





1 Department of Gynaecology, The Affiliated Hospital of Zunyi Medical University, 563000 Zunyi, Guizhou, China
Academic Editor: Michael H. Dahan
Abstract
Background: There are short of systematical analyze of the late-term
pregnancy proportion of women experiencing postpartum hemorrhage and symptomatic
fibroids following uterine artery embolization (UAE). Methods: This was
a systematic literature review and meta-analysis of existing studies.
Results: In total, we identified 497 pregnancies following UAE; 49
patients chose to abort their pregnancies, 79 miscarried during the early- or
middle-terms of pregnancy, and 378 pregnancies successfully progressed into the
late-term (
Keywords
- late-term pregnancy proportion
- postpartum hemorrhage
- symptomatic fibroids
- uterine artery embolization
- meta-analysis
Uterine artery embolization (UAE) was is a commonly applied approach to preserve
organs and treat obstetric hemorrhage, symptomatic uterine fibroids, and uterine
adenomyosis [1]. A significant body of evidence now supports the fact that UAE is
a safe and effective alternative to hysterectomy for the alleviation of obstetric
or gynecological bleeding, or to relieve the pain associated with uterine
adenomyosis [2]. An increasing number of reports have described successful
pregnancy following UAE, thus demonstrating that women can achieve successfully
achieve pregnancy and deliver healthy offspring [3]. However, because UAE can
influence the supply of blood to the uterus, this technique also increases the
risks of adverse pregnancy outcomes, especially with regards to late-term
pregnancies (
Relevant studies were identified by searching the MEDLINE, EMBASE, Cochrane,
OVID, and PubMed, databases using the search terms “uterine artery
embolization”, “uterine artery obstruction”, “UAE”, and “pregnancy”. The
reference lists of the retrieved articles were then hand-searched to identify
additional studies. Studies were included if they described complete pregnancies
after a series of UAE cases. We excluded cases involving ectopic pregnancies and
voluntary terminations following UAE. Individual case reports were excluded. Our
analyses were based on late-term pregnancy (in which delivery occurred after
Statistical analysis was performed using the
Stata 15 meta-analysis package. Summary statistics for age are presented as means
A detailed flowchart of the selection process is shown in Fig. 1. In total, 29
studies met the inclusion criteria and were included in our study; these are
summarized in Table 1 (Ref. [6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34]). Analysis of the selected publications
revealed that long-term follow-up data after UAE were available for 497 women.
The 29 studies included in our meta-analysis reported 3 to 56 pregnancies per
study when considered at the longest reported follow-up point. Analysis showed
that 49 cases selected abortion to terminate their pregnancy, while 79
experienced miscarriage during early- or middle-term pregnancy; 378 pregnancies
lasted to the late-term (
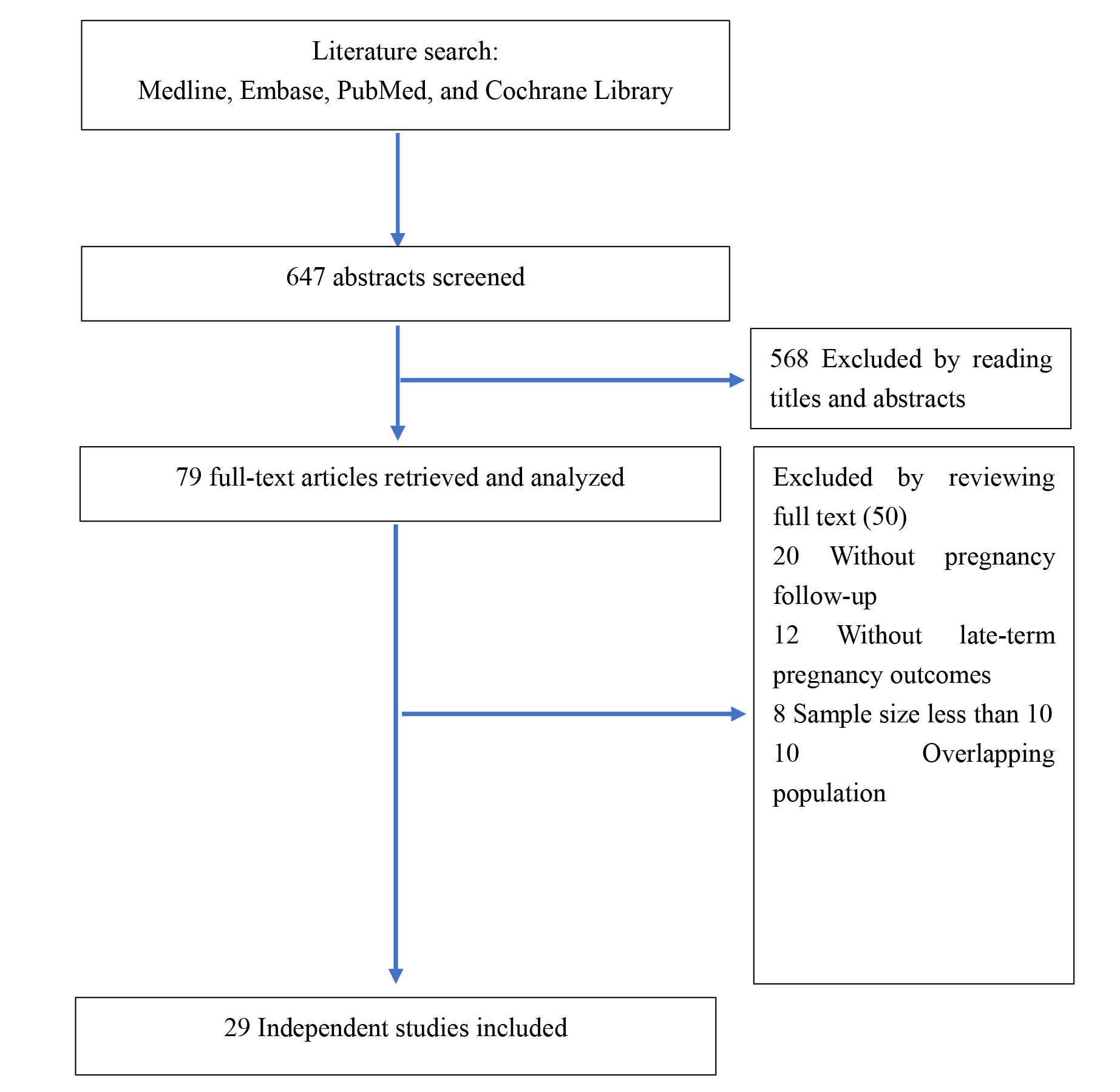 Fig. 1.
Fig. 1.Flowchart shows selection of studies.
| Study | Age | Diagnosis | Embolic agent | Cases | Pregnancy | Miscarriages | Abortion/ectopic | Pregnancy term |
The rate of termed pregnancy (%) |
| Stancato [6] | 20–44 | obstetric hemorrhage | gelatin sponge pledget | 17 | 3 | 0 | 0 | 3 | 100 |
| Ravina [7] | 23–43 (40) | leiomyomata | polyvinyl alcohol | 12 | 12 | 5 | 0 | 7 | 58.33 |
| McLucas [8] | leiomyomata | polyvinyl alcohol | 400 | 14 | 5 | 0 | 9 | 64.28 | |
| Ornan [9] | postpartum hemorrhage | polyvinyl alcohol | 28 | 6 | 0 | 0 | 6 | 100 | |
| Salomon [10] | 23–45 | post-partum haemorrhage | 17 | 5 | 1 | 0 | 4 | 80 | |
| Descargues [11] | postpartum haemorrhage | gelatine sponge | 27 | 10 | 3 | 1 | 6 | 66.67 | |
| Carpenter [12] | symptomatic fibroids | 26 | 26 | 8 | 18 | 69.23 | |||
| Goldberg [13] | 18–59 | Leiomyomata | polyvinyl alcohol particles | 555 | 24 | 6 | 18 | 75 | |
| Kim [14] | 20–40 | polyvinyl alcohol particles | 94 | 8 | 0 | 1 | 7 | 87.5 | |
| Walker [15] | leiomyomata | 1200 | 56 | 17 | 39 | 69.64 | |||
| Eriksson [16] | Massive postpartum hemorrhage | Gelfoam, metallic coils | 20 | 7 | 1 | 6 | 85.71 | ||
| Takeuchi [17] | hysteroscopic removal of a placental polyp | gelatin sponge | 13 | 7 | 0 | 7 | 100 | ||
| Chauleur [18] | primary post-partum hemorrhage | 46 | 19 | 1 | 18 | 94.73 | |||
| Holub [19] | 32.3 |
symptomatic fibroids | nonabsorptive Embosphere trisacryl gelatin particles | 112 | 28 | 0 | 16 | 12 | 100 |
| Mara [20] | 32.2 |
fibroid | Trisacryl gelatin microspheres | 58 | 17 | 0 | 11 | 6 | 100 |
| Pinto [21] | 33–40 | fibroid | tris-acryl gelatin microspheres | 100 | 11 | 3 | 0 | 8 | 100 |
| Sentilhes [22] | severe postpartum haemorrhage | 16 | 0 | 3 | 13 | 100 | |||
| Fiori [23] | 20–43 | postpartum hemorrhage | 34 | 20 | 0 | 8 | 12 | 100 | |
| Firouznia [24] | 35.7 |
symptomatic fibroids | 500-to710-microm polyvinyl alcohol particles | 102 | 15 | 2 | 1 | 12 | 85.71 |
| Gaia [25] | 18–47 | postpartum hemorrhage | absorbable gelatine sponge | 113 | 19 | 1 | 0 | 18 | 94.73 |
| Hardeman [26] | 19–44 | obstetrical hemorrhage | Absorbable materials | 53 | 13 | 0 | 1 | 12 | 100 |
| Bonduki [27] | symptomatic uterine fibroids | polyvinyl alcohol particles | 187 | 15 | 2 | 0 | 13 | 86.67 | |
| Pisco [28] | 36.0 |
fibroid | Polyvinyl alcohol particles (PVA) | 74 | 44 | 4 | 1 | 39 | 97.5 |
| Seiji [29] | gelatin sponge | 211 | 42 | 9 | 3 | 30 | 76.92 | ||
| Poggi [30] | 30.5 |
103 | 17 | 0 | 0 | 17 | 100 | ||
| Cheng [31] | postpartum hemorrhage | 178 | 19 | 4 | 0 | 15 | 78.94 | ||
| Torre [32] | symptomatic multiple fibroids | tris‐acryl gelatin microspheres | 15 | 5 | 0 | 0 | 5 | 100 | |
| Delplanque [33] | 12 | 8 | 0 | 0 | 8 | 100 | |||
| Toguchi [34] | 34.1 |
postpartum hemorrhage | 23 | 14 | 4 | 0 | 10 | 71.43 |
After excluding cases involving ectopic pregnancies or voluntary termination,
the collective proportion of miscarriage was 17.63% (79/448); the lowest rate
was 0% and the highest rate was 30.35% (17/56). The pooled late rate among 448
pregnancies 84.59%, among the 29 studies. After we pooled all of the studies,
the proportion of women achieving late-term pregnancy was 96% (95% CI,
90%–100%) in a random model (I
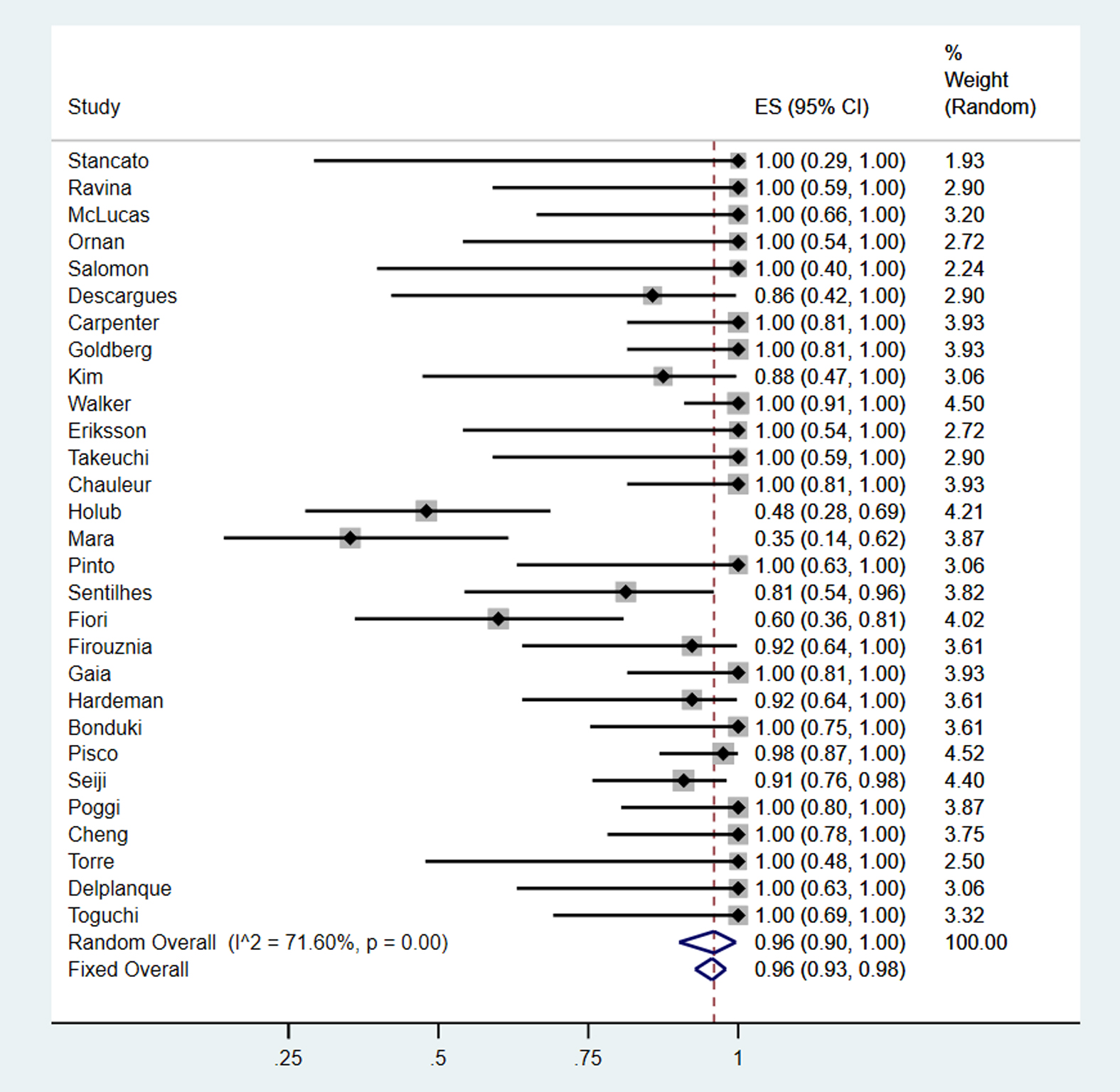 Fig. 2.
Fig. 2.Forest plots showing the total late-term pregnancy rate in women experiencing postpartum hemorrhage and symptomatic fibroids.
Of the 29 studies selected for analysis, 19 studies provided information
relating to the embolic agents that were used. Absorbable embolic agents were
used in 6 studies [6, 11, 17, 25, 26, 29] including 94 pregnancies; of these
pregnancies, there were 13 early miscarriages, 5 ectopic pregnancies or voluntary
terminations, and 76 pregnancies continued to late-term. When pooled, after
excluding ectopic pregnancies or voluntary terminations, we found that late term
pregnancy rate was 92% (95% CI, 79%–100%, I
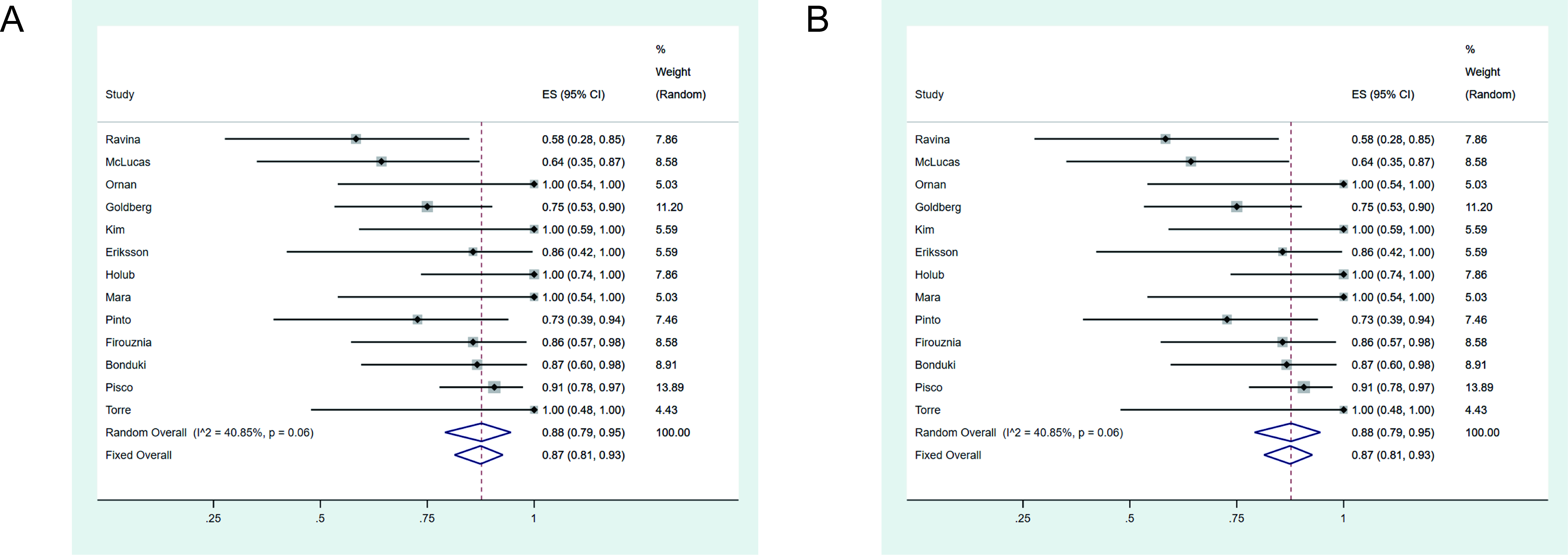 Fig. 3.
Fig. 3.Forest plots showing late-term pregnancy rate when treated by absorbable agents (A) or non-absorbable agents (B).
Non-absorbable embolic agents were used in 13 studies [7, 8, 9, 13, 14, 16, 19, 20, 21, 24, 27, 28, 32] and involved the treatment of 206 pregnancies. Of these, there
were 28 cases of early miscarriage, 30 ectopic pregnancies or voluntary
termination cases; 149 pregnancies lasted to the late-term. The late-term
pregnancy rate was 88% (95% CI, 79%–95%, I
Of the selected studies, 14 reported the use of UAE to treat postpartum
hemorrhage [6, 9, 10, 11, 16, 18, 22, 23, 25, 26, 29, 31, 34]; collectively, these
studies reported 205 pregnancies, 24 miscarriages, and 16 voluntary terminations;
165 pregnancies continued to the late-term. Next, we pooled data relating to
pregnancies in females who underwent UAE because of postpartum hemorrhage. The
late-term pregnancy rate was 93% (95% CI, 85%–93%, I
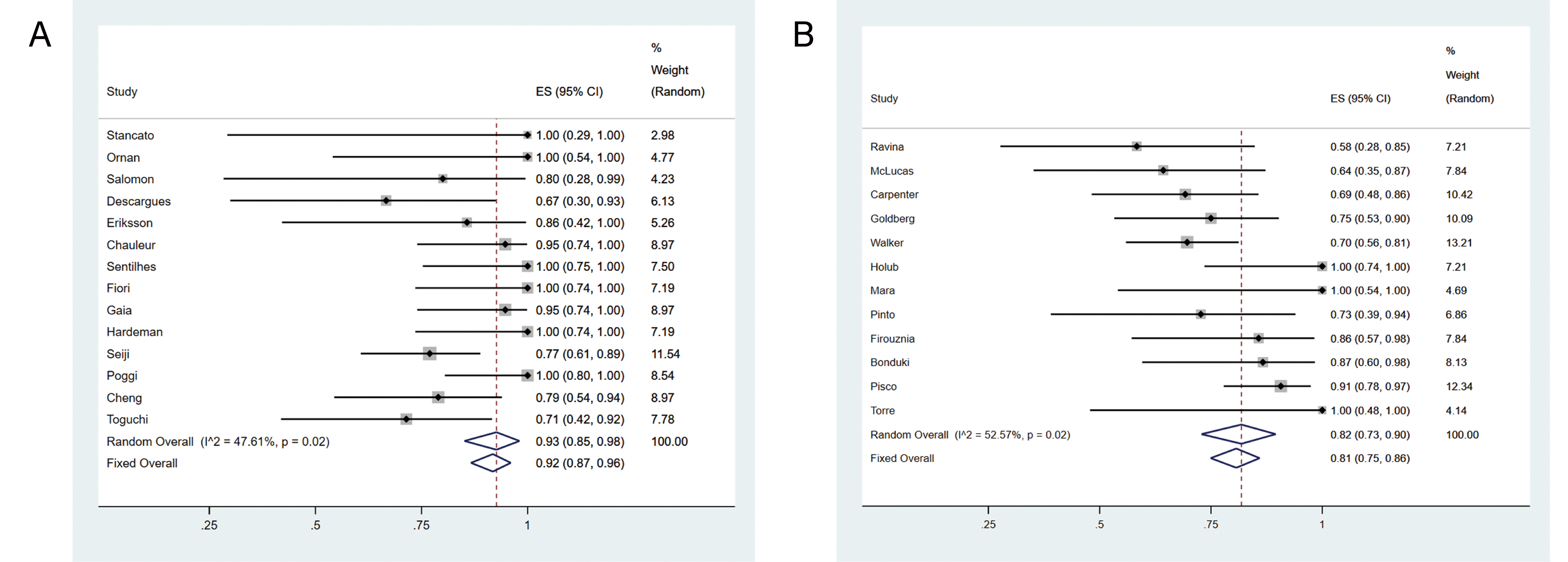 Fig. 4.
Fig. 4.Forest plot indicating the late-term pregnancy rate in UAE treatment due to obstetric hemorrhage (A) and symptomatic fibroids (B).
Twelve studies reported females that chose UAE for the treatment of symptomatic
fibroids [7, 8, 12, 13, 15, 19, 20, 21, 24, 27, 28, 32]. These 12 studies included 267
pregnancies, 52 early miscarriages, and 29 voluntary terminations; 186
pregnancies progressed to the late-term. Pooled data showed that the late-term
pregnancy rate was 82% (95% CI, 73%–90%, I
There are many concerns about the fertility of women following treatment with UAE. For example, a reduction in blood supply can result in atrophy of the uterine endometrium and abnormal fetal development in 2003, Tropeano et al. [35] reported permanent endometrial atrophy in a female with symptomatic fibroids who had been treated by UAE. In another study, Hayden performed a meta-analysis of pregnant females and reported an increased risk of miscarriage after UAE [5]. However, some positive results have also been reported after UAE. For example, Picone [36] reported that fetal growth and umbilical Doppler findings remained normal in the all of the observed cases after pelvic arterial embolization for postpartum hemorrhage. This report was very positive with regards to women who wish to achieve successful pregnancies after UAE treatment. UAE has now been performed for over thirty years, and continues to generate positive results in terms of subsequent pregnancies. However, the relative rate of late-term pregnancies is very diverse; the literature shows that this parameter varies from 58.33% to 100%. We performed this systematic review to provide an up-to-date synthesis of the published data relating to late-term pregnancies after UAE in women who wish to preserve their pregnancies.
Our meta-analysis revealed a high proportion of late-term pregnancies (96%; 95% CI, 90%–100%), although heterogeneity was also evident in the pooled studies. Data showed that the proportion of late-term pregnancies in women who had received UAE were higher than the overall population. This may be due to more careful screening and examination, and also the desire to maintain pregnancies in women who have undergone UAE.
The embolic agents used for UAE can be divided into absorbable agents (e.g., gelatine sponge, Gelfoam) or non-absorbable agents (e.g., polyvinyl alcohol particles). Non-absorbable agents induce permanent embolization; this can potentially reduce the blood supply to the uterus. We divided UAE women into two groups, an absorbable agent group and a non-absorbable agent group. The late-term pregnancy rate was 92% (95% CI, 79%–100%) in the absorbable agent group and 88% (95% CI, 79%–95%) in the non-absorbable agent group. Consequently, it was evident that non-absorbable agents did not affect the fertility of women who received UAE.
There are some controversial results relating to pregnancy in women with fibroids. For example, Lee et al. [37] reviewed a series of pregnancies in women with fibroids and found that uterine fibroids are associated with an increased rate of negative pregnancy outcomes. However, Hartmann et al. [38] reported that women with fibroids are not associated with an increased risk of miscarriage; consequently, there is a clear need to carry out further investigations with regards to the effects of fibroids on pregnancies. In another paper, Homer et al. [5] observed an increased risk of miscarriage after UAE. In our current meta-analysis, the rate of late-term pregnancy was determined to be 93% (95% CI, 85%–93%) in patients who suffered postpartum haemorrhage and 82% (95% CI, 73%–90%) in patients with symptomatic fibroids. We were not able to compare rates between studies due to lack of randomization in such studies. However, it was evident that the rate of late-term pregnancy was lower in patients with symptomatic fibroids than in patients who experienced postpartum haemorrhage and were treated with UAE. Recently, selective progesterone receptor modulators (SPRMs), for example, Ulipristal acetate (UPA), was also shown promising pregnancy results for the females with symptomatic fibroids [39]. However, because of shortage of records of these female enrolled in our study whether or not taken UPA, we couldn’t compare with the pros and cons of the two kinds of treatments.
A successful pregnancy is associated with a range of patient-specific confounding factors, including maternal age, body mass index (BMI), maternal diseases, socioeconomic situations, and parity; these factors may exert independent effects on pregnancy outcomes [40]. Patients with symptomatic uterine fibroids are associated with endometrial atrophy following UAE [35]. However, once pregnancies have been successfully established, then there are good opportunities for a good outcome, as shown by our meta-analysis. When we pooled data from the studies used in our meta-analysis, we observed heterogeneity in terms of population demographics. We could not account for this heterogeneity in our statistical analysis. Despite these potential limitations, the high rate of successful pregnancies is impressive. Reassuringly, our data did not reveal any increased risk for preterm delivery, malpresentation, or IUGR, after UAE treatment.
Collectively, our data indicate that UAE is a beneficial technique but may also be counterproductive for the safety of late-term pregnancies. The results presented herein support the current recommendation that UAE should be considered as a relative contraindication for women who wish to retain their fertility [4].
XZ and LL searched the literature, read the abstract of literature and collected the proper papers, drafted this manuscript, SL checked the literature and analyzed collective datasets, BY designed this study, revised the manuscript and provided finance support for this study. All authors read and approved the final manuscript.
Not applicable.
We thank Jianfeng Li for the help in Statistical analyze, thanks to all the peer reviewers for their opinions and suggestions.
This research received the Guizhou national funding (NO.2021-general 460).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.