



1 Department of Clinical Laboratory, Tianjin Fifth Central Hospital, 300450 Tianjin, China
2 Department of General Surgery, Tianjin Fifth Central Hospital, 300450 Tianjin, China
†These authors contributed equally.
Abstract
Background: The analysis is based on the level of T, B, NK lymphocytes
to evaluate the efficacy of laparoscopic nerve-sparing radical hysterectomy
(LNSRH) for early cervical cancer. Methods: Selected 30 patients with
early cervical cancer who underwent LNSRH surgery in Tianjin Fifth Central
Hospital from December 2019 to January 2021 as the cervical cancer group, and 30
healthy female who underwent physical examination in our hospital during the same
period were selected as the control group. The expressions of CD
Keywords
- T lymphocytes
- B lymphocytes
- NK cells
- early cervical cancer
- laparoscopic extensive hysterectomy with preservation of autonomic nerves
Cervical cancer, also known as carcinoma of uterine cervix, is a common gynecological
malignancy. Human papillomavirus (HPV) is the main risk factor for the cervical
cancer, which is mostly caused by smoking, premature sexual life and immune
deficiency diseases [1]. Most patients may have no symptoms in the early stage,
which is often found through screening. Contact bleeding and abnormal vaginal
bleeding may occur in supplementary patients, and other tissues and organs will
be invaded in the advanced cervical cancer [2]. Therefore, it is very important
to predict early cervical cancer. Some studies have confirmed that patients with
cervical cancer have different degrees of abnormal cellular immune function [3].
CD
30 patients with early cervical cancer who underwent (LNSRH) in Tianjin Fifth Central Hospital from December 2019
to January 2021 were selected as the cervical cancer group which age from 31 to
58 (44.51
The following inclusion criteria were established for cervical cancer: (1) Meet the diagnostic criteria for cervical cancer in the Expert Consensus On Immunoprophylaxis of Human Papillomavirus-Related Diseases [6]. (2) Patients with available 3-year follow-up data (for non-recurring patients; patients who recurred were included even if they did not complete the three-year follow-up period). (3) It belonged to the early stage of cervical cancer. (4) The clinical data were complete and all patients with cervical cancer were operated on in Tianjin Fifth Central Hospital. (5) Good cognitive function. (6) All subjects signed informed consent and was approved by the ethics committee of Tianjin Fifth Central Hospital.
Exclusion criteria were the following: (1) Age
All patients with cervical cancer performed pulmonary function, liver and kidney function and blood routine examination before operation. The steps of LNSRH were (1) cut off the ligaments around the uterus, (2) unfolded the retroflexion of bladder peritoneum, (3) exposed the rectum to lie on one side, opened the rectal space and separated the inferior abdominal nerve, (4) the uterine artery was cut off at 1 cm from the internal iliac artery and the fallopian tube was freed, (5) fully exposed the paravaginal space, (6) identify paravesical space and separate fascia, (7) dissected the blood vessels of the posterior lobe of the bladder cervical ligament, (8) deep uterine vein and inferior abdominal plexus were separated, (9) vut off paravaginal tissue and uterine branch of inferior abdominal plexus, (10) the rectovaginal space was separated, the uterus was removed, and then the pelvic cavity was cleaned. The equipment was evacuated and the incision was sutured after there was no active bleeding.
All patients with cervical cancer were sampled 3 mL of fasting
peripheral venous blood in the morning before operation, 1 day and 3 days after
operation. Healthy women were sampled 3 mL of fasting peripheral venous blood and
then added with CD
The female sexual function index (FSFI) score was used to evaluate female sexual function (a total score from 2 to 36, a high score indicated that sex life was good), and the overall assessment scale of cancer treatment function (FACT-G) score was used to evaluate the quality of life of patients (from 0 to 108, a high score indicated that the quality of life of patients was good).
The statistical analyses were performed using the Statistical Package for the
Social Sciences version 19.0 (SPSS Inc., Chicago, IL, USA). Levene method was
used to test the homogeneity of variance, student’s t test (t
test) was used to independent sample, analysis of variance (ANOVA), were used in
the testing for repeated measurements in comparison between the groups, and
chi-square test were used to compare proportion values. Receiver operator
characteristics (ROC) curve and Pearson correlation analysis was used to analyze
the predictive value of CD
The expression of CD
| Groups | n | CD |
CD |
CD |
CD |
|---|---|---|---|---|---|
| Control group | 30 | 35.49 |
23.01 |
13.03 |
15.88 |
| Cervical cancer group | 30 | 29.87 |
28.32 |
19.17 |
12.18 |
| t | 4.672 | 5.782 | 9.659 | 5.599 | |
| p | 0.001 | 0.001 | 0.001 | 0.001 |
The expression of CD
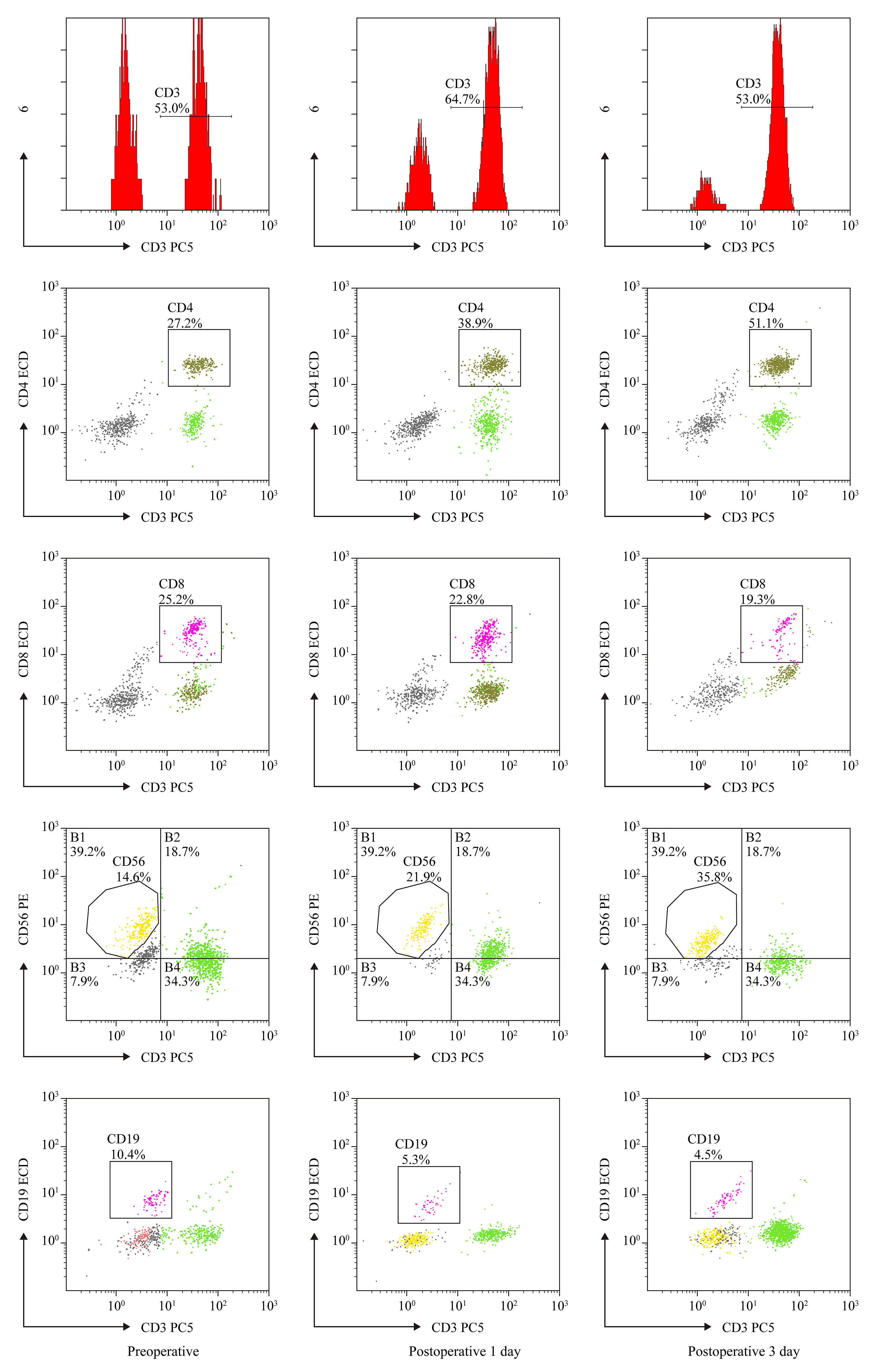 Fig. 1.
Fig. 1.
The CD
| n | CD |
CD |
CD |
CD | |
|---|---|---|---|---|---|
| Preoperative | 30 | 29.65 |
28.21 |
19.02 |
12.32 |
| Postoperative 1 d | 30 | 30.02 |
27.35 |
18.68 |
12.98 |
| Postoperative 3 d | 30 | 33.21 |
25.26 |
16.85 |
14.35 |
| F | 3.360 | 3.252 | 3.322 | 3.316 | |
| p | 0.001 | 0.001 | 0.001 | 0.001 |
The FSFI and FACT-G scores of cervical cancer group were lower than control
group (p
| Groups | n | FSFI (Score) | FACT-G (Score) |
|---|---|---|---|
| Control group | 30 | 35.69 |
89.68 |
| Cervical cancer group | 30 | 26.35 |
64.21 |
| t | 9.197 | 14.240 | |
| p | 0.001 | 0.001 |
FSFI, female sexual function index; FACT-G, overall assessment scale of cancer treatment function.
The expression of CD
| FSFI | FACT-G | |
|---|---|---|
| CD |
r = 0.529 | r = 0.507 |
| p = 0.001 | p = 0.001 | |
| CD |
r = –0.491 | r = –0.439 |
| p = 0.002 | p = 0.003 | |
| CD |
r = –0.532 | r = –0.557 |
| p |
p | |
| CD |
r = 0.532 | r = 0.557 |
| p |
p |
FSFI, female sexual function index; FACT-G, overall assessment scale of cancer treatment function.
The sensitivity of CD
| Index | AUC | p | Sensitivity (%) | Specificity (%) | Accuracy (%) | 95% CI |
|---|---|---|---|---|---|---|
| CD |
0.877 | 0.001 | 63.33 (19/30) | 56.67 (17/30) | 60.00 (36/60) | 0.779–0.974 |
| CD |
0.840 | 0.001 | 66.67 (20/30) | 60.00 (18/30) | 63.33 (38/60) | 0.738–0.942 |
| CD |
0.738 | 0.001 | 73.33 (22/30) | 63.33 (19/30) | 68.33 (41/60) | 0.614–0.862 |
| CD |
0.783 | 0.001 | 70.00 (21/30) | 56.67 (17/30) | 63.33 (38/60) | 0.669–0.896 |
| Four combined detection indexes | 0.929 | 0.001 | 86.67 (26/30) | 53.33 (16/30) | 70.00 (42/60) | 0.867–0.990 |
LNSRH, laparoscopic nerve-sparing radical hysterectomy; AUC, area under the curve; CI, confidence interval.
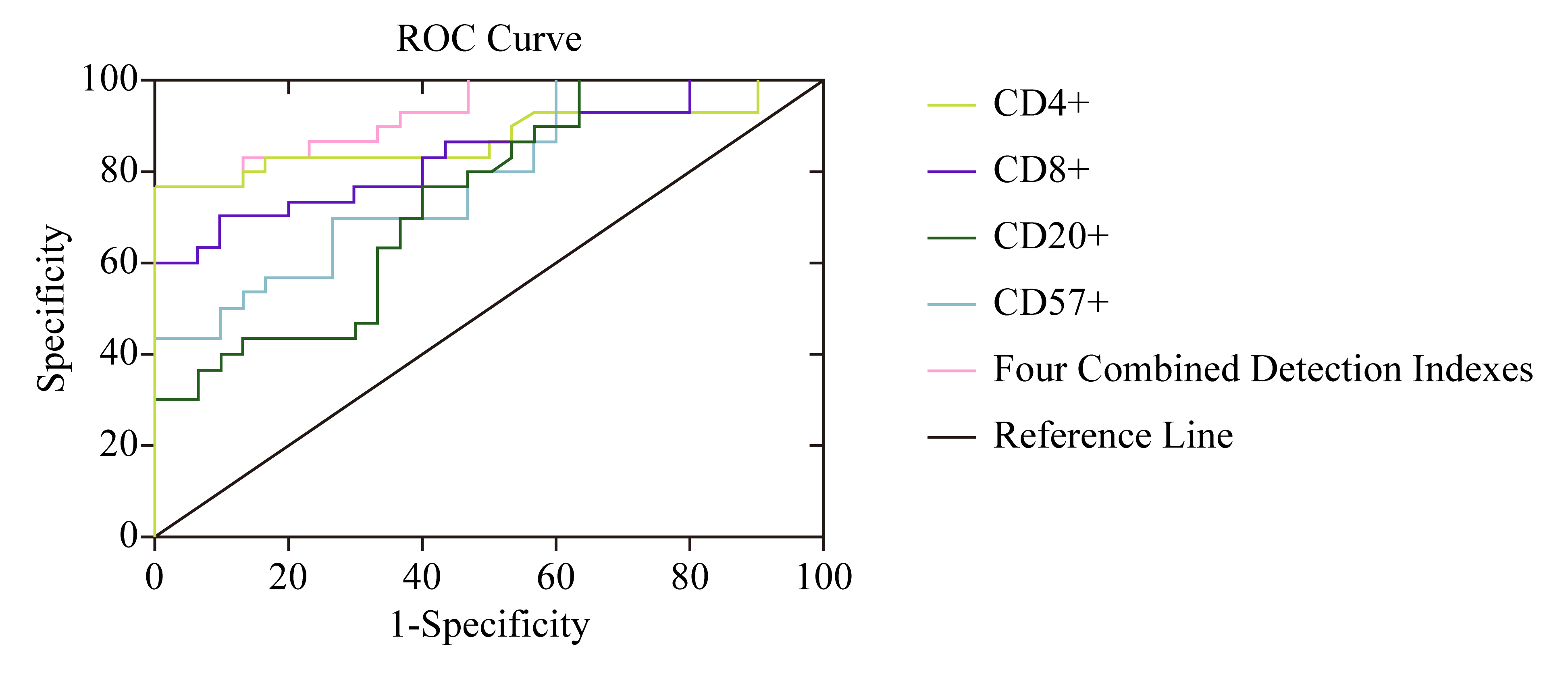 Fig. 2.
Fig. 2.Detection value of CD
Cervical cancer is a common gynecological tumor, with a high incidence of carcinoma in situ at the age of 30–35 and invasive cancer at the age of 45–55 [7]. The disease types are mostly squamous cell carcinoma, adenocarcinoma, adenosquamous carcinoma, clear cell carcinoma, small cell carcinoma, etc. In most cases, cervical cancer is caused by a persistent infection from human papillomavirus (HPV) and developed through a series of precursor dysplastic lesions of the cervical epithelium (i.e., cervical dysplasia) [8]. Human immune dysfunction may lead to cervical cancer. Some studies have shown that the state of the patients immune function can be used to assess the curative effect and prognosis of cervical cancer [9].
The study found that cervical cancer group CD
The study found CD
NK cells can secrete a variety of cytokines and plays a role in hematopoiesis
and immune regulation [20]. CD
The results of the study showed that the sensitivity of CD
Among the limitations of the present study, we mention the retrospective design, the relatively small number of patients included. Interestingly, a recent analysis has confirmed that, in female with the International Federation of Gynecology and Obstetrics (FIGO) stage Ib1-IIa2 cervical adenocarcinoma (CA), there were no significant differences between LNSRH and open surgery in terms of disease-free survival and overall survival [22, 23]. So, further analyses of larger series are needed to better investigate the effect of LNSRH on the survival rate of early cervical cancer (ECC) patients. The main strengths of the current investigation were: FSFI, FACT-G scores were used to evaluate female sexual function and quality of life, the homogeneous and long-term (3-year) analysis of outcomes. The four combined test have good predictive value for the efficacy of LNSRH for early cervical cancer.
In conclusion, our study shows that LNSRH is a feasible, safe and effective procedure that conjugates adequate radicality with an improvement in post-operative functional outcomes. In the present study, we evaluated LNSRH is beneficial to the recovery of cervical cancer patients of life that were investigated. T, B, and NK lymphocytes combined test have good predictive value for the efficacy of LNSRH for early cervical cancer. Our data provide a reliable picture of the everyday clinical scenario in patients affected by early-stage as well as locally advanced cervical cancer. These data may serve as the basis for clinical counselling and future discussions on this relevant topic.
All data generated or analysed during this study are included in this published article.
Conception and design—LH; Administrative support—HZ; Provision of study materials or patients—LH; Data analysis and interpretation—LM; Manuscript writing—All authors; Final approval of manuscript—All authors. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and this study was approved by the Tianjin Fifth Central Hospital Ethics Committee (approval number: 20221110). I confirmed that informed consent was obtained from all patients and their families. I confirmed all methods were carried out in accordance with Helsinki declaration.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.