



 , Ayse Kavasoglu Kaya 2
, Ayse Kavasoglu Kaya 21 Faculty of Health Sciences, Department of Physiotherapy and Rehabilitation, Istanbul Medipol University, 34810 Istanbul, Turkey
2 Department of Obstetrics and Gynecology, Camlıca Medipol Hospital, 34696 Istanbul, Turkey
Abstract
Pain and edema in the legs are the most common problems in pregnancy. This study examined the effect of percussion massage therapy applied to the lower extremities on pain, edema, and quality of life in pregnant women.
Sixty pregnant women between 24 and 36 weeks of pregnancy were included in the study. Pregnant women were randomly divided into two groups: the percussion massage treatment (PMT) group (n = 30) and the control group (n = 30). Twelve sessions of percussive massage therapy were administered to the bilateral medial gastrocnemius, lateral gastrocnemius, peroneus longus, and tibialis anterior muscles of pregnant women included in the PMT group, three times a week for four weeks. The lower extremities of the pregnant women in the control group did not get any massage therapy. A Visual Analog Scale (VAS) was used to assess pain. A tape measure was used to measure the ankle, knee, and thigh circumference. The Fatigue Severity Scale (FSS) was used to evaluate fatigue, and the Short Form-36 (SF-36) was used to assess quality of life.
When comparing pre-treatment and post-treatment results within each group, statistically significant differences were found in both groups in terms of right/left ankle, knee, and thigh circumference measurements, and SF-36 physical function (PF) measurements (p < 0.05). When the difference measurements between the groups were compared, a statistically significant improvement in the PMT group was detected in VAS (p = 0.000), right/left ankle (p = 0.002/p = 0.006) and right/left hip circumference measurements (p = 0.006/p = 0.008), FSS (p = 0.009), and SF-36-role emotional (RE) (p = 0.000), mental health (MH) (p = 0.005), social function (SF) (p = 0.005), and body pain (BP) (p = 0.003) measurements.
PMT was more effective than the control group in parameters such as pain, ankle and thigh circumference measurements, fatigue, and some sub-parameters of quality of life. PMT could be preferred to enhance the quality of life of pregnant women by improving parameters like pain, edema, and fatigue.
The study protocol was registered at ClinicalTrials.gov https://clinicaltrials.gov/ (NCT06338254).
Keywords
- percussion massage therapy
- vibration
- pregnancy
- pain
- edema
- quality of life
Pregnancy is a natural process of approximately forty weeks that begins with fertilization and ends with the birth of the fetus. Physiological, anatomical, and hormonal changes occur throughout the body to maintain physical and metabolic balance during pregnancy. These adaptive changes appear as pain due to the change in the center of gravity, musculoskeletal disorders, and soft tissue edema [1, 2].
Pain during pregnancy is mostly seen in the waist, pelvic, and leg regions. Lumbar lordosis and increased anterior pelvic tilt of the pelvis cause knee and ankle extension. Knee problems manifest as ligament laxity in the knee increases in the second trimester of pregnancy [2]. In a study, it is stated that the risk of musculoskeletal problems during pregnancy is increased by changes in hormones and physiology changes on by pregnancy. While this pain causes pain in all lower extremity muscle groups, the gastrocnemius muscle is often affected [3]. Studies indicate that pregnant women experiencing pain in their lower extremities and lower back who receive education and physical therapy during their pregnancy experience reduced pain and impairment [4]. Stretching, self-mobilization techniques, back strengthening, and postural changes are all included in physical therapy. By stimulating certain body areas, soft tissue massage is a type of physiotherapy that helps relieve a variety of aches and pains, as well as tension, exhaustion, and illnesses, intending to revive the body’s vital energy circulation [5].
Another important condition frequently encountered during pregnancy is edema. During pregnancy, the body physiologically retains water and sodium due to the increase in circulating plasma volume, decrease in osmolarity, and changes in hormones. The resulting increase in extracellular fluid causes pathological edema [6]. In addition, as the uterus grows, it puts pressure on the inferior vena cava, causing edema in the lower extremities. One-third of the edema is in the lower extremities and they encounter this complaint more in the last trimester [7]. Gimunová et al. [8] reported that 95.5% of 140 pregnant women had foot edema. Also, an increase in lower extremity and ankle circumference due to edema was observed in 83% of pregnant women [8]. In pregnant women, the severity of symptoms such as night cramps, bloating, pain, and fatigue may increase due to edema in the lower extremities [9]. Women with leg and foot edema can be treated non-pharmacologically using leg elevation, relaxing, immersion in water, bandaging, compression stockings, foot massage, intermittent pneumatic compression, reflexology, and interstitial fluid movement monitoring [10]. Foot massage is a typical non-pharmacological technique used by medical professionals [11]. Research by Rahimikian et al. [12] demonstrated the efficacy of foot massage therapy in lower extremity physiological edema in pregnant women. The therapy of physiological lower leg edema during pregnancy is not well supported by research at this time.
Pregnancy fatigue may occur due to physiological and psychological factors. Stress and sudden mood changes can cause psychological fatigue. In a psychological context, the working environment and socioeconomic factors affect the level of fatigue [13]. Fatigue, which is excessive in the first trimester of pregnancy, decreases in the second trimester and recurs in the third trimester. Fatigue, edema, and pain during pregnancy play an important role in the quality of life. These symptoms negatively affect the quality of life of pregnant women by restricting their daily life activities and functionality [14].
Percussion massage therapy (PMT) combines traditional massage and vibration therapy principles and provides rhythmic movement and pressure application to the body [15]. Percussion massage therapy produces various results such as increasing body temperature, increasing joint range of motion, accelerating blood and lymphatic flow, and reducing muscle tension and/or stiffness. In percussion massage therapy, proprioceptive stimuli are increased by stimulating the Golgi tendon organ with vibration [16]. Studies have emphasized that percussion massage is a new treatment method that is effective for lower extremity pain and has become widely used recently [15, 16, 17]. In a study, it was stated that individuals who received percussion massage therapy experienced a decrease in perceived pain level and that the use of PMT in addition to the treatment increased the effectiveness of the treatment [17]. There are studies on percussion massage therapy, but they are limited in number [18]. There are almost no studies using PMT on pregnant women. Also, studies on methods used to reduce lower extremity pain and edema in pregnant women are very limited. We believe that percussion massage therapy applied to the lower extremities is an important practice as it can be an alternative approach to symptoms such as pain, edema, and fatigue problems that may occur in the lower extremities during pregnancy. The study aimed to examine the effect of percussion massage therapy applied to the lower extremities on pain, edema, fatigue, and quality of life in pregnant women.
This study was a randomized, controlled, single-blind trial with participants allocated (1:1) to one of two groups. The Non-Interventional Ethics Committee of Istanbul Medipol University in Turkey gave its approval for this trial (File number: E-10840098-772.02-5416, Number:783, date:13/09/2022). The study’s protocol was registered at ClinicalTrials.gov https://clinicaltrials.gov/ under the number NCT06338254. Every participant gave written consent and signed an information sheet, and the research was carried out by the Declaration of Helsinki’s principles.
The study was conducted at the Gynecology and Obstetrics Clinic of Istanbul Medipol University Hospital. Data were collected from September 2022 to June 2023. Pregnant women who participated in the study by the inclusion criteria were informed about the study and volunteered. The study comprised sixty pregnant women who were between 24 and 36 gestational weeks. Pregnancy between the ages of 18 and 40, being in the 24–36 weeks gestation stage, not being at risk of becoming pregnant, having a singleton pregnancy, complaining of lower extremity pain or edema, and offering to participate in the study three days a week were the inclusion criteria. Multiple pregnancies, anemia during pregnancy, circulation issues, cardiovascular illness, chronic orthopedic disease, and orthopedic and vascular diseases related to the feet are the exclusion criteria. Following a screening process that involved sixty-four participants, the study included sixty of those who met the inclusion criteria. The study left out two participants who did not match the inclusion criteria and two participants who chose not to participate (Fig. 1).
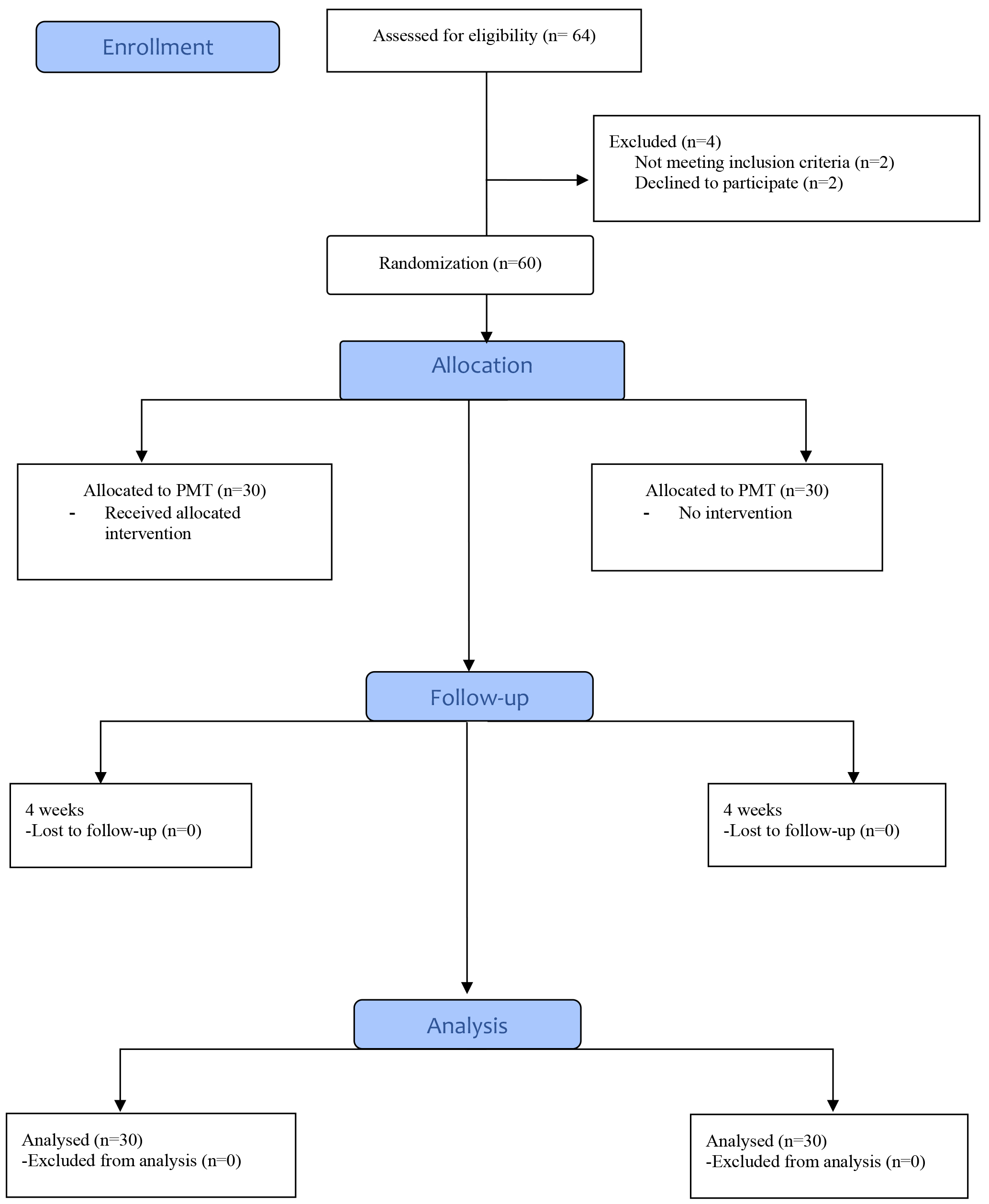 Fig. 1.
Fig. 1.
Flow chart and allocation of the participants, percussion massage treatment (PMT).
Pregnant women were randomly divided into two groups: the PMT group and the control group. Randomization was done with the random.org website. The order in which women were included in the study determined the number assigned to them. Using the randomizer.org website, sixty numbers were distributed at random to divide the individuals into groups based on the order in which they were included in the study. Blinding the participants to group allocations, evaluations, and interventions was done.
The pregnant woman underwent a total of twelve sessions of percussive massage therapy, which was administered to both lower limbs for four weeks. Percussion massage therapy was performed with the flat type head of the Hypervolt (Hyperice, Irvine, CA, USA) device. Pregnant women were asked to lie on an exercise bed for the duration of the treatment. The gadget was utilized at medium speed (level 2, range: 33–40 Hz) for expectant mothers. The researcher physiotherapist did percussion massage to both extremities for five minutes each at different times using the Hypervolt equipment (Fig. 2). The study concentrated on the medial gastrocnemius, lateral gastrocnemius, peronus longus, and tibialis anterior muscles. From posterior to anterior muscle groups, percussion massage was administered longitudinally, moving from distal to proximal and back to distal. For every muscle, the percussion massage began on the medial side and finished on the lateral side. Every muscle received the same amount of time and pressure.
 Fig. 2.
Fig. 2.
Hypervolt device.
No massage therapy was applied to the lower extremities of the pregnant women in this group. Pregnant women were asked to continue their routine check-ups.
VAS is one of the most accurate instruments for measuring pain. It appears frequently in literary works. It applies to adult patients in both healthy and diseased conditions. It is completed easily and in a short time by the participants. The VAS has a line length of 10 cm and consists of a single item. 0 in this line denotes “I have no pain”, and 10 at the end denotes “worst pain”. On a 10-point scale, participants were asked to rate their level of discomfort [19].
A measurement of circumference is used to assess lower extremity edema. Calculating extremities volume is often done by circumference measurement. A non-flexible tape measure was used to take the measurement. When measuring, great care was taken to avoid compressing the tissues. On his back, the patient should be in a comfortable position. Using a tape measure, the width of the calf and thigh, the midline of the patella for the knee, and the medial and lateral malleolar areas for the foot were measured. The physiotherapist used his left hand to hold the portion of the tape measure that displayed the number zero, while his right hand encircled the measurement point, and edema assessments were taken [20].
It involves assessing the degree and timing of fatigue as well as how it affects a person’s day-to-day activities. It addresses how tired each person was during the previous month. There are nine questions in all, with each item on the scale having a score between 1 and 7. All scores were averaged arithmetically. An average of four or more indicates fatigue and an average of more than six indicates chronic fatigue [21]. The validity and reliability of the Fatigue Severity Scale were done by Armutlu et al. [22].
The 36-item test analyzes eight subheadings to determine the degree of quality of life. It comprises assessments of social and physical functioning, role constraints brought on by mental and physical health issues, pain, energy, mental and physical health, and lastly, overall health perception. The 12-month evaluation is covered by the second scale question, and the last month is covered by the remaining questions. All of the questions—aside from the fourth and fifth—are Likert-type. Reversing items 1, 6, 7, 8, 9a, 9d, 9e, 9h, 11b, and 11d on the scale yields the score. The range of the score is 0 to 100. 100 indicates excellent health, whereas 0 indicates bad health [23]. The validity and reliability of the SF-36 were done by Kaya and Icagasioglu [24].
Using the G*power sample size (3.1.9.2) tool, the necessary sample size for the
study was calculated to be 52 with 80% power (
The study was completed by including thirty participants in the PMT group and
thirty participants in the control group. Participants were similar in terms of
demographic characteristics (p
| PMT group (mean |
Control group (mean |
p-value | |
| Maternal age (year) | 30.44 |
34.24 |
0.243 |
| Weight (kg) | 68.64 |
72.98 |
0.345 |
| Height (cm) | 162.55 |
165.08 |
0.126 |
| Gestational age (weeks) | 27.38 |
25.66 |
0.321 |
Abbreviations: PMT, percussion massage therapy; SD, standard deviation.
| Variables | PMT group (n = 30) | Control group (n = 30) | PMT-Control | ||||
| Pre-treat. (mean |
Post-treat. (mean |
p-value | Pre-treat. (mean |
Post-treat. (mean |
p-value | p-diff | |
| VAS | 5.5 |
2.83 |
0.013* | 5.08 |
6.09 |
0.290 | 0.000* |
| Left ankle circ. (cm) | 25.62 |
25.04 |
0.010* | 25.22 |
26.77 |
0.003* | 0.006* |
| Right ankle circ. (cm) | 25.68 |
25.05 |
0.000* | 25.35 |
27.03 |
0.004* | 0.002* |
| Left knee circ. (cm) | 39.00 |
37.61 |
0.003* | 38.52 |
39.20 |
0.003* | 0.573 |
| Right knee circ. (cm) | 39.21 |
39.61 |
0.040* | 36.78 |
38.34 |
0.002* | 0.639 |
| Left thigh circ. (cm) | 50.67 |
45.26 |
0.000* | 48.67 |
50.11 |
0.001* | 0.008* |
| Right thigh circ. (cm) | 51.12 |
46.34 |
0.005* | 49.45 |
50.35 |
0.000* | 0.006* |
| FSS | 4.10 |
3.69 |
0.003* | 4.82 |
5.15 |
0.243 | 0.009* |
| SF-36/PF | 60.83 |
65.55 |
0.042* | 65.55 |
70.83 |
0.007* | 0.143 |
| SF-36/RP | 50.27 |
61.11 |
0.083 | 54.16 |
44.16 |
0.009* | 0.100 |
| SF-36/RE | 50.83 |
62.34 |
0.097 | 55.53 |
40.85 |
0.067 | 0.000* |
| SF-36/Vitality | 51.66 |
62.50 |
0.846 | 47.91 |
46.66 |
0.662 | 0.544 |
| SF-36/MH | 64.22 |
72.66 |
0.009* | 60.00 |
85.00 |
0.709 | 0.005* |
| SF-36/SF | 54.16 |
65.97 |
0.027 | 64.58 |
58.41 |
0.731 | 0.005* |
| SF-36/BP | 49.16 |
63.19 |
0.947 | 42.89 |
38.00 |
0.045* | 0.003* |
| SF-36/GH | 64.72 |
72.22 |
0.009* | 65.00 |
47.91 |
0.800 | 0.384 |
Abbreviations: PMT, percussion massage therapy; SD, standard deviation; treat,
treatment; VAS, visual analog scale; circ, circumference; FSS, fatigue severity
scale; SF-36, Short Form-36; PF, physical function; RP, role physical; RE, role
emotional; MH, mental health; SF, social function; BP, bodily pain; GH, general
health; diff, difference, *: p
This study showed that the PMT group was significantly more effective than the control group in terms of pain status, ankle, and thigh circumference measurements, severity of fatigue, and quality of life parameters such as RE, MH, SF, and BP in pregnant women. It is uncertain what mechanism explains the efficacy of percussion massage therapy on pregnancy problems. The fact that most studies on percussion massage have only been conducted on men and have mostly concentrated on musculoskeletal diseases and sports performance is one factor contributing to the paucity of information in this field [26]. Almost no research has been done on the effects of percussion massage therapy on pregnancy-related lower limb discomfort, edema, and fatigue. This study showed significant improvements were observed in the parameters of pain, edema, and fatigue in the PMT group compared to the control group.
Not only is there little data regarding the benefits of percussive massage for pain relief and recuperation, but less is known about the physiological processes that underlie the treatment’s purported mechanisms of action. Despite this dearth of research, it is still believed that percussion massage works similarly to soft tissue massage, which is a type of massage in which a therapist applies pressure to a patient’s muscles with their hands, ultimately boosting blood flow, encouraging healing, and lessening pain [15]. Percussion massage therapy attempts to lessen pain by suppressing nociceptive pain fibers and activating afferent alpha and beta motor neurons [27]. One study showed a significant reduction in subjective pain sensations in the lumbar spine with vibration therapy. It has also been stated that as pain decreases, quality of life decreases [28]. Games and Sefton [29] noted that vibration treatment offers a technique that might raise tissue blood perfusion and temperature for women who might not be able to finish the activity due to an injury (such as reduced range of motion, discomfort, or swelling). In pregnant women of the PMT group who received vibration, a decrease in pain, edema, and fatigue and an increase in quality of life were observed in our study. We consider that the stimulation created by vibration on the muscular system through the tonic vibration reflex on the lower extremity contributes positively to the analgesic effect.
A common and painful side effect of pregnancy is dependent physiological lower leg edema, or water retention in the lower limbs’ interstitial space. The condition may result in pain, a heavy feeling, cramping at night, and painful paraesthesia [30]. Massage therapy applied to the feet can be beneficial for some disorders like edema in the legs and feet because it transfers extravascular fluid without disturbing intravascular fluid in pregnant women. In a study, the experimental group had a 20 min foot massage daily for 5 days whereas the control group did not receive any intervention beyond standard prenatal care. The result of this study showed that women in the experimental group had a significantly smaller lower leg circumference (right and left, ankle, instep, and metatarsal-phalanges joint) after 5 days of massage compared with the control group [31]. A study conducted determined that pregnancy therapeutic massage has many benefits in increasing blood flow and circulation. Additionally, it causes the brain to release opioids, which are naturally occurring medications that reduce pain [32]. One systematic review determined that foot massage and stockings reduced leg edema and leg symptoms respectively in pregnancy [33]. In our study as well, it was found that the application of PMT was effective in controlling pain and edema. Percussion massage therapy provides the manipulation of the soft tissue of the foot and it may decrease the physiological edema in the lower extremity in pregnant women.
Common physical symptoms such as edema, muscle cramps, and fatigue, may lead to a decrease in the quality of life in the second and third trimesters of pregnancy. There are studies in the literature about the effect of massage and soft tissue mobilization on reducing pain and edema, but as far as we know, there is no study examining the effect of PMT on pregnant women [31]. It was concluded that these results are likely because massage aids in the healing process from muscle exhaustion by promoting blood and lymph circulation, eliminating waste, and supplying nourishment and oxygen [34]. The biggest influence on women’s perceptions of their quality of life is pregnancy fatigue. Consequently, lowering the perceived levels of weariness should be the main goal of initiatives to enhance women’s quality of life [35]. In one study, women who were depressive throughout pregnancy were randomized to either the control group or the group that received moderate massage therapy twice a week from their spouses from 20 weeks of gestation until the conclusion of the pregnancy [36]. Compared to the control group ladies, the pregnant women who had massages had higher quality of life and fewer self-reported cases of leg discomfort, back pain, despair, and anxiety. According to a systematic review, the data regarding the impact of conservative therapy, such as massage or mild pressure, on pain, disability, and quality of life during both short- and long-term pregnancy is highly ambiguous [37]. Acupressure, aromatherapy, and massage were found to be the most effective non-pharmacological approaches in relieving pain in laboring and pregnant women when compared to standard care, according to a meta-analysis conducted by Hu et al. [38]. The authors concluded that the use of nonpharmacological methods reduces the possibility of adverse effects resulting from the use of pharmaceutical therapies. Another study showed the value of back massage in lowering discomfort during the initial stages of labor in primipara mothers when compared to those receiving routine treatment, and it might be implemented as a regular practice in primary care [39]. In our study, we observed an increase in fatigue and quality of life with the reduction of pain and edema. We believe that the application of PMT enhances blood circulation, thus relaxing the muscles in pregnant women, and reducing the sensation of pain and fatigue. Additionally, it was noticed an improvement in their quality of life, particularly in general body pain, mental health, and general health parameters. It can be stated that PMT applied to the lower extremities is one of the methods of coping with some difficulties (pain, edema, fatigue) experienced in pregnant women. With this study, a different perspective was gained from the current literature regarding pain and edema management in pregnant women. It has been shown that pregnancy complications can be reduced with PMT, which is easy to use in daily routine.
The strengths of the present study are the use of PMT, which has not been used before in pregnant women, and examining its effects on the most common pregnancy symptoms. Another strength is that PMT, which is one of the most popular alternative physiotherapy methods, reveals a different way of using it in pregnant women. The short duration of treatment and the inability to follow up on the long-term results of pregnant women are the limitations of the study.
In pregnant women, PMT was observed to be more effective than the control group in parameters such as pain, ankle and thigh circumference measurements, fatigue, and some sub-parameters of quality of life. PMT is not only an easy and effective method for orthopedic problems but also an alternative method for controlling pain and edema in pregnant women. PMT can be preferred to enhance the quality of life of pregnant women by improving parameters like pain, edema, and fatigue. The use of the Hypervolt device, commonly used by physiotherapists for pain control, is more limited in pregnant women. We anticipate that PMT will be a technological and innovative treatment method for the primary issues experienced by pregnant women. Additionally, the ability of PMT to create a larger impact in short treatment durations and its non-invasive nature will also facilitate its use among pregnant women. We consider that it would be good to conduct more studies on how PMT use will affect the quality of life of pregnant women in future studies.
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
MYM and AKK: protocol/project development, data analysis, validation of data analysis, manuscript writing. MYM: data collection, manuscript editing. Both authors contributed to editorial changes in the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The research protocol was approved by the Non-interventional Ethics Committee at Istanbul Medipol University, Turkey (File number: E-10840098-772.02-5416, Number:783, date:13/09/2022), and all participants provided signed informed consent.
The authors sincerely thank all the individuals of the Clinics of Obstetrics and Gynecology, Istanbul Camlica Medipol Hospital.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.