







1 Department of Pediatrics, Key Laboratory of Birth Defects and Related Diseases of Women and Children of the Ministry of Education, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Key Laboratory of Obstetrics & Gynecologic and Pediatric Diseases and Birth Defects of the Ministry of Education, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
Abstract
Background: Published research findings regarding the relationship between the methylenetetrahydrofolate reductase (MTHFR) A1298C polymorphism and the risk of preeclampsia (PE) have generated conflicting results. A meta-analysis was conducted to investigate whether the MTHFR A1298C polymorphism is associated with preeclampsia. Methods: We conducted a systematic search across several databases, including PubMed, Embase, Web of science, China National Knowledge Infrastructure, and Chinese Biomedicine Databases, to identify relevant studies. We then calculated pooled odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) to assess the association between the MTHFR A1298C polymorphism and preeclampsia (PE) risk. Results: A total of 11 studies were enrolled in this meta-analysis. The pooled analyses revealed that MTHFR A1298C polymorphism significantly decreased the risk of PE (allele contrast (A (alanine) vs. C (glutamate) ): OR, 0.81; 95% CI, 0.71–0.93, p = 0.207; homozygote (AA vs. CC): OR, 0.57; 95% CI, 0.40–0.79, p = 0.056; heterozygote (AC vs. CC): OR, 0.62; 95% CI, 0.45–0.87, p = 0.010; dominant model (AA + AC vs. CC): OR, 0.59; 95% CI, 0.43–0.81, p = 0.031; recessive model (AA vs. AC + CC): OR, 0.83; 95% CI, 0.70–0.98), p = 0.817. Conclusion: Present meta-analysis reveals that MTHFR A1298C variant may serve as genetic biomarkers of PE. The study was registered on PROSPERO (https://www.crd.york.ac.uk/prospero/), registration number: CRD42023459681.
Keywords
- MTHFR
- polymorphisms
- preeclampsia
- meta-analysis
Preeclampsia (PE) is the leading contributor to maternal and perinatal mortality globally [1]. It is responsible for an estimated 46,000 maternal deaths and roughly 500,000 fetal and newborn fatalities yearly [2]. Women in low- and middle-income countries bear a disproportionate burden of this disease [3]. The World Health Organization (WHO) has reported significantly higher numbers in developing countries than in developed ones, with approximately seven times higher figures. In Asian regions, gestational hypertensive disorders account for 9.1% of maternal deaths [4, 5]. A variety of environmental factors, including smoking habits, hypertension, diabetes mellitus, advanced maternal age, and obesity, have been linked to PE [6, 7]. However, a great deal of PE patients manifest without the presence of any of these identified risk factors, which suggests that environmental factors are not the only contributors. Genetic factors also appear to play a significant role in PE onset and progression [8, 9, 10].
Single-nucleotide polymorphisms (SNPs) represent variations in the genome that can change biological reactions and disease susceptibility. Several SNPs have been investigated in relation to PE [11, 12, 13, 14]. The enzyme methylenetetrahydrofolate reductase (MTHFR) plays a key role in the metabolism of homocysteine (HCy). It facilitates 5,10-MTHF conversion to 5-MTHF, which leads to the vitamin B12-mediated transformation of HCy to methionine [15, 16]. Decreased MTHFR levels or activity as a result of certain gene mutations can cause slight to moderate plasma HCy level elevations [17]. Several MTHFR gene mutations have been identified as potential links to PE, with the C677T and A1298C the most frequently observed. The most frequently observed mutation is the C-to-T change at nucleotide 677 (C677T) in exon 4, which leads to a substitution ofalanine with valine in the catalytic domain of the enzyme, and decreases its activity. Another mutation at position 1298 in exon 7 (A1298C) replaces glutamate with alanine at codon 429. This mutation also diminishes enzyme function in a similar way [18, 19]. The MTHFR A1298C variant shows a difference in the prevalence of its allelic distribution among different populations and ethnicities. Studies on the association between preeclampsia and this condition have been conducted among Asians, Caucasians, Africans, and Americans. Correlation with the Asian and Caucasian populations was found to be significant [20, 21].
MTHFR A1298C is linked to diminished levels of folate in serum, plasma, and red blood cells, as well as a slight elevation in plasma total homocysteine (tHcy) concentration [22]. Considering the presence of mild hyperhomocysteinemia in women with preeclampsia, the MTHFR A1298C polymorphism could potentially be a genetic factor contributing to the pathophysiology of preeclampsia [23, 24]. In cases of preeclampsia, there is a confirmed hereditary element: women born from preeclamptic pregnancies face an elevated risk of developing the condition during their own pregnancies [10]. Although genetic predisposition is a significant factor in the development of preeclampsia, efforts to establish associations between MTHFR A1298C and preeclampsia have generated inconsistent findings [25, 26, 27, 28]. As a consequence, a meta-analysis was conducted on the published case-control studies to more closely examine the relationship between the MTHFR A1298C polymorphism and PE susceptibility.
A comprehensive search was conducted to find articles that have explored the association between MTHFR polymorphisms and PE risk. Databases that were consulted include PubMed, Embase, Web of science, the China Biomedical Database, and China National Knowledge Infrastructure (CNKI). The search used keywords including “MTHFR A1298C”, “variant”, “polymorphism”, and “pre-eclampsia”. The most recent update to this search was made on January 10th, 2023.
Preeclampsia is defined as high blood pressure (140/90 mmHg or higher) and proteinuria (0.3 g or higher in 24-hour urine collection) in pregnant women at least 20 weeks into gestation. The control group comprised unrelated healthy pregnant women. Pregnant individuals with twin pregnancies, diabetes, systemic lupus erythematosus, liver dysfunction, renal disease, or any other systemic diseases were excluded.
In order to be considered for inclusion, every study, regardless of sample size, needed to satisfy the following criteria: (i) evaluating the association between the MTHFR A1298C polymorphism and PE risk; (ii) being case-control research; and (iii) providing sufficient data for calculating a 95% confidence interval (95% CI) for the odds ratio (OR). A study was excluded if it fell within the following categories: (i) abstracts, reviews, overviews, or editorials; or (ii) lacking sufficient data.
Based on the aforementioned inclusion criteria, two authors (YH and AW) independently extracted information from all eligible and qualified publications. Any discrepancies they encountered were resolved by consulting with corresponding author (KY).
The following information was obtained from all eligible publications: surname of first author, date of publication, country and race of participants, genotyping methods, minor allele frequencies (MAF), and Hardy-Weinberg equilibrium (HWE). Ethnic groupings were classified as African, Asian, Caucasian, or Mixed.
Odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were used for evaluating the strength of the association between the MTHFR A1298C polymorphism and PE risk. In addition, stratified analyses were conducted based on ethnicity.
The Cochran Q statistic and I
Publication bias was investigated by performing a visual inspection of funnel plots, utilizing Egger’s power-weighted regression method and Begg’s rank correlation method [32, 33]. A p-value of below 0.05 was considered to be an indicator of statistical significance [32, 33]. All statistical analyses were conducted using version 13.0 of STATA software (STATA Corp., College Station, TX, USA).
Following the literature review, 22 publications that were deemed worthy of thorough examination were shortlisted. After reviewing the titles and abstracts, eight publications were identified that did not satisfy the criteria for this study and they were excluded. After a close examination of the full texts of the remaining 14 articles, one article was excluded as it predominantly focused on a literature review [34]. In addition, two articles were excluded because they were unrelated to the MTHFR A1298C polymorphism [35, 36]. Ultimately, 11 case-control studies related to the MTHFR A1298C polymorphism and PE were identified [17, 25, 26, 27, 28, 37, 38, 39, 40, 41, 42], all of them conforming to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [43]. The process of document retrieval and research selection can be seen in Fig. 1.
 Fig. 1.
Fig. 1.Literature search and study selection procedures used for the meta-analysis of MTHFR A1298C genetic polymorphism and preeclampsia (PE). MTHFR, methylenetetrahydrofolate reductase
The detailed characteristics of the selected studies are shown in Table 1 (Ref. [17, 25, 26, 27, 28, 37, 38, 39, 40, 41, 42]). Of the chosen studies, six focused on Caucasian participants, two on Asian individuals, two on Mixed-race groups, and one investigated individuals of African descent. The research was conducted in Australia, China, Ecuador, Iran, South Africa, and Tunisia.
| Author | Year | Country | Ethnicity | Sample | Genotyping methods | MAF in controls | HWE |
| Kaiser, et al. [37] | 2000 | Australia | Caucasian | 147/109 | PCR-RFLP | 0.353 | 0.502 |
| Lachmeijer, et al. [38] | 2001 | Australia | Caucasian | 204/338 | PCR-RFLP | 0.391 | 0.080 |
| Pegoraro, et al. [39] | 2004 | South Africa | African | 204/338 | AS-PCR | 0.062 | 0.421 |
| Fan, et al. [25] | 2007 | China | Asian | 64/62 | PCR-RFLP | 0.255 | 0.711 |
| Klai, et al. [17] | 2011 | Tunisia | Caucasian | 44/100 | MPCR | 0.045 | 0.061 |
| Dissanayake, et al. [26] | 2012 | Australia | Caucasian | 175/171 | PCR-RFLP | 0.312 | 0.091 |
| Salimi, et al. [28] | 2015 | Iran | Caucasian | 192/196 | PCR-RFLP | 0.145 | 0.101 |
| Chedraui, et al. [27] | 2014 | Ecuador | Mixed | 150/150 | PCR-RFLP | 0.136 | 0.212 |
| Bozikova, et al. [40] | 2015 | China | Caucasian | 120/105 | TaqMan | 0.357 | 0.553 |
| Chedrau, et al. [41] | 2015 | Ecuador | Mixed | 50/50 | PCR-RFLP | 0.140 | 0.017 |
| Ding, et al. [42] | 2021 | China | Asian | 150/150 | PCR-RFLP | 0.150 | 0.810 |
Abbreviations: PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; AS-PCR, allele-specific polymerase chain reaction; MPCR, multiplex polymerase chain reaction; MAF, minor allele frequency; HWE, Hardy-Weinberg equilibrium.
11 case-control studies were included, which encompassed 1500 patients and 1769 controls. The results of the meta-analysis can be seen in Table 2. The forest plots evaluating the association between the MTHFR A1298C polymorphism and PE risk are shown in Fig. 2.
| Genetic model | Allele contrast | Homozygote | Heterozygote | Dominant model | Recessive model | |||||||
| Variables | Sample size | A vs. C | AA vs. CC | AC vs. CC | AA + AC vs. CC | AA vs. AC + CC | ||||||
| N |
Case/control | OR (95% CI) | p-value |
OR (95% CI) | p-value |
OR (95% CI) | p-value |
OR (95% CI) | p-value |
OR (95% CI) | p-value | |
| Total | 11 | 1500/1769 | 0.81 (0.71, 0.93) | 0.207 | 0.57 (0.40, 0.79) | 0.056 | 0.62 (0.45, 0.87) | 0.010 | 0.59 (0.43, 0.81) | 0.031 | 0.83 (0.70, 0.98) | 0.817 |
| Caucasian | 6 | 882/1019 | 0.88 (0.75, 1.04) | 0.263 | 0.81 (0.54, 1.21) | 0.382 | 0.91 (0.61, 1.36) | 0.264 | 0.85 (0.58, 1.25) | 0.331 | 0.85 (0.68, 1.06) | 0.521 |
| Asia | 2 | 214/212 | 0.83 (0.59, 1.17) | 0.907 | 0.31 (0.11, 0.87) | 0.752 | 0.27 (0.09, 0.77) | 0.566 | 0.30 (0.11, 0.83) | 0.696 | 0.98 (0.65, 1.47) | 0.700 |
| Mixed | 2 | 200/200 | 0.57 (0.39, 0.82) | 0.168 | 0.15 (0.05, 0.45) | 0.007 | 0.16 (0.05, 0.47) | 0.003 | 0.12 (0.05, 0.43) | 0.005 | 0.74 (0.48, 1.15) | 0.853 |
| African | 1 | 204/338 | 0.71 (0.44, 1.13) | NA |
1.14 (0.10, 12.6) | NA |
0.77 (0.66, 0.90) | NA |
1.21 (0.11, 13.4) | NA |
0.67 (0.41, 1.10) | NA |
OR, odds ratios; CI, confidence intervals; A, alanine; C, glutamate.
 Fig. 2.
Fig. 2.Forest plots of odds ratios (ORs) with 95% confidence intervals (CIs) for MTHFR A1298C polymorphism and PE risk stratified by ethnicity. Note: weights and between-subgroup heterogeneity test are from Mantel-Haenszel model. MH, Mantel-Haenszel model.
The MTHFR A1298C polymorphism was found to be significantly associated with the risk of PE in all models (allele contrast (A (alanine) vs. C (glutamate)): OR, 0.81; 95% CI, 0.71–0.93, p = 0.207; homozygote (AA vs. CC): OR, 0.57; 95% CI, 0.40–0.79, p = 0.056; heterozygote (AC vs. CC): OR, 0.62; 95% CI, 0.45–0.87, p = 0.010; dominant model (AA + AC vs. CC): OR, 0.59; 95% CI, 0.43–0.81, p = 0.031; recessive model (AA vs. AC + CC): OR, 0.83; 95% CI, 0.70–0.98), p = 0.817.
The Newcastle-Ottawa Scale (NOS) scores for the selected studies are shown in Table 3 (Ref. [17, 25, 26, 27, 28, 37, 38, 39, 40, 41, 42]). The quality scores for the studies that were included ranged from 7 to 8 points.
| Study | Adequate definition of cases | Representativeness of cases | Selection of control | Definition of control | Control for important factor or additional factor |
Exposure assessment | Same method of ascertainment for cases and controls | Nonresponse rate |
Total quality scores |
| Kaiser et al. [37], 2000 | - | 7 | |||||||
| Lachmeijer et al. [38], 2001 | - | 8 | |||||||
| Pegoraro et al. [39], 2004 | - | 7 | |||||||
| Fan et al. [25], 2007 | - | 8 | |||||||
| Klai et al. [17], 2011 | - | 8 | |||||||
| Dissanayake et al. [26], 2012 | - | 8 | |||||||
| Salimi et al. [28], 2015 | - | 8 | |||||||
| Chedraui et al. [27], 2014 | - | 8 | |||||||
| Bozikova et al. [40], 2015 | - | 8 | |||||||
| Chedrau et al. [41], 2015 | - | 7 | |||||||
| Ding et al. [42], 2021 | - | 8 |
Significant heterogeneity was observed in the heterozygote and dominant models
(heterozygote model, p
 Fig. 3.
Fig. 3.Galbraith plots for the heterogeneity test of MTHFR A1298C polymorphism.
The sensitivity analyses (Fig. 4) and the cumulative meta-analysis (Fig. 5) demonstrated the robustness and stability of the results.
 Fig. 4.
Fig. 4.Sensitivity analysis of associations between MTHFR A1298C polymorphism and PE risk.
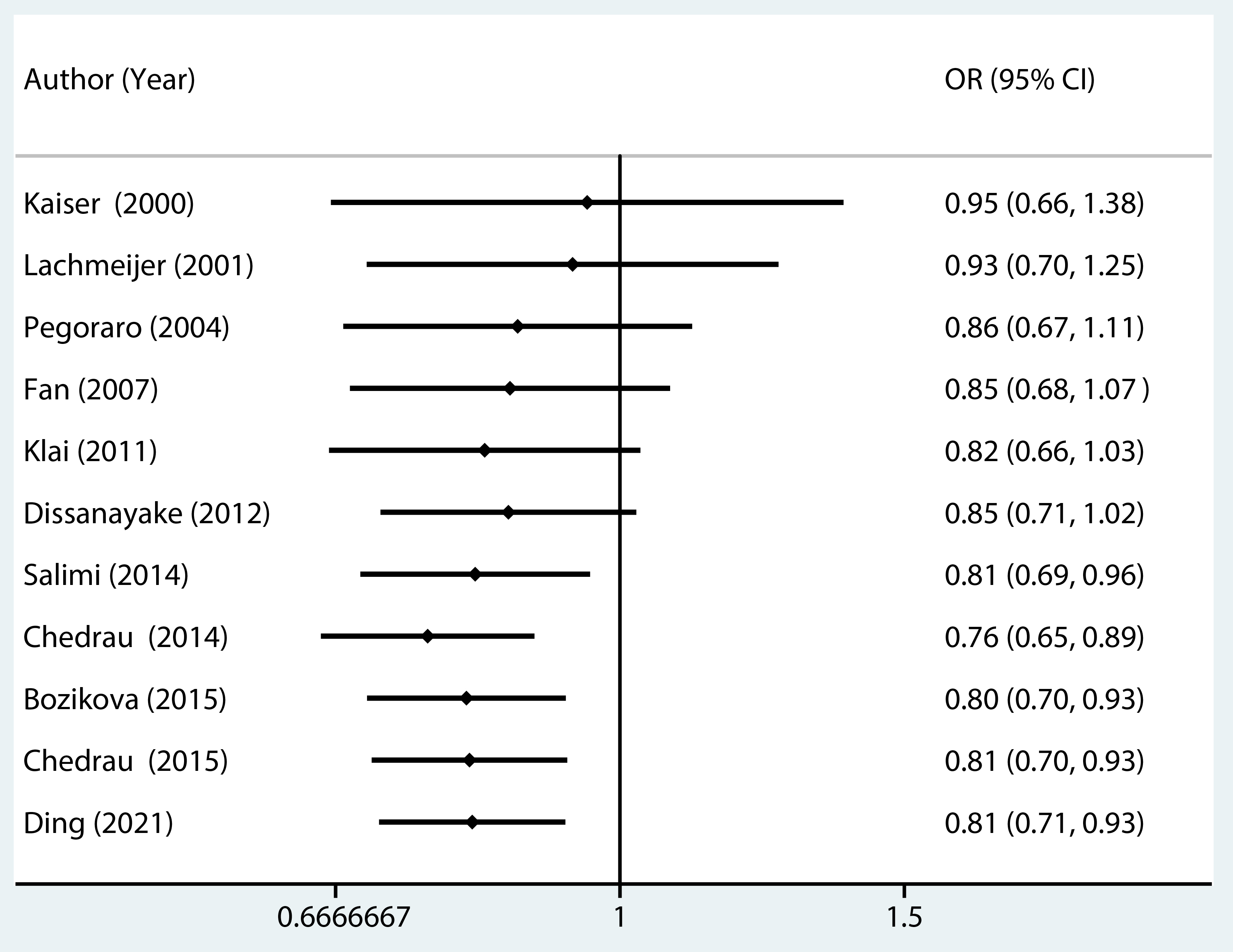 Fig. 5.
Fig. 5.Cumulative meta-analysis of associations between MTHFR A1298C polymorphism and PE risk.
Begg’s and Egger’s [32, 33] tests were conducted as a means of assessing potential publication bias in the literature. As can be seen in Fig. 6, the Begg’s funnel plot showed no signs of asymmetry [32]. Furthermore, the statistical results indicated there to be an absence of publication bias. Results from the Begg’s and Egger’s test were (allele contrast 0.35 and 0.36, homozygote 0.12 and 0.19, heterozygote 0.18 and 0.20, dominant model 0.17 and 0.16, recessive model 0.64 and 0.72).
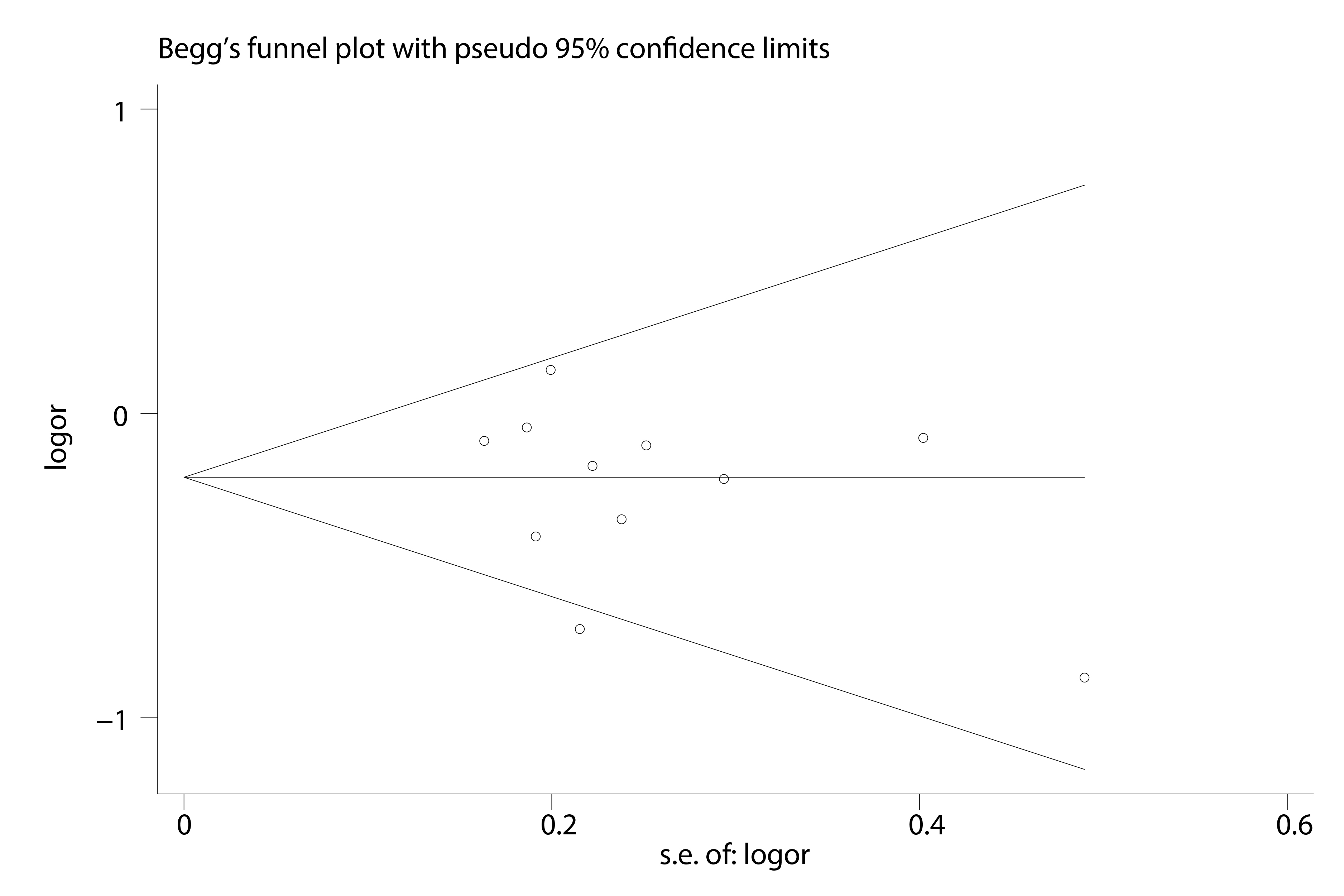 Fig. 6.
Fig. 6.Begg’s funnel plot for publication bias test.
Following a meta-analysis of 11 case-control studies [17, 25, 26, 27, 28, 37, 38, 39, 40, 41, 42], a
significant association was found between the MTHFR A1298C polymorphism and PE
risk. In a subgroup analysis stratified by ethnicity, all the studies examined
showed a significant decrease in PE risk. After the analysis was stratified by
ethnicity, a notably decreased risk was identified among Asian populations for
the homozygote, heterozygote, and dominant models. For mixed populations, there
was also found to be a significant decrease in risk in the allele contrast,
homozygote, heterozygote, and dominant models. In contrast, no significant risk
was detected in Caucasian populations, there reason for this being unclear. A
potential reason may be the variance in the genotype distribution of
MTHFR A1298C CC among Caucasian, Mixed, and Asian populations. The studies
found that the prevalence of the MTHFR A1298C CC alleles in the
3
In this meta-analysis, the studies included in the Asian population category are predominantly from China [25, 42]. We acknowledge that this limited representation of Asian populations, encompassing only one country, could potentially restrict the generalizability of our findings. Therefore, it is imperative to exercise caution when interpreting our results and consider the possibility of regional variations when applying these findings to other Asian populations.
The findings of this study relating to the MTHFR A1298C polymorphism deviate from those of Wu et al. [34]. In their meta-analysis, they could not successfully demonstrate a connection between PE risk and the MTHFR A1298C polymorphism in any of their analyzed models. One potential reason for this inconsistency may be the limited sample size of the earlier study. The meta-analysis of Wu et al. [34] included just six studies that examined the MTHFR A1298C polymorphism and PE risk, resulting in a less refined risk assessment.
With meta-analysis, addressing heterogeneity is a major concern, as high variability among studies can potentially cause biased outcomes. In this research, heterogeneity was identified across the studies in the heterozygote and dominant models. The Galbraith plot analysis identified one study as being the primary contributor to this heterogeneity [27]. Following the removal of this outlier study, a marked reduction in heterogeneity was noticed, although the primary findings remained consistent.
Another major concern in meta-analysis is publication bias potential as a result of the selective representation of studies. In the meta-analysis of this study, Egger’s and Begg’s [32, 33] tests were both used for evaluating this concern. The statistical outcomes, together with the symmetry of the funnel plot, indicated an absence of notable publication bias. More importantly, the results were further bolstered by sensitivity analysis, which affirmed their consistency and robustness. It should be noted that one of the studies that was considered deviated from the Hardy-Weinberg equilibrium (HWE) [41]. However, following the removal of this anomalous study and a data reassessment, the conclusions remained consistent.
There are several limitations with this study: (i) due to the limited sample size and the small number of researches that were included in the meta-analysis, the results may not adequately reflect the true associations; (ii) the analysis was reliant on unadjusted OR estimates as not all the included studies provided adjusted ORs, and where adjusted ORs were provided, the adjustments varied based on factors such as ethnicity, age, or smoking habits; (iii) the genotype distribution of the control group in one study deviated from the Hardy-Weinberg equilibrium (HWE); and (iv) in this meta-analysis, the representation of the Asian population came from two studies that were conducted in China and due to the lack of research data from other Asian populations, the findings may have limited generalizability; (v) compared to our study, the latest Whole Genome Sequencing (WGS) research has utilized a much larger study population, including participants from diverse geographical regions and ethnic backgrounds. These studies possess higher statistical power and encompass broader genetic diversity, thus enabling them to provide more accurate and comprehensive analysis results. Therefore, we anticipate these large-scale studies will offer deeper insights into the association between specific genetic variations and preeclampsia.
In conclusion, our meta-analysis suggests that the MTHFR A1298C variant holds potential as a genetic marker for PE. Nonetheless, additional comprehensive, multicenter studies are essential to solidify and validate our findings.
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
KY conceived and designed the meta-analysis. YH and AW performed the literature search. AW analyzed the data. YH wrote the paper. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Thanks to all the peer reviewers for their opinions and suggestions.
This study was supported by the Key Research and Development Program of Sichuan Province (grant no. 2022YFS0079).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.