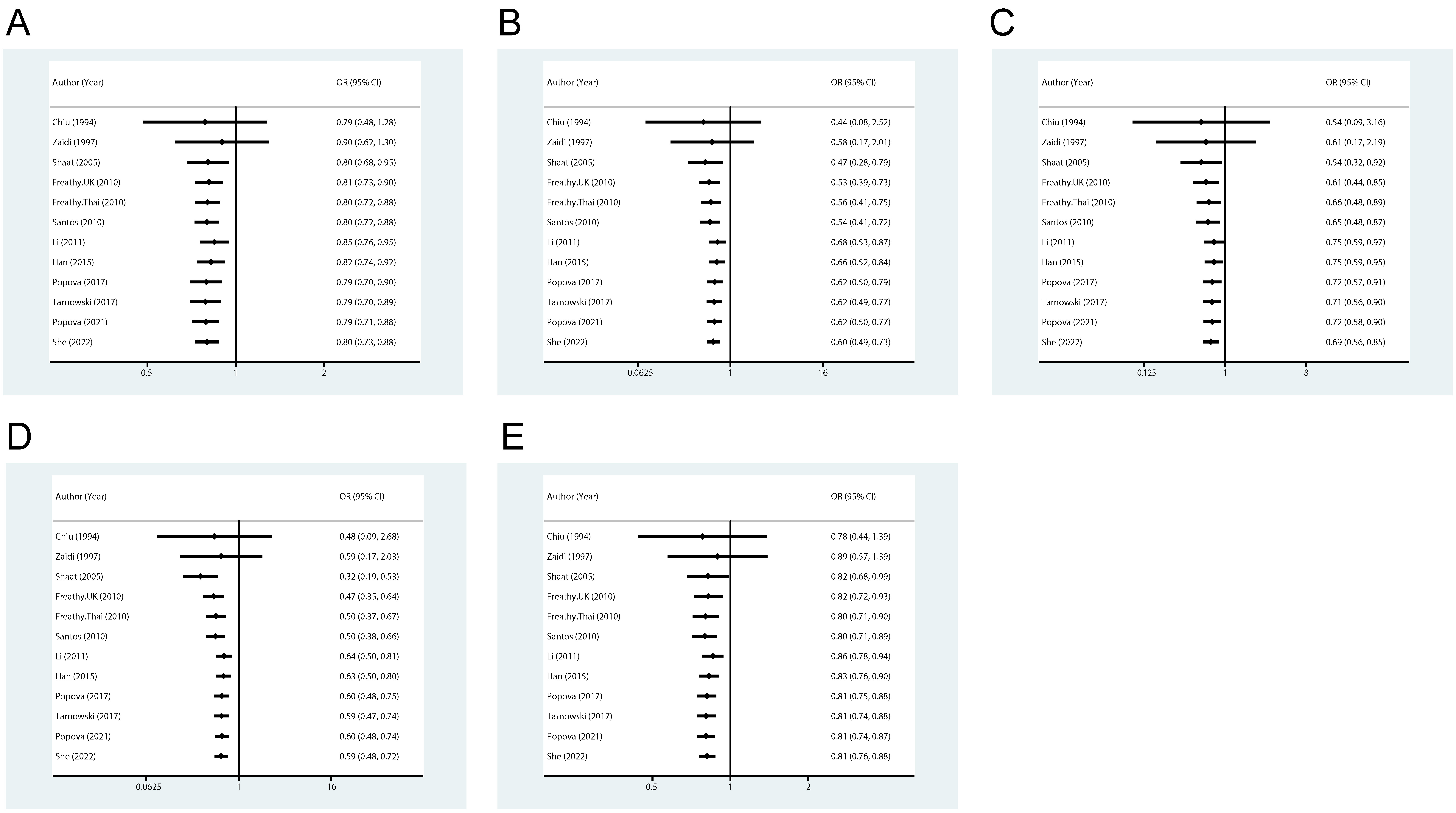 Fig. 5.
Fig. 5.Cumulative meta-analysis of correlation among GDM risk and GCK rs1799884 polymorphism. (A–E) displays the allelic, homozygous, heterozygous, dominant model, and recessive models, respectively.
Egger’s and Begg’s tests were used to determine whether publishing bias existed in the literature. No asymmetric trends was exhibited by Begg’s funnel-plot curves (Fig. 6). Besides, the statistical outcomes showed no bias in publication. Both tests yielded the following outcomes: [homozygote 0.75 and 0.47, allele contrast 0.45 and 0.20, dominant model 0.75 and 0.66, heterozygote 0.37 and 0.29, recessive model 0.37 and 0.24].
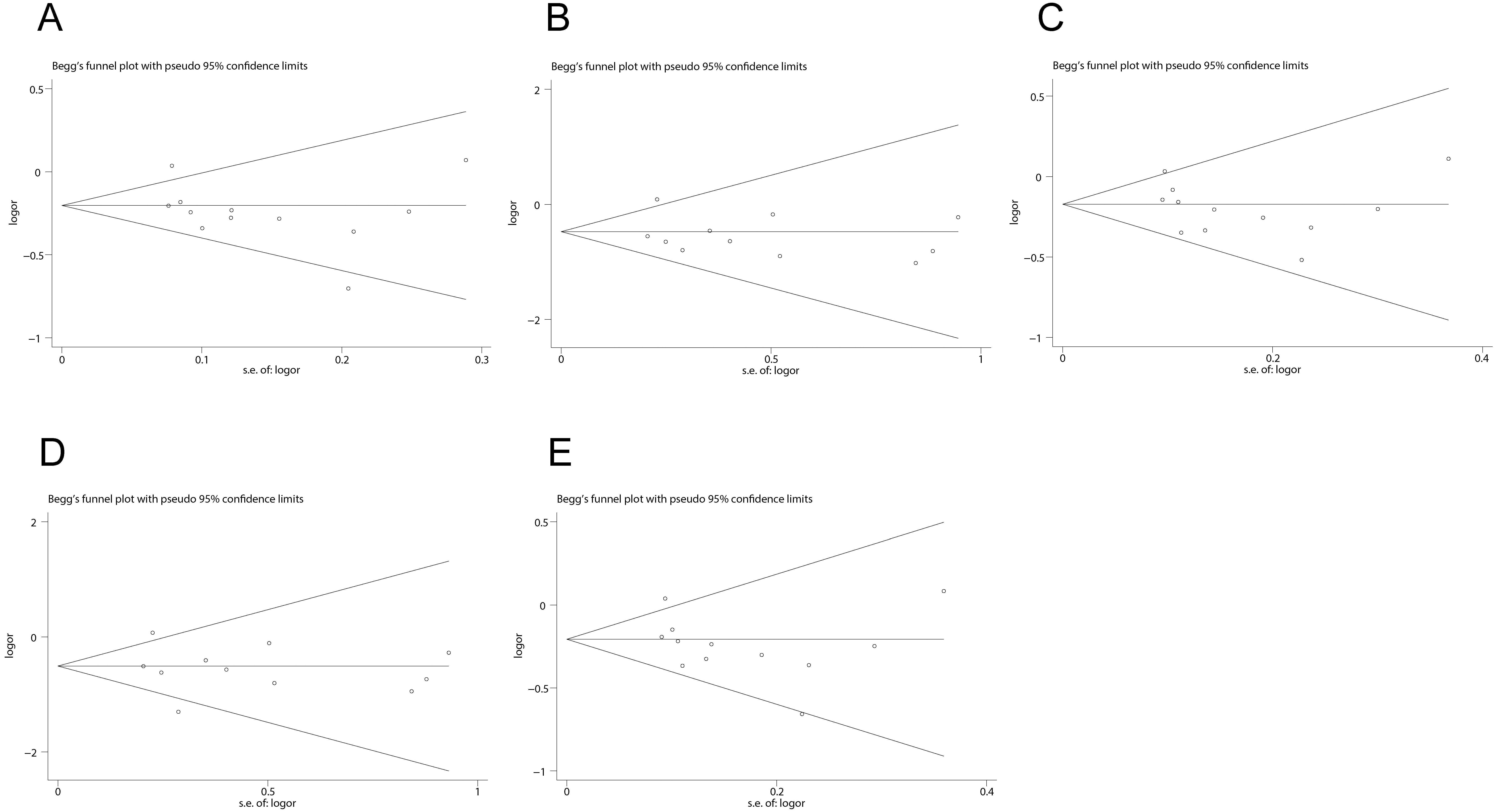 Fig. 6.
Fig. 6.Begg’s funnel plot for publication bias test. (A–E) displays the allelic, homozygous, heterozygous, dominant model, and recessive models, respectively.
TSA was employed to investigate the relationship among GCK rs1799884 and GDM risk. The outcomes revealed that while the cumulative Z value (Z-curve) did not surpass the TSA boundary value, it did cross the TSA boundary, implying that the cumulative amount of information might not have attained the RIS (Fig. 7). This suggests that the conventional meta-analysis might offer a false positive result, and it would be necessary to do additional research to verify the correlation.
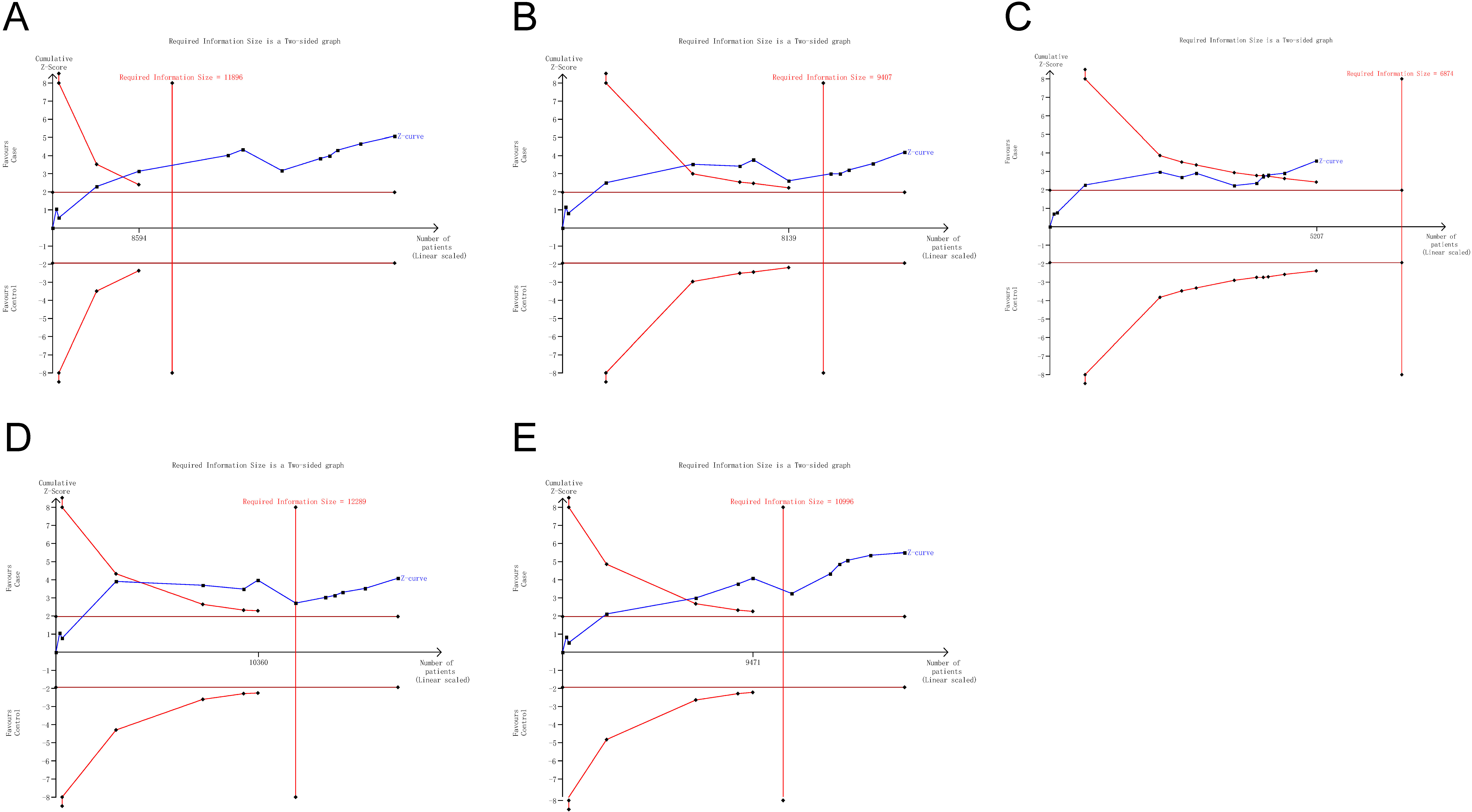 Fig. 7.
Fig. 7.Trial sequential analyses for GDM risk and GCK rs1799884 polymorphism. (A–E) exhibits the allelic, homozygous, heterozygous, dominant model, and recessive models, respectively.
Based on 12 case-controlled investigations, the meta-analysis showed that GCK rs1799884 polymorphism significantly decreased GDM incidence. When we conducted subgroup analysis on the basis of ethnicity, a significantly decreased GDM risk was found among Caucasian descent in all models. We also found a considerably lower GDM risk among Asian descent in all models except dominant model (OR, 0.76; 95% CI, 0.57–1.00).
The findings of the GCK rs1799884 polymorphism are partially consistent with the previous research. In a meta-analysis based on seven investigations, Han et al. [26] found a substantial correlation among GCK rs1799884 and the susceptibility to GDM among individuals of Caucasian descent in all models. However, they did not observe a significant association between GCK rs1799884 and GDM among individuals of Asian descent in the homozygote comparison and recessive model [26]. One possible explanation for the discrepancy is that the relatively small number of samples in previous research (two Asian studies with 1332 cases and 2681 controls) may result in poor reliability results. The current meta-analysis included four case-controlled studies of Asian ethnicity, comprising 4458 controls and 3190 patients.
In a meta-analysis, the extent of heterogeneity is important as non-homogeneous
studies can lead to misleading outcomes. We assessed the significance of
heterogeneity using I
The possibility of publication bias brought on by studies that are only partially reported is a crucial factor to take into account in a meta-analysis. The funnel plot curves and statistical data in our meta-analysis, which included Egger’s and Begg’s tests to evaluate publication bias, showed no indication of publication bias.
The present investigation has several shortcomings: (i) Because of these studies’ restrictive sample number and the limited studies encompassed, the outcomes were inadequate to statistically examine the actual associations; (ii) This research was based on unadjusted OR estimations, since not all incorporated experiments offered adjustable ORs. ORs may have been modulated by various elements, including smoking, ethnicity, or age, even if they were offered; (iii) There was a marked heterogeneity among studies in recessive model and allele contrast.
In summary, as suggested by our meta-analysis, the GCK rs1799884 variant may be useful as a genetic biomarker for GDM. However, more carefully designed investigations conducted across multiple centres are necessary to validate and strengthen our findings.
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
KY conceived and designed the meta-analysis. YH and AW performed the literature search. AW analyzed the data. YH wrote the paper. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.