








 , Hülya Kandemir 2, Selim Kandemir 3, Necim Yalcin 3, Nurullah Peker 4
, Hülya Kandemir 2, Selim Kandemir 3, Necim Yalcin 3, Nurullah Peker 41 Department of Obstetrics and Gynecology, Batman Training and Research Hospital, 72000 Batman, Turkey
2 Department of Obstetrics and Gynecology, Akdeniz University Faculty of Medicine, 07010 Antalya, Turkey
3 Department of Gynecologic Oncology, Antalya Education and Research Hospital, 07000 Antalya, Turkey
4 Department of Obstetrics and Gynecology, Dicle University Faculty of Medicine, 21010 Diyarbakir, Turkey
Abstract
Background: In this study, we aimed to introduce a new technique of
labiaplasty and to evaluate the effect of this novel technique on female genital
self-images, and sexual outcomes and to assess the feasibility of this novel
technique. Methods: We conducted a single-center, retrospective study in
59 women who underwent labiaplasty and vaginoplasty (29 Freya approach technique,
30 classic technique) from 2020 to 2022. Both groups evaluated before (within 7
days) and after (1 month after) surgery with Female Sexual Function Index (FSFI)
and Female Genital Self-Image Scale (FGSIS) questionnaires and all the patients
received postoperative care and follow-up assessments for complications 7 days
and 1 month after surgery. Results: The Freya approach technique was
associated with a shorter operation time (p
Keywords
- FGSIS
- Fibonacci sequence
- FSFI
- golden ratio
- labia minora
- labiaplasty
Female genital cosmetic surgery (FGCS) is a broad term, defined as the surgical alteration of the vulvovaginal anatomy (labiaplasty, vaginoplasty, perineoplasty, clitoral hoodectomy, hymenectomy, labia majora augmentation, and Gspot amplification) [1]. The most popular of the female genital cosmetic surgeries is labiaplasty [2]. In the last five years alone in the USA, the number of labiaplasties has seen a 53% increase [3]. Labiaplasty refers to the surgical reduction of the size of the labia minora. The labia minora contributes sensory and erectile tissue for sexual arousal and intercourse, functions of which require the labia minora to be 1 cm or more in size [4]. Classically, it is considered hypertrophy when the labia minora measure more than 4 cm [5].
Unfortunately, there presently exists no standardization of the procedures
performed. Edge resection [6], wedge resection [7], W shaped resection [8], laser
labiaplasty [9], de-epithelialization [10], composite reduction labiaplasty [11],
custom flask labiaplasty [12], lambda laser nymphoplasty [13], and fenestration
labiaplasty [14] are the most commonly used labia minora reduction techniques
[6, 15]. A variety of techniques have also been described for vaginoplasty [16]
and perineoplasty [17]. The ‘golden ratio’ is very commonly seen in nature, and
it has long been proposed as a characteristic of beauty in nature and in artistic
creations. The golden ratio has been used for years in breast and facial
aesthetic surgeries [18], but we find that it has never been used previously in
female genital cosmetic surgery. We started implementing the golden ratio in
labiaplasty cases as of 2020. To detect the patient satisfaction and quality of
life, specifically designed, validated and reliable patient-reported outcome
measures (PROMs) must be used. The Female Sexual Function Index (FSFI) [19, 20] and the Female Genital Self-Image Scale (FGSIS) [21, 22] questionnaires allow the
efficacy of surgery to be measured from the patient perspective. Our primary goal
was: (1) to determine the golden ratio (inspired by Fibonacci) with a holistic
approach to standardize genital harmony with a purely mathematical ratio other
than existing classification systems [23, 24]. This analysis will identify the
most optimal measures currently in use and provide guidance on the development of
new female genital cosmetic procedure-specific measures, to assess whether the
proportional phi (
This single-center retrospective cohort study was conducted at the Department of Obstetrics and Gynecology of a tertiary care center. The files of 151 women who underwent labiaplasty and/or vaginoplasty by a single operator (EO) between 2020 and 2022 were retrospectively reviewed. The number of patients who underwent both labiaplasty and vaginoplasty was 127 (77 women were operated with Classical Technique (CT) and 50 with FT). Those women who underwent surgery with the FT were defined as the FT group and those women who underwent the CT were defined as CT group. The flowchart of the FT group inclusion process is shown in Fig. 1. 29 women who underwent FT fulfill these criteria agreed to participate and were included in the study.
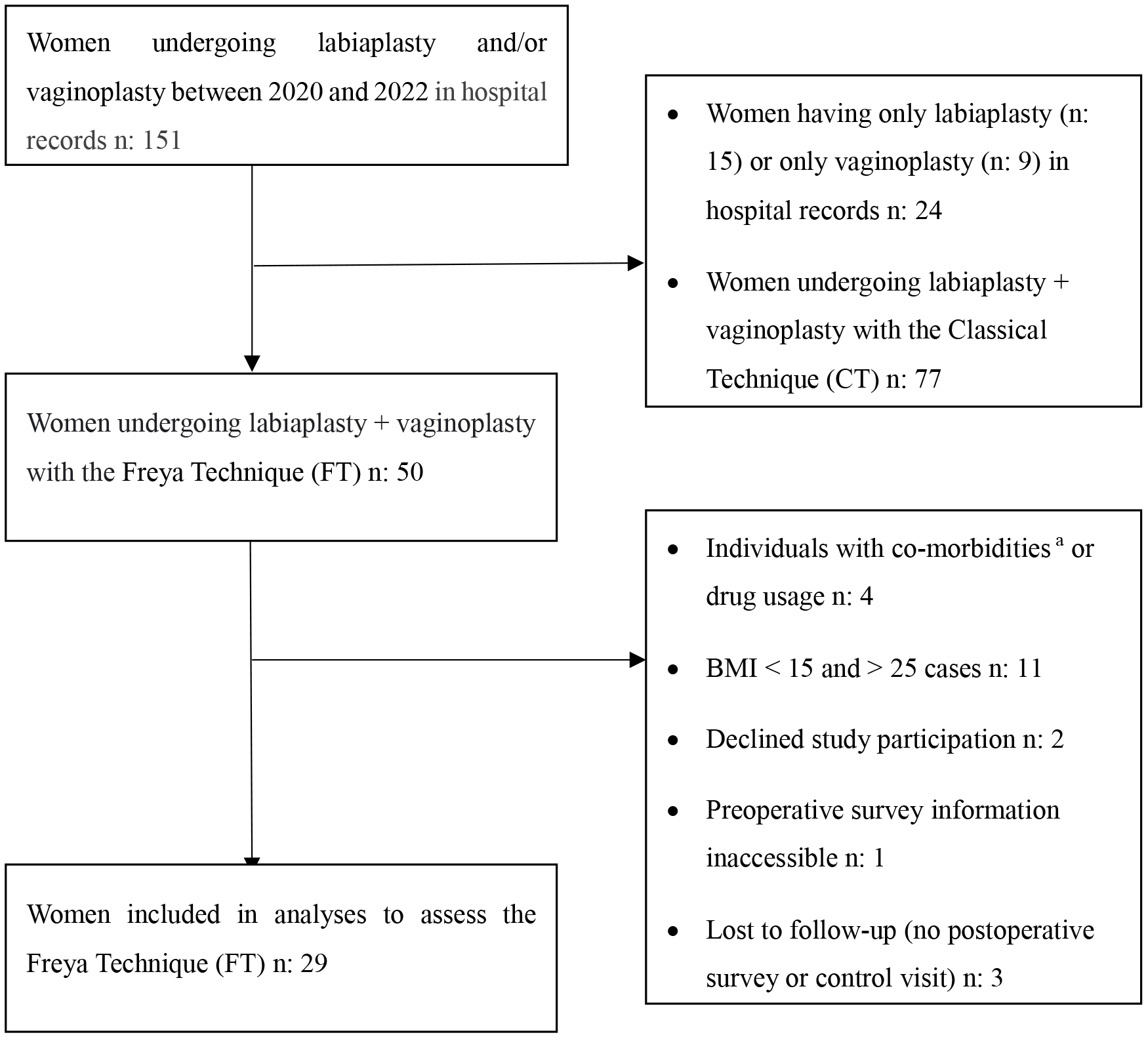 Fig. 1.
Fig. 1.Flowchart of the Inclusion Process of Women with the Freya
Approach Technique. Abbreviations: n, number of patients; BMI, body mass index;
We created a control group of women (n: 77) who underwent the CT between 2020 and 2022 at a tertiary care center. The control group was matched on age, gravida, parity, comorbidity, obesity, and smoking status to women operated using the FT. We randomly selected 30 women who fulfilled the study criteria and agreed to participate in the study. A total of 59 labiaplasty + vaginoplasty cases who fulfilled these criteria agreed to participate and were included in the study. The groups consisted of 29 study women who underwent the FT and 30 comparison women who underwent the CT.
All patients signed an informed consent that allows the participating institution to use their clinical data. Archived patient files and hospital information systems were retrospectively analyzed. Data such as age, body mass index (BMI), gravidity and parity, the number of previous cesarean deliveries and previous uterine surgeries (myomectomy/curettage), FSFI and FGSIS survey results (preoperative and postoperative second month) were analyzed from patient files. Complications were obtained from postoperative day seven and month one examination notes. Monthly examination notes were obtained.
Our hospital is a tertiary care center and detailed anamnesis is taken from
patients who present to our clinic for FGCS (labiaplasty, vaginoplasty or
perineoplasty) (We conducted interviews to obtain descriptive characteristics,
such as age, parity, BMI, marital status, menopausal status, type of delivery,
previous episiotomy, occupation, income status, comorbidities, medication use,
sexual orientation and highest level of education attained). Patients were also
asked whether they had a sexual partner at the time of opting for surgery.
Participants were asked whether they had ever had any kind of cosmetic procedure,
concerns with labial appearance, physical discomfort with clothing and/or
exercise, physical and/or emotional difficulties with sex life, and general
self-consciousness, expectations of surgery, the presenting complaints of which
were recorded Labia minora prolapse, laxity, previous obstetric injury,
functional problems, superficial dyspareunia, chronic irritation (e.g., pain
while wearing underwear or tight clothing or during athletic activities), sexual
dysfunction, pain during intercourse, hypertrophy or asymmetry; postpartum
vaginal laxity (sensation of vaginal laxity), sexual partner’s discomfort with
vaginal laxity, (in addition to their desire of a tighter vagina, their partner
also wanted to feel a tighter vagina), a decrease or lack of ability to reach
orgasm, vaginal flatulence, and urinary incontinence during intercourse. Women
with symptoms and complaints that may have negative effects on the patient’s
sexuality and self-confidence, such as vaginal prolapse, vaginal secretions,
vulvo-vaginitis (more than 10 per year), birth tears in the perineum or bad
episiotomy scars (the woman is uncomfortable with the scar) are evaluated.
Examinations were carried out with all patients in the lithotomy position. The
characteristics of the external genitalia, labial symmetry/asymmetry,
morphological features, color, edge properties of the labia minora, and lengths
and widths of the vaginal opening and vaginal canal diameter (with the number of
fingers that can enter the vagina as two or three fingers) were recorded in the
patient chart. The width of a labium minus was measured from a vertical line
drawn to the base of the labium minus from the widest lateral prominence on
physical examination in centimeters after spreading the labia minora with minimal
traction. We used the Motakef classification to categorize the labia minora
morphologically. Labial protrusion was classified as Class 1 (0–2
cm), Class 2 (2–4 cm), and Class 3 (
All of our cases experienced functional problems. Additionally, those with diabetes, neurological or psychiatric issues, those with a disease or substance abuse, pregnant women, those who have recently given birth (no earlier than one year previously), those with vulvar varicosities, those with pelvic organ prolapse (POP), and those who had previously undergone esthetic genital surgery were not included in our study.
We talk about the CT and the FT (the name Freya was suggested by an artificial intelligence system, the goddess of love, sexuality, beauty and charm in Norse mythology [25]), which are applied in our clinic to all women who apply to our hospital with functional problems and for whom an operation is decided after anamnesis, gynecological examination and psychological evaluation. For both methods, we explain how much the labium minus can be reduced and how much the vaginal opening can be narrowed through the models and digital photographs we have made using 3D printer technology (Fig. 2). How much the vaginal diameter can be narrowed is explained by showing molds of different widths suitable for the patient and explaining that vaginal narrowing will be performed in the mold width requested by the patient. During the consultation, the ideal surgical plan is decided. The patient-centered shared decision-making approach is employed. Then the complications of the operation (CT or FT) requested by the patient (CT or FT) such as wound dehiscence, hematoma, irregular edge formation, scarring, excessive resection, fenestration and shortened vaginal introitus dyspareunia, bleeding, pain, over-tightening of the introitus, bowel or bladder injury, infection, asymmetry, need for revision surgery, blood transfusion, anesthesia techniques and risks are also explained. Every patient is informed by the surgeon (EO (experienced and certified for labiaplasty)) who works in our clinic and developed the Freya approach. Patients who decide to undergo the operation are read the written consent form prepared for this purpose and each patient provides written informed consent.
 Fig. 2.
Fig. 2.Model of vulva produced by 3D printer with software.
FSFI [19, 20] and FGSIS [21, 22] were used to measure satisfaction with genital appearance. FSFI and FGSIS questionnaires were administered to women during face-to-face interviews one week prior to surgery. Their desire to participate in future studies in the same session, demographic data, communication regarding the authorization for the use of examination findings and survey results, and if necessary, informed written consent was obtained from the patient. The FSFI questionnaire consists of 19 questions and evaluates a 6-domain structure that includes desire, subjective arousal, lubrication, orgasm, satisfaction, and pain. The highest score that can be obtained is 36 and the lowest 2 [20]. The FGSIS is a 7-item validated self-report instrument for determining genital self-image. The highest score that can be obtained is 28 and the lowest 7 [22]. In the preoperative period, two erythrocyte suspensions and two fresh frozen plasma preparations were made for each patient. Every patient, except for emergencies, fasted for 8 hours preoperatively. No bowel preparation was made, and to prevent surgery-site infection, prophylactic antibiotics were administered one hour prior to the surgery. Every patient, before entering the operating room, had a urine culture, a cervical and vaginal smear and cytology. Many patients inquire about insurance coverage for this surgery. The ICD-9 (International Statistical Classification of Diseases and Related Health Problems) code 56,620 can be utilized [simple partial vulvectomy].
During the intraoperative period, in every case we managed, the procedure was performed on an inpatient basis. The type of surgery was made according to the patient’s preference every patient received spinal anesthesia and operated in the lithotomy position. Any pubic hair was completely removed, the skin was disinfected three times with povidone iodine solution, the vagina was wiped with povidone iodine, and the patient was covered with a sterile drape. Then, a foley catheter was placed in the bladder. Surgery time was measured from the first skin incision to the last skin suture placement for both techniques.
Classical Technique: In this technique, labiaplasty was performed as originally described by Alter [26] in 1998 with a V-shaped excision of the central portion of most protruding labial tissue and reapproximation of the labial edges (central wedge resection). The labia minora are clamped at the outermost edge, the upper and lower alignment are held and a central wedge or “V” excision is marked in the most protuberant area [27], which usually includes the thickest area of the labium [28]. The surgeon makes a reduction on the basis of the degree of hypertrophy and the patient’s requirements regarding labial edge colour and contour. The primary goal of the operation is to attain minimal or no protrusion of the labia minora beyond the labia majora when the patient is standing. Generally, the labia minora should be covered by the labia majora, if possible. In vaginoplasty, the aim is to decrease the diameter of the vaginal canal by excision of redundant vaginal tissues. The posterior vaginal mucosa is dissected vertically on the midline using a scalpel. Blunt dissection is achieved with a gauze along the lateral aspects of the dissected mucosa until laxity is no longer found and tissue is trimmed to the desired diameter of the vaginal canal. The rectovaginal fascia is approximated circularly with no:0.0 vicryl with two full-round circular sutures separately (with the suture entry lines at 3 and 9 o’clock) with a 2-centimeter horizontal space between them (which is plicated creating a narrower diameter). The remaining posterior wall mucosa is closed using a 2-0 vicryl suture in a continuous crossed manner starting on from the inside to the outside. At the end of the procedures, the vaginal diameter is decreased so that only two fingers can be inserted in at least the lower two-thirds of the vagina. Narrowing of the vaginal entrance (vaginal opening) is performed as described in the FT.
Labiaplasty: The Fibonacci sequence was first described in Indian
mathematics [29]. The ratio of two consecutive Fibonacci numbers tends to the
golden ratio, also known as phi (
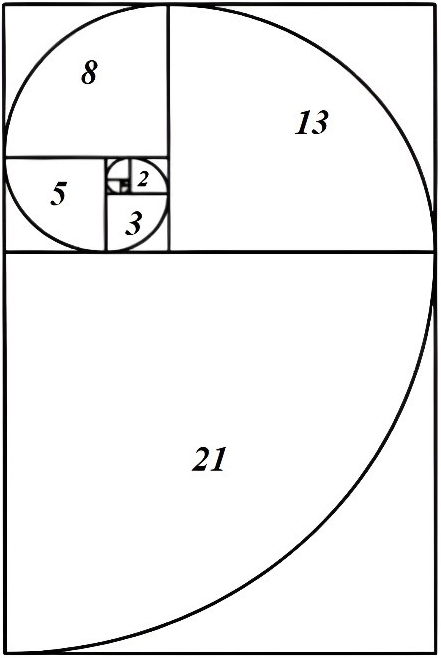 Fig. 3.
Fig. 3.Fibonacci ratios. The golden ratio of 1.618, important to mathematicians, scientists, and naturalists for centuries is derived from the Fibonacci sequence.
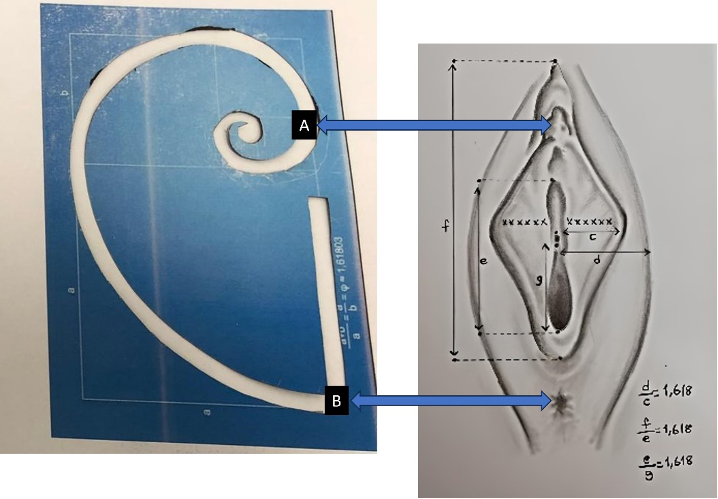 Fig. 4.
Fig. 4.Simulation of Fibonacci spiral to vulva using sticker system. (A) Midpoint of the clitoris; (B) Midpoint of the anus. ((c) postoperative labia minor widest horizontal length; (d) labia major to vaginal introitus horizontal widest length; (e) vertical length of the vaginal introitus; (f) distance from the apex of the clitoris to the posterior forchette skin fold; (g) vertical length of the vaginal introitus from the anterior wall of the vein to the posterior wall of the vagina).
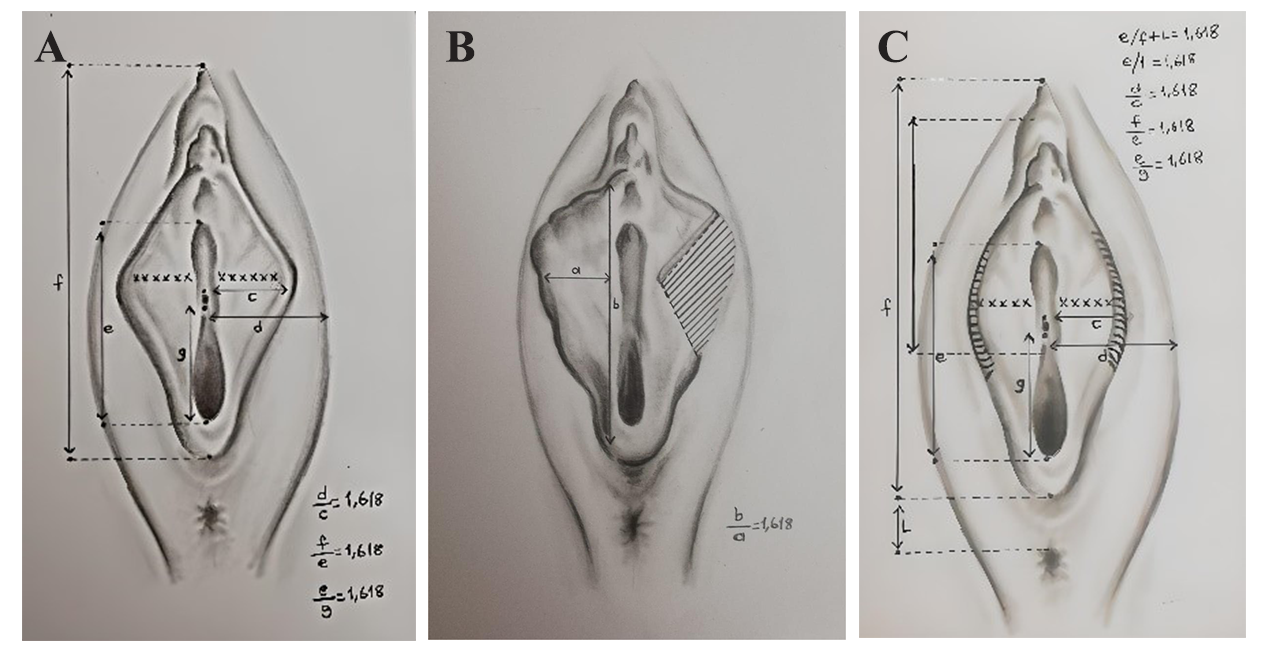 Fig. 5.
Fig. 5.Technical drawings drawn by the artist. (A) Preoperative golden ratio ratios; (B) Calculation of wedge resection according to Fibonacci ratio; (C) Confirmation of Fibonacci ratios in the perioperative period. ((a) labia minor widest horizontal length; (b) labia minor vertical length; (c) postoperative labia minor widest horizontal length; (d) labia major to vaginal introitus horizontal widest length; (e) vertical length of the vaginal introitus; (f) distance from the apex of the clitoris to the posterior forchette skin fold; (g) vertical length of the vaginal introitus from the anterior wall of the vein to the posterior wall of the vagina; (L) distance from the upper border of the anus to the posterior skin line of the vaginal entrance).
Postoperative Management: Fluid replacement, antiemetic and analgesics were used effectively. The patient is mobilized in the sixth postoperative hour. If no urinary injury is present, the catheter is removed after mobilization. Patients are discharged the day after the surgery as long as no complications are experienced. Moreover, we do not routinely prescribe antibiotics upon discharge. Cleaning with an antiseptic solution for three days is encouraged. Sexual intercourse is prohibited for at least four weeks. Patients are seen four weeks and seven days later by the surgeon. Complaints and complications are recorded in the follow-up assessment, and a postoperative questionnaire (FSFI and FGSIS) is completed two months after surgery during a follow-up examination. This study was approved by the Batman training and research hospital ethics committee (Decision No: 787, date 24/10/2020)) and conducted in accordance with the principles of the Declaration of Helsinki. Informed consent forms were obtained from every patient who agreed to participate in the study.
A statistical analysis was performed using the SPSS version 25.0 software (IBM
Corp., Armonk, NY, USA). The Shapiro-Wilk test was used to examine the conformity
of continuous data to the normal distribution. The independent two-sample
t-test was used to analyze the differences in continuous variables
between the two groups when the data conformed to the normal distribution, and
the Mann-Whitney U test was used when the data were not normally
distributed. The Pearson chisquare test and Fisher exact test were used to
evaluate the relationships between the categorical variables. The paired samples
t-test was used to examine the differences between preoperative and
postoperative scale scores for data that were normally distributed, and the
Wilcoxon test was used for data that were not normally distributed. The
relationships between age, number of children and postoperative scores were
analyzed with Spearman’s correlation coefficient. Descriptive data were expressed
as mean
A total of 59 women were included in this study (29 FT, 30 CT). The 59 women
included in the study had at least two symptoms and complaints and all had
Motakeff Class 3 labia minora on examination. All cases in both the CT and FT
groups consisted of individuals who had only normal delivery, had an episiotomy
at delivery, were non-smokers/alcohol users, were married and had active sexual
intercourse, had a BMI
| Freya approach Technique (n: 29) | Classical Technique (n: 30) | Test Statistics | p value | ||
| Age (Mean |
32.55 |
33.47 |
t: −0.704 | 0.484 | |
| Number of living children | |||||
| Median (Min–Max) | 2 (1–4) | 3 (1–4) | U: 402.0 | 0.600 | |
| Operation time | |||||
| 29 (100%) | 10 (33.3%) | ||||
| 0 (0%) | 20 (66.7%) | ||||
| Wound dehiscence n (%) | 2 (6.9%) | 6 (20%) | 0.254 | ||
| Preoperative/Postoperative Hb change percentage | |||||
| 0 | 0 | NA | NA | ||
| 29 (100%) | 30 (100%) | ||||
| Patients undergoing revision labiaplasty n (%) | 1 (3.4%) | 5 (16.7%) | 0.195 | ||
| Patients who underwent revision vaginoplasty n (%) | 0 | 0 | NA | NA | |
| Postoperative labial edema n (%) | 3 (10.3%) | 5 (16.7%) | 0.706 | ||
| Bleeding (vaginal or labium) within 24 hours postoperatively n (%) | 0 | 0 | NA | NA | |
| Postoperative bleeding (vaginal or labial) after 24 hours n (%) | 0 (0%) | 2 (6.7%) | 0.492 | ||
| Patients with complications in the 1st postoperative month n (%) |
2 (6.9%) | 3 (10%) | 1.000 | ||
| Postoperative 24th hour VAS score | |||||
| Mean |
1.93 |
3.63 |
|||
| Median (Min-Max) | 2 (1–5) | 4 (3–4) | U: 87.5 | ||
Abbreviations: SD, standard deviation; t, independent samples t-test; U,
Mann Whitney U test;
While 29 (100%) of the cases approached with FT were operated in less than 90 minutes, only 10 cases (33.3%) were operated in less than 90 minutes with the CT and Visual Analogue Scale (VAS) scores after CT were significantly higher than in the FT group. Regarding postoperative complications, wound dehiscence was observed in two cases (6.9%) in the FT group compared to six cases (20.0%) in the CT group. Only one patient (3.4%) underwent revision labiaplasty in the FT group compared to five patients (16.7%) in the CT group. No postoperative bleeding complications were observed in any of the women in the FT group. Postoperative bleeding complications were observed in two patients (6.7%) in the CT group. Though not significant, there was a trend towards a higher complication rate in the CT group. The primary outcome measures were FSFI and FGSIS. The comparison of preoperative and postoperative FSFI and FGSIS scores in the women who underwent Freya and Classical Techniques is given in Table 2.
| Preoperative | Postoperative | Test Statistics | p value | ||
| Mean |
Mean | ||||
| Median (Min–Max) | Median (Min–Max) | ||||
| FSFI | FT | 16.10 |
28.69 |
Z: −4.707 | |
| 15 (12–24) | 29 (24–32) | ||||
| CT | 12.60 |
25.37 |
Z: −4.787 | ||
| 13.5 (6–18) | 25 (19–33) | ||||
| FGSIS (Feel) | FT | 1.79 |
3.52 |
Z: −4.594 | |
| 2 (1–3) | 4 (3–4) | ||||
| CT | 2.30 |
2.57 |
Z: −1.789 | 0.074 | |
| 2 (1–3) | 2 (2–4) | ||||
| FGSIS (Appear) | FT | 1.76 |
3.24 |
Z: −4.552 | |
| 2 (1–3) | 3 (3–4) | ||||
| CT | 1.90 |
2.33 |
Z: −3.357 | ||
| 2 (1–2) | 2 (2–3) | ||||
| FGSIS (Work) | FT | 1.34 |
3.00 |
Z: −4.893 | |
| 1 (1–2) | 3 (3–3) | ||||
| CT | 1.60 |
2.43 |
Z: −3.987 | ||
| 2 (1–2) | 2 (2–3) | ||||
| FGSIS (Smell) | FT | 1.62 |
1.48 |
Z: −0.943 | 0.346 |
| 2 (1–2) | 1 (1–3) | ||||
| CT | 1.47 |
1.27 |
Z: −1.897 | 0.058 | |
| 1 (1–2) | 1 (1–2) | ||||
| FGSIS (Partner) | FT | 1.79 |
3.31 |
Z: −4.852 | |
| 2 (1–3) | 3 (3–4) | ||||
| CT | 1.87 |
2.70 |
Z: −3.618 | ||
| 2 (1–3) | 3 (2–4) | ||||
| FGSIS (Hcare) | FT | 1.45 |
3.31 |
Z: −4.783 | |
| 1 (1–3) | 3 (3–4) | ||||
| CT | 2.20 |
3.27 |
Z: −4.344 | ||
| 2 (1–3) | 3 (2–4) | ||||
| FGSIS (Embracement) | FT | 1.55 |
3.21 |
Z: −4.615 | |
| 2 (1–3) | 3 (2–4) | ||||
| CT | 1.77 |
3.17 |
Z: −4.363 | ||
| 2 (1–3) | 3 (2–4) | ||||
| FGSIS (Total) | FT | 11.24 |
21.01 |
Z: −4.744 | |
| 11 (9–15) | 21 (19–25) | ||||
| CT | 13.00 |
17.70 |
Z: −4.797 | ||
| 13 (11–15) | 18 (15–20) |
Abbreviations: FSFI, Female Sexual Function Index; FGSIS, Female Genital Self-Image Scale; FT, Freya approach Technique; CT, Classical Technique; Z, Wilcoxon test; SD, standard deviation; Min, minimum; Max, maximum; significant p values shown in bold.
In both groups, postoperative FGSIS scores increased significantly compared to
preoperative FGSIS scores (p
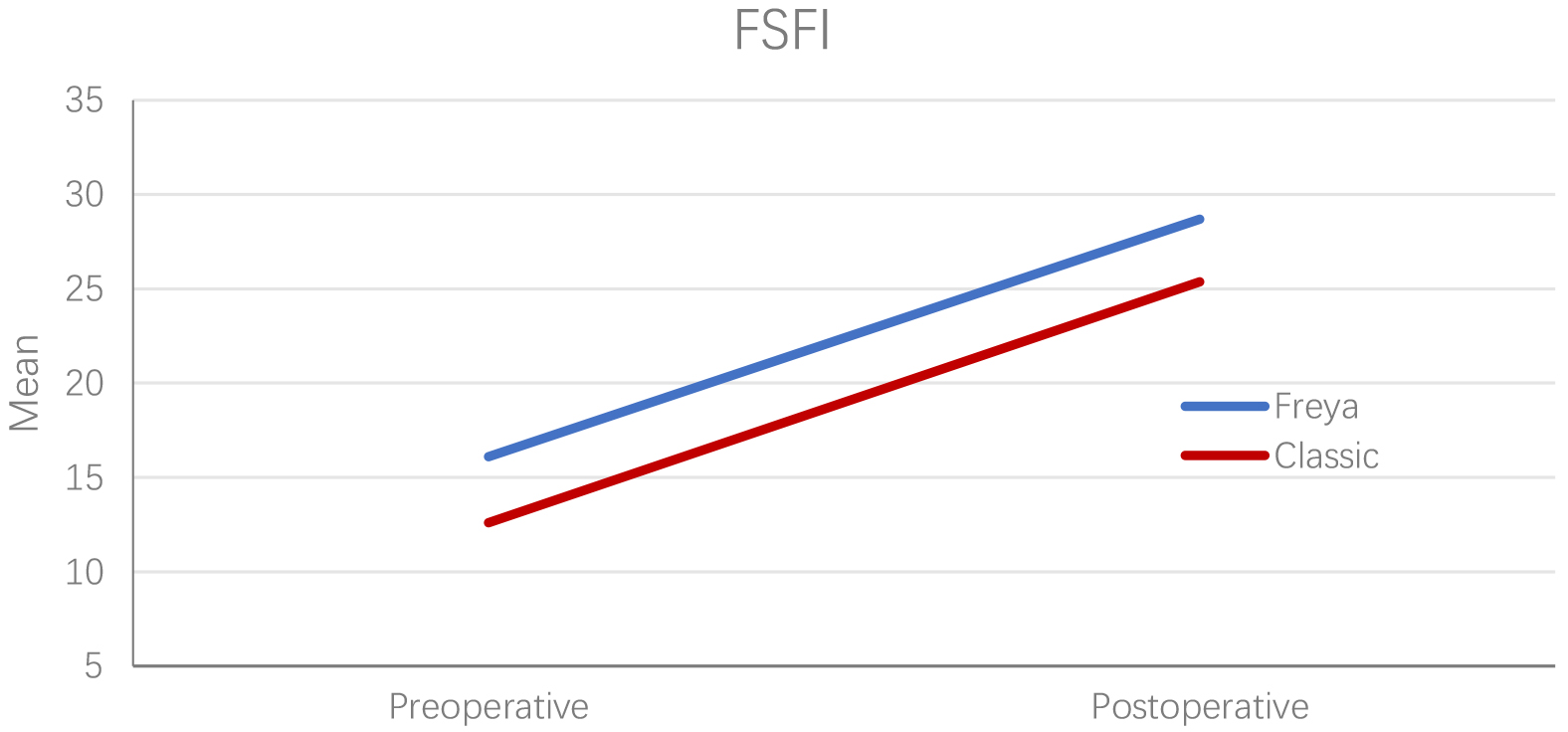 Fig. 6.
Fig. 6.Preoperative and postoperative FSFI scores of women operated with FT and CT. FSFI, Female Sexual Function Index; FT, Freya approach Technique; CT, Classical Technique.
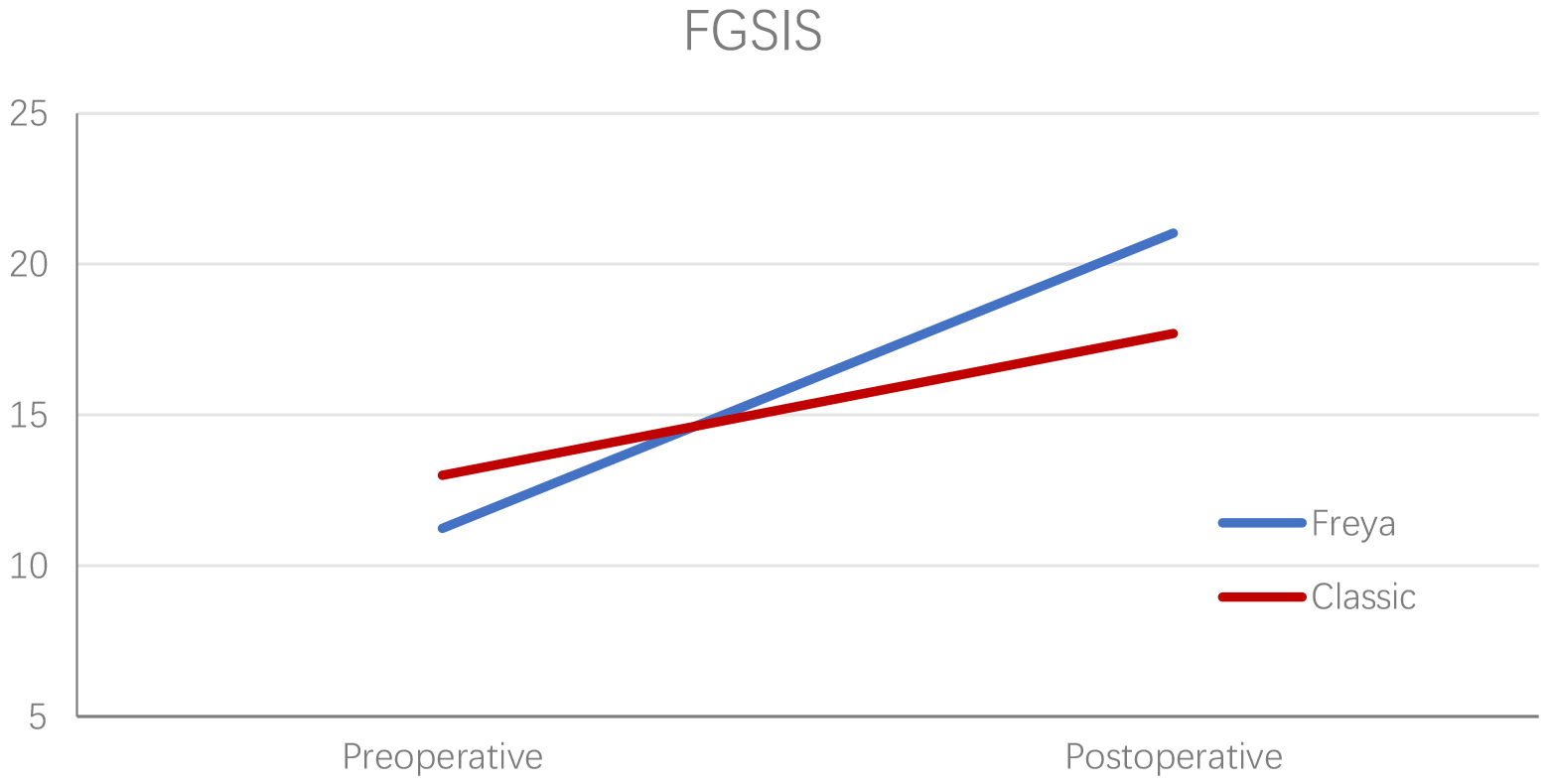 Fig. 7.
Fig. 7.Preoperative and postoperative FGSIS scores of women operated using the FT and CT reliable change on FGSIS questionnaire for the Freya approach technique group at onemonth follow-up (n: 29). FGSIS, Female Genital Self-Image Scale; FT, Freya approach Technique; CT, Classical Technique.
| Freya approach Technique (n: 29) | Classical Technique (n: 30) | Test Statistics | p value | |
| Mean |
Mean | |||
| Median (Min–Max) | Median (Min–Max) | |||
| Preoperative/Postoperative FSFI change percentages (%) | 82.05 |
111.14 |
U: 302.0 | 0.044 |
| 80 (8.33–128.7) | 100 (44–316) | |||
| Preoperative/Postoperative FGSIS change percentages (%) | 89.25 |
37.39 |
U: 17.0 | |
| 90.9 (57.1–122.2) | 38.4 (6.6–72.7) |
Abbreviations: FSFI, Female Sexual Function Index; FGSIS, Female Genital Self-Image Scale; SD, standard deviation; Min, minimum; Max, maximum; U, Mann Whitney U test; %, percent; significant p values shown in bold.
The percent change (mean percent increase scores) of the preoperative and
postoperative FSFI scores was 82.05
| Freya approach Technique | Classical Technique | |||||||
| Postoperative FSFI | Postoperative FGSIS | Postoperative FSFI | Postoperative FGSIS | |||||
| r* | p value | r* | p value | r* | p value | r* | p value | |
| Age | −0.389 | 0.037 | −0.151 | 0.434 | −0.166 | 0.380 | 0.063 | 0.740 |
| Number of Children | −0.070 | 0.703 | −0.100 | 0.605 | 0.368 | 0.046 | 0.496 | 0.005 |
Abbreviations: FSFI, Female Sexual Function Index; FGSIS, Female Genital Self-Image Scale; r*, Spearman’s Correlation Coefficient; significant p values shown in bold.
There was a negative correlation between age and postoperative FSFI scores in
the FT group (r = –0.389, p
FT is an innovative surgical approach described for the first time in the literature, which can be easily applied independent of anatomical variations, provides genital harmony and has fewer complications and much sexual satisfaction and genital self-image scores in the postoperative period.
Negative effects of genital appearance on patients’ sexuality and self-esteem as well as functional discomfort [15] are the motivations of women who request labiaplasty. Unlike some of the previous reports that aesthetics were major concerns, all of our patients reported functional problems and/or sexual problems as their major motivations for surgery. No significant patient report-based differences were observed in functional hygiene problems or discomfort in either group.
The definition of labial hypertrophy has been variably made [23, 24]. In our practice, we considered surgical intervention if a patient has at least two complaints or symptoms and whether we measure the labia minora as Motakef Class 3 [24]. Various techniques to reduce the labia minora have been published with there being no evidence of one surgical technique being better than the other [6, 15]. The most popular algorithms used to define beauty have been the golden proportion, a mathematical ratio of 1:1.618 obtained by dividing the longer part by the shorter part and being equal to the division product of the whole length divided by the longer part [30]. In the CT technique, the labia minora were subjectively shortened. With the FT approach described in this report, inspired by the Fibonacci sequence, we endeavored to capture the golden ratio during labiaplasty and narrow down the vaginal opening. In our opinion, with this approach, we obtained functional labia minora more suitable for genital harmony (Supplementary Figs. 1,2,3,4,5).
Women should be informed about the potential complications of these surgical procedures. Wound dehiscence (9.5%) [31], hematoma (40%) [32], postoperative bleeding [33], pain [5], edema [34], over-resection, fenestration, and shortened vaginal introitus [6] were most common complications. Total complication rates ranged from 4% [28] to 23.8% [31] in wedge resection, 20% [35] in W-shaped resection, and 2% [12] in custom flask labiaplasty. However, our complications were not serious. The overall complication rate was 17.24% for the FT and 43.33% for the CT group with wound dehiscence, edema, and postoperative bleeding. We identified that there was a tendency for the CT to be more likely to develop wound dehiscence than the FT. In addition, our study provides additional information for postoperative VAS scores, where we found that postoperative VAS scores were significantly lower, especially when using this new approach. Another advantage of the new approach was that the operation time was less than 90 minutes. However, more than half of the cases in the CT group took longer than 90 minutes.
Revision labiaplasty rates are in the order of 2.9–19% [6, 28, 34] depending on the techniques. We have shown similar revision labiaplasty rates (FT: 3.4%, CT: 16.7%) in the present study.
Women wanting labiaplasty desire the procedure so as to improve the appearance of the external genitals and enhance their attractiveness, sexual desire, and self-confidence [36]. Little is known about the benefit of sexual function enhancement and partner satisfaction of these surgeries [15, 37]. Surgical techniques have favorable outcomes in terms of patient satisfaction, and satisfaction rates have always exceeded 90% [6]. The results of these studies suggest that genital cosmetic surgery treats both cosmetic and functional issues and enhances sexual satisfaction [15, 38, 39]. In our series, 100% of the patients were satisfied with the aesthetic, functional, sexual, and overall outcomes of their labiaplasties.
Outcomes evidence for labiaplasty is currently insufficient; however, a number
of studies have provided an evaluation of patient satisfaction by means of
questionnaires completed by the patients [34]. Having quantitative, specifically
designed, validated and reliable PROMs would be useful to improve evidence-based
practice, potentially assist with improvements in surgical techniques, and
facilitate the decision-making process of patients and surgeons [15, 37]. In a
systematic review, 96% of women had clinically significant improvements in
questionnaires [3]. In a retrospective study, participating women reported
statistically significant increases in their genital appearance satisfaction,
sexual satisfaction and psychological well-being [39]. We used FSFI and FGSIS
questionnaires to assess changes in sexual function and genital self-image. Our
results from the FSFI and FGSIS scores were consistent with promising findings.
In a prospective cohort study using the FSFI questionnaire, no significant effect
of surgery was noted on desire, lubrication, orgasm, pain, or total score at
either time point, but scores on arousal and satisfaction increased immediately
after surgery, then fell back to baseline levels on follow-up [40]. In another
prospective study, total study group scores on the FGSIS (24.91) were
significantly better than entry, 15.58 (p
The strengths of this study are that it is a new approach, there is a control group, all operations are performed by a single surgeon, the type of operation is based on the patient’s preference, and validated outcome measures are used. The limitations of the current research are its retrospective study design, relatively small sample size on satisfaction, complications, and outcomes (which may not have been representative of the wider population of women seeking labiaplasty), lack of long-term data (only complications one month after surgery and survey evaluations two months after surgery) (meaning that making reliable conclusions regarding postoperative outcomes for patients is currently not possible). Good PROMs need to be developed, as does a reliable method of gathering quantitative measures on sensation before and after labiaplasty.
Many factors should be considered before determining the type of labiaplasty. These include the experience of the surgeon, the extent of the pathology, and the specific characteristics of the patient. This novel labiaplasty approach is simple and safe, and it could be very useful to reduce operative time and postoperative pain by avoiding excessive resection. Moreover, it improves genital appearance and sexual satisfaction. Future research should involve genital surgery focused PROM to assess the outcomes, benefits, and appropriate indications of these different surgical techniques more accurately. We propose the utilization of the golden ratio as the most appealing symmetrical form, which characterizes attractive labias. FT can be explored for achieving a more aesthetically pleasing appearance in labia minora reconstruction during genital gender affirmation surgery for transgender women.
The data obtained from the study can be freely accessed upon contacting the author without neglecting participant information.
EO and NP designed the research study; EO, HK, NY and SK wrote the study; EO performed the surgery; EO, SK, HK, NY analyzed the data and statistics; EO and NY performed literature search; EO and SK critically reviewed the study; NP supervised the final version. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content and agreed to be accountable for all aspects of the work in ensuring that questions related to its accuracy or integrity. All authors read and approved the final manuscript.
This study was approved by the Batman training and research hospital ethics committee (Decision No: 787, date 24/10/2020) and conducted in accordance with the principles of the Declaration of Helsinki. Informed consent forms were obtained from every patient who agreed to participate in the study.
We would like to thank Hamit Can, the art teacher who made the pencil drawings and allowed us to use them in the study.
This research received no external funding.
The authors declare no conflict of interest. Nurullah Peker is serving as one of the Guest editors of this journal. We declare that Nurullah Peker had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Michael H. Dahan.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.