


 , Changwei Chen 1, Shujun Chen 2, Ningjie Lu 3, Jing Zhang 3, Yuanyuan Sun 3,4,*
, Changwei Chen 1, Shujun Chen 2, Ningjie Lu 3, Jing Zhang 3, Yuanyuan Sun 3,4,*
1 Department of Pediatrics, The People’s Hospital of Yuhuan, 317600 Yuhuan, Zhejiang, China
2 Department of Pediatrics, Yiwu Maternity and Children Hospital, 322000 Yiwu, Zhejiang, China
3 Department of Pediatrics, The First Affiliated Hospital of Wenzhou Medical University, 325000 Wenzhou, Zhejiang, China
4 Department of Pediatrics, The Quzhou Affiliated Hospital of Wenzhou Medical University (Quzhou People’s Hospital), 324000 Quzhou, Zhejiang, China
†These authors contributed equally.
Abstract
Bronchopulmonary dysplasia (BPD) is the most common chronic respiratory disease in extreme preterm infants, and inflammation is the main contributor that initiates this lung injury. As platelet-related indicators such as platelet-to-lymphocyte ratio (PLR) and platelet-to-neutrophil ratio (PNR) are potential systemic inflammatory biomarkers and it has been shown to be good predictors of lung diseases. The objective of this study was to assess the potential role of platelet-related indicators in early prediction for BPD.
Neonates with gestational ages <32 weeks (w) from two tertiary neonatal intensive care units between January 2019 and April 2022 were included and the association between the platelet-related indicators and BPD were analyzed by logistic regression analysis and receiver operating characteristic curve.
533 preterm infants were admitted, including 165 preterm infants with BPD and 368 preterm infants without BPD. The infants in the BPD group had higher PLR and PNR at birth, lower platelet (P) count at 2 w than those in the without BPD group. The high PLR at birth, high PNR at birth and low P at 2 w were independently associated with the risk of BPD. PLR at birth represented a predictive value for BPD with the area under the curve (AUC) being 0.589, sensitivity was 0.661, and specificity was 0.579 when the threshold was 135.33. PNR at birth represented a predictive value for BPD with the AUC being 0.576, sensitivity was 0.612, and specificity was 0.589 when the threshold was 129.12. P at 2 w represented a predictive value for BPD with the AUC being 0.668, sensitivity was 0.548, and specificity was 0.711 when the threshold was 285.5. The predictive value of the model was improved when including PLR at birth, PNR at birth, P at 2 w, and gestational age, with AUC being 0.798, sensitivity was 0.754, and specificity was 0.737.
Combining PLR at birth, PNR at birth, P at 2 w, and gestational age improved the value in early prediction of BPD.
Keywords
- platelet
- platelet-to-lymphocyte ratio
- platelet-to-neutrophil ratio
- bronchopulmonary dysplasia
- predict
- preterm infants
Bronchopulmonary dysplasia (BPD) is a severe chronic lung disease of extreme preterm infants. Recently, the advances in perinatal care have resulted in reductions in neonatal morbidity and mortality, but the incidence of BPD has not decreased [1, 2]. BPD has been characterized by arrested alveoli and pulmonary vessel development [3]. Infants with BPD may lead to respiratory dysfunction, cardiopulmonary dysfunction, nervous system development retardation and potential death [4, 5]. The therapeutic approaches for BPD, such as non-aggressive ventilator measures, glucocorticoids, diuretics, caffeine and vitamins, are only partly satisfactory [6].
Inflammation is a major contributor to the pathogenesis of BPD [7]. In BPD
patients, the increase of pro-inflammatory cytokines, such as TNF-
In a previous study, we found that NLR at 72 h after birth can be considered as an important early indicator of BPD in preterm infants [24]. However, the relationship between the platelet-related indicators and BPD remains unknown. In this study, we aimed to assess the potential role of platelet-related indicators in early prediction for BPD.
We conducted an observational, retrospective cohort study to evaluate newborns
born at gestational age
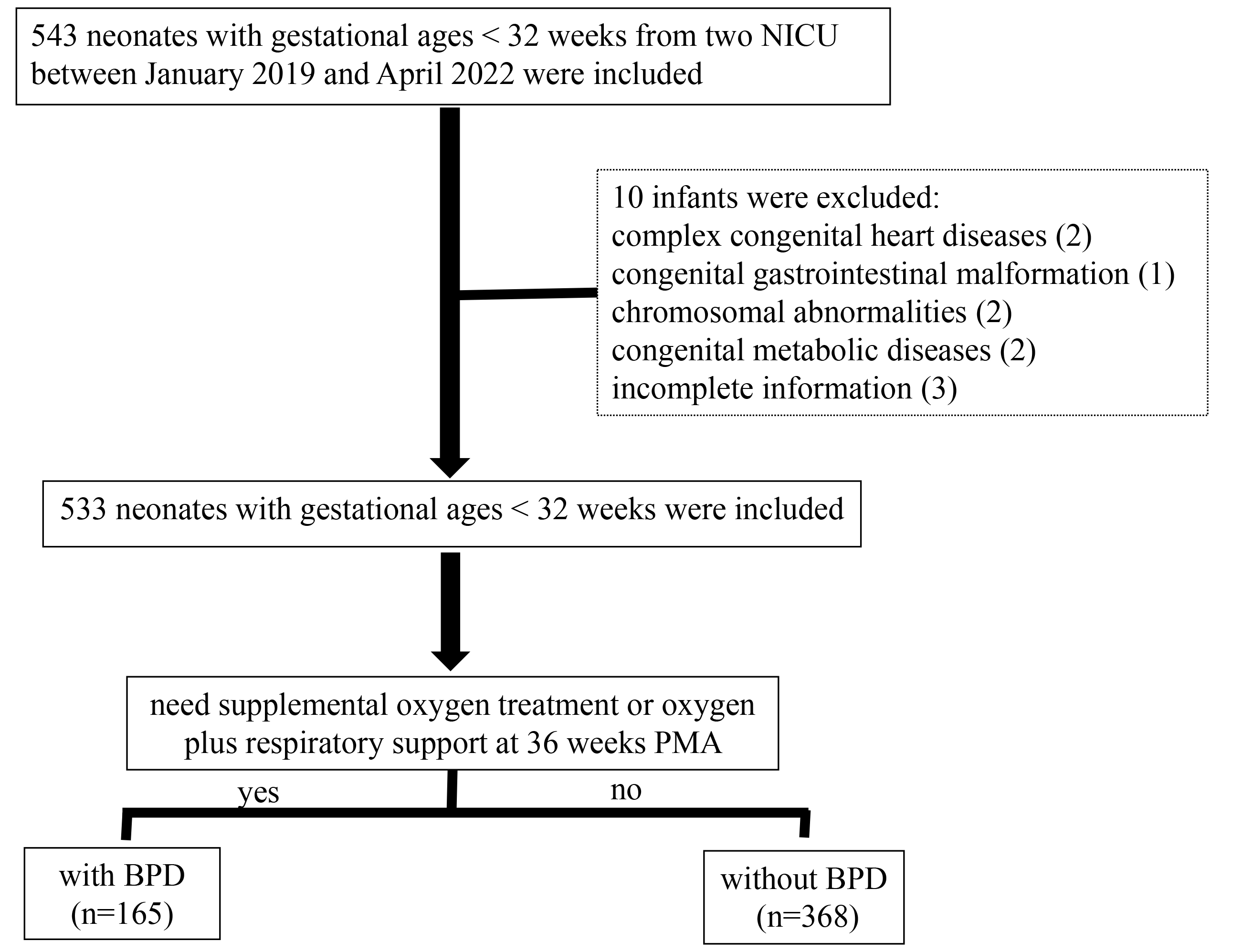 Fig. 1.
Fig. 1.
The flowchart of the study. NICU, neonatal intensive care units; PMA, post-menstrual age; BPD, bronchopulmonary dysplasia.
The data were collected from the hospital electronic medical record system database with the following information collected: sex, gestational age, birth weight, delivery pattern, Apgar score, neonatal respiratory distress syndrome (NRDS), antenatal steroid administration, sepsis, pneumonia, oxygen therapy, mechanical ventilation administration, BPD, retinopathy of prematurity (ROP), intraventricular hemorrhage (IVH), necrotizing enterocolitis (NEC), pulmonary hypertension, duration of NICU stay, comorbidities and maternal health status.
Peripheral blood specimen less than 0.3 mL were harvested from the radial artery or radial vein. Blood samples were placed in standardized tubes containing dipotassium ethylene dinitro tetraacetic acid (EDTA) for complete blood count (CBC). UniCel DxH 800 (Beckman Coulter Inc., Hialeah, FL, USA) was used for CBC analysis. The PLR was calculated as the absolute Platelet (P) count divided by the absolute Lymphocyte (L) count from the CBC. The PNR was calculated as the absolute P count divided by the absolute Neutrophil (N) count from the CBC. The PLR and PNR at birth, 72 h, 1 w, 2 w and 4 w after birth were collected. The standards for blood routine testing referred to our previous study [24].
Statistical analyses were performed by the SPSS 25.0 (SPSS Inc., Chicago, IL,
USA). Continuous variables were presented as the mean
Of the enrolled 533 preterm infants, there were 165 preterm infants with BPD (including 3 who died from respiratory failure within 36 w PMA) and 368 preterm infants without BPD. Baseline demographic and clinical characteristics of the neonates with BPD and without BPD are presented in Table 1. Neonates that were diagnosed with BPD had more unfavorable baseline characteristics compared to neonates without BPD. The gestational age and birth weight were significantly lower in BPD patients and the Apgar scores at 1 min and at 5 min were also significantly lower in BPD patients. The incidence of NRDS, congenital sepsis, and congenital pneumonia were higher in the BPD patients. Days with invasive mechanical ventilation, oxygen therapy, intravenous nutrition therapy and duration of NICU stay were significantly prolonged in the BPD patients.
| Without BPD | With BPD | p | ||
| (n = 368) | (n = 165) | |||
| Male | 207 (56.2%) | 93 (56.3%) | 0.001 | 0.98 |
| Gestational age (weeks) | 30.18 |
28.77 |
10.106 | 0.000** |
| Birth weight (grams) | 1452.45 |
1162.48 |
10.546 | 0.000** |
| Antenatal steroid | 304 (82.6%) | 133 (80.6%) | 0.921 | 0.631 |
| Maternal age (years) | 29.18 |
30.97 |
3.479 | 0.062 |
| Gestational hypertension | 70 (19.0%) | 29 (17.5%) | 10.478 | 0.581 |
| Gestational diabetes mellitus | 77 (20.9%) | 39 (23.6%) | 1.164 | 0.281 |
| In vitro fertilization | 125 (34.0%) | 70 (42.4%) | 3.512 | 0.061 |
| Caesarean delivery | 147 (39.9%) | 53 (32.1%) | 2.975 | 0.085 |
| Apgar score at 1 min | 7.23 |
6.35 |
3.924 | 0.000** |
| Apgar score at 5 min | 9.19 |
8.67 |
4.699 | 0.000** |
| NRDS | 231 (62.7%) | 146 (88.4%) | 36.453 | 0.000** |
| Congenital sepsis | 108 (29.3%) | 74 (44.8%) | 12.173 | 0.001** |
| Congenital Pneumonia | 93 (25.2%) | 88 (53.3%) | 40.000 | 0.000** |
| Invasive mechanical ventilation (h) | 24 (0, 120) | 0 (0, 0) | −7.318 | 0.000** |
| Oxygen therapy (d) | 20.5 (7, 38) | 58 (43, 68) | −14.088 | 0.000** |
| Intravenous nutrition therapy (d) | 15 (10, 23) | 28 (19, 36) | −10.121 | 0.000** |
| duration of NICU stay (d) | 45 (35, 58) | 71 (59, 86) | −12.557 | 0.000** |
**p
The preterm infants in the BPD group had lower P count at 72 h (193.13
| Without BPD | With BPD | T or Z | p | ||
| at birth | n = 368 | n = 165 | |||
| P (109/L) | 232.53 |
225.33 |
1.181 | 0.238 | |
| PLR | 105.61 (66.74, 524.27) | 322.22 (90.60, 594.35) | −3.283 | 0.001** | |
| PNR | 80.49 (41.82, 447.78) | 300.00 (45.99, 544.73) | −2.798 | 0.005** | |
| at 72 h | n = 257 | n = 120 | |||
| P (109/L) | 222.73 |
193.13 |
3.114 | 0.002** | |
| PLR | 94.59 (60.56, 395.39) | 216.60 (70.61, 473.82) | −0.579 | 0.563 | |
| PNR | 82.46 (43.67, 370.62) | 113.56 (41.42, 361.11) | −0.056 | 0.955 | |
| at 1 w | n = 120 | n = 54 | |||
| P (109/L) | 226.27 |
262.71 |
3.944 | 0.013* | |
| PLR | 231.27 (61.59, 729.66) | 269.07 (62.18, 496.63) | −0.888 | 0.375 | |
| PNR | 258.97 (60.23, 687.33) | 323.24 (63.37, 581.97) | −0.374 | 0.708 | |
| at 2 w | n = 334 | n = 142 | |||
| P (109/L) | 300.58 |
237.11 |
5.951 | 0.000** | |
| PLR | 85.53 (56.61, 559.50) | 300.90 (59.33, 524.66) | −1.430 | 0.153 | |
| PNR | 146.00 (76.46, 647.21) | 306.32 (60.95, 789.28) | 1.312 | 0.189 | |
| at 4 w | n = 321 | n = 150 | |||
| P (109/L) | 328.88 |
289.75 |
3.464 | 0.001** | |
| PLR | 99.77 (65.50, 526.04) | 306.32 (60.95, 789.28) | −2.432 | 0.015* | |
| PNR | 244.89 (133.21, 526.05) | 515.79 (125.84, 1021.13) | −0.829 | 0.407 |
*p
| With BPD | ||||||
| B | SE | Wald | p | OR | 95% CI | |
| Gestational age (weeks) | −0.467 | 0.200 | 5.474 | 0.019* | 0.627 | 0.424−0.927 |
| Birth weight (grams) | 0.001 | 0.001 | 0.202 | 0.653 | 1.001 | 0.998−1.003 |
| NRDS | 0.633 | 0.715 | 0.783 | 0.376 | 1.883 | 0.463−7.652 |
| Apgar score at 1 min | 0.108 | 0.101 | 1.142 | 0.285 | 1.114 | 0.914–1.358 |
| Apgar score at 5 min | −0.364 | 0.192 | 3.583 | 0.058 | 0.695 | 0.477−1.013 |
| Congenital sepsis | 0.034 | 0.465 | 0.005 | 0.942 | 1.035 | 0.416−2.572 |
| Nosocomial sepsis | −0.362 | 0.481 | 0.567 | 0.451 | 0.696 | 0.271−1.787 |
| Invasive mechanical ventilation (h) | 0.000 | 0.001 | 0.079 | 0.779 | 1.000 | 0.998−1.002 |
| PLR at birth | 0.001 | 0.001 | 5.984 | 0.014* | 1.001 | 1.000−1.002 |
| PNR at birth | 0.001 | 0.001 | 4.472 | 0.034* | 1.001 | 1.000−1.002 |
| P at 72 h (109/L) | 0.000 | 0.003 | 0.001 | 0.976 | 1.000 | 0.994−1.006 |
| P at 1 w (109/L) | 0.000 | 0.004 | 0.000 | 0.998 | 1.000 | 0.993−1.007 |
| P at 2 w (109/L) | −0.008 | 0.003 | 5.793 | 0.016* | 0.992 | 0.986−0.999 |
| P at 4 w (109/L) | 0.001 | 0.001 | 0.329 | 0.566 | 1.001 | 0.997−1.005 |
*p
The ROC curves of the PLR at birth, PNR at birth and gestational age for the prediction of BPD are shown in Fig. 2 and Table 4. PLR at birth represented a predictive value for BPD with the area under the curve (AUC) being 0.589, sensitivity was 0.661, and specificity was 0.579 when the threshold was 135.33. PNR at birth represented a predictive value for BPD with the AUC being 0.576, sensitivity was 0.612, and specificity was 0.589 when the threshold was 129.12. The most accurate discriminatory gestational age at birth threshold was 30.07 with AUC being 0.749, the sensitivity was 0.601, the specificity was 0.770 for BPD. When combining gestational age with PLR at birth, the AUC was 0.757, the sensitivity was 0.770, and the specificity was 0.628. When combining gestational age with PNR at birth, the AUC was 0.762, the sensitivity was 0.764, and the specificity was 0.629. The predictive value of the model was improved when including gestational age, PLR at birth and PNR at birth with AUC being 0.762, sensitivity was 0.642, and specificity was 0.776. When PLR at birth cutoff was 135.33, PNR at birth cut off was 129.12, gestational age cut off was 30.07, the positive predictive value of BPD was 56.2%.
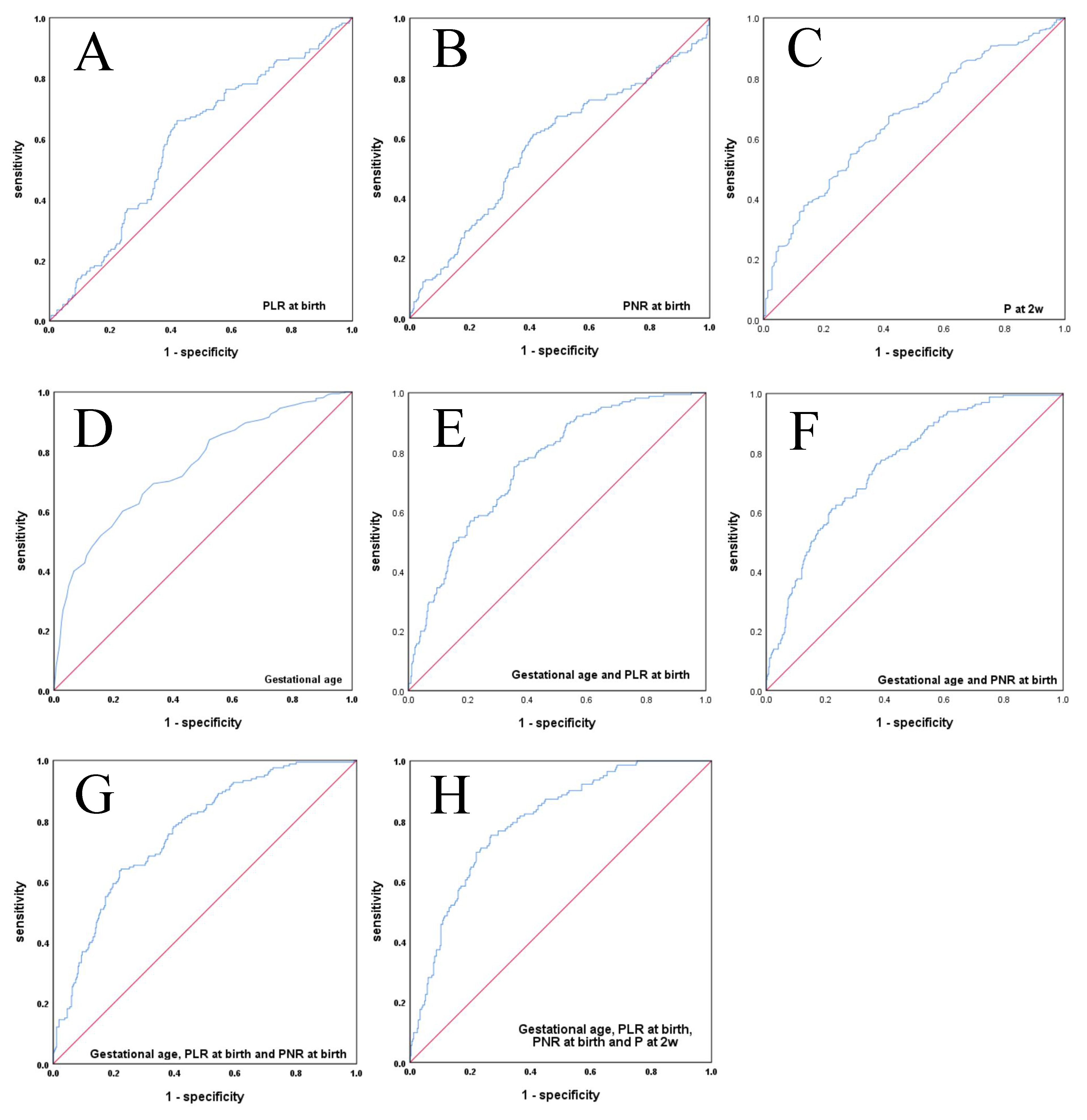 Fig. 2.
Fig. 2.
The ROC curves of the platelet-related indicators and gestational age for the prediction of BPD. (A) The ROC curves of the PLR at birth for the prediction of BPD. (B) The ROC curves of the PNR at birth for the prediction of BPD. (C) The ROC curves of the P at 2 w for the prediction of BPD. (D) The ROC curves of gestational age for the prediction of BPD. (E) The ROC curves of combining gestational age and PLR at birth for the prediction of BPD. (F) The ROC curves of combining gestational age with PNR at birth for the prediction of BPD. (G) The ROC curves of combining gestational age, PLR at birth with PNR at birth for the prediction of BPD. (H) The ROC curves of combining gestational age, PLR at birth, PNR at birth with P at 2 w for the prediction of BPD. ROC, receiver operating characteristic; PLR, platelet-to-lymphocyte ratio; PNR, platelet-to-neutrophil ratio; BPD, bronchopulmonary dysplasia; P, platelet.
| AUC | Sensitivity | Specificity | Cut off Point | p | |
| Gestational age (weeks) | 0.749 | 0.601 | 0.770 | 30.07 | 0.000** |
| PLR at birth | 0.589 | 0.661 | 0.579 | 135.33 | 0.001** |
| PNR at birth | 0.576 | 0.612 | 0.589 | 129.12 | 0.005** |
| P at 2 w (109/L) | 0.668 | 0.548 | 0.711 | 285.50 | 0.000** |
| Gestational age and PLR at birth | 0.757 | 0.770 | 0.628 | 30.07 and 135.33 | 0.000** |
| Gestational age and PNR at birth | 0.762 | 0.764 | 0.629 | 30.07 and 129.12 | 0.000** |
| Gestational age, PLR at birth and PNR at birth | 0.762 | 0.642 | 0.776 | 30.07, 135.33 and 129.12 | 0.000** |
| Gestational age, PLR at birth, PNR at birth and P at 2 w | 0.798 | 0.754 | 0.737 | 30.07, 135.33, 129.12 and 285.8 | 0.000** |
**p
Furthermore, P at 2 w represented a predictive value for BPD with the AUC being 0.668, sensitivity was 0.548, and specificity was 0.711 when the threshold was 285.5. When combining gestational age, PLR at birth, PNR at birth and P at 2 w, the AUC was 0.798, the sensitivity was 0.754, and the specificity was 0.737. When PLR at birth cutoff was 135.33, PNR at birth cut off was 129.12, P at 2 w cut off was 285.8, gestational age cut off was 30.07, the positive predictive value of BPD was 64.6%.
The clinical outcomes of this cohort stratified by the PLR at birth, PNR at
birth and P at 2 w are presented in Table 5. Besides the effect on the occurrence
of BPD, the occurrences of NEC, pulmonary hypertension, IVH grade 3 or 4,
retinopathy of prematurity (ROP) requiring intervention, and death of infants
with PLR
| PLR |
Except PLR |
p | ||
| BPD | 58 (53.21%) | 107 (25.23%) | 31.794 | 0.000** |
| NEC | 11 (10.09%) | 3 (0.71%) | 26.299a | 0.000** |
| Pulmonary hypertension | 11 (10.09%) | 5 (1.17%) | 23.654 | 0.000** |
| IVH grade 3 or 4 | 8 (7.34%) | 2 (0.47%) | 18.641a | 0.000** |
| ROP requiring intervention | 8 (7.34%) | 3 (0.71%) | 15.73a | 0.000* |
| Hospital Stay | 57.16 |
55.61 |
5.817 | 0.000** |
| Death | 6 (5.50%) | 2 (0.47%) | 11.647a | 0.001* |
a, corrected
BPD is a severe clinical syndrome of lung injury that impedes alveolarization and microvascular development in preterm infants. Inflammation, caused by hyperoxia, chorioamnionitis and postnatal infection, is the main factor that initiates lung injury and contributes to BPD in preterm infants. It is clear that inflammation-related signaling pathways, such as NF-kB, Toll-like receptor 4, interferon, and pro-inflammatory cytokines are associated with the development of BPD [25, 26]. Platelets, small anucleate cellular fragments that are released by megakaryocytes, are critical for inflammatory and immune responses. Platelets have been shown to influence leukocyte recruitment and cytokine response [27], to limit bacterial growth and dissemination [28], to influence activation of the vascular endothelium and the coagulation system [29], and to shape immune responses to pathogens and tumor cells [30]. During the development of sepsis, platelets are one of the first cells to respond when the pro-inflammatory and pro-coagulant mechanisms are disrupted [28, 29]. In an inflammatory model, researchers found that many interactions of platelets with the leading edge of adherent neutrophils, and recruited neutrophils searched for activated platelets to initiate inflammation in the early phase [31]. Looney et al. [32] reported that it is vital for the coordinated interactions between neutrophils and platelets in the lung microcirculation of acute lung injury and the elimination of platelets in the blood significantly reduced lung damage in a preclinical study.
Inflammation plays a key role in lung development in extremely preterm infants
and is a major contributor to the pathogenesis of BPD. The lung has been
confirmed to be a primary site of terminal platelet biogenesis with approximately
10 million platelets per hour [33]. Thrombocytopenia is associated with a more
disturbed host response [34]. Therefore, we speculated that the platelet count
may be related to the outcomes of BPD. In our study, we found that the
significant decrease in P counts at 72 h, at 2 w and at 4 w and the significant
increase in P counts at 1 w in infants with BPD, which associations may be due to
inflammation in the pulmonary and peripheral blood. However, Chen et al.
[35] found that the platelet counts at birth were higher in 115 preterm infants
who were delivered at a gestational age
Recently, a number of studies have shown that platelet-related indicators can be used as prognostic biomarkers for a variety of diseases [11, 12, 13, 14, 15, 16, 17, 18]. Several studies demonstrated the significance of PLR and PNR in evaluating and predicting the severity of systemic inflammation, infections, immune and neoplastic diseases [19, 20, 21, 22, 23]. Studies also demonstrated that the PLR as an inflammatory marker along with NLR, which provides information about the disease activity and severity in early onset sepsis [36] and cancer [37]. Yun et al. [38] demonstrated that PNR and PLR as novel inflammatory biomarkers could predict the clinical outcome after aneurysmal subarachnoid hemorrhage. Liao et al. [23] clarified that peripheral blood parameter of NLR and PNR have good applied value in the diagnosis of neonatal pneumonia with high sensitivity and specificity. Similarly, inflammation and immune response depend on N, P and L counts in BPD patients. In our previous study, we confirmed that the higher NLR at 72 h after birth can be considered as an early indicator of BPD [24]. Accordingly, we speculated that the platelet-related indicators may be associated with BPD. In this study, we confirmed that the value of PLR at birth and PNR at birth were higher in preterm infants with BPD, while PLR at birth and PNR at birth were independently associated with the risk for BPD. When combining gestational age with PLR at birth and PNR at birth, the sensitivity and specificity for predicting BPD were improved. At the same time, we found that P at 2 w in infants with BPD was lower than that in infants without BPD, suggesting that it could be used as an independent predictor of BPD. When combined with PLR at birth, PNR at birth, P at 2 w, and gestational age, the sensitivity of the diagnosis of BPD was increased.
Severe complications such as NEC, pulmonary hypertension, IVH and ROP are often
associated with premature infants, which can lead to poor prognosis. In this
study, we observed a correlation between PLR and severe adverse complications.
The occurrences were higher for adverse outcomes such as NEC, pulmonary
hypertension, IVH grade 3 or 4, ROP requiring intervention, and death of infants
with PLR
The main advantage of our research is that platelet-related indicators are easily accessible with no extra expense in the clinic practice. However, the present study has some limitations. The specificity and sensitivity of the indicators are not the strongest, and it is necessary to combine gestational age and other indicators to predict BPD. Meanwhile, the subjects were relatively few and the potential residual confounding could not be eliminated in the data from the regional two-centers. A larger number of subjects and multicenter studies are required to confirm the findings in the present study.
We confirmed that the platelet-related indicators PLR at birth, PNR at birth,
and P at 2 w combined with gestational age, might be considered as a significant
indicator of BPD. Furthermore, the occurrence rates were higher for
adverse outcomes with PLR at birth
BPD, bronchopulmonary dysplasia; PLR, platelet-to-lymphocyte ratio; PNR, platelet-to-neutrophil ratio; NICU, neonatal intensive care units; AUC, area under the curve; NLR, neutrophil-to-lymphocyte ratio; EBR, eosinophil-to-basophil ratio; NEC, necrotizing enterocolitis; PMA, post-menstrual age; EOS, early-onset sepsis; NRDS, newborn respiratory distress syndrome; ROP, retinopathy of prematurity; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; EDTA, ethylene dinitro tetraacetic acid; CBC, complete blood count; N, neutrophil; L, lymphocyte; P, platelet; ROC, receiver operating characteristic; W, week; SE, standard error; 95% CI, 95% confidence interval; OR, odds ratio; SD, standard deviation.
The research data was uploaded as a file of supplementary materials. All data reported in this paper will also be shared by the corresponding author upon request.
XZ and YS designed the research study. CuiC and JZ performed the research. ChaC analyzed the data. SC and NL collected data and drafted the work. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The research protocol was approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (Ethic Approval Number: No.2020-064) and Yiwu Maternity and Children Hospital (Ethic Approval Number: No.000021), and all of the participants provided signed informed consent.
Not applicable.
This research was funded by Taizhou Social Development Science and Technology Project (21ywb136), Zhejiang Medical Health Science and Technology Project, China (2023KY1293), Zhejiang Medical Association clinical research fund project, China (2024ZYC-B51) and Wenzhou Science and Technology Research Project, China (Y2023003).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/j.ceog5110216.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.