



 , Wassan Nori 1,*
, Wassan Nori 1,* , Dina Akeel Salman 1, Abdulkareem H. Issa 2, Wisam Akram 1
, Dina Akeel Salman 1, Abdulkareem H. Issa 2, Wisam Akram 11 College of Medicine/Department of Obstetrics and Gynecology, Mustansiriyah University, 10052 Baghdad, Iraq
2 College of Medicine/Chemistry and Biochemistry Department, Mustansiriyah University, 10052 Baghdad, Iraq
Abstract
Gestational diabetes mellitus (GDM) is one of the most prominent diseases seen in pregnancy that adversely affects materno-fetal welfare. It is usually screened by an oral glucose tolerance test (GTT), which has some limitations. Adiponectin and triglyceride-glycemic (TyG) index were two biomarkers examined in the GDM context with inconclusive effectiveness. This study aimed to examine both markers' performance in screening for GDM among Iraqi women.
An observational cross-sectional study recruited gestational age and body mass index (BMI) matched pregnant at 26–28 weeks into two groups: healthy controls (n = 44/88) and GDM cases (n = 44/88). Participants' demographics, biochemical [FBS (fasting blood sugar), 2hr_GTT (2-hour glucose tolerance test), HDL (high-density lipoprotein), LDL (low-density lipoprotein), total cholesterol, TG (triglyceride), and TyG index], and hormonal (adiponectin) were recorded.
Serum adiponectin was significantly higher among healthy pregnant (8.44 ± 1.12 ng/mL vs. 5.28 ± 0.89 ng/mL); p < 0.0001. In contrast, the TyG index was significantly higher among GDM cases (4.02 ± 0.04 vs. 3.96 ± 0.02; p < 0.0001). Adiponectin showed strong inverse links with FBS, 2hr_GTT with r = (–0.76, –0.80); p < 0.0001, respectively. TyG index was moderately, inversely, and significantly linked to serum adiponectin as r = –0.58; p < 0.0001. Adiponectin and TyG index reliably predicted GDM with a high area under the curve of 0.83 vs. 0.88; p < 0.001, respectively.
Both biomarkers correlated well to GDM parameters and showed high sensitivity and specificity in screening for GDM. Their efficiency, easy integrations in practice, and promising therapeutic application suggested by researchers warrant further studies.
Keywords
- adiponectin
- gestational diabetes mellitus
- screening
- triglyceride-glycemic index
During the last decade, the incidence of gestational diabetes mellitus (GDM) has
witnessed a global increase from 10 to 26 percent, possibly due to the increase
in maternal obesity and maternal age at conception [1]. GDM occurs when insulin
resistance is diagnosed for the first time during pregnancy, mostly during 24–28
weeks of gestation [2]. Although the reason that triggers its development is
poorly understood, there is a consensus that dysfunction of
Currently, the gold standard for establishing a GDM diagnosis is the 75 g oral glucose tolerance test (GTT) [8]. The test has good predictive value, allowing for risk stratification for screened cases. However, it requires multiple blood draws, which makes it time-consuming and stressful for the mothers and thus reduces its acceptability [9, 10]. Some researchers have criticized the test, suggesting that feto-maternal harm is already done by the time of the diagnosis [11]. An urgent need arises for earlier, reliable, and comprehensive screening bio-markers for GDM. Adiponectin is a hormone manufactured by adipose cells; it exhibits anti-inflammation and anti-atherogenic and insulin sensitization properties [12, 13]. Physiologically, adiponectin regulates fat metabolism, and it improves overall insulin sensitivity. Reduced maternal levels suggest increased GDM risk among screened moms as it mirrors glucose intolerance before it clinically manifested [14]. The triglyceride-glycemic (TyG) index is an innovative instrument to estimate insulin resistance (IR), especially among obese individuals and adolescents [15]. The TyG index has been tested in Korean and Brazilian studies and showed promising results [16, 17]. Interestingly, it is accessible in many clinics and has outperformed the Homeostatic Model Assessment of Insulin Resistance in estimating IR. Recently, the TyG index was tested as a potential GDM screening marker; however, the recommendations regarding its performance were inconclusive [16, 17, 18].
This study was designed to examine the performance of maternal adiponectin and the TyG index in screening for GDM among Iraqi women for a more effective and cost-benefit analysis.
Pregnant women attending the National Diabetes Center and Al-Yarmouk Teaching Hospital were invited to enroll in the current case-control study. The enrollment took place over eight months, from 1/8/2021 to 1/4/2022. Pregnant attending consultation clinics eligible for inclusion were invited; verbal and signed consent was obtained before inclusion into the study. Scientific Counsel of Obstetrics and Gynecology/College of Medicine; Mustansiriyah University issued study approval; NO.18 dated 25/2/2021. Enrollment was made to 95 pregnant at a gestational age ranging from (24 to 28 weeks) of pregnancy, with high suspicion of having GDM (high-risk group). They were screened using an oral glucose tolerance test (GTT), which was performed after these directives were made before the test:
Samples were obtained from venous plasma to measure fasting blood glucose level and 2 hours following the administration of 75 grams of glucose dissolved in 300 mL of water. GDM was confirmed based on National Institute for Health and Care Excellence (NICE) Guidelines, including [19]:
Seven pregnant could not tolerate performing the test, so they were excluded from the study. Cases with a confirmed GDM diagnosis as per NICE Guideline [19] were taken as the study group 44/88, while those with no GDM were taken as the healthy controls 44/88; both groups were matched regarding their gestational age body mass index (BMI), and all included cases were native Iraqi females to standardize the study participants; study flow chart Fig. 1.
Inclusion criteria:
Exclusion criteria:
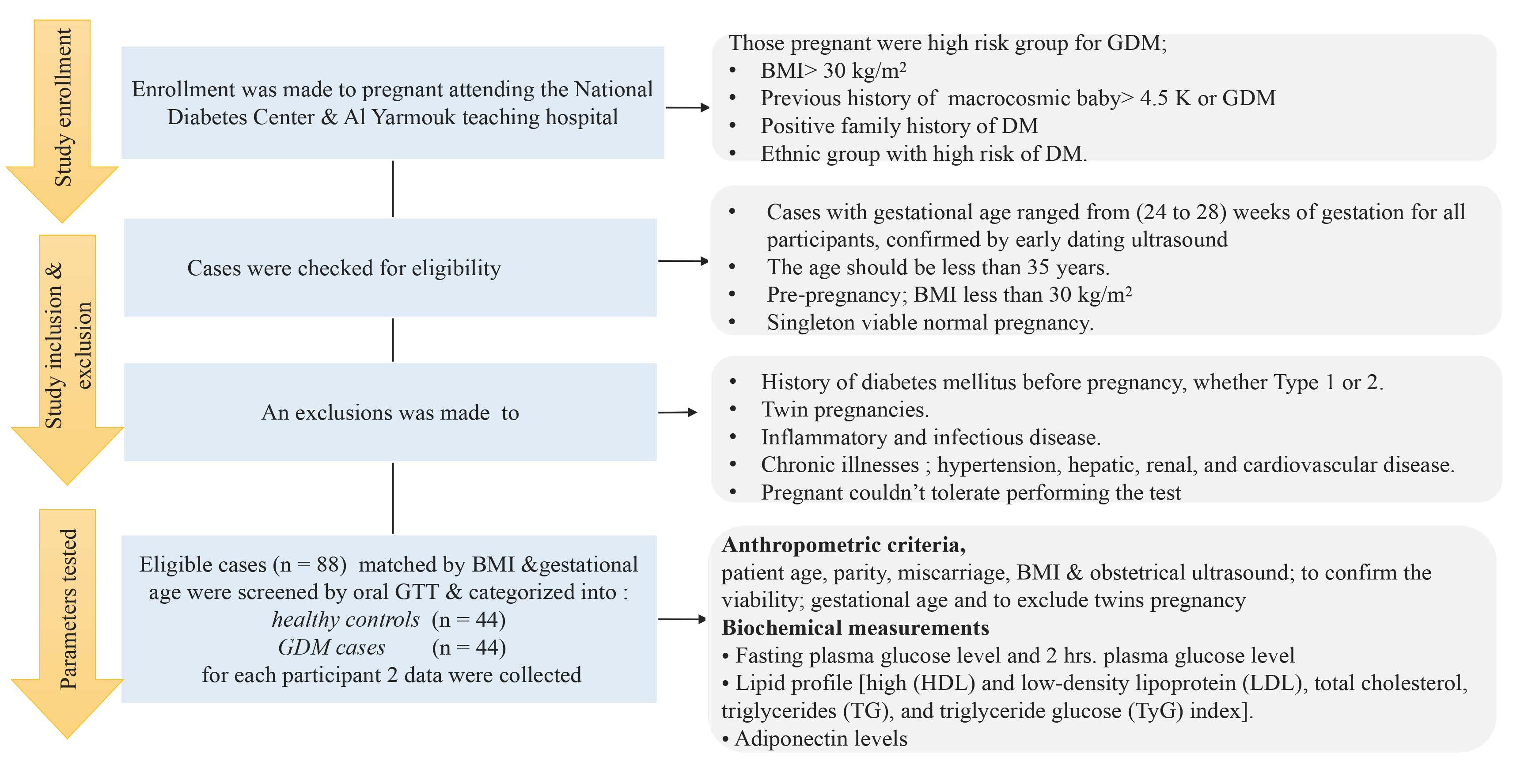 Fig. 1.
Fig. 1.
The study flowchart. BMI, body mass index; GTT, glucose tolerance test; GDM, gestational diabetes mellitus; DM, diabetes mellitus.
The anthropometric criteria including patient age, parity, miscarriage, BMI measurements, and obstetrical ultrasound.
The height and weight (pre-pregnancy weight) were measured to calculate BMI by the following formula: BMI = body weight (kg)/height (m2). An obstetrical ultrasound was done via transabdominal route for all women with a 3–5 MHz transabdominal probe using a PHILIPS HD11 XE (Philips, Tokyo, Japan) to confirm the viability and the gestational age and to exclude multiple pregnancies.
For the biochemical parameters, 5 mL venous blood samples were obtained from the participants after an overnight fast (12 hours). Blood samples were centrifuged, and serum samples were stored at –20 °C until the assay. The HDL, LDL, cholesterol, and TG concentrations were measured by auto analyzer using the colorimetric method. The TyG index was estimated using the following formula [20]:
Ln [fasting triglycerides (mg/dL)
Ln: natural logarithm; fasting triglycerides and fasting blood glucose were calculated following fasting.
Serum adiponectin concentrations were measured using the enzyme-linked immunosorbent assay (ELISA) method kit Cat (No YHBO111HU, Shanghai Biological, Shanghai, China), according to the manufacturer’s instructions, using the quantitative sandwich enzyme immunoassay technique.
The formula for calculating the sampling power for a two-sample comparison of means is [21]:
N =
N =
N = [1.96 + 0.84]2
The data normality was checked by the D’Agostino-Pearson test. The data were
expressed as means and standard deviation (
The basic criteria of the study were showed in Table 1. The maternal age were
statistically higher among cases p = 0.001; while all other parameters
were statistically insignificant (miscarriage, parity , BMI , and gestational
age) as p
| Parameter | Healthy controls (N = 44) | GDM cases (N = 44) | p-value |
| Demographic criteria | |||
| Maternal age (years) | 28.73 |
29.98 |
0.001 |
| Miscarriage ‡ | 0.00 (0.00–1.00) | 1.00 (0.00–1.00) | 0.052 |
| Parity | 3.27 |
2.97 |
0.224 |
| BMI (kg/m2) | 26.42 |
26.73 |
0.105 |
| Gestational age (weeks) | 26.81 |
26.67 |
0.774 |
| Biochemical parameters | |||
| FBS (mg/dL) | 80.23 |
97.18 |
|
| 2hr_GTT (mg/dL) | 111.95 |
145.16 |
|
| LDL (mg/dL) | 114.29 |
113.62 |
0.52 |
| HDL (mg/dL) | 67.235 |
55.39 |
|
| Total cholesterol (mg/dL) | 211.39 |
268.49 |
|
| TG (mg/dL) | 215.24 |
227.74 |
0.0007 |
| TyG index | 3.96 |
4.02 |
|
| Adiponectin (ng/mL) | 8.44 |
5.28 |
|
‡ The analysis was made by was made by Mann-Whitney test for non-parametric data. The rest parameters were normally distributed and analyzed by t-test. FBS, fasting blood sugar; 2hr_GTT, 2-hour glucose tolerance test; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglyceride; TyG index, triglyceride-glycemic index; BMI, body mass index.
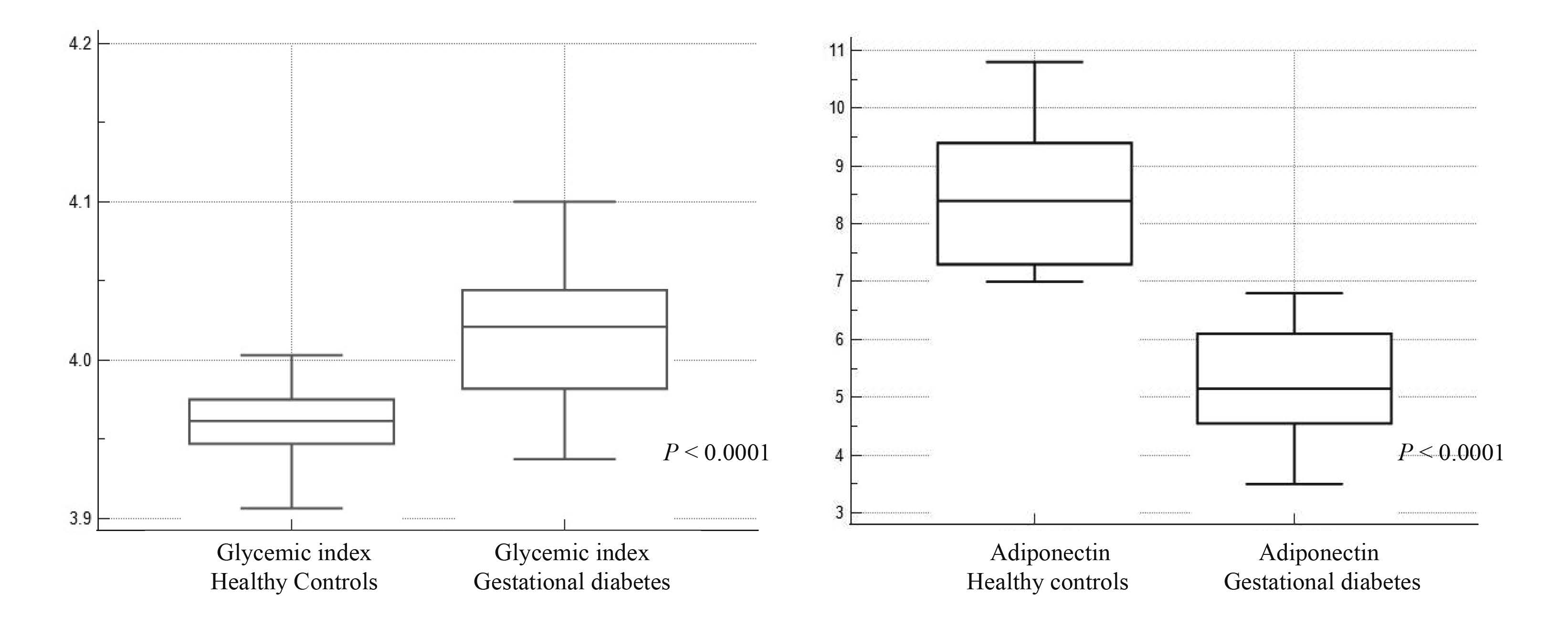 Fig. 2.
Fig. 2.
Box and whisker chart for serum adiponectin and TyG index among healthy pregnant vs. GDM case. TyG index, triglyceride-glycemic index.
Table 2 describes the Pearson correlation between serum adiponectin vs.
some of the study parameters. A strong inverse correlation was proved with fasting blood sugar (FBS), 2-hour glucose tolerance test (2hr_GTT) with r = (–0.76, –0.80); p
| Variable | Correlation coefficient (r) | 95% Confidence interval | p-value |
| FBS | –0.76 | –0.84 to –0.66 | |
| 2hr_GTT | –0.80 | –0.87 to –0.72 | |
| TyG index | –0.58 | –0.70 to –0.42 |
FBS, fasting blood sugar; 2hr_GTT, 2-hour glucose tolerance test; TyG index, triglyceride-glycemic index.
The ROC curve determined the validity of both markers, serum adiponectin and TyG index, in screening for GDM, shown in Fig. 3.
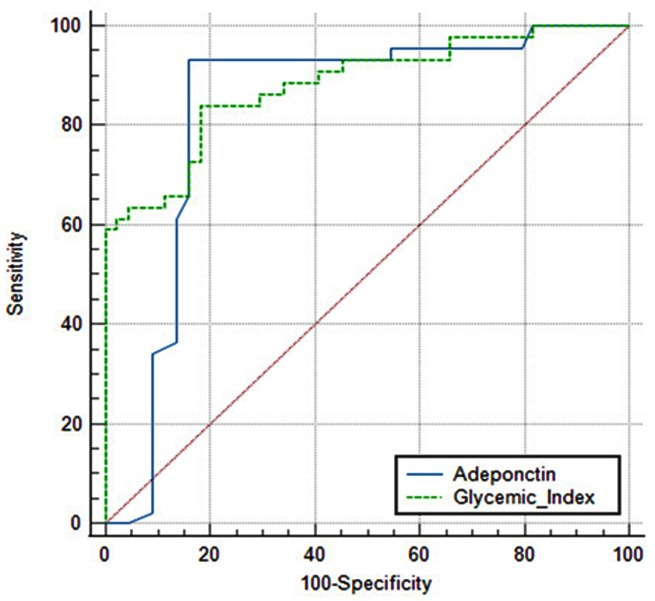 Fig. 3.
Fig. 3.
The ROC curve showing adiponectin and TyG index cut-off value in discriminating GDM cases. ROC, receiver operator characteristic curve.
In Table 3, a pairwise comparison was shown between adiponectin and TyG index
with respect to their respective cut-off values, 95% CI, standard error (SE),
sensitivity, specificity, and significant level among the two markers. It was
shown that both adiponectin and TyG index reliably predicted GDM with a high area
under the curve (AUC) of 0.83 vs. 0.88; p
| Variable | Adiponectin | TyG index | Pairwise comparison |
| Cut-off value | – | ||
| AUC | 0.83 | 0.88 | 0.048 |
| 95% CI | 0.74 to 0.91 | 0.80 to 0.94 | –0.079 to 0.176 |
| Sensitivity | 93.2% | 84.1% | Z statistics 0.73 |
| Specificity | 84.1% | 81.8% | |
| Significant level | p |
p |
0.46 |
AUC, area under the curve; CI, confidence interval.
The analysis confirmed reduced levels of serum adiponectin among cases with GDM. It was significantly and inversely linked to FBS and 2hr_GTT. In line with our results, Gao et al.’s [22] meta-analysis showed an inverse relationship between adiponectin and GDM risk; their study confirmed significantly lower levels among pregnant mothers with GDM vs. mothers with normoglycemic pregnancies. They recommended it as a screening biomarker for GDM. In agreement with our analysis, Bao et al. [23] discussed lower levels of GDM among women in the first and second trimesters.
Hedderson et al. [24] study examined an interesting role of
adiponectin; they linked pre-pregnancy adiponectin with the subsequent risk of
developing GDM, which can be used in practice as a risk stratification tool to
spot high-risk women for GDM before they get pregnant. In accordance with
Hedderson et al. [24], Iliodromiti et al. [25] meta-analysis
confirmed adiponectin prediction for GDM before and at early pregnancy, with a
diagnostic odds ratio of 6.4 and 95% CI of 4.1 to 9.9. Adiponectin levels were
lower in the placenta of affected rodents, underscoring its role in placenta
development. Moreover, adiponectin receptor-2 and not 1 was significantly lower,
which may be the way by which the marker exhibits its effect [26]. The current
study showed a good prediction power for serum adiponectin at high sensitivity
and specificity (93.2%, 84.1%); p
Rodent’s study signified the therapeutic value of adding Adiponectin to diabetic
rates, leading to better glucose levels and protecting against fatty liver [27].
While animal study recommend the therapeutic potential of adiponectin
administration, its role in humans, especially among pregnant women, is yet to be
confirmed [28]. Some suggested its administration to women in the post-natal
periods to reduce their progression risk from GDM into frank type 2 diabetes
(T2D) [12, 29]. Adiponectin is an adipokine secreted by fatty cells and has a key
role in glucose and lipid metabolism. Reduced levels were linked to higher IR and
T2D. Lower levels in pregnancy underscore the metabolic imbalance that defines
GDM [30]. This was confirmed in the current study by a strong statistically
significant correlation of adiponectin to FBS and 2hr_GTT (–0.76, –0.80),
p
The current results showed a significantly high TyG index among GDM cases
p
In accordance with our results, Liu et al. [18] examined the
performance of the TyG index in screening for IR among pregnant women. Their
result highlighted significant differences in the TyG index levels in GDM cases
(4-fold rise) vs. healthy pregnant. They further highlight that the
second trimester was the best time for performing screening by the TyG index,
which can be a promising tool for GDM prediction [18]. Sánchez-García
et al. [31] examined the diagnostic performance of the TyG index
compared to a 2-hour 75-g oral glucose tolerance test in screening for GDM in a
comparative study at 24–28 weeks. They also examined their correlations with
materno-fetal outcomes. TyG index was significantly high among GDM cases,
p
Higher levels of TyG index among GDM cases and its reliability in the prediction
of GDM were discussed by many scientists. Salvatori et al. [32]
conducted a cohort study for women to see the best association between TyG index
and 2 h-75 g oral GTT-derived insulin sensitivity. With the use of machine
learning, the data they recruited on 2-visits, early in pregnancy and at
twenty-sixth weeks, were analyzed. Their result showed a weak positive
association between 2 h-75 g oral GTT and the conventional TyG index. They
proposed a newer improved ratio called TyGIS (the linear function of TyG, body
weight, lean body mass percentage, and fasting insulin), which yielded a much
more efficient ratio in screening for GDM as p
Interestingly, the TyG index served as a prognostic factor for cardiovascular accidents (CVSA) among T2D cases. Long monitoring of the ratio helped stratify the CVSA risk among the following cases and independently predicted the occurrence of those events [35]. The rationale behind the TyG index association with GDM is that the IR, a defining feature of GDM, is correlated with abnormal lipid metabolism, like high TG concentrations. Once IR rises, it damps insulin’s inhibitory effect on liver neogenesis and the peripheral uptake of glucose, leading to hyperglycemia. The high IR increases lipolysis and thus elevates blood lipids, i.e., TG.
Currently, screening for GDM is via oral GTT, the gold standard. However, the
test is time-consuming and sometimes inconvenient for pregnant women. Since the
test takes place in a single session, it offers a limited snip of the dynamic
changes in blood glucose. Not to mention that factors such as stress and physical
activity may trigger some variability in oral GTT test results [11]. The makers
used (adiponectin and TyG index) can be calculated in single blood aspiration,
and the result mirrors a broader picture of blood glucose and lipid metabolism,
allowing a holistic assessment of metabolic health. Not to mention that changes
in the 2-markers under the study occur earlier than oral GTT, which gives time
for intervention [36]. The ROC showed that adiponectin and TyG index reliably
predicted GDM with high AUC 0.83 vs. 0.88; p
(1) By passing oral GTT limitations [9, 10].
(2) Earlier detection for GDM [11].
(3) The analysis confirmed their efficacy for screening with the advantage of less patient burden.
Finding newer biomarkers may improve patients’ identification, especially those that may benefit from robust monitoring and lifestyle changes. This approach will optimize care and align with evidence-based, patient-centered holistic health care.
A multicentric will perform better. The cross-sectional study design adds limitations where the cause and effect cannot be ascertained. Since earlier studies suggested therapeutic and prognostic roles, it would be interesting to see the impact of both markers on feto-maternal outcomes, so we recommend a longitudinal study [14, 15, 17]. As a new marker, the TyG index for GDM screening is an area of research; its overall performance and off values for different ages and settings must be fully established. The therapeutic avenue for adiponectin in pregnant women must be validated in human studies.
The study comprehensively assessed 2-makers and their correlation to the standard screening for GDM in our hospital, a tertiary center with many referral cases, so we believe that diversity was achieved. Both markers performed well in screening for GDM with high sensitivity and specificity, adding to their feasibility and affordability for GDM screening. Confounder that usually hinders study results were addressed by matching gestational age and BMI in addition to the directives done prior to oral GTT. Adherence to that methodological recommendation will improve the reliability of the reached results and validate their efficiency in the screened population [36, 37, 38, 39]. Further research is warranted to explore more clinical applications in practice.
Many biomarkers for GDM are tested in practice; the markers’ affordability, availability, and accuracy are crucial for their implantation in practice. Adiponectin and TyG index performed well in screening for GDM among Iraqi females. They were comparable in performance, and no significant difference appeared upon comparison. Their reliability opens the door for earlier diagnostic and promising therapeutic applications in GDM.
FBS, fasting blood sugar; 2hr_GTT, 2-hour glucose tolerance test; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglyceride; TyG index, triglyceride-glycemic index; BMI, body mass index; HOMA-IR, Homeostatic Model Assessment for Insulin Resistance; IR, insulin resistance; ROC, receiver operator characteristic curve; AUC, area under the curve.
The data supporting this study is available on reasonable request from the corresponding author.
Conceptualization: HAGA and AHI; methodology: WN and DAS; software: WA; investigations and data curation: HAGA and AHI; writing, reviewing and editing: WN and HAGA; drafting and supervision: WN. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board. The scientific and ethical committees at the College of Medicine/Mustansiriyah University approved its protocol (IRB NO.18 dated 25/2/2021). Informed consent was obtained from all subjects involved in the study.
To our beloved university for continued support.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.