

1 Department of Gynecology, The Second Affiliated Hospital of Fujian Medical University, 362000 Quanzhou, Fujian, China
Abstract
This study aimed to evaluate the clinical efficacy and prognostic factors associated with McDonald cervical cerclage in pregnant women with cervical incompetence.
We retrospectively reviewed medical records of 100 pregnant women with cervical incompetence who underwent prophylactic or therapeutic McDonald cervical cerclage between January 2021 and December 2022. The participants were divided into two groups: good prognosis (n = 37) and poor prognosis (n = 63). Baseline characteristics and pregnancy outcomes were compared between the two groups, and multivariate logistic regression was used to identify associated prognostic factors.
The good prognosis group showed lower rates of miscarriage and preterm birth and higher rates of full-term birth compared to the poor prognosis group, but these differences were not statistically significant. Multivariate logistic regression identified various independent risk factors influencing clinical outcomes of McDonald cerclage, including gravidity (odds ratio [OR] = 1.75), having more than two previous births (OR = 2.44), assisted reproductive technology (OR = 1.52), history of cervical conization (OR = 1.88), complete uterine cavity curettage (OR = 1.67), prolonged second stage of labor (OR = 2.19), cesarean section (OR = 1.48), cervical laceration (OR = 1.80), polycystic ovarian syndrome (OR = 1.60), and prophylactic cerclage (OR = 0.73). These factors demonstrated good predictive performance for the prognosis of patients with cervical incompetence, with an area under the curve of 0.793 and sensitivity and specificity values of 0.750 and 0.850, respectively.
The identified risk factors, particularly having more than two previous births, prolonged second stage of labor, and a history of cervical conization, should be considered in the clinical management of pregnant women with cervical incompetence. The protective effect of prophylactic cerclage emphasizes the importance of early detection and timely intervention to improve pregnancy outcomes.
Keywords
- cervical incompetence
- McDonald cervical cerclage
- prognosis
- clinical efficacy
- pregnant women
Cervical incompetence, also termed cervical laxity, is a common gynecological condition and a leading cause of premature birth or miscarriage in the second trimester [1]. It refers to the pathological dilation and relaxation of the cervix that results from abnormalities in the morphology, structure, and function of the internal cervix orifice under a non-labor state, leading to the failure of the uterine cervix to maintain pregnancy to term [2]. Clinically, cervical incompetence is characterized by painless cervical dilation and/or shortening in the absence of contractions, leading to amniotic sac prolapse, membrane rupture, late-term miscarriage, or preterm delivery [3]. The causes of cervical incompetence are generally divided into congenital and acquired factors. Congenital causes include cervical dysplasia, partial uterine dysplasia, and connective tissue disorders, such as Ehlers-Danlos syndrome, which result in structural defects or dysfunction in cervical tissue, reducing its load-bearing capacity. Acquired causes primarily include cervical physical injuries, such as multiple uterine procedures, or drug exposure, like diethylstilbestrol, which can weaken or damage uterine cervical tissue, leading to pathological dilation and relaxation [2, 3]. Currently, objective and clear diagnostic criteria for cervical incompetence are lacking, with the clinical diagnosis relying primarily on the combination of medical history, typical clinical manifestations, and ultrasound findings [3]. Reaching a definitive diagnosis of cervical incompetence is crucial for improving neonatal outcomes, as prompt and appropriate treatment can reduce the risk of late pregnancy miscarriage and premature delivery [4].
The incidence of cervical incompetence ranges from 0.1% to 2% of all pregnancies, and it is recognized as an important cause of miscarriage and premature birth in the third trimester of pregnancy [5]. In a cohort of 175 mid-trimester miscarriage cases, 43.4% of cases were attributed to cervical incompetence, highlighting it as the leading cause of mid-trimester miscarriage [6]. A large Danish cohort study involving 9602 women by Sneider et al. [7] found a 7.3% recurrence rate of extreme preterm delivery (16+0 to 27+6 gestational weeks) or mid-trimester miscarriage, which markedly varied by phenotypes. The highest recurrence rate of 28% was observed in cases of cervical incompetence.
The treatments for cervical incompetence are primarily classified into conservative treatment and surgery. Cervical cerclage is a surgical procedure aimed at preserving cervical integrity to prolong gestation and improve obstetrical outcomes [8], and it is classified into prophylactic, therapeutic, and emergency cerclage [9, 10]. Cervical cerclage is considered the primary and most effective surgical treatment for preventing preterm delivery caused by cervical incompetence [11]. The McDonald and Shirodkar procedures are the two main types of transvaginal cervical cerclage performed during pregnancy. Although the surgical techniques differ, studies have shown no significant difference in neonatal survival rates between the two methods [12, 13]. The Shirodkar cerclage involves placing the suture higher on the cervix, making it more technically challenging and increasing the risk of bleeding, which makes it more suitable for women with a shorter cervix and vagina [14]. In contrast, the McDonald cerclage is less invasive, requiring no dissection into para-cervical tissues, simpler to perform, and easy to remove, making it the preferred method for transvaginal cervical cerclage [14]. However, the specific factors affecting the prognosis following McDonald cervical cerclage have not been fully elucidated. To address this gap, this retrospective study enrolled pregnant women with cervical incompetence admitted to our hospital to assess the clinical efficacy and prognostic factors of McDonald cervical cerclage.
We retrospectively reviewed the medical records of pregnant women with cervical
incompetence who were treated at the Second Affiliated Hospital of Fujian Medical
University between January 2021 and December 2022. Cervical incompetence was
confirmed through imaging examinations. The inclusion criteria for this study
were: (1) a history of multiple spontaneous abortions in the second trimester or
previous cervical surgery, as these factors are strongly associated with cervical
incompetence and help identify high-risk individuals; (2) abnormal findings in
any of the following three sonographic indicators after 12 weeks of pregnancy:
cervical canal width
All the included participants underwent McDonald cervical cerclage, with the choice of prophylactic or therapeutic cerclage based on their clinical history and the timing of the procedure. The McDonald cerclage was conducted under intraspinal anesthesia as previously described [16]. Briefly, the cervix was held with a cervical clamp and gently pulled downward. A horizontal suture was then placed near the internal cervical orifice, and the orifice was closed by tightening the suture around the cervix at the anterior vaginal fornix. Postoperatively, cefuroxime was administered for infection prevention. The medication was discontinued in the absence of obvious signs of uterine contractions, and adjustments to the type and duration of medication were made in cases of fever or vaginal bleeding.
In this study, a poor prognosis was defined by the following: primary cesarean section, macrosomia, low birth weight, premature delivery, miscarriage, hypertension, abnormal amniotic fluid, premature rupture of membranes, postpartum hemorrhage, fetal distress, cesarean section after labor, forceps assisted delivery, neonatal asphyxia, neonatal hypoglycemia, or infection. If any of these conditions occurred, the pregnancy was considered to have an adverse outcome, and the patients were assigned to the poor prognosis group. Conversely, if none of these conditions occurred or if the pregnancy outcome was as expected with no serious complications, the patients were assigned to the good prognosis group. Based on these criteria, the 100 enrolled women were categorized into the good prognosis (n = 37) and poor prognosis (n = 63) groups.
Data were analyzed using SPSS software (version 24.0, IBM
Corporation, Armonk, NY, USA). Categorical data, such as a history of assisted
reproductive technology (ART) and bicornuate uterus, were presented as frequency
n (%). Pearson Chi-square test was utilized
when the expected frequency T
This study included 100 pregnant women who met the inclusion
and exclusion criteria. Of these, 42 women underwent prophylactic cerclage, and
the remaining 58 women had therapeutic cerclage. The mean gestational age at the
time of the McDonald cerclage was 17.05
| Prophylactic cerclage | Therapeutic cerclage | t | p | |
| (n = 42) | (n = 58) | |||
| Gestational weeks, weeks | 17.05 |
22.85 |
13.471 | |
| Operation time, mins | 21.95 |
25.02 |
1.824 | 0.071 |
“t”, the t statistic in t-test.
The 100 pregnant women were assigned to good prognosis (n = 37, aged 28.18
| Variables | Poor prognosis | Good prognosis | t/ |
p | |
| (n = 63) | (n = 37) | ||||
| Age, years | 28.17 |
28.18 |
0.016c | 0.990 | |
| Pro-gestational BMI, kg/m2 | 24.88 |
21.04 |
11.093c | 0.000 | |
| Abortions times, times | 0.87 |
0.25 |
10.851c | ||
| Graviditas, times | 2.29 |
1.90 |
2.112c | 0.040 | |
| Birth times, n (%) | 19.899a | ||||
| 22 (34.92) | 30 (81.08) | ||||
| 41 (65.08) | 7 (18.92) | ||||
| ART | 18 (28.57) | 4 (10.81) | 4.285a | 0.038 | |
| Uterus bicornis | 1 (1.59) | 1 (2.70) | - | 0.605 | |
| Cervical conization | 7 (11.11) | 0 (0.00) | 2.879b | 0.090 | |
| Complete uterine cavity curettage | 30 (47.62) | 10 (27.03) | 4.118a | 0.042 | |
| Premature delivery | 20 (31.75) | 4 (10.81) | 5.601a | 0.018 | |
| Prolonged second stage of labor | 15 (23.81) | 2 (5.41) | 5.596a | 0.018 | |
| Cesarean section | 35 (55.56) | 10 (27.03) | 7.665a | 0.006 | |
| Gestational hypertension | 20 (31.75) | 11 (29.73) | 0.044a | 0.833 | |
| Gestational diabetes mellitus | 25 (39.69) | 15 (40.54) | 0.007a | 0.933 | |
| Cervical laceration | 40 (63.49) | 4 (10.81) | 26.255a | ||
| Vaginal infection | 30 (47.62) | 2 (5.41) | 19.089a | ||
| Kysthitis | 50 (79.37) | 10 (27.03) | 26.605a | ||
| PCOS | 9 (14.29) | 0 (0.00) | 4.195b | 0.041 | |
| McDonald cerclage types | 10.350a | 0.001 | |||
| Prophylactic cerclage | 25 (39.68) | 27 (72.97) | |||
| Therapeutic cerclage | 38 (60.32) | 10 (27.03) | |||
BMI, body mass index; ART, assisted reproduction technology; PCOS, polycystic
ovarian syndrome. “t”, the t statistic in t-test;
“
The 14 prognosis-associated factors identified in Table 2 were further analyzed using a multivariate logistic regression model. Cervical conization was also included in the model because that a history of cervical conization is known to be a risk factor for poor pregnancy outcomes. As displayed in Table 3, 10 factors were identified to independently affect prognosis, including gravidity, having more than two previous births, ART, history of cervical conization, complete uterine cavity curettage, prolonged second stage of labor, cesarean section, cervical laceration, PCOS, and McDonald cerclage types. In addition to McDonald cerclage types (odds ratio [OR] = 0.73, 95% confidence interval [CI]: 0.54~0.99), all other nine factors were identified as risk factors that increase the risk of poor prognosis. Among these, having more than two previous births had the greatest influence on prognosis, with an OR of 2.44 (95% CI: 1.87~3.18), followed by prolonged second stage of labor (OR = 2.19, 95% CI: 1.57~3.05) and history of cervical conization (OR = 1.88, 95% CI: 1.28~2.76).
| Variables | SE | Wald/ |
p | OR | 95% CI | |
| Graviditas | 0.56 | 0.12 | 21.16 | 1.75 | 1.38~2.22 | |
| Birth times |
0.89 | 0.15 | 30.24 | 2.44 | 1.87~3.18 | |
| ART | 0.42 | 0.18 | 5.39 | 0.020 | 1.52 | 1.07~2.15 |
| Cervical conization | 0.63 | 0.20 | 9.46 | 0.002 | 1.88 | 1.28~2.76 |
| Complete curettage of uterine cavity | 0.51 | 0.16 | 10.84 | 0.001 | 1.67 | 1.22~2.28 |
| Prolonged second stage of labor | 0.78 | 0.19 | 16.93 | 2.19 | 1.57~3.05 | |
| Cesarean section | 0.39 | 0.17 | 5.76 | 0.016 | 1.48 | 1.06~2.07 |
| Cervical laceration | 0.59 | 0.14 | 16.64 | 1.80 | 1.37~2.37 | |
| PCOS | 0.47 | 0.21 | 5.24 | 0.022 | 1.60 | 1.06~2.42 |
| McDonald cerclage types | –0.31 | 0.15 | 4.04 | 0.044 | 0.73 | 0.54~0.99 |
ART, assisted reproduction technology; PCOS, polycystic ovarian syndrome;
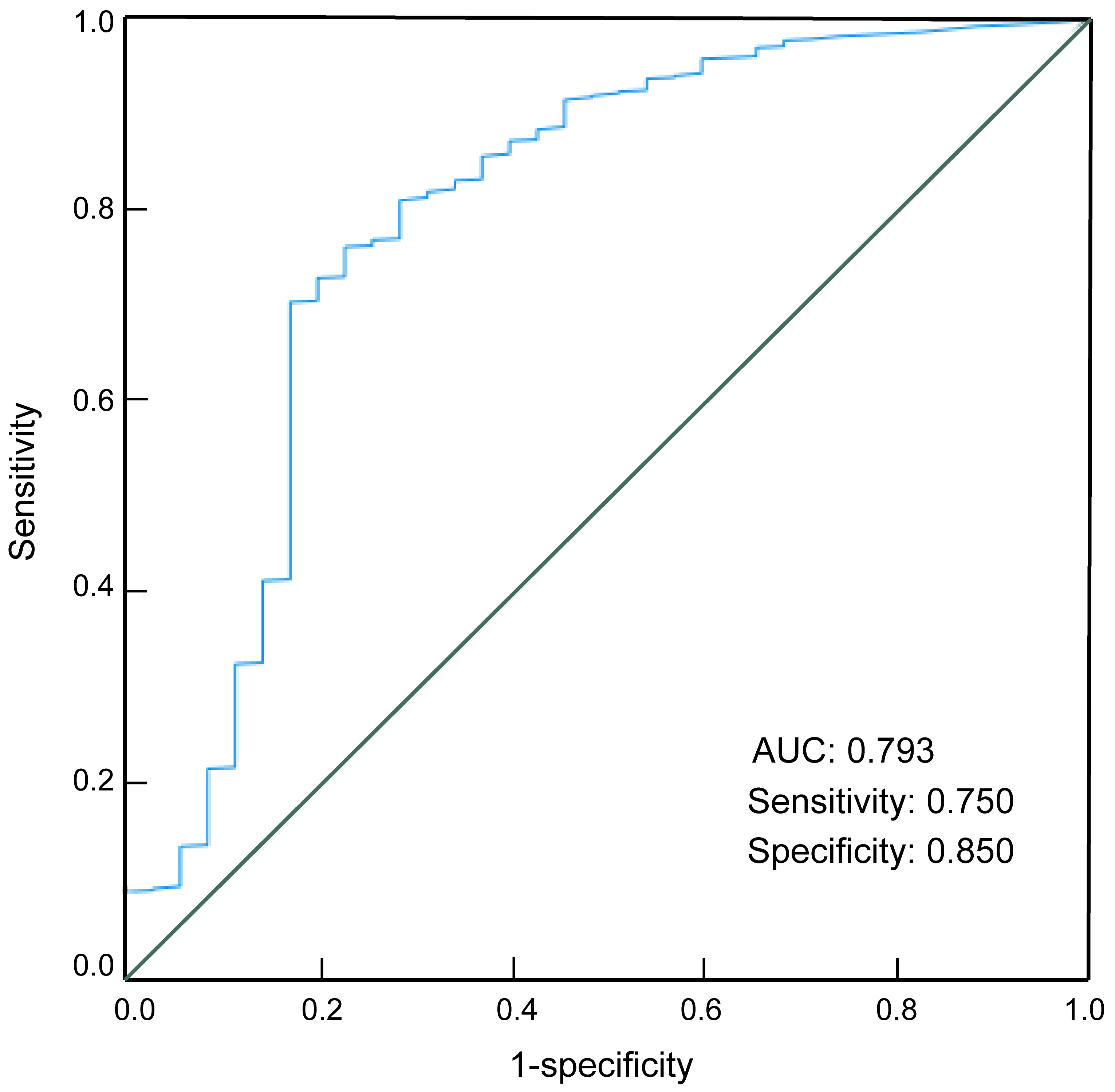
We generated an ROC curve for the prognostic factors identified from the logistic regression analysis. As shown in Fig. 1, these factors demonstrated good predictive performance for the prognosis of patients with cervical incompetence, with an area under the curve of 0.793; the sensitivity and specificity were 0.75 and 0.85, respectively (Table 4).
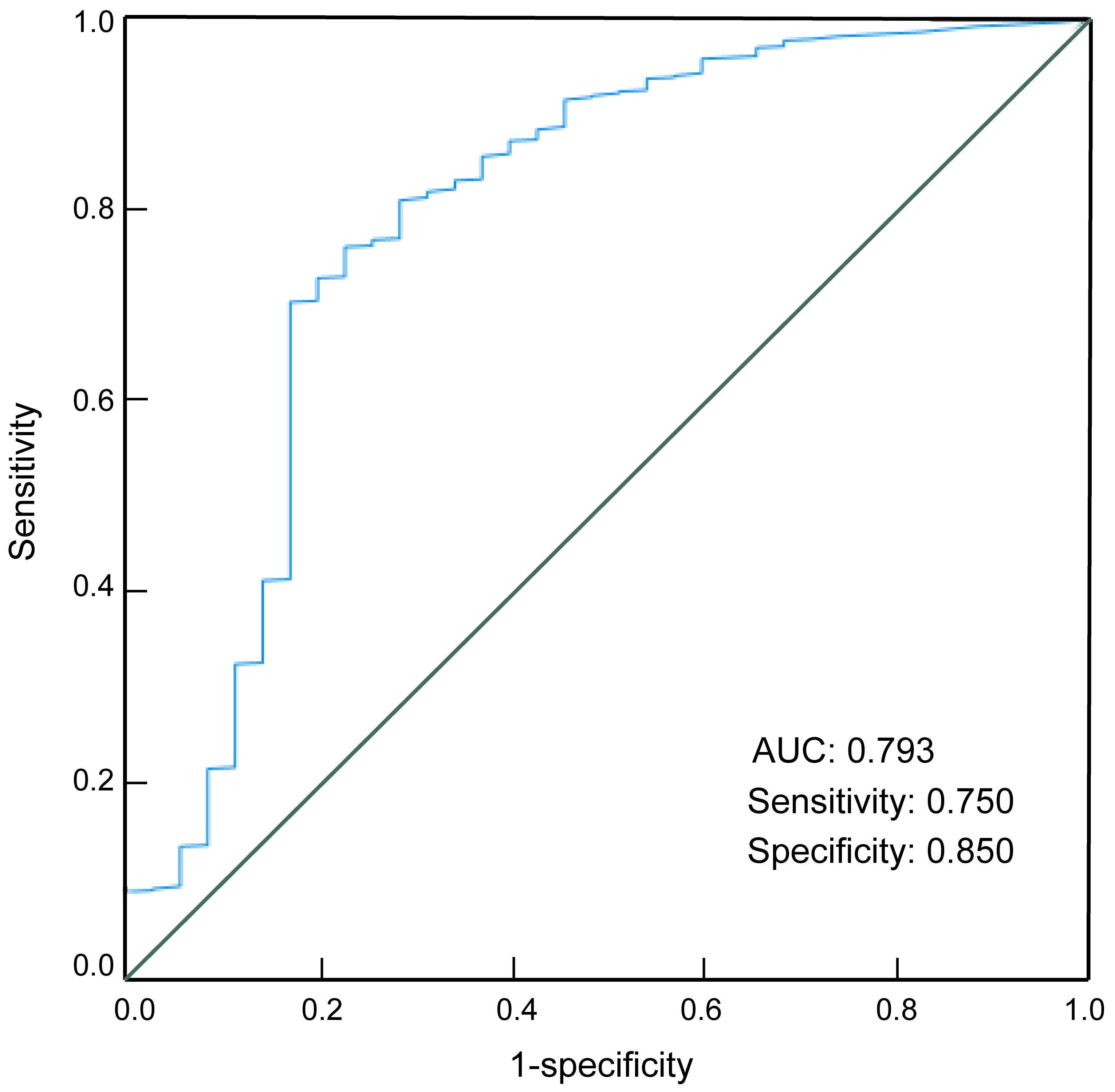 Fig. 1.
Fig. 1.
Receiver operating charcteristic curve for testing the predictive performance of prognostic factors. AUC, area under curve.
| AUC | Cut-off | Sensitivity | Specificity | Youden’s index | p | 95% CI |
| 0.793 | 0.400 | 0.750 | 0.850 | 0.600 | 0.000 | 0.700~0.887 |
Note: AUC, area under curve; ROC, receiver operating characteristic; 95% CI, 95% confidence interval.
Pregnancy outcomes, including miscarriage, preterm birth, term birth, and
neonatal survival, were evaluated and compared between the two prognosis groups
(Table 5). Both groups had similar neonatal survival rates (97.30% vs.
98.41%, p = 0.605). In addition, the good prognosis group showed a
tendency for a higher rate of term birth (97.30% vs. 87.30%) and lower
rates of miscarriage (2.70% vs. 9.52%) and preterm birth (0
vs. 3.17%) compared to the poor prognosis group; however, these
differences were not statistically significant (all p
| Poor prognosis | Good prognosis | p | ||
| (n = 63) | (n = 37) | |||
| Neonatal survival, n (%) | 62 (98.41%) | 36 (97.30%) | - | 0.605 |
| Term birth, n (%) | 55 (87.30%) | 36 (97.30%) | 1.754b | 0.185 |
| Preterm birth, n (%) | 6 (9.52%) | 1 (2.70%) | 0.783b | 0.376 |
| Miscarriage, n (%) | 2 (3.17%) | 0 (0.00%) | - | 0.395 |
Note: “-”, Fisher’s exact test; “b”, continuity-corrected Chi-square test.
Recently, the incidence of cervical incompetence has gradually increased with the increase in cervical procedures and the growing number of older pregnant women. Cervical incompetence is a leading cause of late-term miscarriages or preterm birth, increasing burdens on families and society. Study has shown that for women with cervical incompetence, both prophylactic vaginal cerclage and abdominal cerclage significantly reduced recurrence rates of mid-trimester miscarriage of preterm delivery compared to no cerclage [17]. This suggests that cervical cerclage is an effective and safe surgical option for treating cervical incompetence. However, some patients still experience poor pregnancy outcomes after cervical cerclage, highlighting the need for reliable predictors to evaluate the efficacy of the procedure.
In this study, we retrospectively reviewed the clinical outcomes and prognostic factors in 100 pregnant women with cervical incompetence who underwent McDonald cervical cerclage. We found that the poor prognosis group had a higher proportion of women with more than two previous births or had a history of ART, cervical conization, complete uterine cavity curettage, premature delivery, prolonged second stage of labor, cesarean section, cervical laceration, vaginal infection, cystitis, and PCOS compared to the good prognosis group. Multivariate logistic regression revealed that factors such as gravidity, more than two previous births, ART, a history of cervical conization, complete curettage of uterine cavity, prolonged second stage of labor, cesarean section, cervical laceration, and PCOS were risk factors for worse prognosis after McDonald cerclage. Particularly, more than two previous births had the strongest adverse influences on prognosis, followed by a prolonged second stage of labor and a history of cervical conization.
Regarding McDonald cerclage types, we found that the poor prognosis group had a higher proportion of patients who underwent therapeutic cerclage and a lower proportion of patients who underwent prophylactic cerclage, suggesting that the cerclage type significantly affects prognosis. Further multivariate logistic regression analysis indicated that prophylactic cerclage was a protective factor. Prophylactic cerclage is typically performed in pregnant women with a history of preterm birth or cervical insufficiency. In contrast, therapeutic cerclage is used in the presence of evidence of cervical shortening or dilation during pregnancy. These two cerclage types differ in timing and indications, with prophylactic cerclage being generally more effective as it intervenes before complications arise. Liu et al. [5] demonstrated that both prophylactic and therapeutic cervical cerclage decrease the incidence of recurrent miscarriage or preterm birth and effectively lengthen the pregnancy with live births. Notably, prophylactic cerclage was significantly superior regarding shorter operative time, reduced postoperative hospital stays, later gestational age at delivery, and higher rates of term birth, as well as live births.
The uterine cervix is critical for maintaining a pregnancy to term and undergoes extensive remodeling processes throughout pregnancy and parturition, such as the degradation and reorganization of extracellular matrix components [18]. During parturition, the cervix may experience increased mechanical stress, which can reduce collagen fibers and mucosaccharide content, affecting its anatomical structure and increasing the risk of cervical incompetence and adverse pregnancy outcomes [19, 20]. This may explain the adverse impact of having more than two previous births and a prolonged second stage of labor on prognosis in this study. Complete curettage of the uterine cavity can cause significant mechanical damage to the cervix, promoting the process of foreign body injury, inflammatory response, and repair and regeneration of the cervix, which can affect cervical tension and expansion and increase the risk of cervical incompetence and poor prognosis [21]. Therefore, effective contraceptive measures should be considered to reduce the number of abortions, particularly for unmarried women or unplanned pregnancies. A prolonged second stage of labor can cause continuous cervical dilation and cervical anatomical structure damage, increasing the risk of fetal distress, neonatal asphyxia, and other adverse pregnancy outcomes [22, 23].
A history of cervical conization is known to be a risk factor for poor pregnancy outcomes. Women who have undergone cervical conization often have poorer cervical function during pregnancy compared to those who have not [24, 25, 26]. For instance, based on a cohort of 133 pregnant patients, Hashiramoto et al. [27] found that women with a history of conization exhibited higher rates of spontaneous preterm birth and delivered at earlier gestational week compared to those without a conization history. This is likely due to damage to the mechanical support, integrity, and extensibility of the cervix (shortened cervix), inconsistent proportion of collagen in original versus regenerated cervical tissues, and decreased cervical mucus, leading to poor cervical bearing capacity during pregnancy [24, 25, 26].
The association between ART and cervical incompetence is increasingly recognized. The multiple medications and frequent uterine procedures during ART can increase the probability of cervical incompetence, which is a known cause of miscarriage and premature delivery among pregnant women who receive ART [28]. Gökçe et al. [29] noted that pregnant women who underwent hysteroscopy before embryo transfer had a higher incidence of cervical incompetence between 13 and 27 weeks of gestation, likely due to cervical damage from mechanical dilation. Additionally, assisted reproduction has been identified as a risk factor for preterm delivery in pregnant women with a short cervix, possibly due to the increased risk of hidden infection from the procedures [30]. PCOS, an endocrine disorder associated with infertility and obesity, has also been linked to a higher risk of cervical incompetence [31]. For example, women with cervical incompetence and PCOS often experience earlier average gestational weeks and relatively worse pregnancy outcomes compared to those without PCOS [32]. Therefore, more attention should be given to monitoring cervical changes in pregnant women with PCOS to reduce the risk of miscarriage and premature birth.
In summary, McDonald cervical cerclage for cervical incompetence can prolong the gestational age and reduce the rate of miscarriage and premature delivery, improving maternal and infant outcomes. This study identified various risk factors that adversely affect prognosis in pregnant women with cervical incompetence after McDonald cerclage, including having more than two previous births, a history of cervical conization, and a prolonged second stage of labor. These factors should be considered in the clinical management of pregnant women with cervical incompetence. Additionally, prophylactic cerclage demonstrated a protective effect, highlighting the importance of early detection and intervention in improving pregnancy outcomes.
ART, assisted reproductive technology; CI, confidence interval; OR, odds ratio; PCOS, polycystic ovarian syndrome; ROC, receiver operating characteristic curve; AUC, area under curve.
The data that support the findings of this study are available from the corresponding author, LL, upon reasonable request.
ML and LL designed the research study. ML performed the research and analyzed the data. LL wrote the manuscript. Both authors contributed to editorial changes in the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All participants provided informed consent before their inclusion in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Fujian Medical University (approval number: 2024-136).
Not Applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.