


1 Department of Child Neurology, Institute for Child and Youth Health Care of Vojvodina, 21000 Novi Sad, Serbia
2 Department of Neurophysiology, Institute for Biological Research “Siniša Stanković" – National Institute of the Republic of Serbia, University of Belgrade, 11000 Belgrade, Serbia
3 Faculty of Medicine Novi Sad, University of Novi Sad, 21000 Novi Sad, Serbia
4 Department of Obstetrics and Gynecology, University Clinics of Vojvodina, 21000 Novi Sad, Serbia
5 Department of Pathology, University Clinics of Vojvodina, 21000 Novi Sad, Serbia
6 Department of Neurology, University Clinics of Vojvodina, 21000 Novi Sad, Serbia
Abstract
The 50% maximum probability of breech presentation (BP) implies that the same number of fetuses/newborns with the same characteristics take either BP or cephalic presentation (CP) with equal probability. Sirenomelia offers the possibility to investigate the incidence of BP in the simultaneous presence of several medical entities, each associated with an increased incidence of BP (Potter anomaly, lower limb fusion, prematurity, additional medical entities). The aim of the study is to investigate the probability of BP at delivery in sirenomelic singleton gestations to confirm the rule that the maximum probability for BP is 50%.
A systematic retrospective literature search using the keywords: sirenomelia, sympus apus, sympus monopus, and sympus dipus, in the SCOPUS database. Inclusion criteria: presentation of singleton fetuses at delivery in the second and third trimester of pregnancy. Comparison with chi-square test (level of significance p < 0.5) of overall incidence of BP and CP as well as depending on the type of sirenomelia, prematurity, presence of additional medical entities associated with increased incidence of BP.
In total, 67 articles were identified, and 83 cases were found. The number of cases in BP vs. CP with a statistical difference to expected 50%:50% distribution of presentations: All cases—BP44 CP39 p = 0.583; Premature birth—BP25 CP20 p = 0.456; Term birth—BP17 CP18 p = 0.866; Sympus apus—BP15 CP14 p = 0.853; Sympus monopus—BP6 CP9 p = 0.439; Sympus dipus—BP21 CP14 p = 0.237; With additional entities—BP16 CP10 p = 0.239; Without additional entities—BP23 CP26 p = 0.668. Also, there were no statistically significant differences in the distribution of presentations between premature and term birth (p = 0.589), three types of sirenomelia (p = 0.601), with and without additional entities (p = 0.228).
This study supports the rule that the maximum probability for BP in any medical entity, including sirenomelia, is 50%. The outcome of the BP should be evaluated with the case-control matching procedure: subtract the number of fetuses/newborns from the CP group that is identical to the number of fetuses/newborns in the BP group, with identical characteristics, and add this group to the BP group before comparing them to the rest of the CP fetuses/newborns.
Keywords
- breech presentation
- sirenomelia
- fetal presentation
- sympus apus
- sympus monopus
- sympus dipus
Current practice determines the outcome of breech presentation (BP) by directly comparing BP and cephalic presenting (CP) fetuses/newborns. This direct comparison method is disputed because the highest probability for BP is 50% [1, 2]. When conditions for BP are met, similar to a coin toss, the probability for BP or CP is 50%:50%. Practically, each fetus in BP has a counterpart in CP. The etiology of BP is not due to intentional positioning but is a result of the random filling of intrauterine space. The outcome of BP should be evaluated using the case-control matching procedure: match the number of fetuses/newborns in the CP group to the number of fetuses/newborns in the BP group with identical characteristics, and then add this matched group to the BP group before comparing them to the rest of the CP fetuses/newborns. The comparison between BP and CP using the case-control matching procedure showed that some differences between these two groups were more pronounced, while others, not present in the classical direct comparison procedure, emerged [3]. Therefore, the current practice of assessing BP with a direct comparison of BP and CP introduces bias, reducing the observed differences between these groups.
Identifying a medical entity with 100% or greater than 50% association with BP would challenge the hypothesis that BP is a consequence of random filling of intrauterine space and the need for a case-control matching procedure in evaluating BP group outcomes. We chose sirenomelia to test the rule that the maximum probability for BP is 50%. Sirenomelia is a complex congenital malformation characterized by the fusion of lower limbs, severe urogenital abnormalities, and Potter’s syndrome with a single umbilical artery [4]. The fetus changes its lie and presentation with brief leg extensions [5] and whole-body movements such as kicking and rolling [6]. Besides appropriate movements for changing its presentation, fetuses also require sufficient intrauterine space for optimal movements [7]. In extreme cases, either the lack of appropriate movements or sufficient intrauterine space is followed by 40%–50% of BP at delivery [8]. Sirenomelia offers the opportunity to examine the combined effect of absent fetal movements (fusion of lower limbs) and lack of intrauterine space (Potter anomaly due to oligohydramnios). So far, presentation at delivery in this rare anomaly has not been analyzed.
The aim of the study was to investigate the probability of BP at delivery among fetuses with sirenomelia. The hypothesis is that the maximum probability for BP in sirenomelia is 50%, regardless of the number of medical entities, each associated with an increased incidence of BP compared to the general population.
A systematic literature search was conducted in SCOPUS from August 2022 backwards to identify case reports diagnosed with sirenomelia at delivery. The search was performed using the keywords “sirenomelia”, “sympus apus”, “sympus monopus”, and “sympus dipus”. Two reviewers independently screened publications by title and abstract to mitigate selection bias. Duplicate articles were initially excluded. Articles met the inclusion criteria based on title and abstract and underwent a full-text review. The search strategy and subsequent steps are presented in the Fig. 1.
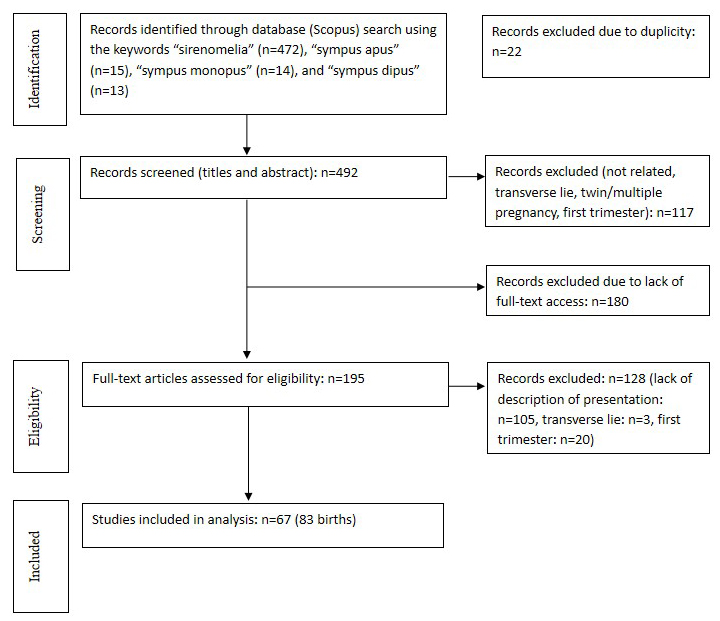 Fig. 1.
Fig. 1.
Research strategy flowchart.
Publications were included if they presented case reports or series of cases involving human subjects and provided information on fetal presentation (BP and CP) in singleton pregnancies at birth. In addition to the term “cephalic presentation”, the terms “uneventful birth”, “unremarkable birth history”, “normal vaginal delivery”, “uncomplicated delivery”, “normal delivery”, “uneventful perinatal”, and “uneventful intranatal period” were considered as CP. Articles were included in the study regardless of their language of publication.
Articles involving twin pregnancies or other multiple pregnancies, as well as those lacking data on fetal presentation or with fetuses in a transverse lie, were excluded. Pregnancies related to the first trimester of gestation were not considered. Articles were excluded if cases were selected solely either on BP or CP.
The data were classified based on several criteria: fetal presentation at
delivery; preterm newborns
A chi-square (
A total of 492 articles were identified in the initial search. The keyword “sirenomelia” retrieved 472 titles from the period 1956 to 2022, “sympus apus” retrieved 15 titles (with 12 duplicates) from the period 1903 to 2022, “sympus monopus” retrieved 14 titles (with 5 duplicates) from the period 1952 to 2002, while “sympus dipus” retrieved 13 titles (with 5 duplicates) from the period 1925 to 2022. Based on abstracts, 117 articles were excluded. Records excluded due to lack of full-text access: n = 180. Available for full-text analysis were 195 articles. Among them, 105 articles lacked a description of the presentation, 3 were excluded due to a transverse lie, and 20 cases were related to the first trimester of gestation. The inclusion criteria were met by 67 articles detailing 83 births relevant to the study [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79]. In 18 cases, CP was determined using keywords unrelated to “cephalic presentation”, as stated in the inclusion criteria [12, 13, 14, 15, 16, 17, 19, 20, 21, 22, 23, 24, 25, 27, 42, 53, 55, 64, 75]. We could not determine from the text whether the birth was at term for three cases [16, 53, 65]. In four cases, it was not possible to define the type of sirenomelia [13, 43, 69, 75]. For eight cases, it was not possible to determine from the articles whether conjoined medical entities existed [21, 22, 43, 51, 52, 55, 56].
In Table 1, the results showed the absence of a statistically significant
difference in the incidence of BP and CP compared to the expected distribution of
50%:50%. No significant difference in the incidence of BP and CP at birth was
observed between prematurely born and term-born newborns with sirenomelia (2
| Category | Breech Presentation No. (%) | Cephalic Presentation No. (%) | Total No. (%) | Chi-square | p-value |
| All cases | 44 (53.01%) | 39 (46.99%) | 83 (100%) | 0.300 | 0.583 p |
| Premature birth | 25 (55.56%) | 20 (44.44%) | 45 (100%) | 0.556 | 0.456 p |
| Term birth | 17 (48.57%) | 18 (51.43%) | 35 (100%) | 1.972 | 0.866 p |
| Sympus apus | 15 (51.72%) | 14 (48.28%) | 29 (100%) | 1.966 | 0.853 p |
| Sympus monopus | 6 (40.00%) | 9 (60.00%) | 15 (100%) | 0.600 | 0.439 p |
| Sympus dipus | 21 (60.00%) | 14 (40.00%) | 35 (100%) | 1.400 | 0.237 p |
| With additional entities | 16 (61.54%) | 10 (38.46%) | 26 (100%) | 1.385 | 0.239 p |
| Without additional entities | 23 (46.94%) | 26 (53.06%) | 49 (100%) | 0.184 | 0.668 p |
In 26 cases, 31 additional medical entities were identified, each individually
increasing the incidence of BP compared to the general population. These entities
included 4 cases of spina bifida, 6 cases of sacral agenesis, 16 cases of
stillbirth, 3 cases of omphalocele, 1 case of hydrocephalus, and 1 case of
unicornuate uterus. There was no significant difference in the incidence of BP
and CP at birth between the group with and without additional medical entities (2
This study, along with others mentioned earlier [1, 2, 3, 8], confirms the rule that the maximum probability for breech presentation in any medical entity is 50% whether examining individual medical entities, different series of the same medical entity, repeated pregnancies in the same conditions, or when several medical entities are simultaneously present. Despite the fact that this study simultaneously observed three and even four medical entities, each with a BP incidence of 30%–40%–50% (fussed legs, Potter anomaly, prematurity and additional medical entities), the incidence of BP did not exceed 50% [8]. This finding is consistent with a previously published study that examined the incidence of BP in the simultaneous presence of twin pregnancies in a double uterus [80].
A limitation of the study is that 18 cases were indirectly determined as CP based on keywords describing the delivery as uneventful or normal. These studies did not explicitly state that the fetus or newborn was in CP. It is possible that in some deliveries considered normal, the fetus was actually in a BP. On the other hand, the omission of CP description at birth (as it is not considered significant for reporting) could lead to a false higher frequency of breech presentation in this study.
The Bernoulli process describes the mathematical abstraction of the coin-flipping statistics. If the probability of an event is 0.5, a large number of attempts will result in a probability close to 50%. When there is a small number of cases in a series, it is possible that all cases will be either in CP or BP. The mathematical expression for this possibility is 1:1/2n, where n is the number of cases in the series. Drawing conclusions from a series with a small number of trials can lead to the erroneous belief that lower limb reduction malformations cause BP in 100% of cases [81, 82].
Previous study has suggested that the fetus may be in CP and BP due to the correlation of its shape with the intrauterine environment [83]. According to this concept, the fetus places its head where there is more space. When the isthmic part of the uterus is more spacious, the fetus is in CP, and when the fundal part is more spacious, the fetus takes BP. For a sirenomelic fetus, the head has a larger circumference than the opposite end with fused legs. In accordance with this, the uniform body shape of sirenomelic fetuses should result in 100% either BP or CP. The results of this study support that the correlation between fetal shape and the intrauterine cavity influences fetal lie. When the fetus outgrows the intrauterine cavity, a longitudinally elongated intrauterine cavity dictates the longitudinal situs of the fetus but not the presentation.
As mentioned in the introduction, it is necessary to consider changing current methods of direct comparison of BP and CP due to bias, which results in decreased differences between these two groups. This approach would shed new light on the outcome of BP and suggest new directions in the management of BP.
Further improvement of fetal well-being related to its presentation should also focus on determining the physiological mechanism of why fetuses deliberately take CP between 24–36 WG. This intentional adoption of CP may represent the achievement of the first gross developmental motor milestone. Understanding its physiological process could have significant clinical implications, similar to distinguishing whether someone is walking or not [84].
This study supports the rule that the maximum probability for BP in any medical entity, including sirenomelia, is 50%. The outcome of BP should be evaluated using the case-control matching procedure. This approach would shed new light on the outcome of BP and suggest new directions in the management of BP. Further improvement of fetal well-being related to its presentation should also focus on determining the physiological mechanism of why fetuses deliberately take CP between 24–36 WG.
The datasets analyzed during the current study are not publicly available due to restrictions related to the access of case reports and case series used in our systematic review, as many of these sources are not open access. However, the corresponding author will make all data reported in this paper available upon reasonable request.
MM, BP, SK, AV, JP, IČ, SS take part in concept, method, collecting data, data analysis, discussion, and writing manuscript; MM, SS and SK takes part in statistical analysis. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We sincerely appreciate the insightful feedback and suggestions provided by the peer reviewers.
The research was supported by the Ministry of Science, Technological Development and Innovation of the Republic of Serbia (Contract numbers: 451-03-66/2024-03/200114 and 451-03-66/2024-03/200007).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/j.ceog5111243.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.