


1 Department of Obstetrics, Xiangya Hospital Central South University, 410008 Changsha, Hunan, China
2 Hunan Engineering Research Center of Early Life Development and Disease Prevention, 410008 Changsha, Hunan, China
Abstract
Twin pregnancies are associated with a higher risk of adverse pregnancy outcomes than are singleton pregnancies. Although the risk factors and predictors of adverse outcomes in singleton pregnancies have been clearly identified in numerous studies, those specific to twin pregnancies remain less consistent. This study was performed to summarize and evaluate the risk factors and predictors of adverse outcomes in twin pregnancies.
A comprehensive review was conducted using the PubMed and Web of Science databases to analyze and identify the relevant risk factors and predictors of avderse outcomes in twin pregnancies.
The risk factors and predictors of adverse outcomes in twin pregnancies are largely similar to those in singleton pregnancies, particularly in relation to preeclampsia and preterm birth and especially for conditions not unique to twin pregnancies. However, there remains a gap in the study of complications specific to twin pregnancies, largely because of their chorionicity.
Early identification of risk factors and predictors for adverse outcomes in twin pregnancies facilitates earlier prevention and intervention and lead to improved management of serious complications in twin pregnancies.
Keywords
- twin pregnancy
- adverse outcome
- risk factor
- predictor
Twin pregnancies carry a high risk of pregnancy complications, including preeclampsia (PE), preterm birth (PTB), selective fetal growth restriction (sFGR), and fetal brain injury, among others. Additionally, monochorionic twin pregnancies have a higher rate of complications because of the shared placenta, which may result in twin-to-twin transfusion syndrome (TTTS) or twin anemia–polycythemia sequence (TAPS) [1]. Newborns from twin pregnancies are at increased risk of adverse outcomes, including birth defects, brain injury, and stillbirth, due to these complications [2]. Although twin pregnancies account for only about 3% of all live births, they represent approximately 15% of neonatal intensive care unit admissions. The management of singleton pregnancies has reached a relatively advanced level, and the risk factors and predictors of adverse complications in singleton pregnancies have been extensively studied [3, 4]. However, fewer studies have specifically addressed the risk factors and predictors of adverse outcomes in twin pregnancies, leading to less consistent management in clinical practice. Therefore, it is crucial to identify the risk factors and predictors of adverse complications in twin pregnancies to improve management and facilitate early intervention.
The PubMed and Web of Science databases were searched for studies reporting on risk factors and predictors of adverse outcomes in twin pregnancies, such as PE, PTB, TTTS, sFGR, and brain injury. All literature related to risk factor and predictors of adverse outcomes in twin pregnancies was considered adequately. The search keywords were defined: twin pregnancy, preterm birth, preeclampsia, twin-to-twin transfusion syndrome, selective fetal growth restriction, fetal brain injury, risk factor, predictor. Subsequently, the exclusion criteria were defined: (1) not evaluating risk factors and predictors, (2) the literature type was neither an article nor a review, (3) full text not retrieved, (4) the language was limited to English. The literature search was led by one author (BW). Titles and abstracts of all related literature were screened independently by two authors (YF and QW). The results and conclusions reached consensus among all authors. Additionally, differences in risk factors and predictors between twin and singleton pregnancies were compared. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram is detailed in Fig. 1.
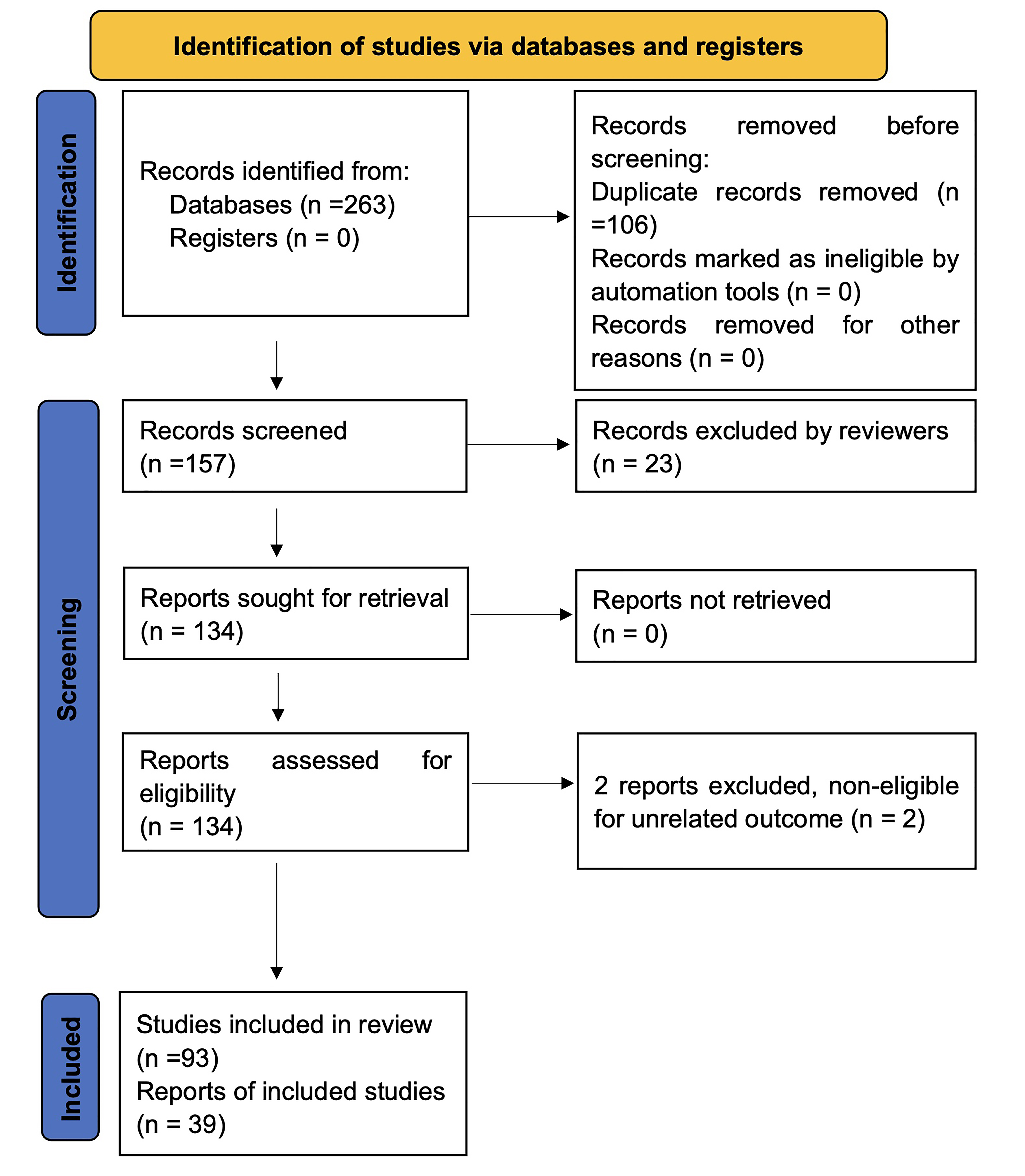 Fig. 1.
Fig. 1.
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram of identification of studies.
PE is a hypertensive disorder involving multisystem impairment, affecting 4.6% of pregnancies and representing a significant cause of perinatal morbidity and mortality [5]. The prevalence of PE is much higher in twin pregnancies than in singleton pregnancies [6], and in twin pregnancies, PE tends to be more severe and have a worse prognosis. Given that twin pregnancies often result in PTB, the relative risk of PE may be underestimated in this group. The incidence of twin pregnancies has increased rapidly over the last 30 years [7]. While significant progress has been made in predicting PE in singleton pregnancies, less information is available for twin pregnancies. Therefore, predicting PE in twin pregnancies is of great significance.
The risk factors for PE in singleton pregnancies are well known, but those in twin pregnancies are less consistent. Hypertensive disorders of pregnancy, including PE, chronic hypertension, and gestational hypertension, are among the most prevalent diseases in pregnancy. Because of its particular pathological mechanisms, PE is a risk factor for many placenta-related diseases. Taguchi et al. [8] found that a family history of hypertension and a history of hypertensive disorders of pregnancy are independent risk factors for PE in twin pregnancies, similar to findings in singleton pregnancies. A study at King Chulalongkorn Memorial Hospital among women with twin pregnancies who delivered after 23 weeks of gestation identified nulliparity and chronic hypertension as risk factors for PE after multivariate logistic regression analysis [9]. Women under 17 years of age with twin pregnancies have a higher risk of PE than those over 17 years of age [10]. Chantanahom et al. [9] pointed out that low gestational weight gain is a significant protective factor against the development of PE. Similarly, Lipworth et al. [11] found that gestational weight gain below Institute of Medicine (IOM) guidelines was associated with PTB before 32 weeks of gestation and a decrease in the risk of PE, while gestational weight gain above IOM guidelines was associated with a higher risk of PE. This suggests that inappropriate gestational weight gain affects more than half of twin pregnancies and is a modifiable risk factor for PE. Gestational diabetes, another prevalent pregnancy complication, continues to rise due to increasing obesity rates among pregnant women. Gestational diabetes is often related to complications such as higher infant weight and cardiometabolic disease. Dave et al. [12] identified gestational diabetes as a risk factor for PE in women with twin pregnancies. Dai et al. [13] conducted a five-year retrospective study and found that in preeclamptic dichorionic twin pregnancies, in vitro fertilization and growth discordance are risk factors for developing early-onset PE. Additionally, intrahepatic cholestasis of pregnancy increases the incidence of PE, highlighting the necessity of routine evaluation for PE in the treatment of women with moderate and severe intrahepatic cholestasis of pregnancy [14].
Several studies have identified predictors of PE. Stepan et al. [15]
found that the soluble fms-like tyrosine kinase 1 (sFlt-1)/placental growth
factor (PlGF) ratio can be applied to predict PE in twin pregnancies. It is worth
noting that PlGF, sFlt-1, and the sFlt-1/PlGF ratio were initially utilized to
predict and monitor PE, PTB, and other placenta-related disorders in singleton
pregnancies, and their role in predicting placenta-related disorders in twin
pregnancies is also significant. Lu et al. [16] reported that
considering early pregnancy serum markers
(
Similar to singleton pregnancies, maternal age, parity, gestational weight gain, history of PE, ethnicity, and gestational diabetes are associated with a higher risk of PE in twin pregnancies [18]. The risk factors of assisted reproduction continue to be debated, with a study reporting an increased risk of PE with assisted reproduction and others reporting no significant difference between spontaneous and assisted reproductive pregnancies [19]. It is possible that assisted reproduction shares risk factors with PE, leading to confounding factors in the analysis.
In singleton pregnancies, guidelines proposed by the American College of Obstetricians and Gynecologists (ACOG) and the National Institute for Health and Care Excellence (NICE), commonly used in clinical practice, suggest that women with one or more high-risk factors or two or more moderate-risk factors should be considered as at high risk for PE [20, 21]. Various prediction models based on risk factors and predictors have been successfully applied in predicting PE in the first trimester of pregnancy by combining maternal risk factors, mean arterial pressure, uterine artery pulsatility index, and PlGF [22, 23]. However, because of the inconsistency in studies on predicting PE in twin pregnancies, the risk factors and prediction models for such pregnancies remain elusive.
PTB refers to delivery before 37 completed weeks of gestation. Globally, approximately 15 million infants are born preterm each year. PTB complications are a leading cause of neonatal mortality and are associated with long-term neurodevelopmental and physical development issues, as well as significant public health challenges [24]. The PTB rate in twin pregnancies has increased significantly over the past three decades because of the rising incidence of twin pregnancies worldwide. The increased incidence of PTB in twin pregnancies, unlike in singleton pregnancies, may be associated with factors such as chorionicity, cervical insufficiency, maternal and fetal complications unique to twin pregnancies, uterine overdistension, and uterine hypoxia [24]. Given the unique physiopathology of twin pregnancies, it is crucial to study them separately from singleton pregnancies and to identify risk factors and predictors with a focus on chorionicity and other twin-specific complications.
Risk factors for PTB in singleton pregnancies include a history of previous PTB,
ethnicity, low maternal body mass index, and periodontal disease. Both
spontaneous PTB and medically indicated PTB (PTB in response to maternal or fetal
complications) have been investigated. In twin pregnancies, a previous
spontaneous singleton PTB is an important risk factor, as identified by
Berveiller et al. [25] in a retrospective cohort study. With regard to
maternal weight, gestational weight gain below IOM guidelines, compared with
weight gain within IOM guidelines, has been linked to PTB before 32 weeks of
gestation [11]. With regard to chorionicity, fetal complications have been linked
with PTB in monochorionic twins, particularly TTTS, TAPS, and other severe
conditions. For example, Marleen et al. [26] found that monochorionicity
is significantly associated with spontaneous PTB before 28, 32, 34, and 37 weeks
of gestation in women who are both symptomatic and asymptomatic for preterm
labor. Single intrauterine death (sIUD) is a relatively common complication in
twin pregnancies, with an incidence of approximately 0.5% to 6.8% [27]. sIUD
often presents with PTB and cerebral palsy in the surviving twin. D’Antonio
et al. [28] found that sIUD in twin pregnancies is linked with a
significant risk of PTB, particularly in monochorionic twins. Twin pregnancies
complicated by sIUD, regardless of chorionicity, are at higher risk of PTB before
34, 32, and 28 weeks of gestation [28]. Interestingly, Qiao et al. [29]
found that exposure to fine particulate matter
With regard to predictors of PTB in twin pregnancies, transvaginal cervical length measurement before 24 weeks is the most significant and widely accepted predictor [31]. Many guidelines, such as those in the NICE guidelines for twin and triplet pregnancies and the ACOG Practice Bulletin for multifetal gestations, indicate that transvaginal cervical length is an effective measure for predicting PTB [32, 33]. Kuhrt et al. [34] found that quantitative fetal fibronectin measured between 22 and 27+6 weeks of gestation was a precise predictor of spontaneous PTB before 30 weeks in twin pregnancies. Similarly, Marleen et al. [35] observed that fetal fibronectin was a significant predictor of PTB among twin pregnancies in women both asymptomatic and symptomatic for preterm labor. Therefore, a combination of quantitative fetal fibronectin concentration and short cervical length could be the strongest predictor of spontaneous PTB [36]. Further studies should address the combination of quantitative fetal fibronectin concentration and transvaginal cervical length in the prevention of PTB in twin pregnancies. One cohort study reported that maternal 25-hydroxyvitamin D concentrations below 75 nmol/L in the late second trimester were associated with an increased risk of PTB in twin pregnancies [37].
Risk factors for developing PTB in singleton pregnancies include prior PTB, low gestational weight gain, monochorionicity, sIUD, and exposure to PM2.5. An interesting study also identified increasing maternal age as a risk factor for PTB in twin pregnancies after in vitro fertilization [38]. It is important to note that short cervical length and quantitative fetal fibronectin concentration are highly associated with spontaneous PTB.
TTTS and sFGR are unique complications in monochorionic pregnancies. TTTS is a severe condition that occurs in 10% to 15% of monochorionic diamniotic twin pregnancies [39]. The Quintero staging system is a critical tool for assessing the severity of TTTS, dividing it into four stages (I–IV). Sonographic examination should be considered for twin pregnancies with a monochorionic diamniotic placenta to monitor the progression and severity of this disease [40]. The natural history of stage I TTTS is relatively favorable, with a perinatal survival rate of 86% and no need for invasive intervention. However, the prognosis of advanced TTTS is very poor, with single or double twin death occurring in 90% to 100% of cases [41]. Fetoscopic laser surgery is considered the best approach for advanced TTTS between 16 and 26 weeks, but data analysis reveals no significant survival benefit, and long-term neurological outcomes remain disappointing [42].
sFGR is characterized by one fetus growing normally while the other is
growth-restricted; it affects 10% to 15% of monochorionic diamniotic twin
pregnancies. It is defined as one fetus being less than the 10th percentile for
fetal weight at the same gestational age, with an estimated fetal weight
difference between the two fetuses of
Stagnati et al. [44] found that monochorionic twin pregnancies with
intertwin nuchal translucency discrepancy, nuchal translucency at the
Chen et al. [48] and Zumaeta et al. [49] found that types II and III sFGR were associated with adverse perinatal outcomes in univariate and multivariate logistic regression analyses, suggesting that these types of sFGR are risk factors for adverse outcomes in sFGR. Similarly, Monaghan et al. [50] found that pregnancies complicated by type II sFGR are associated with a higher risk of adverse perinatal outcomes compared with those complicated by type I sFGR. With regard to the predictors of sFGR, a prospective longitudinal cohort study revealed that the combination of L-phenylalanine, L-leucine, and L-isoleucine in the second trimester significantly predicted the occurrence of sFGR [51].
With regard to TTTS and sFGR, few studies have explored the risk factors and predictors in twin pregnancies, likely because of the low incidence of these conditions. Therefore, more research and attention are needed to better understand these two diseases.
Fetal brain injury can lead to serious long-term neurodevelopmental impairment.
The five types of perinatal brain injuries include hypoxic–ischemic
encephalopathy, intraventricular hemorrhage, periventricular leukomalacia,
perinatal stroke, and cerebral palsy. Hypoxic–ischemic encephalopathy affects
approximately 3 in 1000 live births [52], and therapeutic hypothermia and
postnatal erythropoietin could potentially prevent it [53]. Intraventricular
hemorrhage primarily affects preterm infants (
An increased incidence of brain injury has been observed in monochorionic twins, and the window for potentially effective treatment is narrow. Close monitoring of intrauterine growth and development, emphasizing the importance of umbilical artery Doppler blood flow monitoring and evaluation, and timely termination of pregnancy or selective fetal reduction by vascular occlusion and laser ablation are effective measures to prevent brain injury in surviving fetuses [56].
To date, most studies on fetal brain injury have focused on TTTS. Sileo et al. [57] reported that the overall incidence of diagnosed fetal brain injury in twin pregnancies with TTTS following laser surgery is approximately 2%. Duyos et al. [58] found that in monochorionic twins, the risk of brain injury is higher when sIUD occurs spontaneously. The main risk factors for prenatal brain injury in the surviving twin include gestational age at sIUD, sFGR, and anemia. Spruijt et al. [59] found that fetal brain injury in TTTS is related to recurrent TTTS, TAPS following laser surgery, and lower gestational age at birth. The limited number of studies on fetal brain injury reflects the technical limitations in screening for antenatal brain injury [60]. From a pathological perspective, maternal factors such as gestational hypertension, gestational diabetes mellitus, and intrahepatic cholestasis of pregnancy could be risk factors for fetal brain injury. Risk factors and predictors of the adverse outcome in twin pregnancies are shown in Table 1.
| Complications | Risk factors | Predictors |
| PE | Nulliparity, chronic hypertension, history of hypertension and history of hypertensive disorders of pregnancy, young mother, high gestational weight gain, gestational diabetes, IVF, ICP | sFlt-1/PlGF ratio, |
| PTB | Previous spontaneous singleton PTB, low gestational weight gain, monochorionicity, sIUD, exposure to PM2.5 | Transvaginal cervical length, fetal fibronectin |
| TTTS | Intertwin NT discrepancy, NT |
Amniotic fluid microRNAs, VEGF-R1, VEGF-R2, IL-6 |
| sFGR | Types II and III sFGR | L-phenylalanine, L-leucine, and L-isoleucine |
| Brain injury | TTTS or TAPS following laser surgery, sIUD, lower gestational age at birth | None |
PE, preeclampsia; PTB, preterm birth;
PM2.5, fine particulate matter
Twin pregnancies are more likely to involve serious maternal and neonatal complications, making it crucial to identify the risk factors and predictors of adverse outcomes in twin pregnancies for primary prevention. Some risk factors for adverse outcomes in twin pregnancies are similar to those in singleton pregnancies. However, because of the specific characteristics of twin pregnancies, risk factors for certain conditions, such as sFGR, TTTS, and brain injury, differ significantly from those in singleton pregnancies.
Ultrasonography and clinical staging are important tools for predicting and monitoring unique complications in twin pregnancies, such as TTTS and sFGR, with ultrasonography being a key diagnostic and staging modality. Fetal brain injury is primarily related to PTB and TTTS or TAPS following laser surgery, as well as sIUD.
Future studies on risk factors and predictors should explore the mechanisms underlying the occurrence and development of adverse outcomes in twin pregnancies, many of which remain unclear. In clinical practice, it is essential to recognize the differences between twin and singleton pregnancies. Early identification of risk factors for adverse outcomes in twin pregnancies facilitates earlier prevention and intervention. Better control of predictors can lead to improved management of serious complications in twin pregnancies and prevent poor maternal and infant outcomes.
Conceptualization, BW, WZ, and JH; Data curation, BW, YF, and QW; Formal analysis, BW, YF, and QW; Funding acquisition, WZ and JH; Investigation, BW, YW, JN, LL, XZ, and HZ; Methodology, BW, WZ and JH; Resources, YW, JN, LL, XZ, and HZ; Writing – original draft, BW; Writing – review & editing, JH. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This research was funded by the Natural Science Foundation of Hunan Province (2022JJ40789), and the National Natural Science Foundation of China (82301927, 82371700, 81974236, 81571516).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.