
 , Giulia Armano 1, Luciano Monfardini 1, Alissa Valenti 1, Giuseppe Barresi 1, Alessandra De Finis 1, Isabella Rotondella 1, Davide Scebba 1, Diana Butera 1
, Giulia Armano 1, Luciano Monfardini 1, Alissa Valenti 1, Giuseppe Barresi 1, Alessandra De Finis 1, Isabella Rotondella 1, Davide Scebba 1, Diana Butera 11 Department of medicine and surgery, University of Parma, 43125 Parma, Italy
Academic Editor: Antonio Simone Laganà
Abstract
Introduction: In the last decades, the introduction of laparoscopy and, more recently, of robotic surgery, offered new options for surgical treatment also in gynecological malignancies, as an alternative to open surgery. When considering the best surgical treatment option for gynecological malignancies, evidence about safety, feasibility, and oncological outcomes must be taken into account, to offer the best treatment to the patient. The present review aims to provide an updated scenario over the available evidence in the use of minimally invasive surgery (MIS) in gynecological malignancies. Material and methods: An electronic search was performed using the following keywords: ‘minimally invasive surgery’ and ‘gynecology’, ‘minimally invasive surgery’ and ‘endometrial cancer’, ‘minimally invasive surgery’ and ‘ovarian cancer’, ‘minimally invasive surgery’ and ‘cervical cancer’. The agreement about potential relevance was reached by consensus of the researchers and according to PRISMA statement guidelines. Systematic reviews, meta-analyses, clinical trials, and original articles were included in the present review. Results: Fifty-eight studies were considered eligible for the study, 23 studies regarding MIS in endometrial cancer (EC), 19 studies on MIS in ovarian cancer (OC), and 16 studies regarding MIS in cervical cancer (CC). The total of patients enrolled was 180,057, 131,430 in the EC group, 23,774 in the OC groups, and 24,853 in the CC group. Conclusions: According to the available evidence and current clinical practice, MIS is undoubtedly the gold standard for early-stage EC treatment and may represent an acceptable option even in high-risk EC patients. Concerning OC, MIS is a safe and useful tool for staging purposes in advanced-stage disease, and a treatment option only in high volume centres with expert oncologic surgeons. On the contrary, MIS should be abandoned in the context of CC, exception made for well-selected patients, who received adequate counselling about current evidence.
Keywords
- Minimally invasive surgery
- Endometrial cancer
- Ovarian cancer
- Cervical cancer
Gynecological cancers are a heterogeneous group of malignancies, which differ in epidemiology, morbidity, mortality, prognosis, and treatment options. Thanks to technological implementations in the surgical field, gynecologic oncologic surgery benefits from different available treatment tools [1, 2, 3]. When considering the best surgical treatment option for gynecological malignancies, evidence about safety, feasibility, and oncological outcomes must be taken into account, to offer the best treatment to the patient.
Traditionally, surgical staging for gynecological malignancies was via laparotomy. Open surgery offers an optimal exposure of the surgical field, direct access to the anatomical structures, and a quick assessment of the abdominal and pelvic cavity. However, disadvantages such as intraoperative complications, length of hospital stay, and a long recovery for the patient must be considered. In the last decades, the introduction of laparoscopy and, more recently, of robotic surgery, offered new options for surgical treatment also in gynecological malignancies, as an alternative to open surgery.
Laparoscopy was introduced in oncological surgery more than two decades ago and it was originally applied to colon cancer. Subsequently, randomized clinical trials (RCT) were conducted comparing laparoscopy vs open surgery in endometrial cancer (EC) treatment, with evidence of non-inferiority. These results lead to widespread adoption of minimally invasive surgery (MIS) in gynecologic oncologic surgery [4, 5]. Short-term MIS advantages include a minor length of hospital stay, faster return to normal activity, reduced rate of surgical site infections, less postoperative pain, less blood loss, and reduced incidence of venous thromboembolism, sepsis, and post-operative ileus compared to laparotomy [6, 7].
Regarding long terms outcomes, the LACE trial and LAP2 trial both investigated the impact of a minimally invasive surgical approach on quality of life (QoL) in EC patients. These trials showed the MIS beneficial effect on perceived QoL up to 6 months after surgery, thanks to a faster return to normal activities [4, 5].
A minimally invasive approach is also encouraged in the recommendations for perioperative care in gynecologic oncology published by The Enhanced Recovery after Surgery Society (ERAS) [8]. ERAS recommendations aim to optimize the perioperative and postoperative management of patients, in order to achieve a prompt return to daily activities. ERAS recommendations’ efficacy in enhancing postoperative outcomes has been validated in prospective trials [9].
MIS is also associated with some disadvantages, such as longer operative time, higher costs, and longer surgeons’ learning curve [10]. Terzi et al. [11] reported a plateau in the learning curve for total laparoscopic hysterectomy after 75 cases. The need to perform a consistent number of procedures may explain the higher number of intraoperative complications related to MIS reported in some case series.
The widespread use of laparoscopy raised also some limitations of the technique, such as the need for improved camera control and instrument range in terms of motion and dexterity. Robotic surgery seems to offer the same advantages as laparoscopy with a greater range of motion for the surgeon, better exposure of the surgical field, and better camera control thanks to computer assistance [12].
The currently available surgical robotic system (Da Vinci Surgical System, Intuitive Surgical, Inc., Sunnyvale, CA, US) was approved by the US Food and Drug Administration (FDA) in May 2005 for clinical use in gynecology. Da Vinci was first used in reproductive gynecology for tubal surgery.
Robotic surgery offers enhanced visualization, wristed instrumentation, and improved ergonomics compared to laparoscopy, with a “flatter learning curve” [13]. Lim et al. [14] found that the proficiency plateau for robotic surgery is lower than that for conventional laparoscopy (24 procedures vs 49). These characteristics enable more surgeons to perform minimally invasive interventions, even without a consolidated experience in laparoscopy, while those with advanced laparoscopic skills may perform complex surgical cases that otherwise require an open approach.
Robotic surgery is also characterized by minor intraoperative blood loss and a lower rate of conversion to laparotomy compared to laparoscopy.
Robotic surgery has also some limitations compared to laparotomy and laparoscopy. The currently available robotic system does not offer tactile feedback, but most importantly, the cost of this complex technology limits access to robotic surgery. Robotic surgery is likely more expensive because of the cost of purchasing the robotic system, disposable equipment, maintenance, and longer operative times [15].
Both laparoscopy and robotic surgery are associated with longer operative time compared to open surgery, but available literature comes from a limited surgical experience. Likely, with a growing surgical experience, a minor length of robotic interventions may be reported in the future.
MIS has also some peculiar limitations and possible complications compared to laparotomy.
Most complications in laparoscopic surgery occur during abdominal entry. Incorrect abdominal access can lead to minor complications, such as subcutaneous emphysema and extra peritoneal insufflation, or major and potentially life-threatening complications, including major vessels and bowel injuries. Moreover, not all patients are optimal candidates for MIS. Previous surgery and adhesions may hinder the possibility of a safe minimally invasive approach, requiring conversion to laparotomy [16].
Moreover, patients’ habitus and comorbidities must be considered when selecting the best surgical approach.
Morbid obesity and cardiopulmonary comorbidities, especially in elderly patients, have been hypothesized as relative contraindications to MIS. On the contrary, nowadays we know that both obese patients and elderly patients consistently benefit from MIS, thanks to a minor length of hospital stay and faster recovery [17, 18]. These known advantages in terms of fast recovery, must be balanced with the intraoperative need for CO2 insufflation and steep Trendelenburg position, especially in case of robotic surgery.
Several studies were conducted concerning the best surgical approach in obese patients, especially in the context of EC, where this group of patients was more represented [19].
MIS in obese patients not only gives advantages from a clinical point of view, but also in terms of cost-effectiveness [20]. From a surgical point of view, obese patients are difficult to approach because the laparoscopic gesture is more difficult than in normal-weight patients, and when lymphadenectomy is indicated, it is more difficult to be accomplished [21].
Robotic surgery allows the surgeon to overcome some of the difficulties encountered in obese patients, because it shares the same advantages of laparoscopy, with better exposure of the operating field [22].
In a retrospective study conducted on 655 obese patients with EC [23], robotic surgery was associated with a longer operative time, but a lower rate of conversion to laparotomy, shorter hospital stay, and a doubled number of pelvic lymph nodes removed.
MIS comprehends several surgical techniques, and the treatment choice depends on the surgeon proficiency, available equipment and patients’ characteristics. MIS allows a reduction in complication rate and better aesthetic outcomes, and currently ultra-minimally invasive surgery may offer the same benefits with even better cosmetic results [24].
In conventional laparoscopy and robotic surgery, 5–12 mm trocars are used, in different abdominal areas. The number of trocars depends on surgery complexity.
Minilaparoscopy consists in 3 mm, multi-site instruments. The use of 3 mm trocars allows better aesthetic outcomes, at the same time a reduced size of the instruments may affect their performance, with longer operative time [6].
Single-site robotic surgery (SSRS) and single-site laparoscopy (SSL) consist in a multichannel single trocar, inserted through a 2–3 centimetres transverse umbilical incision. Compared to multi-site surgery, single port surgery is associated with less post-operative pain and shorter recovery [12].
However, SSL is affected by less dexterity and loss of triangulation, thus it may not be the best choice when complex surgical procedures are required [12, 15].
On the other hand, thanks to articulated instruments, SSRS may overcome laparoscopy limitations. However, maybe due to its recent introduction and limited surgeons’ experience with this technique, SSRS has been associated with a higher rate of complications, compared to standard laparoscopy [15].
Thanks to all the advantages we mentioned, after its introduction, MIS was widely adopted in gynecologic cancer treatment. Most importantly, the publication of the LAP2 trial in 2009 provided reassuring evidence also in terms of oncological outcomes [5].
As a consequence, a minimally invasive surgical approach was implemented also in the treatment of cervical cancer (CC), until the publication of LACC study in 2018 [24].
The LACC trial reported an almost 4-fold increased recurrence risk and a 6.6-times higher likelihood of death associated with MIS, compared to open surgery in the treatment of early-stage cervical cancer.
These surprising results not only changed dramatically the surgical approach to CC, but also generated doubts on the safety of MIS in the treatment of endometrial and ovarian cancer (OC).
The present review aims to provide an updated scenario over the available evidence in the use of MIS in gynecological malignancies.
An electronic search was performed in double-blind by two authors (ES and GA). The analysis was conducted from August to September 2021. Research on Pubmed, Web of Science, and Scopus was carried out using the following keywords: ‘minimally invasive surgery’ and ‘gynecology’, “minimally invasive surgery” and “endometrial cancer”, “minimally invasive surgery” and “ovarian cancer”, “minimally invasive surgery” and “cervical cancer”.
The agreement about potential relevance was reached by consensus of the researchers and according to PRISMA statement guidelines. After the first selection, the authors evaluated the full-text copies of selected papers and separately extracted relevant data regarding study characteristics and outcomes. All bibliographies were analysed to evaluate additional eligible studies. Systematic reviews, meta-analyses, clinical trials, and original articles were included in the present review. Studies considered not in line with the purpose of the study, case reports, redundant studies, and articles not in the English language were excluded.
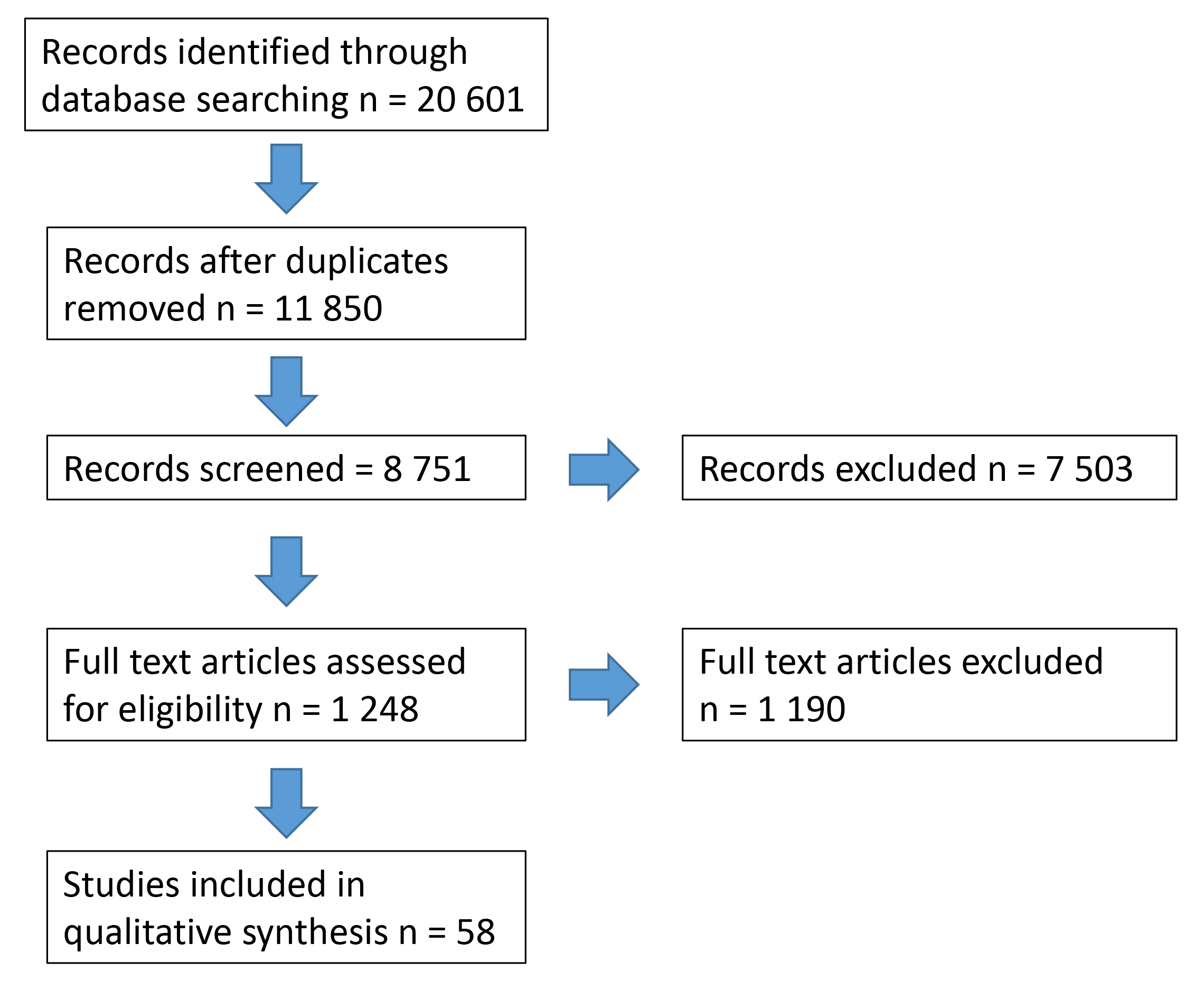
The electronic database search provided a total of 20,601 studies. Of whom, 11,850 duplicates, 1602 case reports, 2150 studies not in the English language, and 4940 works not fitting the review scope were excluded from the analysis. Fifty-eight studies were considered eligible for the study, 23 studies regarding MIS in endometrial cancer (Table 1, Ref. [4, 5, 7, 17, 20, 23, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41]), 19 studies on MIS in ovarian cancer (Table 2, Ref. [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60]), and 16 studies regarding MIS in cervical cancer (Table 3, Ref. [61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76]). The study selection flow-chart was reported in Fig. 1.
| Author, years | Design | Malignancy | Cases | Main results |
| Janda, 2010 [4] | Randomized clinical trial | Endometrial cancer | 332 | Quality of life improvements from baseline during early and later phases of recovery, and the adverse event profile, favour total laparoscopic compared with total abdominal hysterectomy for treatment of stage I EC. |
| Corrado, 2018 [23] | Retrospective cohort study | Endometrial cancer | 655 | Robotic surgery in severely obese women with endometrial cancer is feasible, safe, and reproducible. |
| Walker, 2009 [5] | Randomized clinical trial | Endometrial cancer | 2616 | Feasibility and improved safety profile of laparoscopic comprehensive surgical staging for uterine cancer when compared with the same procedures undertaken via laparotomy. |
| Janda, 2017 [29] | Randomized clinical trial | Endometrial cancer | 760 | Among women with stage I EC, the use of total abdominal hysterectomy compared with total laparoscopic hysterectomy resulted in equivalent disease-free survival at 4.5 years and no difference in overall survival. |
| Capozzi, 2021 [28] | Systematic review | Endometrial cancer | 769 | Both laparoscopic and robotic sentinel lymph node surgical techniques were found to be safe surgical procedures. |
| Perrone, 2021 [36] | Retrospective study | Endometrial cancer | 1221 | Robotic surgery and laparoscopy have similar efficacy and safety for endometrial cancer staging also for the high-risk endometrial cancer patients. |
| He, 2013 [25] | Systematic review | Endometrial cancer | 3616 | Compared with laparotomy, laparoscopic surgery seems to be beneficial in women with endometrial cancer, in particular insofar as postoperative complications and length of hospital stay. |
| Nieto, 2018 [40] | Retrospective study | Endometrial cancer | 94507 | The use of minimally invasive surgery is increasing rapidly for women with stage I-III nonendometrioid uterine tumors. Performance of minimally invasive surgery does not appear to impact survival adversely. |
| Monterossi, 2017 [39] | Retrospective cohort study | Endometrial cancer | 283 | Women with type II endometrial cancer submitted to MIS for hysterectomy experienced fewer complications and similar survival outcomes compared with those who underwent open surgery. |
| Galaal, 2018 [26] | Systematic review | Endometrial cancer | 3944 | For presumed early stage primary endometrioid adenocarcinoma of the endometrium, laparoscopy is associated with similar OS and DFS. Furthermore, laparoscopy is associated with reduced operative morbidity and hospital stay. |
| Gueli Alletti, 2021 [31] | Randomized trial | Endometrial cancer | 154 | The intrauterine manipulator does not affect the LVSI in early-stage endometrial cancer patients undergoing laparoscopic/robotic staging. |
| Scaletta, 2019 [41] | Systematic review | Endometrial cancer | 16425 | MIS appears to be safe in the management of high-risk EC patients, showing better perioperative and postoperative outcomes and comparable oncological outcomes than open surgery. |
| Capozzi, 2019 [20] | Retrospective study | Endometrial cancer | 132 | Minimally invasive techniques are preferable to open surgery both in terms of cost per patient and in terms of peri-operative complications in the setting of obese patients. |
| Gueli Alletti, 2015 [38] | Retrospective cohort study | Endometrial cancer | 89 | Telelap ALF-X approach is feasible and safe for endometrial cancer staging. |
| Bogani, 2014 [17] | Retrospective study | Endometrial cancer | 726 | In elderly women, laparoscopic surgery improves perioperative outcomes compared with open and vaginal approaches without compromising long-term survival. |
| Palomba 2012 [32] | Systematic review | Endometrial cancer | 12 | It is not currently possible to draw any definitive conclusions regarding incidence, risk factors, preventive measures, strategies of management, or prognosis of port-site metastasis after minimally invasive staging of EC. |
| Mourits, 2010 [7] | Randomized clinical trial | Endometrial cancer | 283 | The results showed no evidence of a benefit for total laparoscopic hysterectomy over total abdominal hysterectomy in terms of major complications, but total laparoscopic hysterectomy (done by skilled surgeons) was beneficial in terms of a shorter hospital stay, less pain, and quicker resumption of daily activities. |
| Martinez, 2010 [33] | Retrospective study | Endometrial cancer | 295 | The incidence of isolated port site metastasis can be maintained virtually to 0% by an adequate operative technique. We believe that port site metastasis in patients with uterine cancer cannot be used as an argument against laparoscopic staging in uterine cancer. |
| Cervical cancer | 921 | |||
| Cardenas-Goiocoechea, 2010 [35] | Retrospective study | Endometrial cancer | 275 | Robotic-assisted surgery is an acceptable alternative to laparoscopy for minimally invasive staging of endometrial cancer. |
| Gaia, 2010 [34] | Systematic review | Endometrial cancer | 1591 | Perioperative clinical outcomes for robotic and laparoscopic hysterectomy appear similar with the exception of less blood loss for robotic cases and longer operative times for robotic and laparoscopy cases. |
| Walker, 2012 [27] | Randomized clinical trial | Endometrial cancer | 2181 | Comprehensive surgical staging of endometrial cancer can be performed laparoscopically with relatively small differences in recurrence rates. |
| Iavazzo, 2013 [30] | Systematic review | Endometrial cancer | 534 | The available clinical evidence suggests that the application of uterine manipulators has no clear correlation with the recurrence of the endometrial carcinoma. |
| Gueli Alletti, 2019 [37] | Prospective multicentre trial | Endometrial cancer | 30 | Percutaneous surgical staging seems to be a feasible approach for endometrial cancer staging. |
| Author, years | Design | Malignancy | Cases | Main results |
| Jochum, 2020 [44] | Systematic review | Ovarian cancer | 7213 | An overwhelming consistency of the evidence suggests the likely effectiveness of minimally invasive surgery in selected cases of ovarian cancer, even in advanced stages. |
| Cardenas‑Goicoechea, 2019 [56] | Systematic review | Ovarian cancer | 3231 | Complete cytoreductive surgery after neoadjuvant chemotherapy via minimally invasive surgery appears feasible and safe in selected patients with advanced ovarian cancer. |
| Fagotti, 2019 [57] | Retrospective multicenter observational study | Ovarian cancer | 127 | A minimally invasive approach may be considered in the management of patients with advanced ovarian cancer who have undergone neoadjuvant chemotherapy. |
| Uccella, 2020 [60] | Systematic review | Ovarian cancer | 372 | MIS should be considered as a possible alternative to laparotomy for secondary cytoreduction of recurrent ovarian cancer in highly selected cases, at dedicated oncological centers and possibly in the context of well-conducted scientific research. |
| Abitbol, 2019 [54] | Retrospective cohort study | Ovarian cancer | 91 | Robotic surgery for the management of selected patients with ovarian, tubal, and peritoneal cancers in the interval debulking setting seems to be feasible and warrants further investigation as a surgical option. |
| Shi, 2019 [48] | Meta-analysis | Ovarian cancer | 647 | The robotic surgery and laparoscopy presented the same effect in the treatment of ovarian cancer. It failed to show oncological safety and recurrence by pathological stages or histologic types. |
| Matsuo, 2020 [45] | Retrospective trial | Ovarian cancer | 4822 | MIS procedures, in the treatment of early stage ovarian cancer, performed at hospitals with a higher surgical volume may be associated with improved short-term perioperative outcomes. |
| Gallotta, 2016 [43] | Retrospective cohort study | Ovarian cancer | 96 | There is no relevant difference between the robotic and laparoscopic approaches in staging early-stage ovarian cancer. |
| Gallotta, 2014 [50] | Multicentric retrospective study | Ovarian cancer | 300 | Patients with apparent early stage ovarian cancer can safely undergo laparoscopic surgical management. |
| Gueli Alletti, 2019 [42] | Systematic review | Ovarian cancer | 4423 | MIS in advanced ovarian cancer is comparable to the standard laparotomic management in terms of oncological outcomes but with improved perioperative and psychological results. The selection of patients is crucial to perform a successful surgery. |
| Gueli Alletti, 2017 [55] | Single-institution, propensity-matched study | Ovarian cancer | 93 | Minimally invasive interval debulking surgery seems to play an important role in the quality of life and oncologic outcomes. |
| Gallotta, 2017 [59] | Retrospective cohort study | Ovarian cancer | 58 | For selected patients, laparoscopy is a feasible and safe approach to optimal cytoreduction for patients with recurrent ovarian cancer. |
| Fagotti, 2008 [51] | Prospective clinical trial | Ovarian cancer | 113 | The “Fagotti score” appears a reliable and flexible tool to predict optimal cytoreduction in advanced ovarian cancer. |
| Park, 2013 [46] | Metaanalysis | Ovarian cancer | 346 | The operative outcomes of a laparoscopic approach in patients with early-stage ovarian cancer could be compatible with those of laparotomy. |
| Knisely, 2020 [47] | Systematic review | Ovarian cancer | 1509 | Existing studies do not demonstrate any deleterious survival effects associated with minimally invasive surgery for ovarian cancer. |
| Fagotti, 2015 [58] | Retrospective cohort trial | Ovarian cancer | 22 | The minimally invasive approach for secondary cytoreduction plus hyperthermic intraoperative intraperitoneal chemotherapy (HIPEC) is safe and efficient in terms of toxicity and postoperative outcomes for single isolated relapse. HIPEC should not be considered a major contraindication to a minimally invasive approach. |
| Gallotta, 2021 [49] | Retrospective study | Ovarian cancer | 254 | MIS can be offered in appropriately selected early stage ovarian cancer patients, since pathological and probably molecular features are more important than surgical approach to impact survival. |
| Nezhat, 2010 [52] | Retrospective study | Ovarian cancer | 32 | Laparoscopy can be used for diagnosis, triage, and debulking of patients with advanced ovarian, fallopian tube, or primary peritoneal cancer and is technically feasible in a well-selected population. |
| Fanning, 2011 [53] | Retrspective cohort trial | Ovarian cancer | 25 | It appears that laparoscopic-assisted cytoreduction has significantly less morbidity than laparotomy cytoreduction and produces survival similar to optimal laparotomy cytoreduction, but less than “ultraradical” laparotomy cytoreduction. |
| Author, years | Design | Malignancy | Cases | Main results |
| Nitecki, 2020 [63] | Systematic review | Cervical cancer | 9499 | Among patients undergoing radical hysterectomy for early-stage cervical cancer, minimally invasive radical hysterectomy was associated with an elevated risk of recurrence and death compared with open surgery. |
| Pedone Anchora, 2020 [71] | Multicentric retrospective study | Cervical cancer | 423 | The main determinant factor in the choice of surgical approach is a tumor diameter of 20 mm. Women with |
| Bogani, 2020 [76] | Retrospective case-control study | Cervical cancer | 70 | Primary conisation might overcome the risk of local recurrence after laparoscopic radical hysterectomy in early stage cervical cancer. |
| Brandt, 2020 [69] | Retrospective study | Cervical cancer | 196 | MIS approach did not seem to compromise oncologic outcomes in patients who underwent radical hysterectomy for early stage cervical carcinoma. |
| Chiva, 2020 [68] | International cohort observational study | Cervical cancer | 1272 | Minimally invasive surgery in cervical cancer increases the risk of relapse and death compared with open surgery. |
| Ramirez, 2018 [61] | Randomized clinical trial | Cervical cancer | 631 | In this trial, minimally invasive radical hysterectomy was associated with lower rates of disease-free survival and overall survival than open abdominal radical hysterectomy among women with early-stage cervical cancer. |
| Köhler, 2019 [65] | Retrospective study | Cervical cancer | 1389 | The combined laparoscopic-vaginal technique for radical hysterectomy with avoidance of spillage and manipulation of tumor cells provides excellent oncologic outcome for patients with early cervical cancer. |
| Capozzi, 2021 [75] | Systematic review | Cervical cancer | 1112 | Transperitoneal laparoscopic lymphadenectomy approach shows a higher rate of intraoperative complications compared to extraperitoneal laparoscopic lymphadenectomy for nodal staging in locally advanced cervical cancer, while no significant difference was found between the two techniques when postoperative complications were analyzed. |
| Melamed, 2018 [66] | Retrospective cohort study | Cervical cancer | 2461 | In an epidemiologic study, minimally invasive radical hysterectomy was associated with shorter overall survival than open surgery among women with stage IA2 or IB1 cervical carcinoma. |
| Kim, 2019 [70] | Retrospective matched cohort study | Cervical cancer | 724 | In patients with stage IB1, especially in those with cervical mass size |
| Cusimano, 2019 [67] | Retrospective cohort study | Cervical cancer | 958 | Minimally invasive radical hysterectomy is associated with increased rates of death and recurrence in patients with stage IB cervical cancer even after controlling for surgeon volume. |
| Paik, 2019 [64] | Multi.institutional retrospective cohort study | Cervical cancer | 476 | In this analysis, laparoscopic radical hysterectomy was associated with lower rates of disease free survival but not overall survival in early stage cervical cancer patients without adjuvant treatment. |
| Wright, 2012 [62] | Retrospective study | Cervical cancer | 1894 | Uptake of minimally invasive radical hysterectomy for cervical cancer has been slow. Both laparoscopic and robotic radical hysterectomies are associated with favourable morbidity profiles. |
| Salvo, 2021 [74] | Retrospective study | Cervical cancer | 646 | The 4.5-year disease-free survival rate did not differ between open and minimally invasive radical trachelectomy. |
| Kuznicki, 2020 [72] | Systematic review | Cervical cancer | 58 | Fertility sparing surgery of early cervical cancer with vaginal radical trachelectomy, abdominal radical trachelectomy, or minimally invasive radical trachelectomy have comparable oncologic outcomes in carefully selected patients, with reproductive outcomes favoring vaginal radical trachelectomy. |
| Nezhat, 2020 [73] | Systematic review | Cervical cancer | 3044 | Fertility-sparing surgery is a reasonable alternative to traditional radical hysterectomy for early-stage cervical cancer in women desiring fertility preservation. Minimally invasive approaches to fertility-sparing surgery had equivalent oncologic outcomes compared with an abdominal approach. |
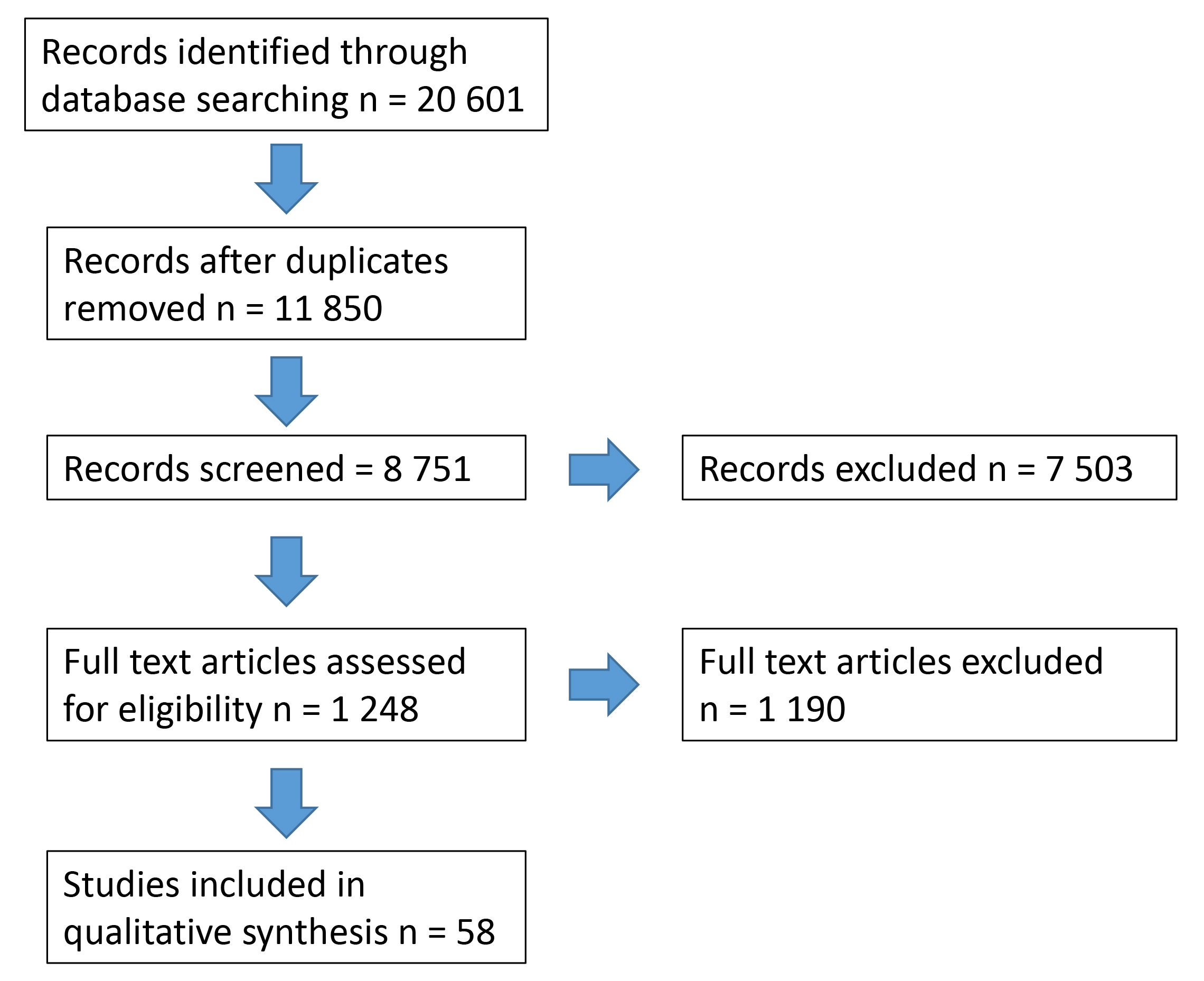 Fig. 1.
Fig. 1.Prisma study flow diagram.
The total of patients enrolled was 180,057, 131,430 in the EC group, 23,774 in the OC groups, and 24,853 in the CC group.
To illustrate the results of the research, the main findings are reported in chapters and distinguished for the type of gynecological malignancy.
EC is the most common gynecologic malignancy in developed countries, accounting for over 60.000 cases each year in the United States [77]. Five-year overall survival (OS) ranges from 74 to 91% in patients without distant metastasis. Surgery is the main treatment for early-stage EC cases. Obesity and older age are the main risk factors for EC. Other risk factors for EC include nulliparity, unopposed estrogen intake, and late menopausal state.
Thanks to the early presentation of symptoms and a prompt diagnosis, surgery is often curative [78]. Surgical staging for EC includes hysterectomy, salpingo-oophorectomy, and lymph node assessment [79, 80, 81, 82]. At present, MIS is the gold standard approach in the case of EC confined to the uterus [83, 84]. Traditionally surgery was performed in laparotomy, but since the advent of laparoscopy in 1990, several studies demonstrated that laparoscopic surgery is a feasible option.
Current guidelines published in 2020 by the European Society of Gynaecological Oncology, the European Society for Radiotherapy and Oncology, and the European Society of Pathology (ESGO/ESTRO/ESP) [85] define minimally invasive approach as the preferred surgical option in early-stage EC, while, extension outside the uterus and cervix are contraindication to MIS [86, 87, 88]. According to the American College of Obstetricians and Gynecologists and the National Comprehensive Cancer Network (NCCN), MIS should be the standard surgical approach for EC [89].
Several RCT compared laparotomy to laparoscopy. In a systematic review conducted by Hong Ying He, considering 9 RCT, laparoscopy is associated with a longer operating time and a minor length of hospital stay [25]. Furthermore, a higher rate of intraoperative complications was reported in patients who underwent MIS. In the Authors’ opinion, the higher rate of intraoperative complications may be due to the little experience with laparoscopy at the time of the study (1996). Moreover, the high number of patients assigned to the “laparoscopy group” enrolled in the LAP2 study (1696 vs 920 assigned to the laparotomy group), influenced the results of all systematic reviews citing this data [5].
On the other hand, when considering major intraoperative complications, such as bladder, ureteric, bowel, and vascular injury, a Cochrane published in 2018 showed no differences between laparoscopy and laparotomy [26].
In 2009 a randomized prospective study on 2600 patients was conducted. The LAP2 study demonstrated that laparoscopy is associated with a lower rate of complications, low intraoperative blood loss, and a minor length of hospital stay compared to laparotomy [5, 27].
Laparoscopy has benefits also in short-term outcomes, such as recovery after surgery, hospital stay, adverse events, and quality of life after the intervention [4, 90, 28].
In 2012 an ancillary analysis of the LAP2 trial was conducted [27]. The authors reported only small differences in laparoscopy compared to laparotomy and a slight increase in recurrence rate for patients treated with laparoscopy, not statistically significant. No differences were shown in OS, recurrence-free survival (RFS), and patterns of recurrent disease.
Recently, the LACE trial compared total laparoscopic hysterectomy (n = 353) with total abdominal hysterectomy (n = 407) in the stage I EC treatment [4]. The results showed equivalent survival outcomes in the two groups [29].
Regarding the pattern of recurrence, concerns were raised for the hypothetic risk of augmented frequency of vaginal cuff recurrence and the possible localization at the port site [91]. In the analysis conducted in 2012 on recurrence and OS in patients enrolled in the LAP2 study, no statistically significant difference was found in vaginal recurrence between laparoscopy and laparotomy [27].
Iavazzo et al. [30] reported no clear correlation between the uterine manipulator and recurrence. Different authors suggested sealing the tubes and minimizing the movements of the uterine manipulator during the intervention to overcome this risk.
A recent prospective randomized clinical trial (ROMANHY trial) investigated the influence of the use of intrauterine manipulators (IUM) on lymphovascular space invasion (LVSI) status and peritoneal cytology. However, no difference was found between the two groups with no adverse impact of IUM on OS and disease free survival (DFS) [31].
Concerning port site metastasis, they may be related to understaging of microscopic EC localization and not to laparoscopy per se [32]. On the other hand, safe deflation through the trocars has been suggested by some authors to reduce the risk of port-site metastasis [33]. In the LAP2 study, 4 port-site recurrences were described, and ¾ occurred in patients with advanced disease [5].
At present, no prospective trials are investigating the safety of robotic surgery in the treatment of EC patients. However, data from retrospective case series and metanalysis reported similar advantages for robotic surgery and laparoscopy in the reduction of intraoperative complications compared to laparotomy, without detriment of oncological outcomes [34, 35].
Moreover, recent retrospective studies showed that robotic surgery may be a better choice compared to laparoscopy in EC treatment, with a lower rate of conversion to laparotomy, and a higher rate of nodal assessment accomplished especially in obese patients [23, 36].
After the publication of the LAP2 trial, laparoscopy became the gold standard for EC treatment [5, 27]. While several clinical trials demonstrated the safety and effectiveness of MIS for low-risk EC [37, 38], only a few retrospective studies have been published regarding safety in high-risk EC cases. A minimally invasive approach may be extremely beneficial in this set of patients, thanks to enhanced recovery and reduced morbidity.
Monterossi et al. [39] conducted a wide retrospective analysis on patients with type II EC, 141 patients underwent laparotomic surgery and 142 patients underwent MIS. The Authors concluded MIS was a safe approach also in this setting of patients, with favorable oncological outcomes. Conversely, patients with stage III who underwent laparotomy had a better OS than the MIS group.
In 2018 an analysis on the National Cancer Database was conducted, to assess the use of MIS in uterine cancers (n = 94,507) in the subset of high-risk histologic subtypes. The authors found no difference in OS in patients who underwent MIS compared to the laparotomic approach [40].
In conclusion, current evidence regarding the safety and feasibility of MIS in the setting of high-risk EC is limited and comes exclusively from retrospective trials. Available data suggest that high-risk EC is not a contraindication to an MIS approach and oncological outcomes appear not to be affected [41]. Nevertheless, strong evidence from large prospective trials is still lacking.
OC accounts for almost 20,000 new cases per year in the United States [77]. Differently from EC, OC is associated with high mortality rates and advanced stage at diagnosis. Globally, OC is the eighth most common cause of cancer-related death in women, with a five-year survival rate below 45% .
The OC standard treatment includes surgery plus intravenous chemotherapy. The main prognostic factor in ovarian cancer treatment is a complete cytoreduction at primary debulking surgery (PDS). However, in almost 80% of cases, OC is at advanced stage at the time of presentation.
Often, due to the spreading of the disease at the time of diagnosis, upfront surgery may require invasive and destructive surgery, with inacceptable morbidity, or a complete resection of gross tumor may not be feasible at upfront surgery. In these cases, patients are candidate to neoadjuvant chemotherapy followed by interval debulking surgery (IDS), to remove bulky disease and improve response to adjuvant chemotherapy.
In order to maximise benefits from chemotherapy on tumor burden and microscopic residual disease on peritoneal surfaces, the use of hypertermic intraperitoneal chemotherapy (HIPEC) and, more recently, of pressurised intraperitoneal aerosol chemotherapy (PIPAC) has been proposed at the time of primary or secondary cytoreductive surgery for OC [92]. However, currently there are no large, prospective randomized trials supporting their use in the routine practice [93].
Currently, there is equivocal and limited evidence about the use of MIS in OC patients [42, 94].
According to the current guidelines [93], the standard procedure for OC treatment and staging is open surgery. The open approach allows better macroscopical exploration and removal of the gross tumor without mass rupture. Laparotomy is believed to be superior at identifying occult metastasis through increased exposure and palpation that could otherwise be missed by MIS [95]. In clinical practice, MIS has been considered with encouraging results for early-stage ovarian carcinomas in high volume centres with experienced surgeons [43, 44, 45]. Available data show that MIS represents a safe option for the diagnosis and staging of early-stage OC [46]. However, nowadays no prospective randomized trials have been published yet about the safety of MIS in OC treatment [47, 48, 96].
Possible limitations of a minimally invasive approach derive from the risk of cyst rupture with cells spillage and a hypothetical suboptimal evaluation of the abdominal cavity. A careful selection of eligible patients and the use of a protected bag may overcome the risk of cells tumor spreading [49]. Gallotta et al., [50] in a large retrospective trial, reported an enhanced recovery after MIS compared to open surgery, an optimal retroperitoneal assessment, and an MIS non-inferiority in terms of oncological outcomes with respect to laparotomy.
In the context of advanced stage OC, staging laparoscopy is a largely accepted tool to candidate patients to upfront surgery or neoadjuvant chemotherapy. Fagotti et al. [51] proposed a laparoscopic scoring system to evaluate the feasibility of an optimal cytoreduction. This scoring system has been validated in prospective trials. Furthermore, an accurate selection of patients is crucial to avoid unnecessary laparotomy when optimal cytoreduction is not achievable.
Current international guidelines mention the execution of a diagnostic laparoscopy as a part of the diagnostic workup in advanced ovarian cancer, to obtain detailed information about the intra-abdominal disease burden and a histopathological diagnosis [93].
Concerning MIS as a treatment option in advanced stage OC, only a few, retrospective, non-randomized studies have been published on this topic. The need for an accurate assessment of residual disease and for the performance of major surgical procedures, such as bowel resection and upper abdominal surgery, limits the employment of minimally invasive approach.
However, the possibility for a successful laparoscopic approach also in case of diaphragmatic involvement has been reported [97].
Nezhat et al. [52] reported a case series on 32 patients with advanced ovarian cancer who underwent laparoscopic staging. In 17 cases a laparoscopic cytoreduction was performed, 11 patient underwent laparotomic cytoreduction. The assignment to laparoscopic debulking surgery vs open surgery was left to surgeon judgement. The results showed an higher rate of complete cytoreduction and a longer DFS in the laparoscopy group. However a bias of selection must be considered, since patients were not randomized to laparoscopic vs laparotomic cytoreduction.
Fanning et al. [53] published a study of 25 patients with advanced stage ovarian cancer who underwent laparoscopic PDS. Only in in the 36% of cases a complete cytoreduction was achieved.
In conclusion, currently there is not enough evidence to consider MIS a safe option for PDS in advanced stage OC. Moreover, there is a lack of objective criteria to select patients who may benefit from this approach, without detriment of oncological outcomes.
There are also some concerns in the employment of MIS in IDS, such as the inability to assess completely the abdominal cavity, which raises the question of whether the approach can yield the same rates of complete resection compared with an open approach.
The feasibility of minimally invasive IDS in selected patients, with optimal response to chemotherapy, has been explored in small, non-randomized, retrospective studies [54]. IDS is the main option in patients with unresectable disease at the time of diagnosis or in patients with poor physical conditions, who may benefit from a less extensive surgical treatment [98, 99]. IDS increases the rates of optimal cytoreduction with less surgical morbidity and without affecting oncological outcomes [55, 56].
Currently, there are no strict recommendations about the ideal patient to candidate to IDS or the best surgical approach, nevertheless, MIS is not the standard treatment. The international MISSION study, which included 127 OC patients with partial and complete response to neoadjuvant chemotherapy, showed no differences in OS in the case of low complexity cytoreductive surgery between MIS and laparotomy [57].
However, in the absence of large prospective randomized trials, nowadays there is no strong evidence available regarding an adequate assessment of residual disease in IDS with MIS compared to laparotomy, as a consequence there is not enough reassuring evidence about the oncological safety of MIS in this setting of patients. Moreover, a minimally invasive approach would not be the preferred choice in case of complex surgery, such as bowel resection, diaphragm stripping, and retroperitoneal dissection.
In a recent meta-analysis comparing the performance of IDS with MIS, the author affirmed that optimal cytoreduction can be accomplished via MIS in patients with complete clinical response to chemotherapy and low tumor load on diagnostic laparoscopy [56].
Currently, the LANCE trial is an ongoing international, prospective, multicentre randomized phase III trial comparing MIS interval cytoreductive surgery vs open surgery in terms of DFS. Results from this study may offer more definitive evidence about the MIS role in OC patients [100]. Considering the feasibility of MIS as a staging procedure in advanced OC and the potential survival benefit deriving from intraperitoneal chemotherapy, the association of MIS and HIPEC or PIPAC during surgery for OC has been explored. Currently, intraperitoneal chemotherapy should not be considered a standard procedure, however MIS is not a contraindication for intraperitoneal chemotherapy [58].
Concerning recurrent OC, surgical treatment plus chemotherapy has no clear benefit in terms of OS and RFS compared to chemotherapy alone. Surgical treatment should be considered only in case of complete cytoreduction at cytoreductive surgery, good performance status of the patient and platinum-sensitivity [101].
In recurrent OC, MIS is a useful tool to assess the extension of recurrent disease and the feasibility of a surgical treatment [101, 102]. In a recent retrospective study, the potential role of MIS has been evaluated in 58 patients with single relapse, platinum sensitive OC, with evidence of safety and optimal secondary cytoreduction [59].
A recent systematic review of the literature including 372 patients with OC recurrence [60], affirms that MIS is a safe and feasible option compared to laparotomy in selected patients, with single-site recurrent disease or few localizations of relapses, in the context of highly specialized centres with skilled surgeons.
Fagotti et al. [58] conducted a retrospective analysis on 22 patients with recurrent OC, eligible for surgery, who underwent MIS secondary cytoreductive surgery (SCS) or open SCS with HIPEC. The results showed evidence of benefit in terms of postoperative outcomes in the MIS group. However, oncological outcomes were not discussed in this study.
CC is the fourth most common malignancy in the world. In 2020 CC accounted for 13,800 new cases in the United States [77]. Differently from other malignancies, due to the implementation of tools for prevention and early detection, its incidence and related mortality have dramatically decreased in the last 50 years, but only in those countries with access to cytological screening programs [103].
CC is still the most common gynecologic malignancy in low-income countries and an important cause of morbidity and mortality, due to the lack of resources to support screening and local prevention programs.
The standard treatment for CC is radical hysterectomy and pelvic lymphadenectomy. In 1992 MIS was introduced in CC treatment. For 25 years, multiple retrospective publications reported the feasibility, advantages, and oncologic safety of the minimally invasive approach .
Radical hysterectomy was reported to be safely accomplished with MIS, with better postoperative outcomes compared to open surgery [62]. Moreover, promising results were reported with robotic radical hysterectomy compared to laparoscopy, thanks to a major dexterity, of great value in radical procedures, less intraoperative complications and apparently, good oncological outcomes [104].
Before 2018, international guidelines [105, 106] recommended both open surgery and MIS for early-stage CC patients.
The publication of the LACC trial in 2018 imposed a change in the recommendation for CC surgical treatment approach [61]. This prospective randomized trial showed that MIS had lower DFS and OS compared to the open approach. Unexpectedly, randomization and recruitment were suspended because of a higher rate of recurrences and death in the group randomized for MIS. Women randomized to the minimally invasive arm experienced almost 4 times the risk of recurrence and 6 times the risk of death compared with women randomized to laparotomy.
The reasons for the MIS inferior outcomes are not known yet. The use of IUM, the effect of CO2 insufflation on tumor cells’ spread, and open colpotomy have been discussed as possible causes [63, 64]. In the hypothesis of tumor spreading during cervical manipulation, various surgical strategies have been proposed, including the Kohler vaginal cuff performed before surgical treatment [65]. Anyway, definitive oncological safety must be proven with prospective trials.
A recent metanalysis [63] aimed to discuss the results from the LACC trial with available “real world metanalysis”, comparing the risk of recurrence and death between patients who underwent minimally invasive vs open radical hysterectomy for early-stage CC. The selection included only higher quality observational studies and the results confirmed the LACC trial’s results. Furthermore, several retrospective trials corroborated these findings and the international guidelines were updated according to the most recent evidence [66, 67].
In the SUCCOR study, an observational multicentre European retrospective cohort
study, the authors confirmed the MIS inferiority compared to open surgery. On the
other hand patients with previous conisation and with tumor size
Regarding the relation between tumor size and the detrimental effect of MIS,
different retrospective trials reported the MIS non-inferiority compared to open
radical hysterectomy in terms of DFS and/or OS for tumor size
In conclusion, MIS may be considered is in case of tumor size
Currently, MIS is an accepted option when fertility-sparing surgery is feasible, such as laparoscopic-assisted vaginal radical trachelectomy and laparoscopic radical trachelectomy [72, 73, 74]. Laparoscopy is also the preferred surgical route for nodal surgical staging, before concurrent chemo/radiotherapy and in case of fertility-sparing surgery [75].
Furthermore, a minimally invasive approach may be considered after conisation without residual disease (stage IA1, IA2 cervical cancer), in patients requiring hysterectomy [76].
Two prospective randomized trials exploring the role of MIS in patients with CC have recently been initiated. The first is the RACC trial, a Swedish multicentre prospective trial comparing robotic vs open surgery for the treatment of early-stage CC [107]. The use of an IUM is not allowed, and the closure of the vagina before colpotomy is recommended but not mandatory. The second one is a multicentre randomized controlled trial designed in China, with a planned enrolment of 1448 patients [108]. In their protocol, the use of an IUM and the method of vaginal excision are to be reported. These trials may provide stronger evidence concerning the safest treatment of early-stage CC patients.
According to the available evidence and current clinical practice, MIS should be the treatment of choice in the major part of surgical gynecological conditions. In particular, MIS is undoubtedly the gold standard for early-stage EC treatment and may represent an acceptable option even in high-risk EC patients. Concerning OC, MIS is a safe and useful tool for staging purposes in advanced-stage disease, and a treatment option only in high volume centres with expert oncologic surgeons.
On the contrary, MIS should be abandoned in the context of CC, exception made for well-selected patients, who received adequate counselling about current evidence.
ES—Conceptualization, Methodology, Writing and original draft, Writing and review & editing. GA—Conceptualization, Methodology, Writing and original draft, Writing and review & editing. DB—Data curation, Software and supervision. GB—Data curation, Software. ADF—Visualization, Investigation. LM—Visualization, Investigation. AV—Software, Validation. IR—Software, Validation. DS—Software, Validation. All authors read and approved the final manuscript.
Not applicable.
Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.