

 , Nafiye Yilmaz 2, Eser Colak 1, Nilufer Bayraktar 3, Yusuf Aytac Tohma 4, Hulusi Bulent Zeyneloglu 4
, Nafiye Yilmaz 2, Eser Colak 1, Nilufer Bayraktar 3, Yusuf Aytac Tohma 4, Hulusi Bulent Zeyneloglu 41 Department of Gynecology and Obstetrics, Faculty of Medicine, Baskent University, 42080 Konya, Turkey
2 Department of Reproductive Endocrinology, Ministry of Health Ankara City Hospital, 06800 Ankara, Turkey
3 Department of Biochemistry, Faculty of Medicine, Baskent University, 06810 Ankara, Turkey
4 Department of Reproductive Endocrinology, Faculty of Medicine, Baskent University, 06810 Ankara, Turkey
Academic Editor: Antonio Simone Laganà
Abstract
Background: The current study tested the level of endocan, which is
thought to have an effective role in both endothelial dysfunction and
inflammation, in infertile women with endometriosis treated with in
vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI). It is based on
the hypothesis of chronic inflammation in the pathophysiology of endometriosis.
Methods: This prospective case–control study included a total of 64
women who were in the IVF/ICSI program. The women were divided into two groups:
endometriosis (n = 32) and non-endometriosis (n = 32). Their baseline
characteristics, stimulation parameters, and IVF/ICSI outcomes (clinical
pregnancy and live birth rates) were recorded. Blood samples collected at the
beginning of the IVF cycle for endocan levels were analyzed with a sandwich
enzyme immunoassay and the results were documented. Results: The endocan
levels in the endometriosis group were significantly higher than those in the
non-endometriosis group, i.e., 5010 pg/mL and 2738 pg/mL, respectively
(p
Keywords
- Endocan
- Endometriosis
- in vitro fertilization
Endometriosis is seen in about 5%–10% of women in the reproductive age group. Although the retrograde menstruation theory was first proposed, its pathophysiology has not been elucidated. Endometriosis is associated with the inflammatory response and this process is thought to be associated with endothelial dysfunction and carcinogenesis. Inflammatory mediators (TNF-alpha, IL-1b, and IL-6) in the endometrial tissue were increased in cDNA array analysis in cases of endometriosis [1]. It has also been reported that inflammatory cells (neutrophils and macrophages) show higher chemotactic activity throughout the menstrual cycle in women with endometriosis compared to women with normal endometrium [2]. T cell expression and the CD4/CD8 ratio are also higher than in those with ectopic endometrium [3]. In addition, endometriosis inhibits endothelial function [4]. Endometriosis is also a risk factor for severe pelvic inflammatory disease. Thus, inflammation is both cause and effect. The intraperitoneal inflammation effect of endometriosis in infertile patients is emphasized [1, 5]. Interestingly, it is stated in recent reviews that exposure to environmental endocrine disrupting chemicals (phthalates, bisphenols, and pesticides) and genital subclinical infections may affect the development of endometriosis by causing permanent immune dysregulation. The vulva and cervicovaginal microbiota are affected, the local defense mechanism and homeostasis are impaired, and a subclinical inflammatory response occurs [6].
The spontaneous monthly fecundity rate in endometriosis patients is between 2% and 10%, which is lower than that in healthy women. ART can be recommended in the event of inability to conceive despite surgery, unsuccessful insemination attempts, or other reasons for infertility. It is predicted that the chance of pregnancy is lower when advanced disease is detected (moderate-severe endometriosis or deep infiltrative), and in vitro fertilization (IVF) may be recommended as the first option in these patients [7, 8]. It has been reported that women with endometriosis who underwent IVF have lower fertilization rates. These results may be due to high cytokine levels and deterioration of oocyte quality [9].
Endocan (endothelial cell-specific molecule 1 [ESM-1]) is a unique soluble dermatan sulfate proteoglycan derived from the endothelium. It has the ability to bind to various bioactive molecules associated with cellular signaling and adhesion and thus regulates the proliferation, differentiation, migration, and adhesion of different cell types. An increase in the tissue expression or serum level of endocan reflects endothelial activation and neovascularization, which are marked pathophysiological changes associated with inflammation and tumor progression. Endocan has been studied as a blood-based and tissue-based biomarker for numerous cancers and inflammation and yielded promising results. Endocan has been shown to play a critical role in terms of mitogenic and migratory effects on vascular endothelium induced by vascular endothelial growth factor (VEGF) [10]. It has an influence on endothelial dysfunction as a mediator of systemic inflammation and is associated with cardiovascular disease [11]. Different studies support its role in systemic inflammation [12]. Additionally, there are studies documenting higher endocan levels in endometrial and ovarian cancer [13]and women with polycystic ovary syndrome [14, 15] compared to control groups. Moreover, in a recent study, higher endocan levels were reported in women with endometriosis compared to the control group. It has been reported that endocan has higher sensitivity than CA 125 in predicting endometriosis (93% and 87%, respectively) [16].
The main purpose of our study was to compare the endocan levels of women with endometriosis who started IVF with women without endometriosis. It was investigated whether there is a relationship between endocan levels and clinical pregnancy and live birth rates. It has been hypothesized that women with endometriosis, who are thought to have chronic inflammation in the foreground, have high endocan levels and this reduces the implantation of the embryo.
This study was designed prospectively and approved by Baskent University Institutional Review Board and Ethics Committee (Project no: KA19/139, 09.07.2019) and supported by Baskent University Research Fund. Power analysis was performed using G Power 3.1 (Düsseldorf, Germany) [17]. The sample size calculation was done by two-tailed power analysis with a test comparing two independent groups based on mean endocan levels. During the design of our study, a pilot study was conducted because there was no identical study in the literature. Endocan levels of 10 patients from both groups were measured and the effect size was determined as 0.73. Based on the pilot study, the sample size that provides a significant difference between the two groups after the power analysis was 62 subjects, with a minimum of 31 subjects for each group (alpha: 0.05, power: 80%, Cohen’s d: 0.73). A total of 64 women who underwent IVF/intracytoplasmic sperm injection (ICSI) cycles between June 2019 and March 2020 met the criteria and were included in the study.
The study (endometriosis) group consisted of 32 infertile women undergoing IVF/ICSI treatment with endometriosis that was diagnosed by laparoscopy, magnetic resonance imaging (MRI), or ultrasonography (USG). Twenty-two women in the endometriosis group were diagnosed laparoscopically. The other ten patients were diagnosed with endometrioma ultrasonographically (homogeneous persistent diffuse low-level echoes without neoplastic components) and had symptoms of endometriosis (dysmenorrhea, dyspareunia, chronic pelvic pain, pain with bowel movements or urination, or excessive bleeding). The ultrasound images were confirmed by MRI. The control group (non-endometriosis) consisted of 32 women undergoing IVF/ICSI treatment without endometrioma and endometriosis symptoms. Women with any ovarian cyst or at least one suspected symptom of endometriosis were excluded from the study for the control group. Women who were diagnosed with a disease that led to chronic inflammation (diabetes mellitus, hypertension, malignancy, thyrotoxicosis, or urticaria) in the last year, women who had had an infection or leukocytosis in the last month, and women who had used an antiaggregant in the last month were excluded from the study. Written informed consent was obtained from every woman for the use of their data.
Controlled ovarian hyperstimulation was applied as a short antagonist protocol and fresh embryo transfer was planned for all cycles. Gonadotropin (GND) dose (follitropin alfa and/or human menopausal gonadotropin) was determined based on antral follicle count (AFC), women age, and BMI. Then, the dose was adjusted with serial USG and E2 measurements. An oocyte trigger was applied when the mean diameter of two or more follicles was 17 mm. Oocyte retrieval was performed transvaginally under general anesthesia 36 h after the trigger application. Choriogonadotropin alfa was administered as a trigger in all cycles. Embryo transfer was performed at the cleavage or blastocyst stage 2–5 days after oocyte retrieval. Two embryos were transferred to six patients in the endometriosis group and four patients in the non-endometriosis group. Since the embryo did not develop, transfer was canceled in 4 cycles in the endometriosis group. Single embryo transfer was performed in all other patients. The luteal phase was supplemented by transvaginal administration of micronized progesterone (Crinone gel, Merck Group, Darmstadt, Germany) from the day of oocyte recovery.
Age, BMI, duration of infertility, indication of IVF treatment, hormone levels (Fsh, E2, Lh), and AFC were recorded as baseline characteristics. Controlled ovarian hyperstimulation (COH) monitoring parameters, total dose of GND used, endometrial thickness on the trigger day, the total number of oocytes retrieved, MII oocyte count, and the number of obtained embryos were noted. Clinical pregnancy was determined by the presence of at least one gestational sac documented by transvaginal USG two weeks after a positive pregnancy test. Live birth rates were calculated by dividing the number of pregnancies resulting in live births by the number of cycles with embryo transfer. Endocan levels in the blood samples were analyzed by a clinical biochemist in the laboratory and the results were recorded.
Samples taken using a serum separator tube were maintained at room temperature
for 2 hours. They were then centrifuged at 4
Serum ESM-1 level was measured by sandwich enzyme immunoassay using 96-well
microplates (Cloud-Clone Corp. CCC, Wuhan, China) according to the manufacturer’s
instructions. The detection limit was 6.2 pg/mL. The intra- and interassay
variabilities were 10% and 12%, respectively. The microplate provided in this
kit is pre-coated with an antibody specific for ESM-1. The samples were then
added to the appropriate microplate wells with ESM-1-specific biotin-conjugated
antibody and incubated at 37
SPSS 25.0 (Başkent University licensed, IBM Corporation, Armonk, NY, USA)
was used in the analysis of variables. The compliance of the data to a normal
distribution was evaluated with the Shapiro–Wilk test and variance homogeneity
with the Levene test. Student’s t-test and the Mann–Whitney U test were
used in comparing two independent groups with each other. In a comparison of
categorical variables with each other, Pearson’s chi-square and Fisher’s exact
tests were used. In cases where the expected frequencies were less than 20%, an
evaluation was made with the Monte Carlo simulation method to include these
frequencies in the analysis. The cut-off values according to the parameters were
evaluated by ROC analysis. The area under the curve, sensitivity, and specificity
were calculated. Quantitative variables are mean
Sixty-four GnRH antagonist cycles were screened prospectively. There were no
significant differences in terms of age, BMI, or baseline characteristics (E2,
Lh, FSH, AFC, duration of infertility, and indication of IVF treatment) between
the endometriosis (n = 32) and non-endometriosis (n = 32) groups (p
| Endometriosis | p value | |||
| No | Yes | |||
| (n = 32) | (n = 32) | |||
| Mean |
Mean | |||
| AGE | 31.25 |
32.75 |
0.243 | |
| BMI (kg/m |
23.5 (16–33) | 24.0 (19–35) | 0.62 | |
| FSH (day 2) (mIU/mL) | 7 (2–14) | 6.5 (2–15) | 0.98 | |
| Lh (day 2) (mIU/mL) | 5 (2–10) | 5 (2–13) | 0.97 | |
| E2 (day 2) (pg/mL) | 36.0 (10–140) | 37.5 (8–157) | 0.45 | |
| Peak E2 (pg/mL) | 1545.38 |
2099.75 |
0.009 | |
| Peak progesterone (ng/mL) | 0.45 (0.10–1.90) | 0.65 (0.10–1.70) | 0.06 | |
| Gonadotropin dose (IU) | 1800.0 (1150–4500) | 2080.0 (1200–5400) | 0.33 | |
| Number of total oocyte | 9.0 (2–16) | 8.0 (1–20) | 0.43 | |
| Number of MII oocyte | 8.0 (1–14) | 6.5 (0–17) | 0.483 | |
| Number of embryos | 4.5 (1–12) | 3.5 (0–11) | 0.382 | |
| Endometrium thickness | 10.0 (8–15) | 10.0 (5–15) | 0.83 | |
| ENDOCAN level (pg/mL) | 2738.0 (604–8875) | 5010.5 (867–10456) | 0.024 | |
| n (%) | n (%) | |||
| Grade of embryos | ||||
| Clivage (stage) | 26 |
18 |
0.040ŧ* | |
| Blastocyst | 6 |
10 |
||
| None | 0 |
4 |
||
| Antral folicle count | ||||
| 1–4 | 3 (9.4) | 4 (12.5) | 0.747ŧ | |
| 5–9 | 11 (34.4) | 13 (40.6) | ||
| 18 (56.3) | 15 (46.9) | |||
| Indication of ART | ||||
| Unexplained | 13 (40.6) | 14 (43.8) | 0.945ŧ | |
| Male factor | 10 (31.3) | 11 (34.4) | ||
| Poor ovarian reserve | 6 (18.8) | 5 (15.6) | ||
| Tubal factor | 3 (9.4) | 2 (6.3) | ||
| Clinical pregnancy | ||||
| Positive | 18 (56.3) | 11 (34.4) | 0.079ŧ | |
| Live birth rate | 16 ( 50) | 8 (25) | 0.039ŧ* | |
| Duration of infertility | ||||
| 11 (34.4) | 10 (31.3) | 0.999ŧ | ||
| 21 (65.6) | 22 (68.8) | |||
| Endocan level | ||
| r | p value | |
| Clinical pregnancy rate | –0.88 | 0.492 |
| Live birth rate | –0.103 | 0.418 |
| Endometriosis (yes) | 0.284 | 0.023 |
| Peak estradiol level | 0.116 | 0.36 |
| Spearman’s rho Test (two-tailed), r, Correlation coefficient; *bold value means
p | ||
The limit values determined for endometriosis as a result of ROC analysis
performed according to the endocan cut-off value are statistically significant
(p
| Variable | Cut off value | Endometriosis | p value | |
| No | Yes | |||
| n | n | |||
| Endocan | 25 | 15 | 0.0161* | |
| 7 | 17 | |||
| Sensitivity (95% CI)/Specificity (95% CI) | PPV/NPV | AUC | ||
| 53.13 (34.7–70.9)/78.12 (60.0–90.7) | 70.8 (%)/62.5 (%) | 0.664 | ||
| Roc Curve Analysis, Se, Standard error; AUC, Area under the ROC curve; PPV,
positive predictive value; NPV, negative predictive value; *bold value means p | ||||
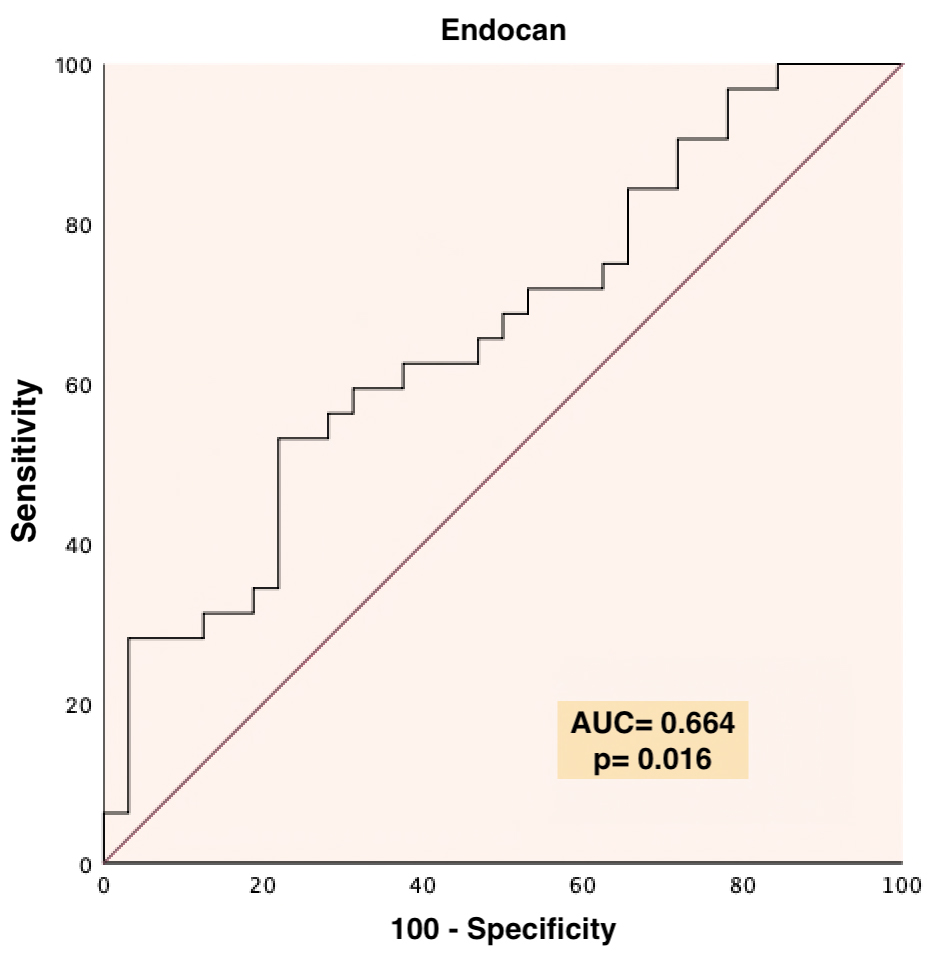 Fig. 1.
Fig. 1.ROC curve for endocan (with cut-off value calculated for Endometriosis).
Based on the ROC analysis performed according to the endocan cut-off point,
there was no statistically significant difference between the values below and
above the endocan cut-off value determined for the clinical pregnancy and live
birth rates (p
In our research, women with endometriosis undergoing IVF/ICSI treatment had significantly higher endocan levels than those without endometriosis did; however, live birth rates were significantly lower. Although endocan levels contribute to the prediction of endometriosis, we did not find any predictive effects on clinical pregnancy or live birth rates.
ESM-1 was first described in 1996 by Lassale et al. [18]. It has been reported that it may have strong effects on vascular cell biology and is associated with inflammation. Subsequent articles reported that endocan plays a role in the development of vascular tissue in health and disease. In particular, the expression in the “tip cells” of developing blood vessels significantly increased [10, 19]. Actual evidence suggests that the increase in endocan expression induced by pro-angiogenic factors (VEGF, FGF-2) is associated with tumor neovascularization, angiogenic change in stem cells, and remodeling [20]. In fact, increased endocan expression has been reported in tumors with high neovascularization such as the lung, colon, liver, and kidney [21, 22, 23, 24]. In recent studies, increased endocan levels were reported in both ovarian and endometrial cancer, but this elevation was not detected in the healthy and benign controls [13]. A study of this proteoglycan showed that women with polycystic ovary syndrome have increased endocan levels, which may predict an increased risk of cardiovascular disease [14, 15]. However, a comparative study involving women with premature ovarian failure did not report any changes in endocan levels [25].
Endometriosis is a chronic inflammatory, progressive, hormone-dependent
disease. Its etiopathogenesis is multifactorial and it can lead to infertility in
diverse ways [7]. The most highlighted theory is the inflammatory process, which
leads to retrograde menstruation [1]. The relation between inflammation on
peritoneal surfaces and infertility has been emphasized in the literature [1, 5].
It may also reduce fertility by decreasing oocyte quality and degradation in
endometrial receptivity. Surgical and medical approaches can be applied to ensure
fertility. The IVF/ICSI strategy is a strong option for patients if indicated.
Both oocyte quality and endometrial receptivity play an important role in success
in IVF/ICSI practice, and, in this process, endothelial dysfunction may be
associated with increased endocan levels. Our study was designed on this basis
and endocan levels in women with endometriosis were found to be higher, as in the
previous study by Güralp et al. [16]. They found higher endocan
levels in women with endometriosis and reported a positive correlation between
the stages of the disease and endocan levels. However, they noted a
nonsignificant difference in women with advanced stage (stage 3–4) endometriosis
compared to early stage (stage 1–2) [16]. The positive link between stage and
endocan levels in their study is consistent with previous studies [26] showing
that endocan levels correlate with the severity of inflammation. In a study to
understand its role in inflammation, it was shown that endocan expression and
blood level induced by inflammatory cytokines (IL-1, TNF-
We found a weak positive correlation between endocan levels and the presence of endometriosis. We have no evidence about whether this link is caused by the inflammatory process or vascular endothelial pathologies. However, we obtained findings that the increase in endocan expression that is likely triggered by endothelial dysfunction was not correlated with clinical pregnancy or live birth rates in patients that received IVF treatment. Thus, we concluded that it has no remarkable effect on endometrial receptivity, which plays an important role in implantation. However, this result will be clarified in new studies with endocan levels to be studied in endometrial tissue samples.
When the IVF results were studied in the presence of endometriosis in a robust meta-analysis, a lower implantation and clinical pregnancy rate and a poorer oocyte response were noted compared with tubal factor infertility. Moreover, advanced disease was associated with worse outcomes [27]. In the meta-analyses published later, the results in early stage disease were similar to other indications, but, in advanced stage disease, less oocyte retrieval and lower implantation rate and pregnancy outcomes were reported [8, 28]. In large data series published with an up-to-date and different perspective, according to the Society for Assisted Reproductive Technologies Database, women with endometriosis had higher cancelation and lower pregnancy rates after IVF. However, interestingly, they reported a higher live birth rate in women who were diagnosed with isolated endometriosis without an additional diagnosis, compared to women who received IVF treatment for other reasons [29]. In our results, the live birth rate was significantly lower in the endometriosis group and clinical pregnancy was insignificantly low. However, both the cycle cancelation rate and blastocyst formation were slightly higher in the women with endometriosis. These results may be consistent with those of previous studies, but the women in our study were patients with IVF indication not only with endometriosis but also with other accompanying diagnoses. Therefore, although it is difficult to say that endometriosis is directly responsible for negative IVF results, it has at least an indirect effect. Our priority was to examine the relation between negative results and endocan in this group, and no relationship was found between IVF outcomes and endocan levels. As a matter of fact, both the controlled ovarian stimulation parameters and the number of oocytes and embryos obtained were at comparable levels in the two groups. Only peak estradiol levels were high in the endometriosis group but no correlation was detected.
Our research has some limitations. Apart from the variables examined for the
relation between endocan levels and inflammation, the results could be confirmed
by including other biochemical markers of inflammation like CRP, interleukins, or
TNF-
High endocan levels, which are thought to be expressed by endothelial dysfunction, in women diagnosed with endometriosis, a chronic inflammatory disease, and undergoing IVF/ICSI treatment due to infertility indicate that new studies are needed. However, it was observed that there was no relationship between endocan and stimulation parameters, clinical pregnancy, or live birth rates during the IVF process. However, it should be kept in mind that infertility also has a multifactorial etiology and new studies that will cover other variables that may cause inflammation other than endometriosis will shed light on this issue.
MC, NY, HZ designed the study. MC, EC and YT conducted the research and collected the data. NB preserved the collected samples and tested them using ELISA method. MC, EC and YT analyzed the data. MC, NY and HZ wrote the article. All authors contributed to the article. All authors have read and approved the final article.
All subjects gave their informed consent for inclusion before participating in the study. The study was carried out in accordance with the Declaration of Helsinki and the protocol was approved by the Baskent University Institutional Review Board and Ethics Committee Ethics Committee (Project no: KA19/139, 09.07.2019).
We would like to express our gratitude to everyone who supported the writing of this article. We thank all referees for their comments and suggestions.
This study was supported by Baskent University Research Fund (Project no: KA19/139).
The authors declare no conflict of interest.