




1 Department of Gynecology and Obstetrics, The Second Affiliated Hospital of Fujian Medical University, 362000 Quanzhou, Fujian, China
2 Department of Ultrasound, The Second Affiliated Hospital of Fujian Medical University, 362000 Quanzhou, Fujian, China
3 Department of Radiology, The Second Affiliated Hospital of Fujian Medical University, 362000 Quanzhou, Fujian, China
Abstract
Objective: A caesarean scar defect (CSD), a niche in the uterus, is an emerging long-term complication after caesarean section (CS). With rising rates of CS, the risk of post-caesarean iatrogenic complications has increased, although many women may be diagnosed incidentally while asymptomatic. We present a review of the diagnosis and treatment of CSD. Mechanism: We describe the current state of treatment of CSD in terms of diagnosis and the different treatment options. Findings in Brief: The diagnosis can be confirmed by transvaginal sonography, hysteroscopy and other imaging examinations. At present, therapy is dependent on the presence of symptoms, the size of the CSD, and secondary infertility. Non-invasive management includes oral contraceptives and the levonorgestrel-releasing intrauterine system (LNG-IUS), which can improve the clinical symptoms of prolonged menstrual periods to some certain extent. Currently, the principal therapy is surgery, and micro-invasive surgical management includes transvaginal, hysteroscopic and laparoscopic procedures. However, there is no unified surgical selection standard, and the selection of surgical methods and the effect of surgical management are also controversial and need to be further studied. Conclusions: The aim of this review is to summarize and compare the selection of diagnostic and therapeutic methods and the differences in the curative effects of these therapeutic methods for CSD.
Keywords
- caesarean scar defect (CSD)
- non-invasive treatment
- laparoscopy
- transvaginal sonography
- hysteroscopy
Caesarean section (CS) is one of the most frequently carried out surgical operations in modern obstetrics worldwide [1]. In recent decades, the caesarean delivery (CD) rate has increased significantly [2]. This has resulted in a globally increasing discussion of the impact and complications of the procedure [3]. The rates of some of these complications, such as uterine rupture, ectopic pregnancy, placenta previa and stillbirth, are constantly increasing [4]. However, there has been paid more attention to the main long-term complications of CS [1] which is caesarean scar defect (CSD), and obstetrics complication of CSD which are caesarean scar pregnancy and Placenta accrete spectrum disorders.
CSD refers to a myometrial defect resembling a pouch on the uterine incision after CS. More specifically, it is characterized by the separation of the myometrium at the incision of a previous caesarean scar on the lower uterine segment [5]. This defect contributes to the occurrence of symptoms such as abnormal uterine bleeding [6], chronic pelvic pain, caesarean scar pregnancy, dysmenorrhea and secondary infertility [7]. The guidelines for the diagnostic and therapeutic criteria of CSD are still unclear. At present, the treatment choices for CSD include conservative and surgical treatment, such as oral contraceptives, the levonorgestrel intrauterine system (LNG-IUS) and transvaginal, laparoscopic, or hysteroscopic repair.
The aim of this review is to provide a comprehensive and wide overview of the current literature by analysing the diagnosis and medical and surgical management of CSD to provide a reference for the selection of a clinical therapy project.
At present, there are no definitive diagnostic criteria for CSD [1]. The diagnosis is based mainly on the medical history, clinical symptoms and auxiliary examination of patients. Patients with a history of CS have different clinical symptoms, such as chronic pelvic pain, postmenstrual spotting [8], infertility, and scar pregnancy, and some patients may be diagnosed incidentally while asymptomatic. Therefore, auxiliary examination should be further performed. There are currently multiple imaging methods that can be used for the diagnosis of CSD, such as ultrasonography, hysteroscopy, sonohysterography, and magnetic resonance imaging (MRI), which can be applied to evaluate the lower anterior myometrium and make a diagnosis of CSD. A prospective cohort study mentioned that the incidence of CSD was 44.4% at 6 months after CS. In addition, lower abdominal pain and scar pain were more pronounced when CSD was observed in transvaginal sonography (TVS) [9].
TVUS is a simple, low-cost, most common usage and non-invasive examination to evaluate the integrity of the lower myometrium on the anterior wall [10, 11]. During routine scans, the use of a low-resolution ultrasound machine could neglect the pouch. Togas Tulandi et al. [1] reviewed the literature and discovered that the detection rate of CSD can reach 42%–88% when used by TVUS. Cecilia Fabres reported that TVUS was highly 100% correlated with hysteroscopy in the diagnosis of CSD, and the two diagnostic methods have similar positive and negative predictive values [12]. TVUS and sonohysterography showed no significant difference in evaluating and measuring the thicknesses of the residual myometrium, and TVUS examination readily identified this anatomic defect during the period of postmenstrual bleeding [13].
Compared with transabdominal ultrasound, TVUS decreased the limitation of conditions, such as intestinal gas accumulation, degree of bladder filling and fat layer thickness of the lower abdominal wall, and TVUS can more clearly show the shape of the CSD and its adjacency. Three-dimensional TVUS can clearly display the coronal plane, which makes up for the limitation of two-dimensional TVUS (Fig. 1A) and more intuitively and comprehensively shows the lesion morphology (Fig. 1B). Consequently, it is considered to be the preferred method for screening CSD. However, the level of the sonographers and the timing of the examination can easily influence the result of the CSD, especially the missed diagnosis of the smaller CSD.
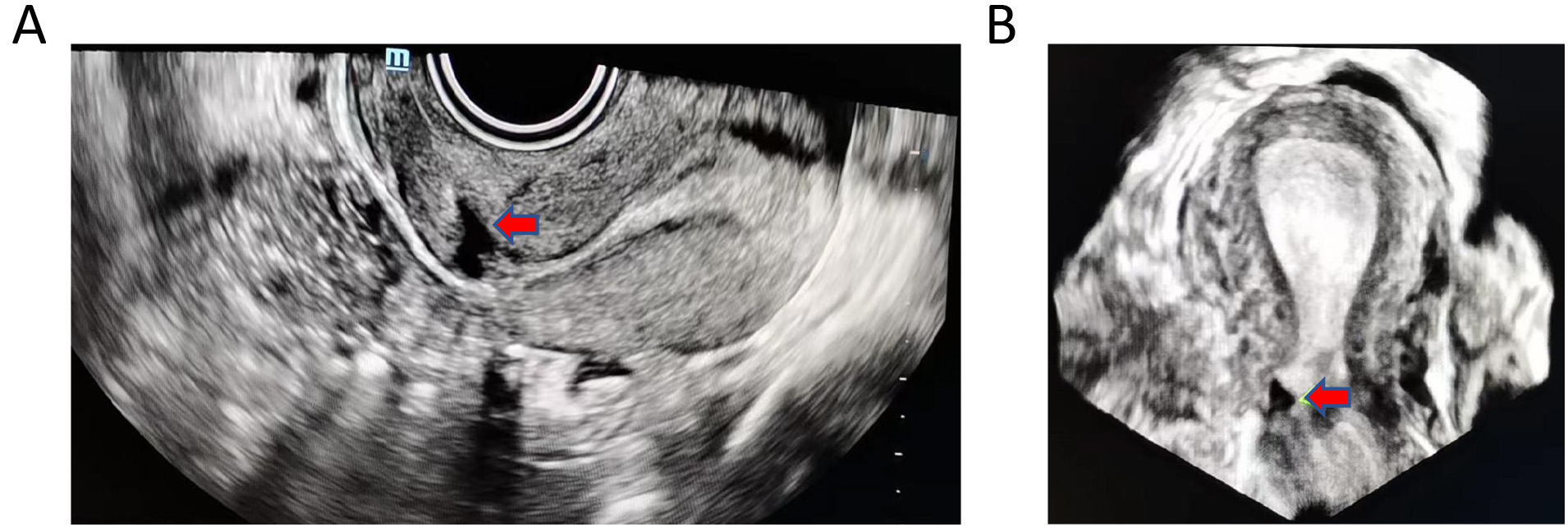 Fig. 1.
Fig. 1.Ultrasound images of CSD. (A) Transvaginal two-dimensional ultrasound. (B) Transvaginal three-dimensional ultrasound. The red arrow indicates the location of the CSD. CSD, caesarean scar defect.
Ultrasound contrast agent is injected into the uterine cavity, and TVUS shows typical wedge-shaped or cystic dark liquid in the lower segment of the uterus. The CSD is more common in SHG than in TVUS, which shows that SHG has higher sensitivity [14, 15, 16, 17, 18]. Interestingly, the scar defect in SHG seems deeper and larger [14, 19]. SHG is classified into saline infusion sonohysterography (SIS) and gel instillation sonography (GIS) according to which ultrasound contrast agent is used. As the contrast agent increases the contrast between the defect and uterine wall, SIS has a higher specificity and sensitivity than TVUS for identifying CSD [20]. One study demonstrated that 56.0% of women with a history of CS had a niche detected by GIS [17]. Van der Voet et al. [19] reported that the niches were visible in all women using GIS at 6–12 weeks after CS, and the prevalence of defects detected by GIS (64.5%) was higher than that detected by TVUS (49.6%). However, some researchers believe that SHG can enlarge defects and thus the size of the CSD [21].
The contrast agent is perfused into the uterine cavity, and the defect is observed on X-ray. The CSD appears as cystic, banded or linear defects on X-ray imaging. HSG can be used to evaluate the CSD, but the width and length of the defect are increased compared with those on ultrasound, and this is associated with the outside pressure during the examination [22]. HSG has some limitations, such as the lack of measurement of myometrial thickness and the accumulation of mucus or blood in the CSD, which can lead to a missed diagnosis of CSD [23]. Consequently, HSG has been gradually replaced by SHG.
Through hysteroscopy, the structure of the CSD can be directly seen in the depression of the uterine incision, such as the “valve” on the incision margin, highly vascularized on the surface, accumulation of old blood or mucus and sometimes the growth of endometrial tissue in the depression. Hysteroscopy is currently considered to be the best method for the diagnosis of CSD due to its direct and clear visualization and potential therapy [12]. Dominguez et al. [24] mentioned that there is gradual agreement to recommend hysteroscopic repair of CSD as the preferred method as long as the residual myometrium is at least 2.5–3 mm. However, it cannot be used to assess the residual myometrial thickness (TRM).
MRI of CSD shows the occurrence of an iso-signal or high-signal on T1-weighted imaging (W1) (Fig. 2A) and a high-signal on T2W1 (Fig. 2B–D). MRI has advantages in the display of soft tissue and clearly images of the site of the CSD and the absence of the myometrium. Additionally, it has the advantages of its non-invasiveness and lack of radiation. Taru Gupta et al. [25] reported that MRI was better than TVUS, but the difference in the rate of CSD identification was not statistically significant. However, the disadvantages of MRI include its high cost and longer examination time, so it is not the best first-choice option to screen for CSD.
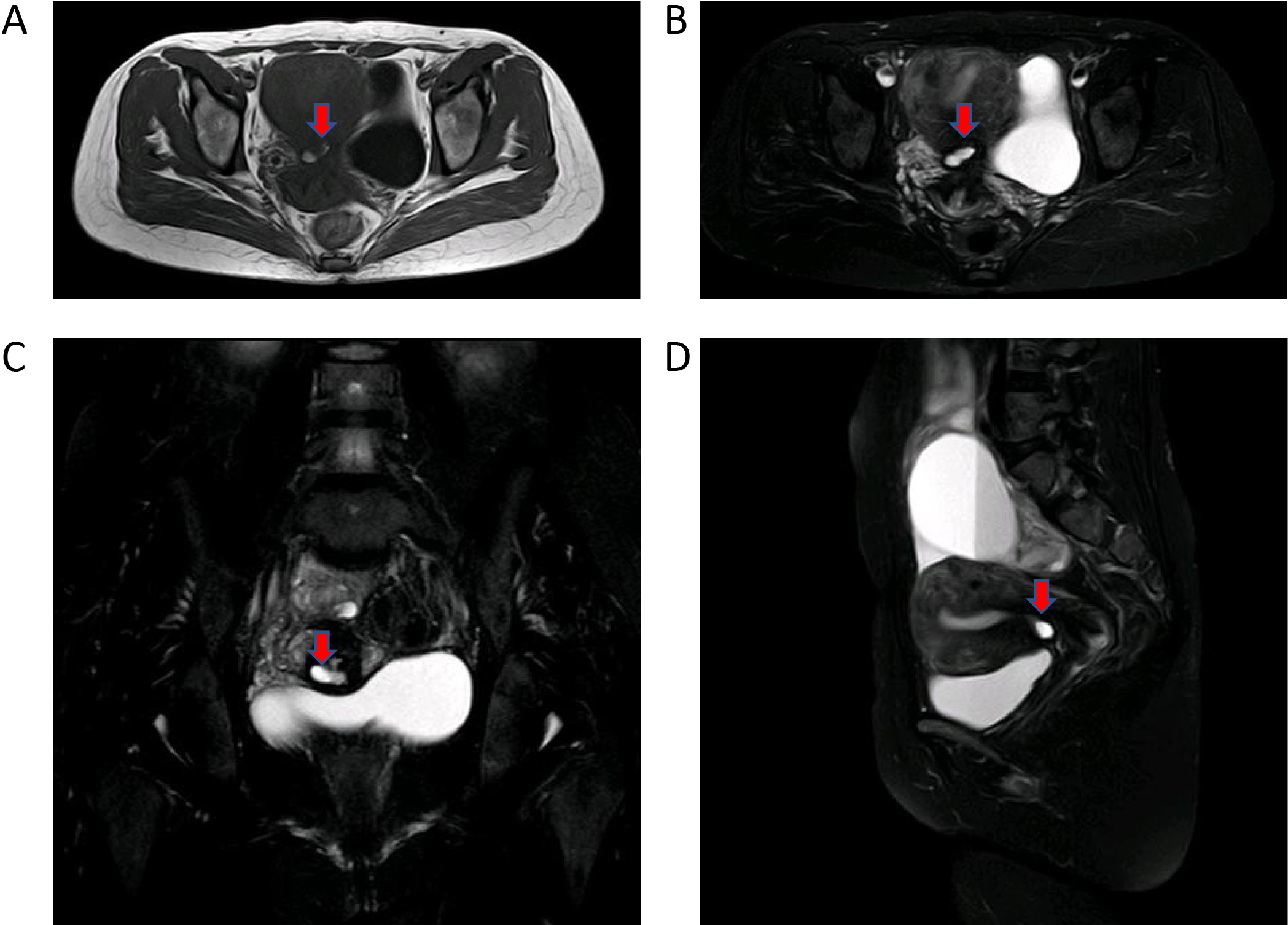 Fig. 2.
Fig. 2.Nuclear magnetic resonance (MRI) images of CSD. (A) Transverse section of the pelvis (T1W1). (B) Transverse section of the pelvis (T2W1). (C) Coronal section of the pelvis (T2W1). (D) Sagittal section of the pelvis (T2W1). The red arrow indicates the location of the CSD. CSD, caesarean scar defect.
Consequently, TVUS is more affordable, is non-invasive and yields reliable results, and it is the best first-choice option to screen for CSD [23]. For some cases, several studies have suggested SIS as a diagnostic tool for planning surgical treatment [6, 26].
The therapeutic options for CSD comprise various regimens depending on the plans for pregnancy, the presence of clinical symptoms, secondary infertility and the willingness to undergo surgery [27, 28]. However, the efficacy of therapy has yet to be ascertained. For the diagnosis of CSD with no plan for pregnancy, routine surgical repair is not recommended [23]. Therapy options for CSD are as follows.
When there is no plan for pregnancy or the patient declines surgery, short-acting oral contraceptives are the typical choices for abnormal uterine bleeding (AUB) as the clinical manifestation. This is a short-term treatment. It can effectively improve the symptoms of AUB but does not heal the defect, so the symptom recurrence and the complications of hormones are still important issues [29].
There are quite a few studies on the application of the LNG-IUS to CSD. Xuyun Zhang et al. [30] performed a prospective evaluation of five methods applied to treat CSD, and the duration of menstruation was similar before and after treatment in the LNG-IUS group. Thus, given this lack of difference, the therapeutic application of the LNG-IUS is inadequate, but the long-term clinical efficacy of the LNG-IUS remains to be determined.
The indication for surgical treatment is a diagnosis of CSD with corresponding clinical symptoms and the experience of therapeutic effects by the patient. Surgical treatment for CSD can prevent recurrence and restore the normal anatomy of uterus after drug cessation. Therefore, there are many studies suggesting different surgical approaches to repair the CSD [7, 27, 31, 32], including laparotomy, hysteroscopy (HP), laparoscopy (LP), transvaginal repair (TVR), and combined HP with LP (LH). Currently, minimally invasive surgery is the most common procedure for CSD. The timing of surgery is generally 2–3 days after the completion of menstruation if menstruation is normal and generally between 7–9 days if bleeding during menstruation is abnormal.
Laparotomy is the traditional surgery for the CSD repair. Because of the large surgical field and ease of operation, it is suitable for CSD with serious adhesions in the pelvic cavity. However, due to its disadvantages regarding the large scale of operative trauma and slow postoperative recovery, it is not the first choice to treat CSD at present.
TVR is performed by dissecting the bladder from the cervix and uterus, exposing
the cervix and lower uterine segment to clarify the position of the CSD,
resecting the defect and suturing the two layers. TVR is a minimally invasive and
effective surgical approach [33]. Zhou et al. [34] suggested that TVR
relieved the symptoms of postmenstrual spotting and anatomically corrected the
scars. Moreover, the optional timing for TVR is an interval
Electric resection is performed by placing the hysteroscope and an electric
resection ring (or an electric rolling ball) into the uterine cavity, and
hysteroscopic electric resection is then performed. HP can remove the upper valve
of the CSD by blocking the outflow of menstrual blood [37]. HP contributes to
alleviating the clinical symptoms of AUB, but it cannot change the anatomic
abnormalities of the CSD [31]. In a retrospective review, Xie et al.
[38] reported that the operative efficacy of HP (64.5%) was significantly
inferior to that of vaginal surgery (93.5%), whereas patients who underwent HP
had a shorter operative time (25 vs. 55 min) and less blood loss (10 vs. 50 mL).
Bingqing Lv et al. [39] compared HP combined with LP to HP alone, and
the results showed similar pregnancy rates between the two methods (61.5% vs.
73.3%; p = 0.505); however, the interval between the operation and
pregnancy was much shorter in the HP group than in the HP combined with LP group
(10 vs. 27 months). One study showed that the effective rate of menstrual
improvement was 59%–100% [40]. Additionally, Florio et al. [26]
stated that bipolar electrocision should be performed when the TRM muscles are
not too thin (
LP has the advantages of a full field of vision, less trauma, shorter operation
time and faster recovery. It has been advocated for defects (TRM
When the CSD does not protrude from the serosa layer, LP does not directly observe the CSD. Thus, LP alone may not completely resect the scar. LH can solve the problems of the poor location ability of LP and incomplete repair of HP for CSD. During HP, the scope of CSD can be identified by the light transmission of the hysteroscope, and suturing of the CSD can be confirmed after laparoscopic repair [23]. During LP, the bladder can be fully pushed down, and the risk of bladder injury can be minimized. In addition, surgical treatment of other pelvic diseases, such as endometriosis, can be immediately performed [50]. LH is better than LP or HP alone, but the disadvantages of LH are its longer operation time and higher cost.
In addition to some of the specialised procedures for repairing CSD mentioned above, there is another type of repairment of CSD when found in a repeated CS. In repeat lower segment caesarean section (LSCS), we found some women with a significant scar defect in the anterior uterine wall (Fig. 3). One prospective study noted that a modified surgical technique concentrated on identification, mobilisation and location of the retracted myometrial fringes by a unique experienced obstetrician [51]. The purpose of this is to make the recovery of anatomical results consistent. The result showed no diverticula in all cases at three months postpartum on pelvic ultrasound. The mean residual scar thickness was 8.4 mm) [51]. In summary, it makes sense to discover and reconstruct the structure of the lower myometrium while repeating the cesarean section.
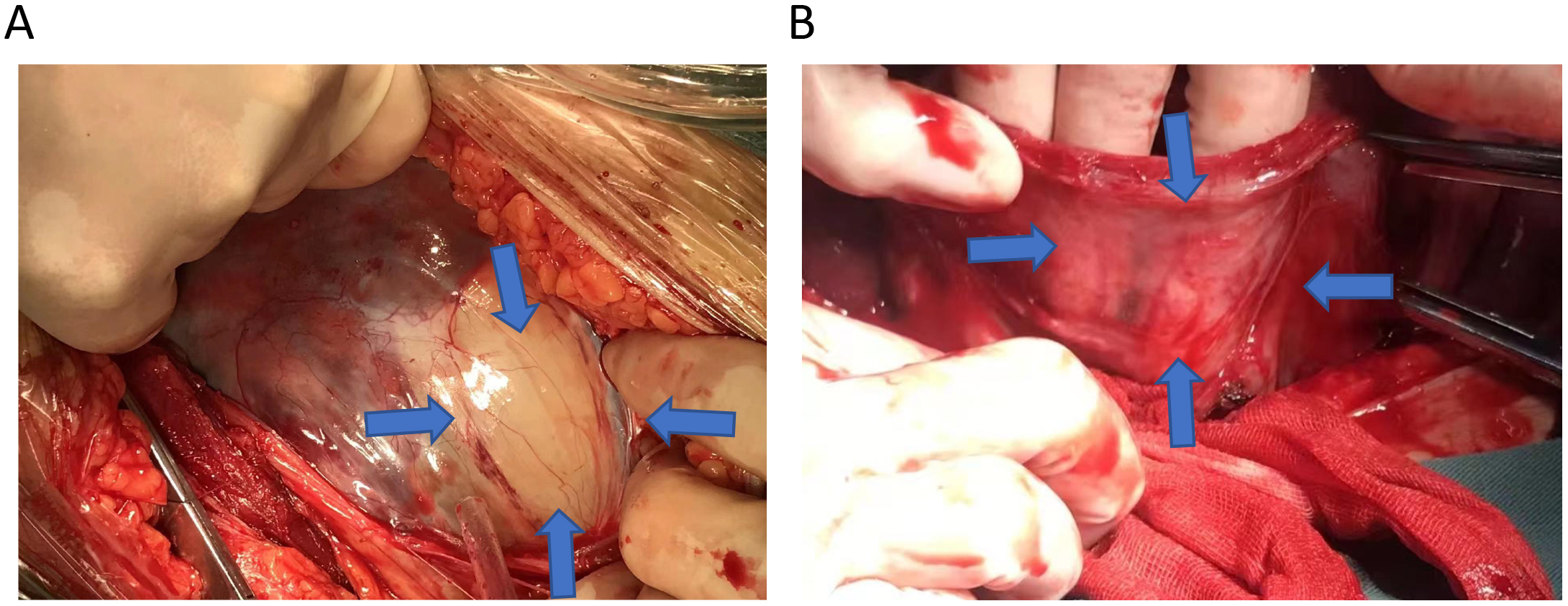 Fig. 3.
Fig. 3.CSD in repeated CS. The blue arrow points to the CSD. (A) The lower segment of the uterus in late pregnancy after opening the abdominal cavity. (B) Lower segment of the uterus after removal of the fetus following incision of the uterus. CSD, caesarean scar defect. CS, caesarean section.
At present, there is still no uniform standard regarding the principles of treatment of CSD worldwide. The following aspects remain controversial: (1) the basis for the diagnosis of CSD on symptoms, imaging or a combination of both; (2) the necessity and duration of pharmacological treatment; and (3) the criteria for selecting different surgical procedures for CSD.
Post-caesarean CSD has become a common clinical condition. The most direct way to reduce the CSD is to reduce the rate of caesarean delivery. The associations between CSD and pelvic pain, dysmenorrhea and infertility requires more study. The most popular therapy appears to be hysteroscopic isthmoplasty. However, the efficacy of laparoscopic or vaginal surgery remains to be seen. These treatments should be considered for specific patients until an optimal treatment for symptomatic women with CSD is identified. At this point, we still need randomized controlled trials to obtain concrete evidence to support effective treatment for CSD.
ZW and YK designed and performed the research study. SL and FH analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This work was supported by the Fujian Provincial Health Technology Project (No. 2019-1-15).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.