
 , Bogdan Dorobaț 3, Maria Mădalina Doldur 4, Ana-Maria Cioca 4, Ionița Ducu 5,*, Bianca Margareta Mihai 2, Corina-Aurelia Zugravu 1,6, Corina Grigoriu 1,7,*, Valentin Varlas 1,2
, Bogdan Dorobaț 3, Maria Mădalina Doldur 4, Ana-Maria Cioca 4, Ionița Ducu 5,*, Bianca Margareta Mihai 2, Corina-Aurelia Zugravu 1,6, Corina Grigoriu 1,7,*, Valentin Varlas 1,21 Department of Obstetrics and Gynecology, “Carol Davila” University of Medicine and Pharmacy, 020021 Bucharest, Romania
2 Department of Obstetrics and Gynecology, Filantropia Clinical Hospital, 011171 Bucharest, Romania
3 Department of Interventional Radiology, Bucharest University Emergency Hospital, 050098 Bucharest, Romania
4 “Carol Davila” University of Medicine and Pharmacy, Faculty of Medicine, 020021 Bucharest, Romania
5 Department of Obstetrics and Gynecology, Life Memorial Hospital, 010719 Bucharest, Romania
6 Fundamental Sciences Department, “Carol Davila” University of Medicine and Pharmacy, 020021 Bucharest, Romania
7 Department of Obstetrics and Gynecology, Bucharest University Emergency Hospital, 050098 Bucharest, Romania
Academic Editor: Michael H. Dahan
Abstract
Background: Uterine arteries embolization (UAE) is a minimally invasive
procedure with good results when it is used as interventional treatment for
patients diagnosed with benign or malignant uterine tumors. The main
gynecological malignancies that are complicated by hemorrhages and would benefit
from UAE are cervical cancer and endometrial cancer in late inoperable stages or
following surgery. Methods: During five years, in the Bucharest
University Emergency Hospital’s Obstetrics and Gynecology Department, from 605
patients to whom trans-catheter embolization of the uterine arteries was
performed, 33 (5.45%) were diagnosed with cervical cancer (n = 31) and
endometrial cancer (n = 2) in the advanced stage addressed for heavy acute
vaginal bleeding and secondary anemia. Results: For those patients, UAE
was used as palliative treatment. The average age of the patients in the
evaluated group was 48.7
Keywords
- uterine artery embolization
- cervical cancer
- endometrial cancer
- acute uterine bleeding
- palliation
- heavy vaginal bleeding
- secondary anemia
- mesh
Genital hemorrhages can be a life-threatening complication in general, with an incidence ranging from 0.7% to 100% in advanced gynecological malignancies [1]. In these latter cases, vaginal bleeding is related to local tumor invasion, tumor angiogenesis, systemic effects of cancer, or oncological treatments [2]. These episodes may vary from low-grade discharges to episodic heavy bleeding. This seriously affects the lives of many patients and can increase morbidity either by secondary anemia and its complications or by hemorrhagic shock [3]. Despite these facts, there are no consistent definitions of bleeding or treatment response for locally advanced-stage cancers. Also, the existing literature is inconsistent in outcome measures, time points, and method assessment [4]. Facing this challenging complication, physicians need to find the best, quickest, safest method to stop the bleeding, to reduce the time for inpatient care and the need for blood transfusion, and also to enable their patients to be hemodynamically stable, so they can further proceed with the next phase of their treatment, which could be radiotherapy, chemotherapy, or both. As treatment options, the literature describes several methods categorized as surgical (hypogastric artery ligature) and non-surgical (uterine artery embolization or Mohs’ paste local application) [5]. It appears that arterial embolization is one of the best available methods to control massive bleedings in gynecologic malignancies, as it provides visualization of the bleeding site and enables targeted, minimally invasive therapy to achieve hemostasis [6].
Uterine arteries embolization (UAE) has been described as an effective and safe method of treating massive vaginal hemorrhage for patients diagnosed with benign and malignant uterine tumors [7]. An interventional radiologist performs a percutaneous angiographic procedure, typically under fluoroscopic guidance and local anesthesia. The embolic material is injected into the vessels serving the tumor, which are preferentially occluded, and the blood supply is stopped in that specific area. This technique dates since 1904 when Dawbarn [8] described preoperatory paraffin injection in the external carotid artery for malignant head and neck tumors. In the Gynecology field, it was first used in malignant afflictions in 1976, and since then gained so much popularity being a highly effective method (the success rate varies between 86% and 100%) in reducing or even stopping vaginal bleeding, increasing the quality of life for these patients and reducing complications caused by local invasion and hemorrhages [6].
Field et al. [9] showed in a retrospective study that the use of selective arterial embolization (SAE) in major bleeding from advanced cervical cancer leads to a decrease in the repeated vaginal message, avoidance of severe anemia (and even hemorrhagic shock), as well as in selected cases of emergency radiotherapy. The authors used SAE (including selective embolization of the internal iliac artery) in half cases and UAE in the other half, with very good results.
The main gynecological malignancy complicated by hemorrhages and benefit from UAE intervention are locally advanced cervical cancer. The palliative embolization procedure can also be applied in local/regional recurrence or inoperable tumors in cervical cancer and rare cases of endometrial or ovarian cancer. Cervical cancer represents the fourth most frequent cancer localization in women, responsible for 7.5% of female cancer deaths worldwide in 2018 [10]. It is a significant public health problem in Romania due to unsuccessful screening programs, despite its declining as number of deaths and mortality rate over the last two decades [11].
Advanced cervical cancer, including stage FIGO IIB and above, is usually treated with chemoradiation only to improve survival benefits. Some oncologists also include advanced stages IB3 and IIA2, so the initial recommendation is chemoradiotherapy, and only in some cases, radical hysterectomy is indicated. However, there are countries where patients selected in stage IIB may benefit from radical hysterectomy or neoadjuvant chemotherapy followed by radical hysterectomy. On the other hand, pelvic exenteration may be indicated in recurrent local/regional or persistent disease after radiotherapy, this surgery is performed only in centers with a high level of expertise in oncological surgery [12]. In conclusion, according to international guidelines, surgical treatment for cervical cancer is indicated up to stage IIA1 [12, 13].
Unfortunately, most patients are diagnosed in more advanced stages of the disease when surgery is not an option anymore, and these patients become an emergency due to the massive bleeding they present at the hospital. In this situation, these patients may benefit from additional palliative care in the form of UAE. Endometrial cancer is the most frequent form of gynecological cancer in developed countries. Though rarer, ovarian cancer is worth mentioning alongside cervical and endometrial cancer as an important malignancy that hemorrhages can complicate [14, 15].
The main objective of this study is to highlight the importance of using UAE in advanced forms of gynecologic cancer that presents with massive vaginal bleeding in patients who followed or not specific oncological treatment, as an emergency measure to stabilize the patient to establish subsequent therapeutic management.
We conducted a retrospective observational study analyzing 33 patients hospitalized in the University Emergency Hospital, Obstetrics and Gynecology Department, Bucharest during 01.01.2015–30.04.2020, diagnosed with locally advanced cervical cancer (31 cases) and endometrial cancer (2 cases) with heavy vaginal bleeding and subsequent anemia.
The inclusion criteria for our study regarding uterine artery embolization performed for hemostatic purposes was heavy acute vaginal bleeding superimposed one of the following: (i) patients diagnosed with cervical or endometrial cancers who were not compatible with a radical surgical treatment, (ii) patients who already received surgical oncological treatment. Regarding the staging of the cases, our study included cervical cancers that were FIGO staging IIB and above. The two cases of endometrial cancer included in the study were inoperable with associated comorbidities and severe anemia. We also included patients with local relapse.
The exclusion criteria were patients for which the vaginal bleeding associated with malignancies was managed and contained by the use of vaginal mesh. Considering the emergency context for which the selected patients were admitted, the histopathological data for most of them was not available, and we did not think of it as inclusion criteria.
During the same period, another 57 embolizations were performed for oncological pathology but which did not meet the criteria to be included in the study because the vaginal bleeding was not accompanied by anemia, or the cases were delayed for surgery for endometrial cancer.
Regarding the technical aspects of the embolization, it is performed by injecting particles of a special embolic material into the vessels that supply the tumor through a brachial or femoral approach, creating a local, very efficient intravascular hemostasis (up to 100%). The procedure occurs in an angiography suite (radiologic imaging is used for guidance). Moderate sedation with short-acting narcotics and benzodiazepines is administered intravenously to diminish pain and anxiety (dexamethasone in a single dose has a positive effect on possible side effects, such as postoperative nausea and vomiting).
The first step is called diagnostic aortography, which is performed by positioning a catheter at the L1 vertebral level to allow imaging of the uterine artery origin and the pelvis. After the site of bleeding is found, selective and super-selective arteriography is performed to pinpoint the pathologic process’s location and plan the next step: the start of the embolization phase of the procedure. Both uterine arteries must be examined. Gelfoam (absorbable gelatin sponge) is more often used as a temporary agent for self-limited processes [16]. The embolic particles are injected into the bloodstream and get carried away until it reaches the vessel that serves the bleeding tumor. These vessels are selectively occluded, being bigger vessels with a faster flow than the healthy ones that serve the healthy part of the organ. The procedure stops when the blood flow in the tumor is ceased. Patients may need to repeat the procedure due to recurrent bleeding [17].
Before the procedure, it is imperative to investigate the patient’s
hemoleucogram, transaminases, blood urea nitrogen, creatinine level, glomerular
filtration rate (GFR), activated partial thromboplastine time (aPTT),
international normalized ratio (INR), fibrinogen level, and an electrolyte panel.
In our group, we used WHO criteria for defining obesity as body mass index ˃30,
hypertension as systolic blood pressure
Using various online libraries, we have conducted a literature survey on the use of the UAE in gynecological malignancies and the implied benefits.
Data was obtained from the patient’s observation sheets and was analyzed using SPSS 12.0 software (IBM Crop., New Orchard Road Armonk, NY, USA). Descriptive tests were applied, as well as correlation tests and logistic regression. We carried out exploratory correlation (Spearman Rho test, due to the non-normal distribution of numeric variables and the ordinal character of other variables) between different variables, mainly between age, days of hospitalization, markers of inflammation, degree of anemia, and other different comorbidities present in our patients. The multinomial logistic regression had the presence and type of anemia as dependent variables and as independent ones, age, comorbidities, and type of cancer. The threshed for significance in all statistical tests was set as 0.05.
In the time frame of this study, transcatheter embolization of the uterine
arteries was performed on 605 patients, of which 33 (5.45%) were diagnosed with
an advanced stage of cervical and endometrial cancer with massive vaginal
hemorrhage and secondary anemia. The average age of the patients in the evaluated
group was 48.75
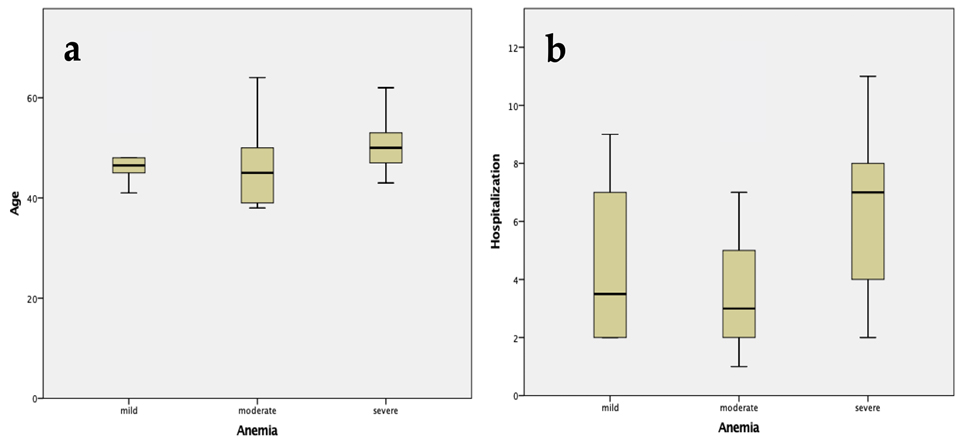
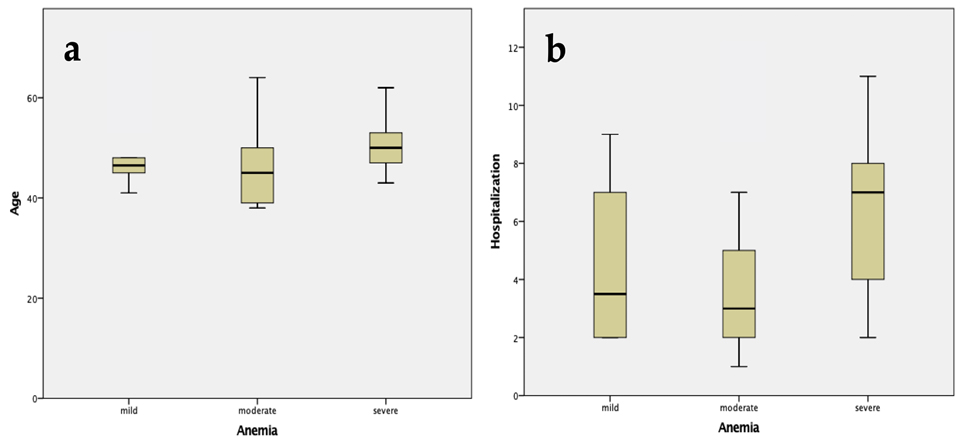 Fig. 1.
Fig. 1.The graphical representation of the anemia degree as function of (a) age and (b) hospitalization period of patients included in the cohort.
It has to be emphasized that 72.72% of patients were under 50, highlighting the growing trend of these two forms of gynecological cancer among young women.
A summary of the patient’s data is presented below in Table 1.
| Age, mean |
48.75 | |
| Area of residence | ||
| urban | 15 | |
| rural | 18 | |
| BMI (No. of patients) | ||
| 1 | ||
| 32 | ||
| Anemia (No. of patients) | ||
| severe anemia (Hb |
9 | |
| moderate anemia (Hb from 8 to 10.9 g/dL) | 14 | |
| mild anemia (Hb from 11 to 11.9 g/dL) | 10 | |
| Arterial blood pressure | ||
| 6 | ||
| 27 | ||
| Diabetic patients | 2 | |
| GFR* (No. of patients) | ||
| 1 | ||
| 32 | ||
| Cancer type | ||
| cervical | 31 | |
| endometrial | 2 | |
| Hospitalization period according to anemia degree (days) | ||
| severe | 6.44 | |
| moderate | 3.78 | |
| mild | 4.5 | |
In our group, we had 2 patients (6%) diagnosed with diabetes, 1 patient (3%) with renal disease, and 5 patients (15.15%) with hypertension disease; obesity had been encountered in only 1 case. As it is easily seen, the associated pathology was poorly represented. Considering that in our cohort, only one patient was over 65 years of age, it is obvious that all associated pathologies can not be considered as confounding factors for inpatient care duration. Renal complications associated with kidney pathology by invasion/compression of the tumor present in our cohort in only one patient were correlated with diabetes and hypertension. In the study group with late stages of gynecological cancer, kidney insufficiency was observed in only one patient (3%).
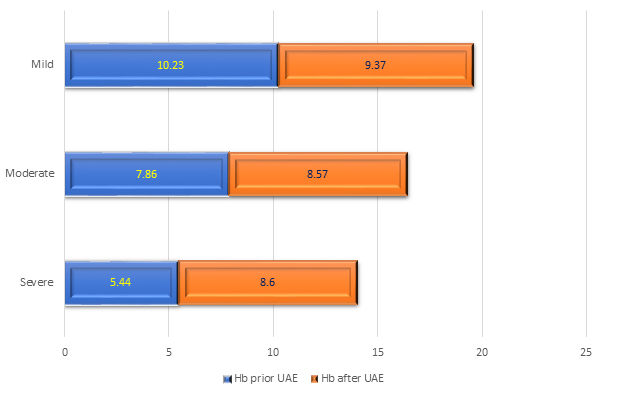
Secondary anemia due to vaginal hemorrhage has been diagnosed in 33 patients
(36.66%); using hemoglobin’s (Hb) threshold, they were classified as : severe
anemia (Hb
| Anemia | Hb prior UAE | Hb after UAE | p-value |
| Severe | 5.44 |
8.60 |
0.042 |
| Moderate | 7.86 |
8.57 |
0.086 |
| Mild | 10.23 |
9.37 |
0.250 |
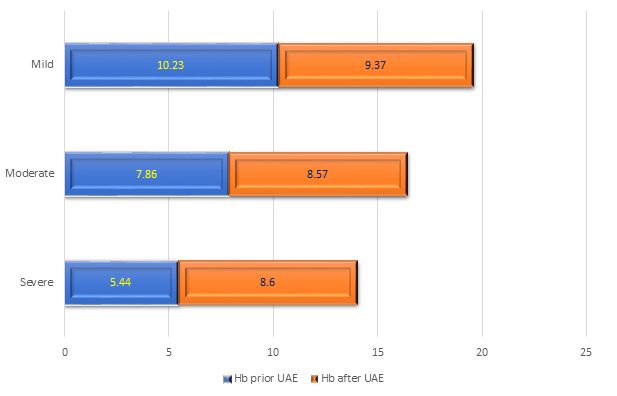 Fig. 2.
Fig. 2.The corrected anemia before and after the UAE procedure.
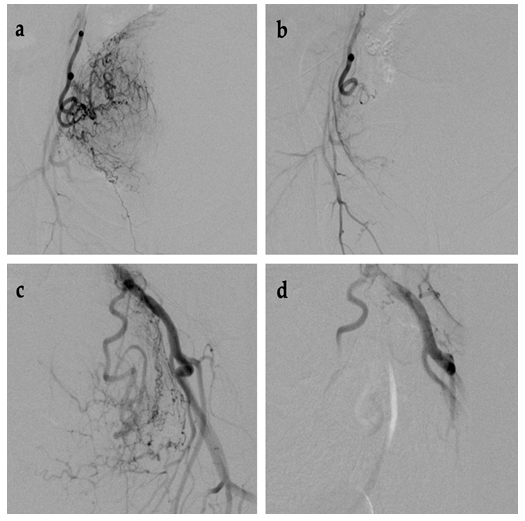
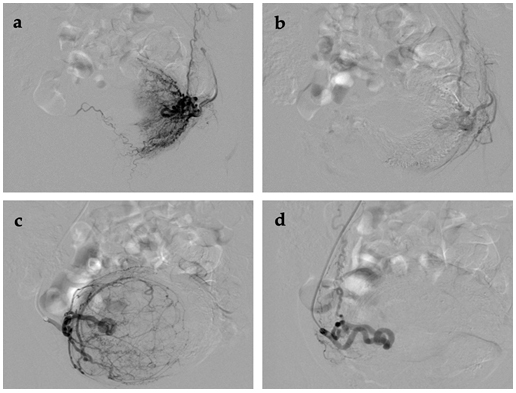
As shown in Figs. 3,4, we can assess the success of the UAE procedure in cervical and, respectively, selected cases of endometrial cancer by the complete obstruction of the blood vessels at the expected embolization sites. All the patients were given lidocaine as a local anesthetic and a contrast agent (omnipaque or iomeron) for the procedure. The patients also received painkillers: tramadol and non-steroidal anti-inflammatory drugs according to their needs. Only 2 (6%) patients needed hydrocortisone because of an allergic reaction to the contrast agents, and 12 (36.3%) of them received complimentary hemostatic agents, such as carbazochrome, etamsylate, and vitamin K. Associated infections were reported in 7 patients (21.2%), and large spectrum antibiotics were administered.
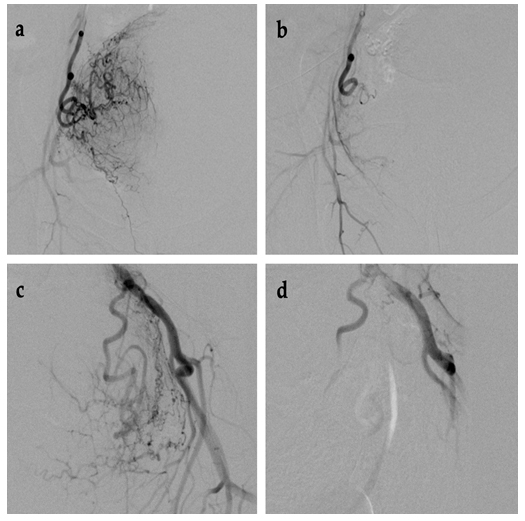 Fig. 3.
Fig. 3.Imaging of UAE procedure in cervical cancer, before and after. (a,b) Left side. (c,d) Right side.
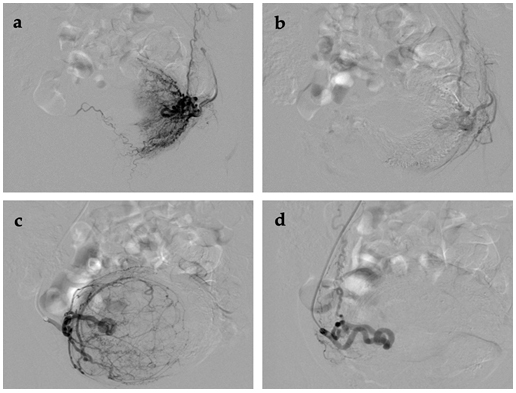 Fig. 4.
Fig. 4.Imaging of UAE procedure in endometrial cancer before and after. (a,b) Left side. (c,d) Right side.
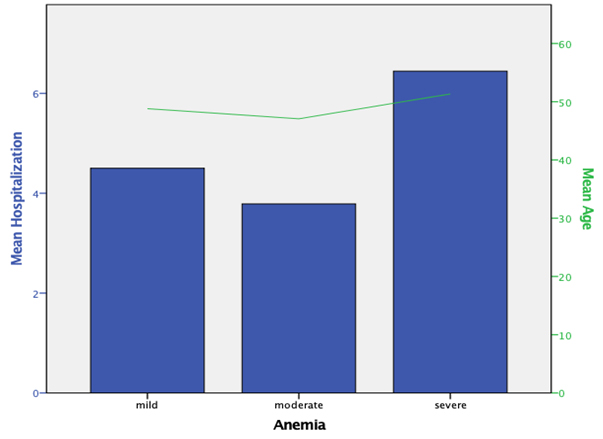
Besides a higher incidence of anemia, a prolonged hospital stay was also
associated with cervical cancer. The average number of days of hospitalization
for inpatient care was 4.72
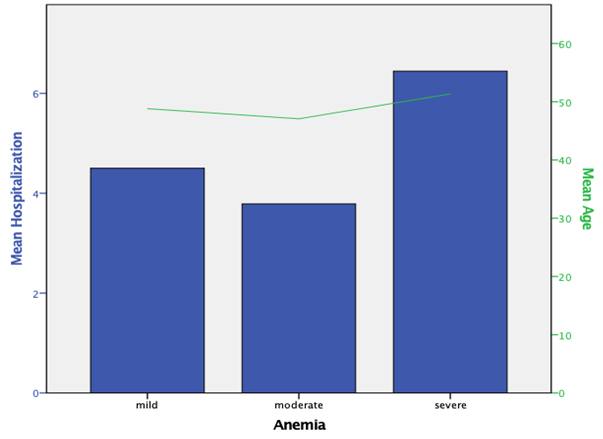 Fig. 5.
Fig. 5.The evolution of hospitalization period according to age and anemia.
Given the context of the associated pathology, and the existing oncological complications, the appearance of acute bleeding can lead to a rapid decompensation. Being a critical patient, vaginal bleeding has to be ceased as quickly as possible, with minimum hospitalization and adverse reactions. Uterine embolization is the safest treatment choice, covering all these conditions and serving as a modern form of palliative care for cancer-associated hemorrhages. In our study group of gynecological cancers, kidney insufficiency was observed in only one patient (3%), data in opposition with the literature stating that 21% of late-stage cervical cancer presents urinary tract obstruction [19].
Interventional radiologists use a combination of drugs to control pain and reduce anxiety. Thus, an anxiolytic from the benzodiazepines class may be prescribed before the procedure. Local anesthesia is obtained at the site of the intervention by injecting lidocaine. Antiemetics (ondansetron) are recommended to avoid vomiting. Nonsteroidal or steroidal anti-inflammatory drugs together with a proton pump inhibitor to lower gastric acidity (omeprazole) are commonly associated with analgesic drugs to control post-procedural symptoms [20]. Antibiotics are among the most common pharmaceutical agents to prevent post-procedure infections [21].
Katz et al. [16] categorize embolic materials into two general classes, whether they provide permanent or temporary occlusion. Permanent occlusion is preferable for progressive disease (tumors), whereas a temporary embolic agent is appropriate for self-limited processes (traumatic lesions). The prototypic temporary embolic agent is absorbable gelatin sponge (Gelfoam), water-insoluble gelatin that allows vessel recanalization within several weeks after placement. Permanent embolic materials include particulate agents (polyvinyl alcohol [PVA] foam and microspheres), metallic coils and plugs, and liquid polymers. They act by mechanical occlusion and may also activate thrombin and promote fibroblast growth [16].
Database research Pubmed, Medscape, and other medical journals highlighted some studies to emphasize the beneficial role of UAE in patients with complicated gynecological malignancies with severe bleeding and subsequent anemia that underwent trans-arterial embolization as palliative means of care for hemorrhage control; this was our main inclusion criteria. A summary of our literature survey can be seen in Table 3 (Ref. [22, 23, 24, 25, 26, 27, 28, 29, 30, 31]).
| Authors | Year | No. of patients | Cause of bleeding | Complete control of bleeding after UAE | Recurrences |
| Pisco [22] | 1989 | 108 | pelvic neoplasms | 74 patients (68.51%) | 23 patients (21%) |
| Yamashita [23] | 1994 | 17 | malignant neoplasms | 10 patients (58.82%) | 7 patients (41.18%) |
| Mihmanli [24] | 2001 | 6 | 4 cervix carcinoma, 1 endometrium carcinoma, 1 ovarian carcinoma | 6 patients (100%) | - |
| Yalvac [25] | 2002 | 8 | inoperable neoplasms | 8 patients (100%) | - |
| Lin [26] | 1996 | 1 | pelvic tumor | 1 patient (100%) | - |
| Hatremi [27] | 2005 | 1 | cervical cancer | 1 patient (100%) | - |
| Alméciga [28] | 2020 | 47 | cervical cancer | 45 patients (95.7%) | 8 patients (17.1%) |
| Bi [29] | 2021 | 16 | cervical cancer | 16 patients (100%) | - |
| Aggarwal [30] | 2018 | 1 | cervical cancer | 1 patient (100%) | - |
| Nogueira-García [31] | 2015 | 6 | cervical cancer | 6 patients (100%) | - |
The reported success rates of UAE in managing acute bleeding range between 58.82–100% as the only procedure for the control of the bleeding. Another important fact to be stated is that its effectiveness also includes malignant pathology of the genital tract and is not limited to cervical cancers. In our case, the success rate of the UAE in stopping the bleeding was 100% of the patients, thus allowing the overcoming of the critical moment and the correction of the secondary anemia. Studies comparing UAE to surgical therapies [6, 32] state that the clinical outcomes of UAE are similar to or even better than the outcomes of surgery, with bringing up that these patients have advanced stages of cancer, with associated afflictions, in which a palliative surgical procedure would involve a long operating time and a great difficulty, increasing the patients’ morbidity. The low rates of UAE complications are due to the low number of transfusions and the lack of surgical and anesthetic complications caused by a longer duration of the intervention. Patients’ choice for this procedure is influenced by the short duration of hospitalization, resumption of activity, and faster social reintegration related to surgical ligation.
Based on these currently limited reports and our clinic’s experience, it appears that arterial embolization plays a significant role in urgent control of massive bleeding in gynecologic malignancies as it provides visualization of the bleeding site and enables targeted, minimally invasive therapy to achieve hemostasis [6] . Furthermore, after UAE, the need for blood transfusion diminished in almost all cases, and additional, potential complications related to blood transfusion were prevented. The most common side effect (pain due to tissue necrosis) is prevented with mild analgesics for 1–2 days.
The article reinforces the need for interventional radiology departments in all regional emergency centers. Another notable mention is that ligation of the hypogastric artery as surgical management of vaginal bleeding in gynecological malignancies is a valid option. It can be performed either by laparotomy or by laparoscopy. In elderly patients with comorbidities, preferably in advanced stages of cervical cancer, surgical ligation is a feasible procedure that should be adopted only in centers where UAE is not available [33, 34].
An important mention needs to be made: Bucharest University Emergency Hospital is the only regional institution with an Interventional Radiology Department, available through the national health insurance system. Many patients from the studied group were urgently referred to our department, a tertiary center specialized in interventional radiology in gynecological practice. The post-procedure follow-up of the UAE was not possible because the patients continued the therapeutic plan in the territorial oncology service after exceeding the critical moment. In this regard, patients selected by the authors are all managed by UAE, considering its advantages compared to a surgical ligation advocated by the literature. This article does not compare surgical and non-surgical methods for patients with inoperable gynecological malignancies but augments the successful use of UAE in these cases as its aim.
The study’s strength lies in the success of emergency management of vaginal bleeding associated with inoperable cervical and endometrial cancers. The peculiarity of this study is achieved by solving in an emergency unit the maximum investigated and uninvestigated cases, with inoperable gynecological cancers that appear for the first time in the emergency room with incoercible vaginal bleeding, to which the vaginal message is not a solution.
The limitation of the study is the lack of a control group in which the effectiveness of the UAE is compared with the surgical ligation for the management of vaginal bleeding of gynecological malignancies, as well as the medium-term monitoring of these cases with predictable evolution.
Uterine artery embolization is a modern technique used in managing patients with advanced stages of cancer associated with uncontrollable genital bleeding with anemia and in which surgical resolution is often no longer possible. This procedure for selected cases reduces morbidity and mortality in the gynecological conditions presented, being a less invasive method of palliative care that provides doctors with the therapeutic window needed to treat anemia and offers the possibility of continuing cancer treatment.
Take away message: UAE is a good rescue tool for the emergency medical care of hemorrages related to advanced gynecological malignancies.
Conceptualization—REB; methodology—BD, MMD; software—CAZ, AMC and MMD; validation—REB, CG; formal analysis—CAZ and BMM; investigation—REB, ID, BD and CG; resources—REB, BD and ID; writing - original draft preparation—REB, MMD and ID; writing - review and editing—REB, VV and BMM; visualization—AMC; supervision—REB, VV and CG. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of University Emergency Hospital (No. 75121/8.12.2021). The data col-lected retrospectively did not contain personal information, without the need of informed consent or the consent of the patient/legal representative in the case of minors. The present study is a retrospective study with anonymization of cases and did not require in-formed consent from the patients.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. REB and VV are serving as one of the Guest editors of this journal. We declare that REB and VV had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to MHD.