


1 Department of Perinatology, Division of Obstetrics and Gynecology, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
2 Department of Anesthesiology and Intensive Therapy, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
3 Institute of Anatomy, Faculty of Medicine, University of Ljubljana, 1000 Ljubljana, Slovenia
4 National Institute of Public Health, 1000 Ljubljana, Slovenia
5 Department of Public Health, Faculty of Medicine, University of Ljubljana, 1000 Ljubljana, Slovenia
6 Faculty of Medicine, University of Ljubljana, 1000 Ljubljana, Slovenia
Abstract
Background: Opioid over-prescription after cesarean delivery (CD)
delays postoperative recovery, interferes with breastfeeding and may prompt
persistent opioid use after hospital discharge. We evaluated the effects of
implementing a multimodal stepwise analgesic regimen on opioid consumption and
pain scores after CD. Methods: This was a retrospective before-after
study. Opioid intake (expressed as morphine milligram equivalents (MME)) and pain
scores (using the 11-point numerical rating score) within 24-hours following
planned cesarean delivery under spinal anesthesia without intrathecal morphine
were compared before vs. after change in post-cesarean analgesia regimen. This
included intensified non-opioid analgesia with quadratus lumborum block and
shifting from scheduled to as-needed opioids. Mann-Whitney U test was used for
statistical comparison (p
Keywords
- Analgesia
- Cesarean delivery
- Cesarean section
- Opioids
- Regional anesthesia
Cesarean delivery (CD) rate in Slovenia has risen significantly over the last decades, as in most countries worldwide, and has recently plateaued at approximately 21% [1, 2, 3]. Effective analgesia after CD is a very important component of high-quality perinatal care, as it enables early ambulation, prevention of thromboembolic complications, breastfeeding, and mother-infant bonding [4]. Undertreating post-CD pain is associated with delayed postoperative recovery, postpartum depression and development of persistent pain [5, 6]. Opioids are usually prescribed in the first days following CD together with paracetamol and non-steroidal anti-inflammatory drugs (NSIADs) in order to achieve adequate pain control [7, 8]. However, well-known side effects of opioids such as nausea, vomiting and sedation have been shown to interfere with interaction between mother and infant and worsen the postpartum experience in a dose-dependent manner [6, 7]. Moreover, it has been reported that 1 in 300 opioid-naive patients exposed to opioids post-CD will become persistent opioid users [9]. This makes post-CD analgesia an important public health issue given the epidemic proportions of prescription opioids abuse in several countries [10]. Consumption of prescription opioids, especially tramadol, has risen significantly over the last years in Slovenia as well [11].
A multimodal stepwise post-CD analgesia has been recommended in order to limit opioid use while avoiding undertreating pain [7, 8]. Multimodal analgesia comprises two or more medications with different mechanisms of action to achieve synergistic analgesic effects. Ideally, post-CD analgesics should be combined with regional anesthesia techniques, such as transverse abdominis plane (TAP) or quadratus lumborum blocks (QLB) to further reduce postoperative pain [12, 13, 14, 15]. In addition, pain management should follow a stepwise approach beginning with non-opioid medications followed by opioids only when needed to treat breakthrough pain.
The purpose of this study was to evaluate the effects of implementing a multimodal stepwise analgesic regimen with intensified non-opioid analgesia combined with QLB and shifting from scheduled to as needed opioids on opioid consumption and pain scores after CD.
In this retrospective before-after study, we compared opioid intake in the first 24 hours following planned CD before vs. after introduction of a multimodal stepwise analgesic regimen at the Department of Perinatology, Division of Obstetrics and Gynecology, University Medical Center Ljubljana, Slovenia. The study was approved by Republic of Slovenia National Medical Ethics Committee on 14 May 2019, reference number 01220-251/2019/4. A written informed consent was obtained.
Before August 2019, a combination of opioids (scheduled administration of tramadol 100 mg every 8 hours intravenously and piritramide 3 mg intravenous boluses for breakthrough pain) with 1 g paracetamol per 8 hours and metamizole 2.5 g every 12 hours intravenously was routinely used for analgesia in the first 24 hours after CD at our institution.
In August 2019, as a response to growing awareness of opioid over-prescription as well as the US Food and Drug Administration warning on prescribing tramadol to breastfeeding women, a multimodal stepwise approach to pain management was implemented for patients after CD. New analgesic regimen consisted of intravenous paracetamol 1 g 6 hourly, intravenous metamizole 2.5 g at 12 hourly, and intravenous diclofenac 75 mg/orphenadrine 30 mg (Neodolpasse 250 mL, Fresenius Kabi Austria GmbH, Graz, Austria) at 12 hourly intervals. Three mg boluses of intravenous piritramide were administered for breakthrough pain. This analgesic regimen was introduced as part of a randomized clinical trial examining the effectiveness of posterior QLB (ClinicalTrials.gov identifier: NCT04000308). Therefore, in addition to analgesics medications described above, all women after intervention received posterior QLB (performed immediately following CD under ultrasound guidance with 20 mL 0.25% levobupivacaine per side).
Only women with American Society of Anesthesiologists physical status 2 and 3,
uncomplicated singleton pregnancy with a gestation of at least 37 weeks and CD
under spinal anesthesia using 1.8–2.2 mL hyperbaric bupivacaine 5 mg mL
We compared opioid consumption within 24 hours after CD expressed as morphine milligram equivalents (MME) (http://clincalc.com/Opioids/, last accessed March 13th, 2021) in last consecutive 58 women fulfilling inclusion criteria before introduction of new analgesic regimen (pre-intervention group) and first consecutive 58 women (post-intervention group) fulfilling inclusion criteria. We also analyzed the use of analgesic opioid and non-opioid medications separately and proportions of women requiring no opioids (opioid-free) as well as those requiring 10 MME or more in the two groups. In addition, we compared pain scores using an 11-point numerical rating score (NRS) (from 0, no pain; to 10, worst pain imaginable) in the pre-intervention vs. post-intervention groups.
Data were described using median and interquartile range (IQR). Comparisons were
carried out between the study groups using Mann-Whitney U test. The Chi-square
test was used for qualitative variables when comparing background characteristics
of women and to compare the proportions of women requiring 0 MME as well as
A total of 130 women were assessed for eligibility. Of these, 14 did not meet inclusion criteria and 2 refused to participate in the study, leaving 116 women who were included in the analysis: 58 in pre-intervention and 58 in post-intervention group. Demographic and obstetric data are summarized in Table 1. No significant differences in these characteristics were observed between the two study groups. The race of all women included was Caucasian.
| Characteristic | Pre-intervention (n = 58) | Post-intervention (n = 58) | p-value |
| Maternal age (years) | 33 (30–35) | 31 (29–36) | 0.35 |
| BMI at delivery (kg/m |
30 (27–32) | 28 (25–31) | 0.38 |
| Nulliparity | 15 (26%) | 19 (33%) | 0.38 |
| Education* | 6 (5–6) | 6 (5–7) | 0.14 |
| Neonatal birth weight (g) | 3575 (3218–3763) | 3370 (3073–3615) | 0.10 |
| Estimated blood loss at delivery (mL) | 500 (500–500) | 500 (500–500) | 0.47 |
| The data are presented as median (interquartile range) or n (%); BMI, body mass index; *educational attainment using the Statistical Office of the Republic of Slovenia grading (from 0, no education; 12, PhD degree). | |||
There was a 86% reduction in the median MME of all opioid medications
administered in the first 24 hours after CD (14 (IQR 14–18) mg pre-intervention
vs. 2 (IQR 2–4) mg post-intervention; p
| Analgesic | Pre-intervention (n = 58) | Post-intervention (n = 58) | p |
| MME (mg) | 14 (14–18) | 2 (2–4) | |
| Tramadol (mg) | 300 (300–300) | 0 (0–0) | / |
| Piritramide (mg) | 3 (3–9) | 3 (3–6) | 0.85 |
| Paracetamol (mg) | 3000 (3000–3000) | 4000 (4000–4000) | / |
| Metamizole (mg) | 5000 (5000–5000) | 5000 (5000–5000) | / |
| Diclofenac/Orphenadrine (mg) | 0/0 (0–0/0–0) | 150/60 (150–150/60–60) | / |
| TAP block | 8 (14%) | 0 (0%) | 0.004 |
| QLB | 4 (7%) | 58 (100%) | |
| The data are presented as median (interquartile range) or n (%); MME, morphine milligram equivalents of all opioids administered; TAP, transversus abdominis plane; QLB, quadratus lumborum block. | |||
The implementation of the novel analgesic regimen was associated with a
significant increase in patients receiving no opioids after CD (26 (45%)
post-intervention vs. 0 (0%) pre-intervention; p
Fig. 1 presents postoperative pain (assessed using NRS) in the pre- vs. post-intervention groups at 1, 2, 4, 6, 12 and 24 hours after CD. Pain scores were statistically higher at 2 and 4 hours post-CD in the post-intervention group (1 (IQR 1–2) vs. 2 (IQR 1–3); p = 0.001, and 2 (IQR 1–3) vs. 2 (IQR 2–3); p = 0.03, respectively). At 6 hours post-CD, when the scores were highest in both groups during the entire 24-hour period assessed, women in the post-intervention group reported lower pain (3 (IQR 2–4) vs. 2 (IQR 2–3); p = 0.02). Although statistically significant, differences in NRS between the two study groups were small (proximally 1 point on the 11-point NRS) and can be viewed as clinically insignificant. Moreover, since the NRS scores were equal or less than 3, the pain intensity can be considered mild in both groups.
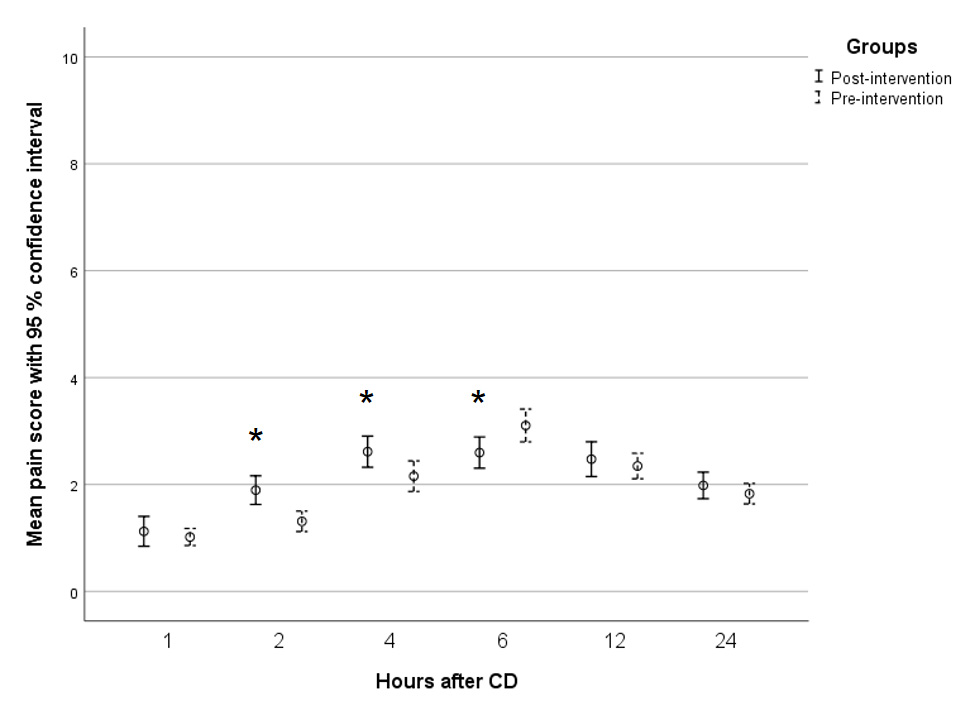 Fig. 1.
Fig. 1.Pain Numerical Raring Score at 1, 2, 4, 6, 12, and 24 hours
after cesarean delivery (CD). * presents statistical significance (p
Intensified non-opioid multimodal analgesic regimen allowed shifting from scheduled to as-needed opioids for post-CD pain management without increase in pain scores. This resulted in significant reduction in opioid consumption after CD.
The results of our quality improvement initiative are in accordance with those of Smith et al. [8], who also observed a reduction in post-CD opioid use associated with scheduled paracetamol and NSAIDs with opioids used only for breakthrough pain. The authors only report reduction in median opioid use per day of hospital stay and not specifically for the first day after CD, when most women experience worst pain and more frequently receive opioids for pain control. Despite this, median MME of opioid analgesic per day administered in their study (10 mg) was still significantly higher than the doses observed at our institution (2 mg). This is even more remarkable considering that most women received intrathecal morphine, which has not been used at our institution. There are several potential explanations for differences in post-CD opioid use in the different settings. First, certain cultural differences in expectation and perception of pain related to birth play an important role in postoperative opioid request [16, 17, 18]. Second, CD at our institution are performed using a Pfannenstiel skin incision just above the pubic hairline with some elements of the Misgav Ladach technique. Visceral and parietal peritoneum are not closed and rectus abdominis muscles are not approximated during CD, which has been proved to reduce acute post-surgical pain [19]. Third, our intervention included not only a change in analgesic medication regimen but also the implementation of QLB, which has been shown in several trials to reduce short-term pain and postoperative opioid requirements after CD [12, 20, 21, 22]. Our results support the opioid-sparing effect of QLB and suggest that this method should be included in multimodal analgesic regimens, especially when intrathecal morphine is not used [12, 13, 14, 15, 20, 23]. Indeed, the use of intrathecal morphine has been shown to be associated with significant side effects such as nausea, vomiting and pruritus with up to 24 hours duration which can significantly affect the quality and speed of postoperative recovery and the mother-baby interaction [14].
The overall reduction in opioid consumption following CD is important for several reasons. Opioid side effects, such as sedation, nausea and vomiting, delay postoperative mobilization and thus increase risks of postpartum thromboembolic complications. These remain one of the most important causes of maternal mortality in developed countries, including Slovenia [3, 24, 25, 26]. Moreover, reducing the in-hospital opioids after CD helps preventing persistent opioid use after hospital discharge [9]. Ultimately, the transfer of medications given to the mother after CD to the breast-fed infant should also be considered. A relative-infant dose (RID) quantifies the amount of neonatal drug exposure relative to the mother’s dose, expressed as a percentage and weight-adjusted for the neonate. RID greater than 10% is generally considered high. Paracetamol, metamizole and diclofenac all have their RID far below 10% [9]. Similarly, RID of opioids are usually below 10% [27]. However, substantial individual variations of opioid metabolism exist in both mother and infant, potentially causing opioid overdose in some infants even if the theoretically estimated dose of the drug received through milk is small [7]. This is especially true for tramadol. Some breast-fed infants metabolize this opioid to its active form much faster than usual causing potentially life-threatening adverse effects, such as lethargy and respiratory failure [7]. The US Food and Drug Administration restricted the use of tramadol in children under 17 years of age as soon as in 2015, expanding this warning to breastfeeding mothers in 2017 [28, 29].
Our study has several limitations, namely the relatively small sample size, single-center setting, and before-after retrospective study design. Study design may have been a source of performance and measurement bias given the increasing awareness of opioid over-prescription among physicians and nursing staff. Furthermore, we used pain scores as proxy for adequate pain control but did not have any direct data on actual patient satisfaction with our post-CD analgesic regimen. We routinely provide satisfaction surveys to every patient discharged from our institution and noted no complaint of undertreated pain during both the pre-intervention and post-intervention group timeframes. However, these surveys are not specifically focused on analgesia evaluation and can also not be viewed as definitive proof of pain management non-inferiority. We also lack data on long-term outcomes, such as persistent pain, postpartum visits to obstetrical triage or emergency departments due to postoperative pain and opioid use after discharge. On the other hand, the major strength of quality improvement initiative is its multidisciplinary nature. Significant reduction in opioid consumption without significant increase in pain scores would not have been possible without close collaboration between anesthesiologists, nursing/midwifery staff and obstetricians.
Multimodal non-opioid analgesic regimen allowed shifting from scheduled to as-needed opioids for post-CD pain management. This resulted in significant reduction in opioid consumption in the first day after CD without significant increase in pain scores.
All authors contributed significantly to the study conception and design. Material preparation and data collection were performed by UV, TA, IB and ML. Data analysis was performed by UV, TSP and ML. The first draft of the manuscript was written by UV and ML, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
The study was approved by Republic of Slovenia National Medical Ethics Committee on 14 May 2019, reference number 01220-251/2019/4. A written informed consent was obtained.
Thanks to all the peer reviewers for their opinions and suggestions.
This research was supported by the tertiary funding grant from the University Medical Centre Ljubljana, Slovenia (grant number TP 20180063).
The authors declare no conflict of interest.