


 , Yinfen Wang 3,*
, Yinfen Wang 3,*
1 Maternal Health Care Department, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science & Technology, 430015 Wuhan, Hubei, China
2 Department of Obstetrics, Yuyao Maternity and Child Health Care Hospital, Yuyao Second People’s Hospital, 315402 Ningbo, Zhejiang, China
3 Department of Obstetrics, Ningbo Women and Children’s Hospital, 315012 Ningbo, Zhejiang, China
†These authors contributed equally.
Abstract
To determine the factors associated with successful external cephalic version (ECV) of breech presentation at term in China.
Pregnant patients who underwent ECV for a breech presentation at term from January 2020 to January 2023 were included in this retrospective observational study. From the candidate demographic and clinical factors a logistic regression model was employed to detect the predictors of ECV success. A receiver operating characteristic (ROC) curve was constructed to test the discriminative capacity of the final model.
The success rate of ECV in 207 pregnancies with a breech presentation at term was 68.6%. The rates of failed ECV after four to five attempts were 45/207 (21.7%), and suspected foetal hypoxia was present in 7 out of 207 (3.38%) babies. Three factors—an increased amniotic fluid index (AFI), the use of terbutaline and lower head circumference to femur length (HC/FL) ratio predicted the probability of a successful ECV. The area under the ROC curve (c-statistics) was 0.735 (95% confidence interval (CI) 0.649–0.800).
An increased AFI, use of terbutaline, and a lower HC/FL ratio were all associated with successful ECV and can be used to estimate the chances of ECV success. ECV for breech presentation is a safe procedure with a reasonable success rate which increases the likelihood of a vaginal birth.
Keywords
- external cephalic version
- breech presentation
- risk factors
- prediction model
The incidence of non-cephalic presentation in full-term pregnancies is 3–4% worldwide [1]. Due to a higher risk of foetal asphyxia and intrauterine accidents during delivery [2], more pregnant women with non-cephalic presentation choose caesarean section (CS). In China, the rate of CS in non-cephalic presentation is estimated to be 90% [3]. Although CS is relatively safe, there are growing concerns about infection, repeat procedures, and placenta accreta are leading to a preference for external cephalic version (ECV). ECV is a procedure where pressure is applied to a woman’s abdomen to achieve a vertex presentation via a controlled forward or backward rotation [4]. A successful ECV considerably elevates the chance of vaginal delivery.
ECV has been performed in Ningbo Women and Children’s Hospital since 2012. Initially, only a small number of patients opted for this procedure. As the preference for vaginal delivery increased, queries about the rate of ECV success and its related factors became more prevalent. The success of ECV is linked to several factors [5, 6], with the success rate ranging from 35 to 86% [7]. To improve data-driven shared decision-making in our hospital, we assessed the rate of successful ECV and developed a model to predict the probability of a successful ECV.
The Ethics Committee of Ningbo Women and Children’s Hospital approved (approval number: EC2030-050) our retrospective study, which was conducted in accordance with the Declaration of Helsinki. Data on maternal medical history and delivery outcomes were obtained from the hospital records. This study included all women who opted for ECV between January 2020 and January 2023. The inclusion criteria were singleton pregnancy and a non-cephalic presentation at 37–38 weeks gestation, scheduled for ECV. The exclusion criteria included the following: (a) preterm labour, oligohydramnios, rupture of membranes, severe foetal growth restriction, uterine malformation, prior abruption or prior caesarean delivery; (b) incomplete medical history and/or surgical records.
A successful ECV was defined as obtaining a cephalic presentation after the procedure, confirmed by ultrasonography. The primary outcome measured was successful ECV, and the secondary outcomes included assessing maternal and neonatal well-being, including emergency CS, admission to the Neonatal Intensive Care Unit (NICU), and Apgar score of 7 or less at 5 minutes after birth.
Before undergoing ECV, patients had to fast for six hours. They were given information about the option of having neuraxial anaesthesia (NA) for the procedure, and the advantages and disadvantages of undergoing ECV under NA. Participants were able to decide whether to choose or decline NA.
Experienced obstetricians conducted the ECV in operating rooms equipped with emergency CS facilities, real-time ultrasound guidance, and foetal heart rate monitors. Each patient received a 0.25 mg subcutaneous terbutaline injection and, if chosen, NA before undergoing a maximum of five attempts of ECV. Emergency CS was performed if foetal hypoxia was detected. Suspected fetal hypoxia refers to the likely occurrence of ongoing reduced oxygen supply to fetal tissues from analysis of cardiotocographic tracings, electrocardiography, or fetal blood sampling. If the foetus did not turn after four or five attempts, it was considered “not turning at all”. “Still breech presentation with ECV” was defined as the foetal position successfully turned to cephalic presentation after ECV but returning to the breech presentation before the onset of labour. After the procedure, the foetal heart rate was monitored continuously for 30 minutes to 2 hours, regardless of the outcome. Additionally, an ultrasound was performed to evaluate the foetal presentation. Rh-negative women with Rh-positive partners received Anti-D immunoglobulin. Once no further intervention was needed, these women were advised to continue routine antenatal care until delivery.
Independent t-tests were used to compare normally distributed continuous
variables (maternal age, body mass index (BMI) at ECV, gestational weeks during ECV, estimated foetal weight (EFW) during
ECV, head circumference to femur length (HC/FL) ratio, amniotic fluid index (AFI)). For categorical variables (parity, placental
implantation, loops of nuchal cord, use of tocolytics, neuraxial anaesthesia), the
Chi-square test was employed. Continuous variables were presented as mean
Between 2020 and 2023, 261 patients underwent attempts for ECV. However, 54 patients opted for CS and their data was excluded from this study. The remaining 207 women underwent ECV, among whom 142 (68.6%) women had a successful outcome, while 65 (31.4%) had a failed ECV and delivered by CS (Fig. 1).
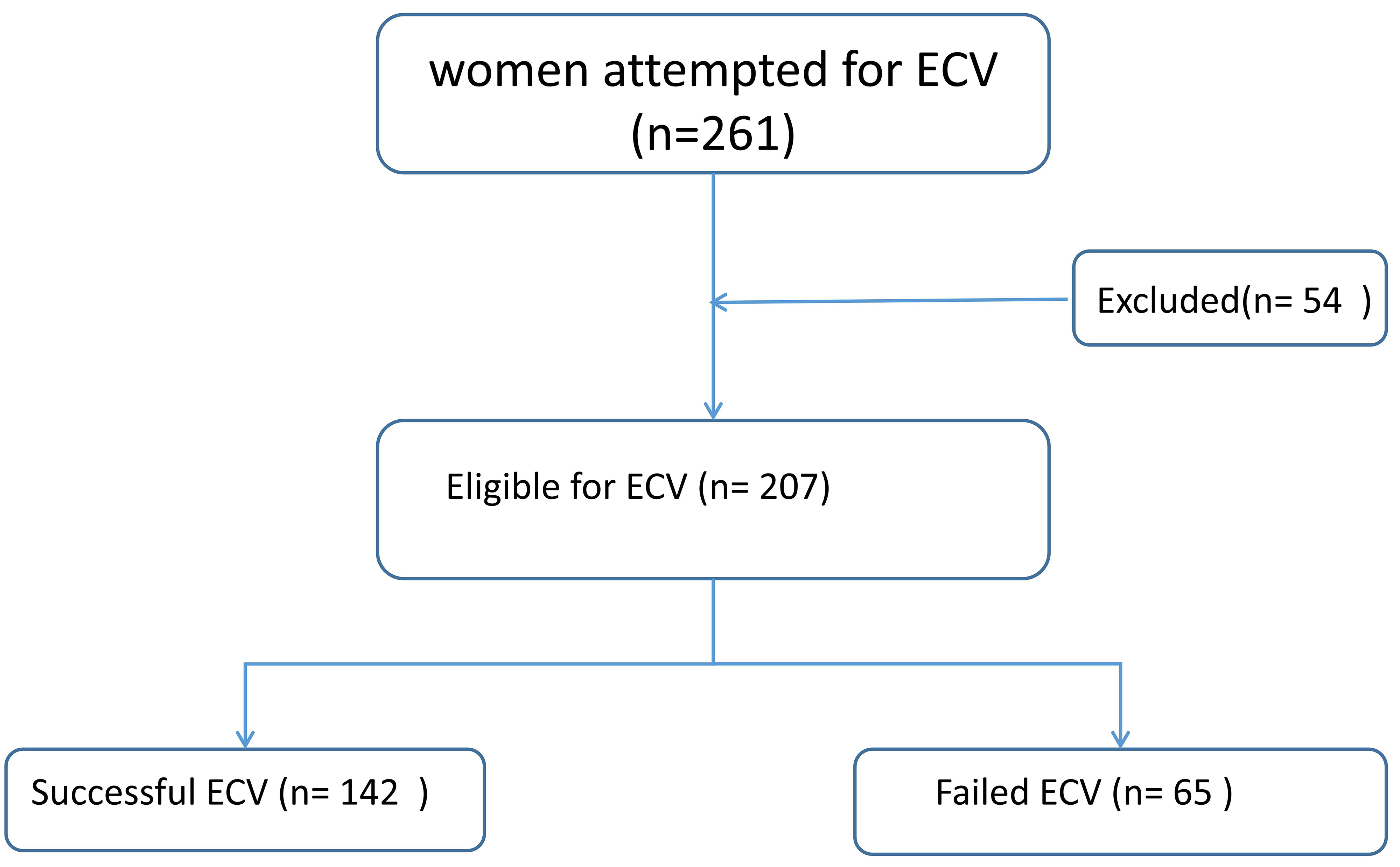 Fig. 1.
Fig. 1.
Flow chart of patient selection. ECV, external cephalic version.
The major reasons for failed ECV were the inability to turn the foetus after four to five attempts (45/207 cases, 21.74%), foetal stress with suspected foetal hypoxia (7/207, 3.38%), placental abruption (6/207, 2.90%), continued breech presentation following ECV (6/207 cases, 2.90%) and cord prolapse (1/207, 0.48%) (Table 1).
| Reasons | Number of cases | % (N = 207) |
| Failed ECV not turning at all | 45 | 21.74 |
| Suspected foetal hypoxia | 7 | 3.38 |
| Placental abruption | 6 | 2.90 |
| Continued breech presentation | 6 | 2.90 |
| Cord prolapse | 1 | 0.48 |
The demographic and clinical characteristics of all participants are shown in Table 2. The HC/FL ratio was significantly higher in the ECV failure group than in the success group (p = 0.008). Additionally, the amniotic fluid index and the use of tocolytics were significantly lower in the ECV failure group than in the success group (p = 0.006 and p = 0.001). There was no statistically significant difference in age, body mass index at ECV, parity, gestational weeks, placental implantation, loops of nuchal cord, neuraxial anaesthesia and EFW during ECV between the two groups.
| Characteristics | Successful group | Failed group | p value | |
| (n = 142) | (n = 65) | |||
| Maternal age (years) | 31.12 |
30.58 |
0.379 | |
| BMI at ECV (kg/m2) | 25.83 |
26.04 |
0.660 | |
| Parity, n (%) | 0.391 | |||
| Nulliparous | 63 (44.4%) | 33 (50.8%) | ||
| Multiparity | 79 (55.6%) | 32 (49.2%) | ||
| Gestational weeks during ECV (weeks) | 37.90 |
37.83 |
0.581 | |
| EFW during ECV (kg) | 3.09 |
3.06 |
0.532 | |
| HC/FL ratio | 4.79 |
4.88 |
0.008 | |
| Placental implantation, n (%) | 0.392 | |||
| Anterior | 55 (38.7%) | 25 (38.5%) | ||
| Posterior | 74 (52.1%) | 30 (46.2%) | ||
| Lateral or Fundal | 13 (9.2%) | 10 (15.4%) | ||
| AFI (cm) | 12.5 |
11.0 |
0.006 | |
| Loops of nuchal cord (yes), n (%) | 57 (40.1%) | 22 (33.8%) | 0.387 | |
| Use of tocolytics (yes), n (%) | 126 (88.7%) | 45 (69.2%) | 0.001 | |
| Neuraxial anaesthesia (yes), n (%) | 33 (23.2%) | 19 (29.2%) | 0.356 | |
Data in the table are presented as n (%), and mean
The results of a multivariable logistic regression analysis showed that the level of AFI (odds ratio (OR) = 1.107, 95% confidence interval (CI): 1.006–1.029, p = 0.0033) and the use of terbutaline were positively associated with ECV success (OR = 2.612, 95% CI: 1.183–5.769, p = 0.0153). In contrast, the HC/FL ratio (OR = 0.125, 95% CI: 0.017–0.551, p = 0.0114) was negatively associated with ECV success (Table 3).
| Characteristics | Univariable logistics analysis | Multivariable logistics analysis | |||||
| OR | 95% CI | p value | OR | 95% CI | p value | ||
| Maternal age (years) | 0.585 | –1.732 to 0.662 | 0.839 | ||||
| BMI at ECV (kg/m2) | 1.229 | 0.718 to 1.132 | 0.680 | ||||
| Parity, n (%) | |||||||
| Nulliparous | Ref | Ref | |||||
| Multiparity | 0.938 | 0.212 to 0.084 | 0.939 | ||||
| Gestational weeks during ECV (weeks) | 0.934 | –0.318 to –0.179 | 0.511 | ||||
| EFM during ECV (kg) | 0 | –134.1 to –55.2 | 0.681 | ||||
| HC/FL ratio | 1.086 | 0.016 to 0.148 | 0.0164* | 0.125 | 0.017–0.551 | 0.0114 | |
| Placental implantation, n (%) | |||||||
| Anterior | Ref | Ref | |||||
| Posterior | 0.967 | 0.475 to 1.971 | 0.927 | ||||
| Lateral or Fundal | 0.525 | 0.186 to 1.480 | 0.223 | ||||
| AFI (cm) | 1.016 | 1.03 to 1.029 | 0.0087* | 1.017 | 1.006–1.029 | 0.0033 | |
| Loops of nuchal cord (yes), n (%) | 0.939 | –0.207 to 0.081 | 0.381 | ||||
| Use of tocolytics (yes), n (%) | 2.606 | 1.097 to 6.188 | 0.0086* | 2.612 | 1.183–5.769 | 0.0153 | |
| Neuraxial anaesthesia (yes), n (%) | 1.061 | –0.069 to 0.188 | 0.557 | ||||
Notes: * p
Developing predictive models based on the results of multivariate analysis, which included the HC/FL ratio, AFI, and the use of tocolytics, evaluating the model fit with relevant tests; and use ROC curve analysis to determine the predictive accuracy of the model. The area under the ROC curve (c-statistics) is 0.735 (95% CI: 0.649–0.800), indicating a good discriminative ability of the model (Fig. 2).
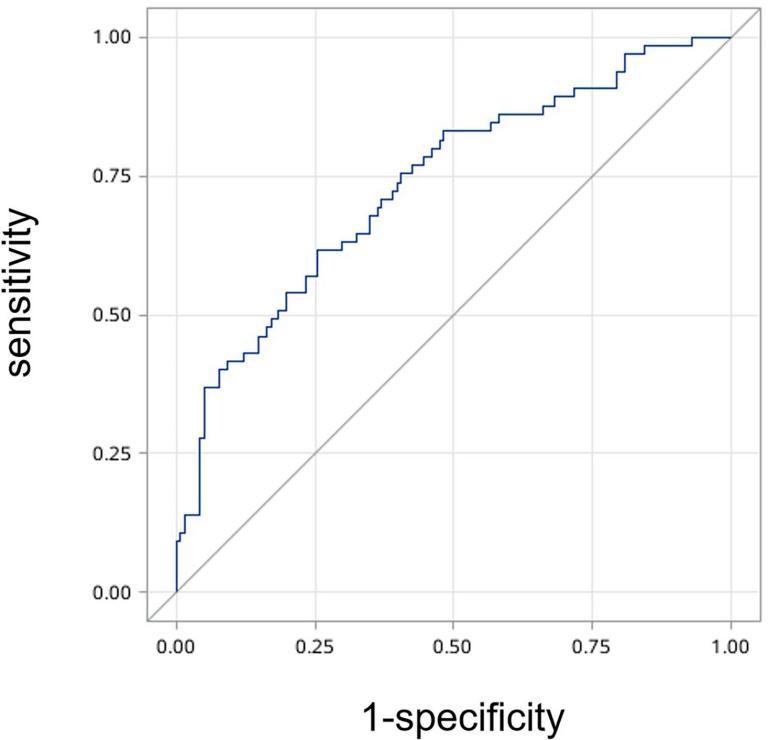 Fig. 2.
Fig. 2.
Receiver operating characteristic (ROC) curve of the ECV outcome prediction model.
We conducted a retrospective study to identify the factors associated with the outcome of ECV. The success rate of ECV in this study was 68.6%. The independent determinants of the outcome were AFI, use of terbutaline, and ratio of HC/FL. The other variables examined in the study, including age, body mass index at ECV, parity, gestational weeks, placental implantation, loops of nuchal cord, neuraxial anaesthesia and EFW, did not show statistically significant association with the success rate of ECV.
The existing literature reports the success rate of ECV to be between 30% and 70%, with an average of 53%, which is consistent with our study [5, 6]. The primary cause of an unsuccessful ECV is the foetus failing to turn despite four to five attempts. Although two experienced physicians conducted the procedure and the maternal position aligned with the operation, the difficulty in assessing the palpation of the foetal head and the engagement of the foetus in the maternal pelvis, can affect ECV outcome. Even if the first attempt at ECV was unsuccessful, if the woman strongly desired a vaginal delivery, a second attempt could be made under NA. Although anaesthesia was used to facilitate ECV in the current study, concerns related to its use, as well as potential issues such as abnormal bleeding and hypotension, remain significant and warrant further discussion. Emergency CS is a serious complication of ECV [11]. The incidence of emergency CS in our present study was 6.25% (13/207), which was higher compared to the 1.0 to 4.2% range reported in other studies [12, 13]. The common reason for emergency CS was suspected foetal hypoxia during ECV [14]. It is noteworthy that a case of cord prolapse occurred eight hours after successful ECV, suggesting the importance of continuous monitoring in cases of premature rupture of membranes.
In this study, a higher level of amniotic fluid index was positively associated with successful ECV. Similar studies conducted in Germany and Australia also demonstrated that AFI was independently associated with the outcome of ECV [15, 16], with the optimal cut-off value being 12.3 cm (Table 3). One of the strengths in our study was the inclusion of women with an AFI below 8 cm (14/207). This inclusion is noteworthy, as some studies have refrained from performing ECV in patients with an AFI below 8 cm [17], while other obstetricians have set a threshold of AFI below 10 cm [18]. Remarkably, our study involved six patients with successful ECV with AFI ranging from 5–8 cm, along with eight patients experiencing failed ECV within the same AFI range. This result suggests the need for a future replication study across multiple sites, focusing on cases with AFI ranging from 5–8 cm.
In this study, the HC/FL ratio was inversely related to successful ECV. This ratio was obtained from patient characteristics, aligning with the results of De Castro’s study [19] and it can reduce measurement errors from different sonographers. Contrary to our findings, other studies have reported diverse results, suggesting the lack of HC association with ECV success [20, 21]. This discrepancy could stem from the ongoing debate regarding the accuracy of B-ultrasound in evaluating HC [22, 23]. Based on our study, there appears to be an increased probability of ECV failure in pregnant patients with higher HC/FL ratios.
The use of terbutaline also showed a positive association with the success of ECV, consistent with the results of a randomised controlled study on terbutaline [24]. Other studies support the use of terbutaline to improve the chances of successful ECV. However, data were insufficient to analyse the adverse effects of terbutaline [25, 26]. Thus, there is a pressing need for a randomised controlled trial with a larger sample size.
Several strengths are evident in this study. The considered variables were all objective, easily available, and clearly defined, contrasting with factors dependent on more subjective markers such as possibility of palpation of the foetal head. Our principle was that if women opted for ECV, we would attempt it, even when the AFI was below 5 cm. In the initial phases of implementing the procedure, both uterine tocolytics and neuraxial analgesia were employed. However, with the advancement of technology and the refinement of emergency caesarean delivery procedures, only uterine tocolysis is now frequently employed. Neuraxial analgesia has since been discontinued and only uterine tocolytics was used, owing to technological advances and the refinements of emergency CS.
The study presents several limitations. Firstly, for patients with failed ECV, no further ECV was attempted. Secondly, as this is a single-site study, further multi-site randomised controlled trials are warranted. Lastly, although this study addressed some confounding factors, certain important variables have not been incorporated, which could compromise the validity of the results. Therefore, further investigations involving diverse populations are necessary to substantiate our findings.
Our study adds to the limited evidence that higher AFI, use of terbutaline, and lower ratio of HC/FL are all associated with successful ECV and can be used to estimate the success of the procedure. ECV for breech presentation is a safe procedure with a favourable success rate, increasing the likelihood of vaginal births thereby offering a viable alternative to surgical delivery in suitable cases. We recommend that our findings be confirmed in larger samples, including patients from different institutions.
The datasets used and/or analysed in this study are available upon request from the corresponding author.
ZRD and XYZ: Data collection, manuscript writing and data analysis; AEC and XBH collected data and processed the data, participated in the writing of the corresponding results section, and plotted Tables 1,2. XBH performed statistical analysis. YFW designed the research study, revised the language of the first draft and checked and revised the overall content and data, defines and categorizes ultrasound data and participates in the writing of ultrasound-related sections in the Materials and Methods section. All the authors reviewed and approved the final version of the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Ningbo Women and Children’s Hospital (approval number: EC2030-050). All data were collected from the electronic medical record system in the department of Obstetrics. Data were anonymised and de-identified before analysis. Since this is a retrospective study, informed consent could not be obtained from the patients or their families/legal guardians. With the approval of the approval agency, informed consent was waived.
We would like to express our gratitude to all those who assisted in the writing of this manuscript. We extend our thanks to all the peer reviewers for their valuable opinions and suggestions.
This study was supported by Medical Science and Technology Project of Zhejiang Province, China (2022KY1162 and 2021YZD02) and funded by the project of NINGBO Leading Medical & Health Discipline (2010-S04 and 2023Z183).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.