





 , Paola Francesca Sagrada 2, Lorenzo Sogaro 1, Serena Migliaccio 1, Marilena Farella 1, Marco Soligo 1
, Paola Francesca Sagrada 2, Lorenzo Sogaro 1, Serena Migliaccio 1, Marilena Farella 1, Marco Soligo 11 Obstetrics and Gynecology Department, Public Hospital of Lodi, 26900 Lodi, Italy
2 Medical Oncology Department, Public Hospital of Lodi, 26900 Lodi, Italy
Abstract
Background: Cesarean Scar Pregnancy (CSP) is a life-threatening
condition following an ectopic implantation within the scar of a previous
cesarean delivery and no guideline is shared about optimal treatment options.
Methods: We present a retrospective study comparing the outcomes of
patients with CSP diagnosed before the 10th week of gestation treated by systemic
or local Methotrexate (MTX) for pregnancy termination, followed by hysteroscopic
placental removal. After MTX administration, the weekly decrease-rate of beta
Human Chorionic Gonadotropin subunit (
Keywords
- cesarean scar pregnancy
- ectopic pregnancy
- hysteroscopy
- methotrexate
- outpatient hysteroscopy
Cesarean Scar Pregnancy (CSP) is an uncommon ectopic pregnancy occurring in about 1 out of 500 women who underwent one or more cesarean deliveries. It is caused by a blastocyst implantation and placental growth within a cervical-isthmic uterine scar [1]. Based on Vial’s classification, two clinical entities known as type 1 and 2 were recognized, depending on different implantation areas and pathways of placental development. In type 1, CSP implantation overlaps with the uterine scar and its growth pursues a cranial direction towards the endometrial cavity. In type 2 the placental development is ventrally-directed, growing within the cesarean scar niche towards the isthmic serous surface and bladder base. In both cases, life-threatening complications such as near-term previa/accreta or uterine rupture in the first months of pregnancy can be expected, respectively [2]. Due to these assumptions CSP termination is widely warranted to avoid maternal morbidity and to spare fertility. To improve the safety of management an early diagnosis of CSP based on established sonography criteria is of pivotal value [3]. No guideline for CSP treatment is currently shared and the choice among many proposed strategies are based on both individual clinical condition and single Institutional skills. Surgical excision by abdominal, laparoscopic, vaginal, hysteroscopic or curettage techniques, pregnancy termination by Methotrexate (MTX) administration, Uterine Artery Embolization (UAE), high-intensity ultrasound, intrauterine double-balloon insertion, as alone or combined treatments, summarized more than 30 procedures proposed to treat CSP [4]. MTX is an antimetabolite drug showing a competitive reversible binding with respect to natural dihydrofolates and acting as inhibitor of the dihydrofolate-reductase (DHFR), a key enzyme synthesizing the tetrahydrofolates needing for synthesis of purine and pyrimidine rings [5]. MTX has been widely used for pregnancy termination in patients with CSP, either by systemic or local administration [4, 5, 6]. This latter option of administration was found to improve the clinical results with respect to the systemic route, although about one third of patient required further treatments [4, 7]. Sequential surgical removal of CSP terminated by MTX or UAE has shown a reduction of treatment failures and adverse outcomes [8, 9]. First pioneered by Wang et al. [10] hysteroscopic removal of CSP was found safe and effective either as primary treatment or after MTX or UAE pregnancy termination [8, 9, 11]. Herein, we report a retrospective study conducted on two series of patients, comparing the clinical outcomes of systemic and local administration of MTX, followed by hysteroscopic placental removal to treat CSP.
The study was conducted at the Obstetrics and Gynecology Department of the
public Hospital of Lodi (Italy) from January 2010 to August 2022. We selected all
patients suffering from CSP that underwent a sequential treatment consisting of
MTX administration followed by hysteroscopic pregnancy removal. The clinical data
was retrieved from both the Institutional data-base and the first Author (GG)
personal file collection of patients suffering from CSP admitted during the study
period. The diagnosis of CSP was made accordingly with recognized Transvaginal
Ultrasound (TVUS) and eco-color Doppler criteria; myometrial thickness of the
uterine scar was not always reported and we did not consider this sonographic
variable for CSP classification [2, 3]. All therapeutic procedures were performed
in accordance with the ethical standards of the national research committee and
with the 1964 Helsinki Declaration with its amendments. Given the retrospective
nature of the study, the lack of guidelines for CSP management and the urgency to
start an effective therapy for pregnancy termination, formal Institutional
Ethical Board approval was not applicable. However, before MTX administration an
approval for the use of an off-label drug was obtained from the Local Health
Authority whereas patient agreement was obtained by a signed informed consent and
a tailored informative note. Until 2017, 50 mg/sqm MTX was administered through a
systemic intramuscular route whereas subsequently, a local hysteroscopy-guided
subchorionic MTX administration by 50 mg/sqm was used in an outpatient clinic
setting, according to a previously described technique. Briefly, using a double
flow 4mm to 5mm operative hysteroscope, we firstly gained the coelomic space of
the gestational sac by opening the capsular decidua and the chorionic membrane.
Thereafter, using a 17-gauge needle adaptable to the operative channel of
hysteroscope, we injected MTX melted in 2 cc of saline within the subchorionic
placental site under vision (Fig. 1) [12]. In all patients the serum level of
Human Chorionic Gonadotropin beta-subunit (
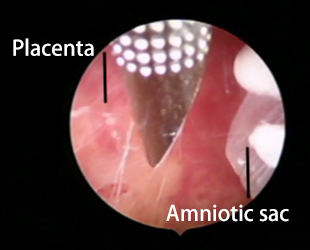 Fig. 1.
Fig. 1.Subchorionic hysteroscopically-guided local MTX administration. The tip of a 17-gauge needle is shown within the coelomic space of a CSP before the injection in the subchorionic space of placental ectopic implantation.
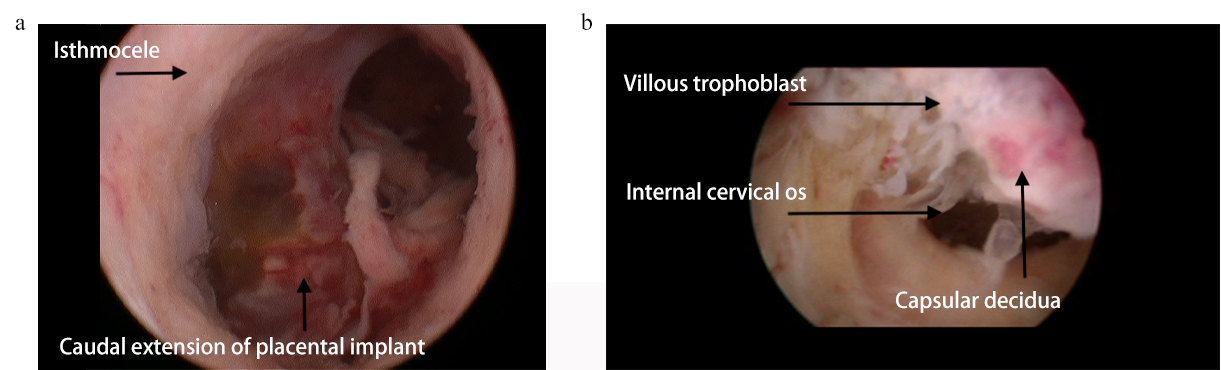 Fig. 2.
Fig. 2.Panoramic view of Type 1 and Type 2 CSP according to Vial’s classification [2]. (a). Type 1 CSP is shown, partially involving the cranial boundary of the cesarean scar niche. (b). the placental implantation within the cesarean scar niche identifies a type 2 CSP.
Parametric baseline characteristics were compared in both groups using
two-tailed Fisher’s exact test. Continuous variables such as patient age and
gestational age, time from MTX administration to the defined drop in
During the study-period, 14 patients suffering from CSP were managed by primary
MTX administration followed by hysteroscopy placental removal. Eight of them
underwent systemic MTX whereas in six patients the MTX priming was accomplished
through an outpatient hysteroscopy-guided subchorionic local injection. This
latter procedure resulted uneventful and easy to accomplish, leading to the
discharge of all patients within a few hours from intervention. The two groups
were similar for all baseline characteristics, as shown in Table 1. In Fig. 3 we
represented the basal
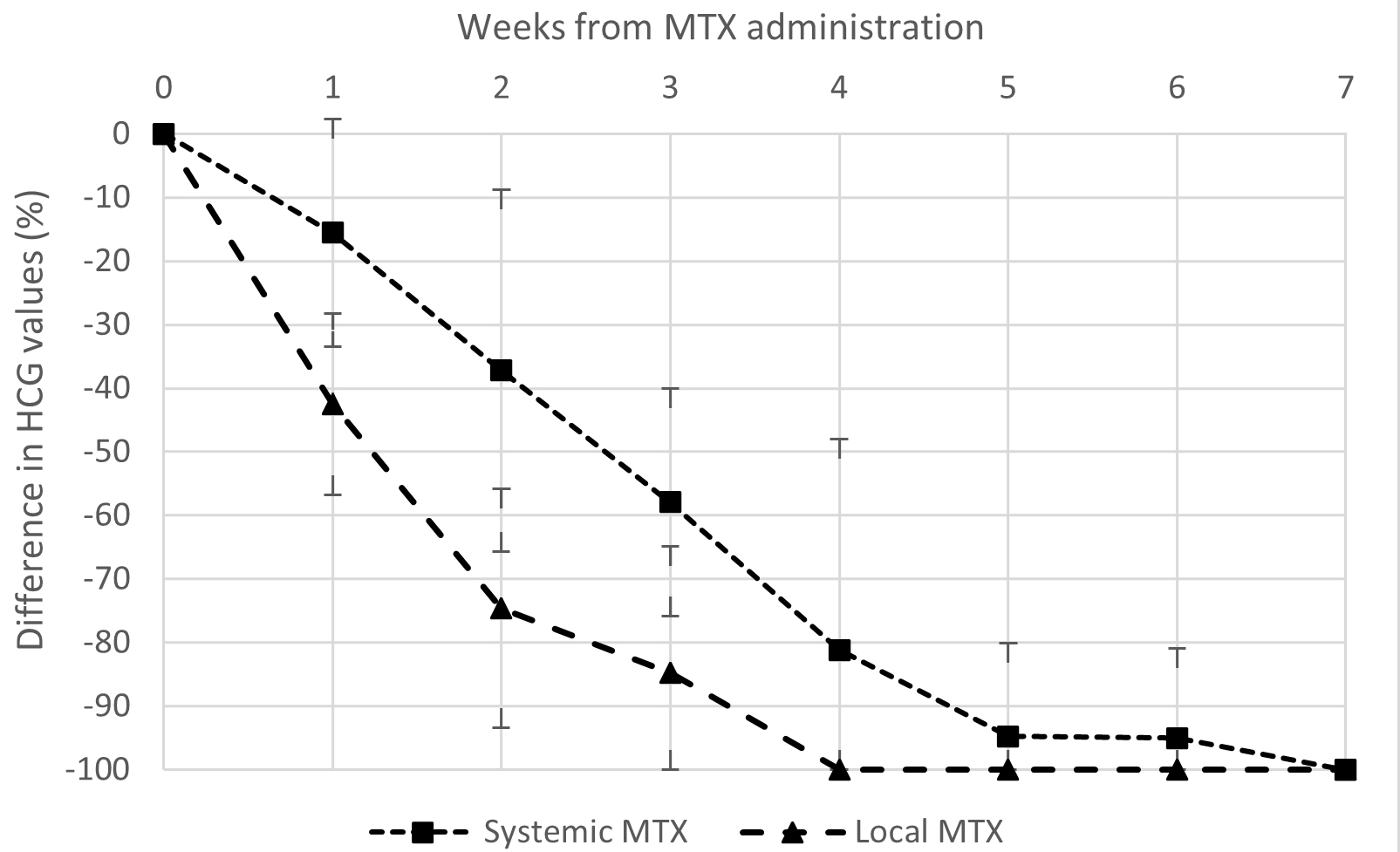 Fig. 3.
Fig. 3.Evolution in time of mean (
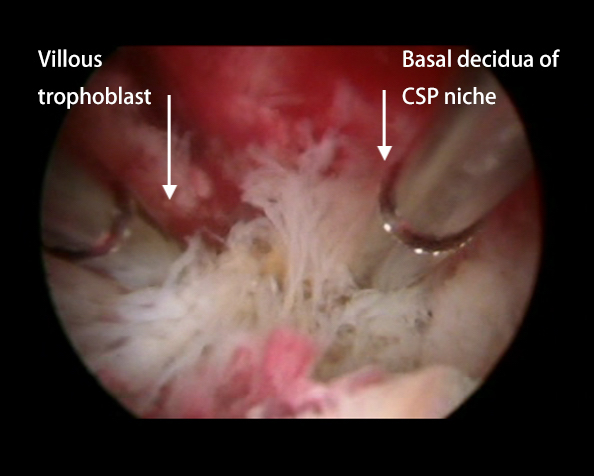 Fig. 4.
Fig. 4.Placental separation. The villous trophoblastic tissue (whitish tissue on the left) separation from basal decidua (pinkish tissue on the right) of CSP, using the cold mechanical action of resectoscopic loop is in progress.
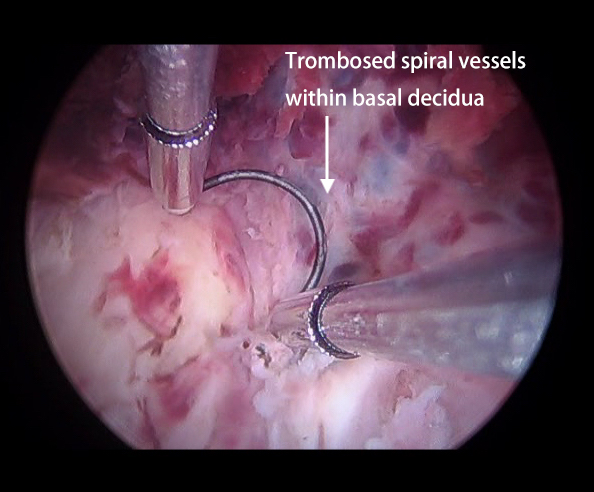 Fig. 5.
Fig. 5.The thrombosed spiral vessels within the niche of type 2 CSP appearing during placental separation below the basal decidua and the lack of an easy plane of separation suggest the diagnosis of concurrent adherent placenta.
| Parameter | Systemic MTX (n = 8) | Local MTX (n = 6) | p-value |
|---|---|---|---|
| Age (years), mean (range) | 33.6 (22–44) | 35.2 (28–42) | 0.7461 |
| Previous CD, % | |||
| One previous CD | 62.5% | 50% | 0.8831 |
| More than one previous CS | 37.5% | 50% | |
| Gestational age (days), mean ( |
48.9 ( |
52.5 ( |
0.5883 |
| CSP type, % | |||
| CSP type 1 | 25.0% | 33.3% | 1 |
| CSP type 2 | 75.0% | 66.6% | |
| Viable pregnancy, % | 50% | 66.6% | 0.6272 |
| Uterine bleeding, % | 62.5% | 33.3% | 0.5920 |
| Outcome | Systemic MTX (n = 8) | Local MTX (n = 6) | p-value | |
|---|---|---|---|---|
| Time from MTX administration to desired drop of |
27.1 ( |
16.3 ( |
0.0056 | |
| Time from MTX administration to hysteroscopy (days), mean ( |
33.4 ( |
20.5 ( |
0.0164 | |
| Need for second dose of MTX, patients number | 3 | 0 | 0.2088 | |
| Operative time (min), mean ( |
26.3 ( |
23.5 ( |
0.7463 | |
| Hemoglobin levels (g/dL) | ||||
| Preoperative Hb, mean ( |
12.3 ( |
11.1 ( |
0.0526 | |
| Postoperative Hb, mean ( |
11.9 ( |
10.9 ( |
0.1743 | |
| Difference (postoperative – preoperative Hb), mean ( |
–0.48 ( |
–0.17 ( |
0.1542 | |
| Deficit of saline (mL), mean ( |
165 ( |
100.0 ( |
0.5582 | |
*Desired drop in
In this comparative report we found that MTX administration, followed by hysteroscopic pregnancy surgical removal, is safe and effective to treat CSP. Local MTX should be preferred, due to the significant quicker times of trophoblastic demise and surgical resolution with respect to the systemic route, without the need of additional drug’s administration. MTX is an antimetabolite drug widely used to treat ectopic pregnancies, including CSP. Its effect is based on the cytocidal action of highly proliferating trophoblastic cells, allowing pregnancy termination [4, 5, 14]. The competitive and reversible nature of MTX binding to DHFR, a key enzyme in intracellular folate homeostasis, leads cell-drug concentration and exposure-time in target tissue as two main determinants of cytotoxicity [5]. The short half-life of MTX and the impaired blood supply to placental tissue implanted within a scarred uterine niche have been advocated to understand the low effectiveness of systemic MTX used as unique therapy to treat CSP [4, 5, 14, 15]. By enhancing drug concentrations within the target tissue, local intra-gestational MTX administration through ultrasound-guided procedures improved the clinical results with respect to systemic route. Nevertheless, even local MTX administration used as single therapy fails or leads to complications in about one third of patients, requiring further treatment measures [4, 6, 7]. A scheduled combined treatment, based firstly on pregnancy termination by MTX or UAE followed by timed placental surgical removal by controlled D&C or hysteroscopy, enhances the rate of successful procedures to more than 90% of cases [8, 9, 16, 17]. Allowing the performance of an intervention under vision, hysteroscopy placental removal yielded safer results with respect to D&C by avoiding cervical-isthmic anatomy damage and permitting an effective electrosurgical control of bleeding [8, 16, 18]. In addition, there are few doubts that hysteroscopy provides better details about the anatomy of CSP, allowing a more careful placental separation, lowering operative times and medical costs with respect to major surgery such as vaginal, laparoscopic or laparotomic excisional procedures [1, 4]. The safety and effectiveness of hysteroscopy used both as primary and combined treatment for CSP removal was largely demonstrated. In some hundreds of patients suffering from CSP reported in current literature, very few perioperative adverse outcomes and need of further therapy were recorded [8, 13, 16, 18]. According to these findings the present study confirmed the safety and effectiveness of the resectoscopic treatment after MTX priming; in no case was a perioperative adverse outcome recorded and in no patient was further therapy required. Both systemic and local MTX administration resulted effective to obtain the embryo’s demise; however, based on TVUS imaging we found in all patients the persistence of the ectopic gestational sac until hysteroscopic removal, confirming the delayed times of CSP complete resolution after both systemic and local MTX administration [4, 7, 14, 15]. In 2016 we first described a safe and effective hysteroscopy technique of local subchorionic MTX administration followed by resectoscopic placental removal and since then we have used that technique to manage all types of CSP [12]. We assumed an advantage of hysteroscopy with respect to sonography-guided MTX administration because of a more selective drive, accomplished under direct anatomic visualization, to the target tissue represented by the intervillous spaces of placental implantation site. To our knowledge, in current literature CSP termination by gestational sac local hysteroscopy-guided administration of embryocidal agents such as MTX and ethanol was experienced in only two patients, successfully treated by subsequent resectoscopic placental removal and D&C, respectively [19, 20]. More recently, a case report from Casadio et al. [21] described a successfully conservative procedure based on hysteroscopically-driven myometrial peri-gestational sac injection of MTX, followed by placental removal using a 6-mm truclear hysteroscopic morcellation system. This sequential technique to treat CSP appears conceptually very similar to that proposed in the present study.
Although this study is retrospective and carried-out on only a small series of
patients, the present experience demonstrates the significant advantage of local
with respect to systemic MTX to obtain a prompt decline of
The therapeutic management of CSP using MTX, firstly aimed at pregnancy
termination and followed by timed hysteroscopic placental removal, is safe and
effective, both by systemic or local administration. Nevertheless, local MTX
administration led to significantly faster
The datasets used and analyzed during the current study are available from the corresponding Author on reasonable request.
GG—Conceptualization and design of the study, senior surgeon accomplishing, describing and collecting data of all interventions; PFS—Conceptualization of MTX effects on CSP; LS—Analysis and interpretation of data; SM—Clinical management of patients by planning follow-up, ultrasonographic assistance; MF—Clinical management of patients by planning follow-up, ultrasonographic assistance; MS—Analysis and interpretation of data. All authors read and approved the final manuscript.
All procedures were performed in accordance with the ethical standards of the national research committee and with the 1964 Helsinki Declaration with its amendments. Given the retrospective nature of the study, the lack of guidelines for CSP management and the urgency to start an effective therapy for pregnancy termination, formal Institutional Ethical Board approval was not applicable. Before MTX administration an approval for the use of an off-label drug was obtained from the Local Health Authority whereas patient agreement was obtained by a signed informed consent and a tailored informative note.
We thank Mrs Caroline Calnan, a native English speaker with expertise in medical papers, for the grammar and style revision of the manuscript.
This research received no external funding.
The authors declare no conflict of interest. Giancarlo Garuti is serving as one of the Editorial Board members of this journal. We declare that Giancarlo Garuti had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Paolo Casadio.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.