


 , Min Liu 1,*,†
, Min Liu 1,*,†1 Department of Nutrition, The Third Xiangya Hospital, Central South University, 410013 Changsha, Hunan, China
2 Department of Obstetrics and Gynecology, The Third Xiangya Hospital, Central South University, 410013 Changsha, Hunan, China
3 Department of Geriatrics, First Affiliated Hospital of Hunan Normal University of Central South University, 410013 Changsha, Hunan, China
4 Department of Radiology, The Third Xiangya Hospital, Central South University, 410013 Changsha, Hunan, China
†These authors contributed equally.
Abstract
Background: The prevalence of gestational diabetes mellitus (GDM) has been increasing globally, which has led to substantial implications for long-term maternal health including diabetes. The present study aimed to explore the rate of postpartum glucose screening (PGS) of women with GDM based on WeChat management and explore factors affecting the rate of PGS and impaired glucose regulation (IGR). Methods: In this prospective trial, GDM patients were enrolled in our WeChat platform groups. Demographic and medical data were collected at the baseline surveys and follow-up visits. GDM patients were managed throughout their pregnancies via the WeChat platform. We sent messages, involving multidisciplinary care, medical nutritional therapy, and glucose monitoring every three days in the chat groups, and reminded them to go to the hospital to complete PGS. Questionnaires about PGS via the WeChat platform were sent to those women who had delivered within 4 to 12 weeks postpartum. Answers to the questionnaires [understanding the necessity of postpartum oral glucose tolerance testing (OGTT) screening, and the results of 42-day postpartum OGTT screening, as well as the reasons for failing to finish postpartum screening, and the ways to get nutrition knowledge for GDM patients] were collected. Results: From 1 January 2016 to 31 August 2019, 490 participants were included in our WeChat groups, 375 of whom completed questionnaires. Among the 375 participants, 277 (73.9%) had completed post-partum 75 g OGTT, 202 (72.9%) had normal glucose levels, and 75 (27.1%) had impaired glucose regulation (IGR). Univariable logistic analysis and stepwise regression analysis demonstrated that a previous history of GDM and cesarean delivery were the two variables influencing PGS (odds ratio (OR): 0.44, 95% confidence interval (95% CI): 0.20–0.94; OR: 1.88, 95% CI: 1.04–3.39, respectively). Insulin treatment during pregnancy and cesarean delivery were found to have a significant association with postpartum IGR (OR: 3.74, 95% CI: 1.97–7.08; OR: 1.83, 95% CI: 1.02–3.28, respectively). Conclusions: The WeChat messaging platform may be a useful tool to promote postpartum OGTT screening in women with GDM. Women who failed to return for PGS were more likely to have prior GDM than those who returned for PGS. Women who had postpartum IGR were more likely to use insulin treatment during pregnancy and more likely to deliver by cesarean delivery compared to those who had normal postpartum glucose results. Clinical Trial Registration: The present study was registered at ClinicalTrials.gov Protocol Registration and Results System https://classic.clinicaltrials.gov/ (No. NCT02893072).
Keywords
- gestational diabetes mellitus (GDM)
- oral glucose tolerance test
- postpartum period
- WeChat platform
- insulin treatment
Gestational diabetes mellitus (GDM) is defined as any degree of abnormal glucose results during pregnancy [1]. GDM is one of the most common medical complications of pregnancy and it is increasing in prevalence globally, due to the background of an increase in the rates of obesity in women of reproductive age and rise in maternal age [2]. Women with a history of GDM have an increased risk of developing impaired glucose regulation (IGR) [3, 4]. Approximately 50% of women with GDM developed diabetes within 5 years after their pregnancies [5]. Also, metabolic syndrome and cardiovascular diseases are commonly reported to be associated with GDM [6]. These long-term outcomes not only threaten the health of women but also increase the economic burden to the health care system. Therefore, it imperative to systematically manage GDM patients and to identify, intervene, and prevent these patients from developing a chronic disease.
The 6-week postpartum visit with a 75 g oral glucose tolerance testing (OGTT) is
crucial for the long-term health of GDM women. Therefore, a plethora of clinical
practice guidelines recommend postpartum glucose screening [7, 8, 9]. In China, women
who failed to pass the 75 g OGTT postpartum (fasting
Research has shown that maternal age, body mass index (BMI), race/ethnicity, and family history are associated with the prevalence of GDM and type 2 diabetes mellitus (T2DM) [17]. This study aimed to (1) check the screen rate of the WeChat platform management in GDM women; (2) explore independent predictors of the completion rate of postpartum OGTT, and postpartum IGR via the WeChat platform management.
In the single-site, prospective trial, we recruited patients diagnosed as GDM during 24 to 28 weeks gestation from the Third Xiangya Hospital of Central South University, Changsha, China. Inclusion criteria included the diagnosis of GDM according to International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria [18], and ability to give informed consent. Exclusion criteria were the diagnosis of diabetes prior to pregnancy, multiple gestation, and patients who were taking medications known to influence glucose homeostasis prior to enrollment. This study was approved by the Institutional Review Boards of the Third Xiangya Hospital, Central South University (No: 2020-S262), China, and was also registered at ClinicalTrials.gov Protocol Registration and Results System (No. NCT02893072). Written informed consent was obtained from all participants before entering the trial.
GDM patients from 1 January 2016 to 31 August 2019 were enrolled in our WeChat
platform groups. The included patients who joined our WeChat
platform group were managed by two researchers. Both researchers had undergone
systematic academic training, possessed rigorous scientific research thinking and
were qualified to organize drug clinical trials. The researchers were responsible
for collecting the demographic data and clinical information at baseline survey
and follow-up visits via the WeChat platform or face-to-face consultation in the
outpatient department. The GDM women who visited in outpatient department would
make an appointment with the obstetrics and physician on the same day. The
individual participant data was recorded independently by both researchers. GDM
patients were invited to the WeChat group on their first visit to the clinical
nutrition department. The researchers offered nutrition knowledge about GDM based
on the WeChat platform every three days following the establishment of the chat
group. The messages involve nutrition advice (such as what is low glycemic index
food, and how to prepare a balanced diet etc.), the importance of postpartum
screening (such as the incidence of GDM progressing to diabetes mellitus (DM),
the importance of postpartum screening to diagnose DM, and what should be done
for early identification of T2DM etc.), and multidisciplinary care (such as the
original video educating how to test fingertip blood glucose and insulin
injection procedure). We reminded them to go to the hospital for the follow-up
screening of postpartum OGTT via the WeChat platform.
For those patients who did not respond to us
on the WeChat platform, researchers sent them a private message to make sure they
received our message. In January 2020, we identified participants who had
delivered within 4 to 12 weeks from the establishment of the database at the
patient’s first visit. In February 2020, a questionnaire was sent via WeChat to
those participants. The questionnaire included the maternal postpartum OGTT and
postpartum glucose results. In addition, medical documents such as OGTT report
sheets and prescriptions were delivered as photos via WeChat, and the original
data was persevered. Pre-pregnancy body mass index (BMI) was calculated by
dividing pre-pregnancy weight in kilograms by the square of height,
and categorized as low, normal, and
overweight (
We allocated participants who completed questionnaires into two groups: patients who completed OGTT postpartum were included in group 1 and patients who did not complete OGTT postpartum were included in group 2. Postpartum OGTT was defined as completion of the OGTT between 4 and 12 weeks postpartum. We also allocated participants who completed postpartum OGTT into two groups: normal or abnormal glucose tolerance. The collected data is presented in the flowchart (Fig. 1).
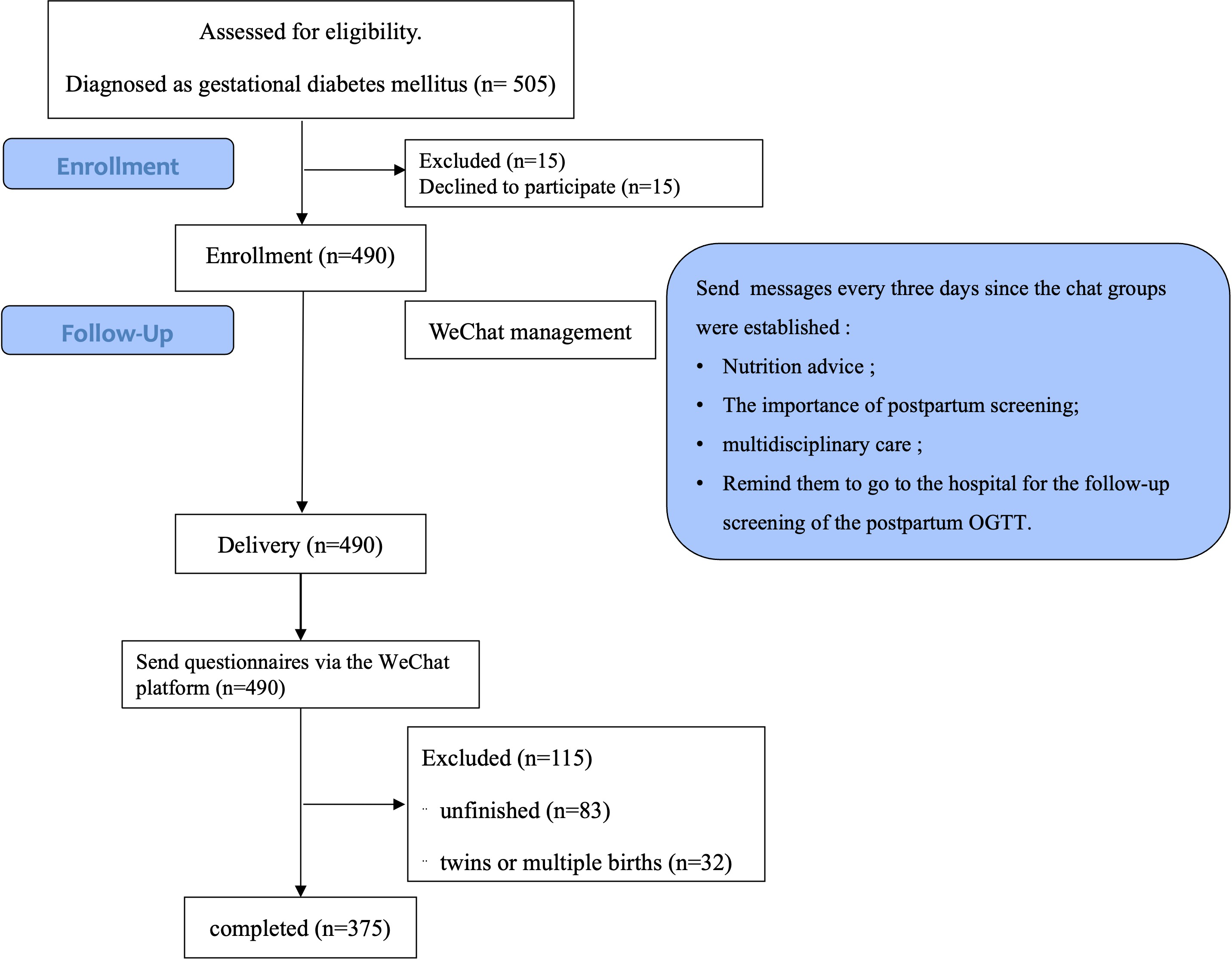 Fig. 1.
Fig. 1.Flowchart. OGTT, oral glucose tolerance testing.
Postpartum OGTT means that GDM patients who had delivered previously between 4
and 12 weeks finished a standard oral 75 g glucose tolerance test. The diagnosis
of postpartum diabetes is based on the diagnostic criteria established by the
American Diabetes Association in 2016 [21]. Three situations (normal glucose
tolerance (NGT), impaired glucose tolerance (IGT), and DM)
were recorded. DM was diagnosed as fasting plasma glucose (FPG)
This study was powered to detect the rate of postpartum OGTT under the management of the WeChat platform. With an expected standard deviation (SD) of 0.1 and an allowable error of 0.01, we calculated that the sample size necessary was 384 participants. We aimed to recruit 480 participants to account for a predicted approximate 20% withdrawal rate.
The principal statistical analysis was for the primary outcome of postpartum OGTT rate and for the secondary outcomes of the normal rate of postpartum OGTT results, factors influencing the obtaining the situation of postpartum OGTT, and factors influencing abnormal postpartum glucose results. Missing data were assumed to be missing at random. Where the missing values occurred at the baseline visit, we used available data from the follow-up visit. If the missing value occurred at the end of the study, we used a last-observation-carried-forward rule. We imputed missing data within a timed series using a mean imputation rule.
All analyses were performed using Stata version 14.0 (Stata version 14.0, Stata Corp, College Station, TX, USA). The individual participant data at baseline and follow-up was entered independently by both researchers. The percent agreement on the data entry between the two researchers was 100%. The data was compared in the two groups in which women did or did not receive postpartum glucose screening using the two-tailed t test and the chi-square test.
Univariable logistic analysis and stepwise regression analysis were used for the
following outcomes: factors influencing the obtaining of postpartum OGTT and
factors influencing abnormal postpartum glucose results. We included the
demographic and clinical parameters as independent variables and completion
situation of the postpartum OGTT screening status (or postpartum IGR) as
dependent variable. We then conducted univariable logistic analysis and chose the
variables whose p
A total of 490 patients participated in our project from 1 January 2016 to 31
August 2019. Three hundred and seventy five completed our online
questionnaire in February 2020 and were included in our analysis. The percentage
of the participants in the years 2016, 2017, 2018, and 2019 were almost the same
(22.5%, 26.1%, 25.3%, and 26.1%, respectively, p
| Baseline of study participants | n (%) | |
| Maternal age (years) | ||
| 2/375 (0.5) | ||
| 25 |
65/375 (17.3) | |
| 30 |
170/375 (45.3) | |
| 138/375 (36.8) | ||
| Participants numbers | ||
| In year 2016 | 84 (22.5%) | |
| In year 2017 | 98 (26.1%) | |
| In year 2018 | 95 (25.3%) | |
| In year 2019 | 98 (26.1%) | |
| Race | ||
| Han nationality | 358/375 (95.5) | |
| Others | 17/375 (4.5) | |
| Education level | ||
| High school degree or lower | 63/375 (16.8) | |
| College or bachelor’s degree | 280/375 (74.7) | |
| Master’s degree or above | 32/375 (8.5) | |
| Income (dollars/month per household) | ||
| 3/375 (0.8) | ||
| 139 |
15/375 (4.0) | |
| 417 |
77/375 (20.5) | |
| 696 |
162/375 (43.2) | |
| 118/375 (31.5) | ||
| Insurance | ||
| Have medical insurance | 364/375 (97.1) | |
| No medical insurance | 11/375 (2.93) | |
| Gravidity | ||
| Primigravida | 135/375 (36.0) | |
| Multigravida | 240/375 (64.0) | |
| Pregnancy methods this time | ||
| Natural conceive | 359/375 (95.7) | |
| Assisted reproductive technology | 16/375 (4.3) | |
| Medical history | ||
| No diseases | 328/375 (87.5) | |
| Polycystic ovary syndrome | 37/375 (9.9) | |
| Hyperlipidemia | 11/375 (2.9) | |
| Hypertension | 4/375 (1.1) | |
| Adverse pregnancy events | ||
| No diseases | 123/375 (32.8) | |
| Miscarriage | 143/375 (38.1) | |
| Macrosomia | 33/375 (8.8) | |
| Caesarean section | 104/375 (27.7) | |
| GDM | 35/375 (9.3) | |
| Stillbirth fetus | 13/375 (3.5) | |
| Family history of diabetes | ||
| Yes | 82/375 (21.9) | |
| No | 293/375 (78.1) | |
| Pre-pregnancy BMI (kg/m |
22.9 (15.9–40.9) | |
| Low ( |
22/375 (5.9) | |
| Normal (between 18.5 and 23.9 kg/m |
245/375 (65.3) | |
| High ( |
108/375 (28.8) | |
GDM, gestational diabetes mellitus; BMI, body mass index.
| Findings from the questionnaire | n (%) | |
| Understand the necessity of postpartum OGTT screening | ||
| Yes | 356/375 (94.9) | |
| No | 19/375 (5.1) | |
| Finished postpartum OGTT screening | ||
| Yes | 277/375 (73.9) | |
| Yo | 98/375 (26.1) | |
| Results of 42-day postpartum OGTT screening | ||
| Normal | 202/277 (72.9) | |
| IGT or IFG | 69/277 (24.9) | |
| Diabetes | 6/277 (2.2) | |
| Reasons for not completing postpartum screening | ||
| People’s time was occupied by taking care of baby | 39/98 (39.8) | |
| People believed that glucose could return to normal after delivery | 32/98 (32.7) | |
| People had no symptoms | 22/98 (22.5) | |
| Waiting time was so long in hospital | 20/98 (20.4) | |
| Others | 14/98 (14.3) | |
| Ways to get nutrition knowledge for GDM patients | ||
| Obstetrician | 24/375 (6.4) | |
| Nutritionist | 254/375 (67.7) | |
| Network | 85/375 (22.7) | |
| Professional lecture | 2/375 (0.5) | |
| Others | 10/375 (2.7) | |
OGTT, oral glucose tolerance testing; IGT, impaired glucose tolerance; IFG, impaired fasting glucose.
In order to assess predictors for those who were screened for OGTT versus those
who were not, questionnaire results were divided into group 1 (completed
postpartum OGTT) and group 2 (did not complete postpartum OGTT). There were
significant differences between the two groups regarding parameters such as age,
race, educational level, gravidity, history of miscarriage, history of
macrosomia, history of GDM, family history of diabetes, delivery mode, and
average household income (p
| Group 1 [n (%)] | Group 2 [n (%)] | p | ||
| Age (years) | ||||
| 169 (61.0) | 68 (69.4) | |||
| 108 (39.0) | 30 (30.6) | |||
| Race | ||||
| Han nationality | 262 (94.6) | 96 (98.0) | ||
| Other | 15 (5.4) | 2 (2.0) | ||
| Education level | ||||
| High school degree or lower | 46 (16.6) | 17 (17.3) | ||
| College or bachelor’s degree | 203 (73.3) | 77 (78.6) | ||
| Master’s degree or above | 28 (10.1) | 4 (4.1) | ||
| Gravidity | ||||
| Primigravida (%) | 100 (36.1) | 35 (35.7) | ||
| Multigravida (%) | 177 (63.9) | 63 (64.3) | ||
| History of miscarriage | ||||
| Yes (%) | 107 (38.6) | 36 (36.7) | ||
| No (%) | 170 (61.4) | 62 (63.3) | ||
| History of macrosomia | 177 | 63 | ||
| Yes (%) | 24 (13.6) | 9 (14.3) | ||
| No (%) | 153 (86.4) | 54 (85.7) | ||
| History of GDM | ||||
| Yes (%) | 21 (11.9) | 14 (22.2) | ||
| No (%) | 156 (88.1) | 49 (77.8) | ||
| Family history of diabetes | ||||
| Yes (%) | 60 (21.7) | 22 (22.4) | ||
| No (%) | 217 (78.3) | 76 (77.6) | ||
| Pre-pregnancy weight (kg) | 57.69 |
58.00 |
0.800 | |
| Pre-pregnancy BMI (kg/m |
22.84 |
22.93 |
0.840 | |
| Delivery mode | ||||
| Natural birth | 123 (44.4) | 52 (53.1) | ||
| Caesarean section | 154 (55.6) | 46 (46.9) | ||
| Average household income per capita | ||||
| 139 to 417 Dollars | 12 (4.3) | 6 (6.1) | ||
| 417 to 696 Dollars | 57 (20.6) | 20 (20.4) | ||
| 696 to 1390 Dollars | 117 (42.2) | 45 (45.9) | ||
| More than 1390 Dollars | 91 (32.9) | 27 (27.6) | ||
| Predictor variables | Univariable analysis | Stepwise regression analysis | |
| OR (95% CI) | OR (95% CI) | p value | |
| Maternal age ( |
1.10 (0.60–2.03) | ||
| Nationality (minority) | 1.57 (0.17–14.18) | ||
| Conception way (in-vitro fertilization) | 2.26 (0.24–20.91) | ||
| BMI before pregnancy | 0.85 (0.49–1.49) | ||
| Weight gain during pregnancy | 0.97 (0.69–1.37) | ||
| History of GDM | 0.42 (0.19–0.94) | 0.44 (0.20–0.94) | 0.03 |
| History of macrosomia | 0.80 (0.32–2.01) | ||
| Level of education | 1.62 (0.89–2.95) | ||
| Average household income per capita | 1.13 (0.79–1.64) | ||
| Family history of diabetes | 1.26 (0.53–2.99) | ||
| Insurance | 0.45 (0.05–4.40) | ||
| Insulin treatment during pregnancy | 1.57 (0.63–3.90) | ||
| Delivery mode (caesarean section) | 1.73 (0.91–3.28) | 1.88 (1.04–3.39) | 0.04 |
| Gestational age at delivery | 0.88 (0.32–2.47) | ||
| Ways of baby feeding (breast feeding) | 0.91 (0.69–1.21) | ||
OR, odds ratio; 95% CI, 95% confidence interval; GDM, gestational diabetes mellitus.
To assess predictors for those who had abnormal postpartum glucose results, the
questionnaire result for those who had completed postpartum OGTT were divided
into group 1 (IGT or IFG or DM) and group 2 (normal glucose results). There were
significant differences between the two groups regarding parameters such as age,
history of miscarriage, and delivery mode (p
| Variables | Completed postpartum OGTT (n = 277) | IFG/IGT/DM (n = 75) | NGT (n = 202) | p value | |
| Maternal age (years) | |||||
| 169 (61.0) | 38 (50.7) | 131 (64.9) | 0.030 | ||
| 108 (39.0) | 37 (49.3) | 71 (35.1) | |||
| Race | |||||
| Han nationality | 262 (94.6) | 68 (90.7) | 194 (96.0) | 0.080 | |
| Other | 15 (5.4) | 7 (9.3) | 8 (4.0) | ||
| Education level | |||||
| High school degree or lower | 46 (16.6) | 14 (18.7) | 32 (15.9) | 0.880 | |
| College or bachelor’s degree | 203 (73.3) | 51 (68.0) | 152 (75.2) | ||
| Master’s degree or above | 28 (10.1) | 10 (13.3) | 18 (8.9) | ||
| Gravidity | |||||
| Primigravida | 100 (36.1) | 20 (26.7) | 80 (39.6) | 0.040 | |
| Multigravida | 177 (63.9) | 55 (73.3) | 122 (60.4) | ||
| History of miscarriage | |||||
| Yes | 107 (38.6) | 38 (50.7) | 69 (34.2) | 0.010 | |
| No | 170 (61.4) | 37 (49.3) | 133 (65.8) | ||
| History of macrosomia | 177 | ||||
| Yes | 24 (13.6) | 6 (10.9) | 18 (14.8) | 0.490 | |
| No | 153 (86.4) | 49 (89.1) | 104 (85.2) | ||
| History of GDM | 177 | ||||
| Yes | 21 (11.9) | 9 (12.0) | 12 (11.8) | 0.960 | |
| No | 156 (88.1) | 66 (88.0) | 90 (88.2) | ||
| Family history of diabetes | |||||
| Yes | 60 (21.7) | 21 (28.0) | 39 (19.3) | 0.120 | |
| No | 217 (78.3) | 54 (72.0) | 163 (80.7) | ||
| Delivery mode | |||||
| Natural birth | 123 (44.4) | 23 (30.7) | 100 (49.5) | 0.005 | |
| Caesarean section | 154 (55.6) | 52 (69.3) | 102 (50.5) | ||
| Average household income per capita | |||||
| 139 to 417 Dollars | 12 (4.3) | 3 (4.0) | 9 (4.5) | 0.220 | |
| 417 to 696 Dollars | 57 (20.6) | 19 (25.3) | 38 (18.8) | ||
| 696 to 1390 Dollars | 117 (42.2) | 33 (44.0) | 84 (41.6) | ||
| More than 1390 Dollars | 91 (32.9) | 20 (26.7) | 71 (35.1) | ||
NGT, normal glucose tolerance; IGT, impaired glucose tolerance; IFG, impaired fasting glucose; DM, diabetes mellitus.
| Predictor variables | Univariable analysis | Stepwise regression analysis | |
| OR (95% CI) | OR (95% CI) | p value | |
| Maternal age ( |
1.03 (0.48–2.18) | ||
| Nationality (minority) | 7.72 (1.13–52.83) | NA | |
| Conception way (in-vitro fertilization) | 0.06 (0.01–0.67) | NA | |
| BMI before pregnancy | 1.12 (0.37–3.35) | ||
| Weightgain during pregnancy | 0.82 (0.54–1.25) | ||
| History of GDM | 1.45 (0.49–4.28) | ||
| History of macrosomia | 0.38 (0.11–1.37) | ||
| Level of education | 0.63 (0.31–1.31) | ||
| Average household income per capita | 0.73 (0.46–1.16) | ||
| Family history of diabetes | 2.33 (0.89–6.08) | NA | |
| Insulin treatment during pregnancy | 3.84 (1.51–9.73) | 3.74 (1.97–7.08) | |
| Delivery mode (caesarean section) | 2.70 (1.19–6.13) | 1.83 (1.02–3.28) | 0.040 |
| Gestational age at delivery | 0.47 (0.16–1.43) | ||
| Ways of baby feeding (brest feeding) | 0.73 (0.52–1.04) | NA | |
OR, odds ratio; GDM, gestational diabetes mellitus; NA, not included in the stepwise regression analysis.
The prevalence of GDM has been increasing globally including China. In Tianjin,
a cosmopolitan city in North China, the prevalence of GDM increased from 2.3% in
1999 to 8.1% in 2012 [4]. GDM has substantial implications for long-term
maternal health including a 13-fold increased risk of GDM [22] in a subsequent
pregnancy and a 10-fold higher risk of developing DM later in life as compared to
those with normal glycemia level in pregnancy [3]. Given the global prevalence of
metabolic diseases, GDM management should now shift to early postpartum
prevention strategies to reduce the progression of GDM toward type 2 diabetes and
address long-term maternal metabolic risks. Many clinical practice guidelines
recommend screening for blood glucose in the postpartum period [7, 8]. Persistent
hyperglycemia for the diagnosis of T2DM in the immediate postpartum period
(within 1–3 days) is uncommon. Thus, delayed glucose testing is recommended to
occur 4 to 12 weeks postpartum when IGT is detected in 17% to 23% of women with
antecedent GDM pregnancies. The National Institute for Health and Care Excellence
(NIHCE) endorses FPG testing at 6 to 13 weeks postpartum. This has the potential
to increase the rate of missed diagnosis as up to 40% more women having T2DM
using the 75 g OGTT as compared with FPG alone. Thus, the NIHCE recommends an
abnormal screening FPG (
Major organizations have proposed that GDM patients complete postpartum OGTT screening at 4–12 weeks postpartum as it is the most convenient evidence-based approach [9, 23]. Ideally, all GDM patients need to undergo an OGTT at their 6-week postpartum visit. Postpartum OGTT screening has the potential to identify individuals with IGT or IFG, which may be reversible [24]. Chang et al. [10] found that only 282 (13.1%) of 2152 Chinese GDM patients completed glucose screening after delivery. Researchers from USA found that 40.85% to 45% GDM patients finished postpartum glucose screening in the USA [11, 25]. A study from France showed that only 154 (38.1%) of 404 GDM patients participated in the postpartum OGTT [26]. A 13-year Italian cohort study found that only 26.3% of GDM women had a postpartum OGTT [27].
Many researchers are seeking ways to improve the postpartum glucose screening rate following GDM. Carson et al. [28] found that contacting patients proactively via phone calls, or postal reminders increased the postpartum testing rate from the average of 33% up to 60%. Another study found that phone calls from nutritionists reminding patients to attend postpartum visits increased postpartum glucose test rates (36% vs. 17%) [29]. DIAMIND study of Australia found that a short message service reminder significantly increased the attendance for postpartum OGTT, and mothers preferred to receive electronic reminders, particularly text messages, sent by the study team or their clinicians [30, 31]. It was also shown to be effective for the Kaiser Permanente Northwest (KPNW) GDM Care to use electronic medical record data and an electronic system automated reminder call [32]. In our study, we used WeChat as a platform to manage the follow-up issues for GDM patients. With the high usage rate of the WeChat platform in China, almost all GDM women are likely to use it. Our questionnaire distributed via the WeChat platform showed that 94.9% of the GDM patients understood the necessity of postpartum OGTT screening, and 73.9% of those were screened for OGTT 4–12 weeks after delivery. The percentage of postpartum glucose screening in our study was much higher than the other Chinese study which showed that only 13.1% of GDM patients completed glucose screening after delivery [18].
Stepwise logistic regression analysis showed that only two parameters “GDM history” and “delivery mode (cesarean section)” were significant. Women with a previous history of GDM were less likely to complete postpartum OGTT than those who did not have GDM (OR: 3.74, 95% CI: 1.97–7.08), and women who had a cesarean section were more likely to return to the hospital to complete postpartum OGTT than those with a vaginal delivery (OR: 1.83, 95% CI:1.02–3.28). It has been suggested that enhancing education provided to women with a history of GDM may improve postpartum OGTT screening rates. Our results are similar to the findings recently published by Hunt et al. [33] who reported that women who failed to return for postpartum glucose testing were more likely to report prior GDM. However, in contrast to our results, the factors they identified as being associated with postpartum glucose testing were public insurance [19], older age, nulliparity, higher income or education [34], lower diagnostic glucose levels, and not requiring insulin during pregnancy [33]. Different ethnicities, and economic abilities of patients and inclusion criteria of studies may lead to differences in the findings.
The other principal finding in our study was that those who used insulin during pregnancy and those who had a cesarean section had a higher rate of abnormal postpartum OGTT results. This may be due to the fact that those who used insulin treatment during pregnancy or had a cesarean section had a higher glucose level during pregnancy, making it more difficult to return to normal glucose levels after delivery.
Our study did not use a control group to compare the rate of postpartum blood glucose screening with and without WeChat-based management. The source of nutrition advice provides limited information on the patient’s nutrition knowledge. In addition, due to the limitation of experimental samples, our conclusions may not comprehensively reflect all situations, and further expansion of the sample size is needed to promote the generalizability of the findings. All participants received questionnaires to ask whether they had completed their screening in the study. This part of the study could also further increase screening rates independently of the WeChat messaging, which may be a confounding factor. Follow-up via hospital records may avoid this issue. Despite the limitations, our study also has notable strengths.
Considering the close relationship between GDM and chronic diseases like T2DM, identifying and implementing interventions to decrease the incidence of associated health complications is a priority [6]. Previous study has shown that breastfeeding, postpartum healthy dietary intake and regular exercise can reduce progression to diabetes for women with a history of GDM [6]. In a 10 years follow-up observation, intensive lifestyle modifications along with the use of metformin were found to reduce progression to T2DM significantly [6]. Future studies should explore the utility of social medial platforms for enhancing nutrition knowledge and GDM management.
The WeChat messaging platform may be a useful tool to enhance postpartum OGTT screening among women with GDM. Women who failed to return for postpartum glucose screening (PGS) were more likely to report prior GDM than women who returned for PGS. Women who had postpartum IGR were more likely to use insulin treatment during pregnancy and more likely to deliver by cesarean section compared to women who had normal postpartum glucose results.
The data that support the findings of this study are available on request from the corresponding author Min Liu upon reasonable request.
Study concepts were prepared by ML and YFL. The study was designed by HL. Data acquisition was performed by HYP and CXC. Quality control of data and algorithms was carried out by MW and CMM. Data analysis and interpretation was conducted by GF and JRW. Statistical analysis was performed by HN and JYW. The manuscript was prepared and edited by HL. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Institutional Review Boards of the Third Xiangya Hospital, Central South University (No: 2020-S262).
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This work was supported by the Natural Science Foundation of Hunan Province (No. 2022JJ40749), the Project of Scientific Research Plan of Health Committee of Hunan Province (202203065334), and the Scientific Research Project of Hunan Provincial Health Commission (No. B2017032).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.