




 , Massimo Maria Salvatori 1, Doriana Scaldaferri 1, Silvio Tartaglia 4, Giovanni Larciprete 1
, Massimo Maria Salvatori 1, Doriana Scaldaferri 1, Silvio Tartaglia 4, Giovanni Larciprete 11 Department of Obstetrics and Gynecology, San Giovanni Calibita Fatebenefratelli Isola Tiberina Hospital, 00186 Rome, Italy
2 Service of Medical Statistics and Information Technology, Fatebenefratelli Foundation for Health Research and Education, AFaR Division, 00186 Rome, Italy
3 Department of Woman and Child Health and Public Health, Fondazione Policlinico Universitario A. Gemelli, IRCCS, 00168 Rome, Italy
4 Department of Biomedicine and Prevention, University of Rome Tor Vergata, 00133 Rome, Italy
Abstract
Background: One of the most important causes of preterm birth (PTB) is cervical insufficiency, which usually it’s treated by performing a surgical cervical cerclage (CC). Currently, a valid alternative to surgical treatment is represented by the application of a non-invasive intravaginal silicon device called Arabin® pessary (AP). The aim of the study is to compare these two therapeutic approaches in terms of gestational and neonatal outcomes. Methods: In this observational cohort study, we retrospectively evaluated the pregnant women between 18 and 24 gestational weeks referred to the Department of Obstetrics and Gynecology of San Giovanni Calibita Fatebenefratelli Hospital of Rome from 2015 to 2017 with the diagnosis of threatened preterm birth. The 26 women were divided into groups according to the treatment received: cervical cerclage (Group-1, in-patient) and Arabin® pessary (Group-2, out-patient), both in combination with vaginal progesterone (PG). The primary outcome was the gestational age at delivery, and various secondary maternal and neonatal outcomes were considered. Results: The results do not show a statistically significant difference between the two groups, both in terms of gestational and neonatal outcomes. Considering surgical risks (anesthesia, blood loss), recovery-time and economic costs of CC, AP showed very interesting advantages resulting in more favorable cost-benefits relation. Conclusion: We confirmed once again that out-patient combination of AP and vaginal PG is a safe, non-invasive choice as treatment of PTB. Unfortunately, the small population doesn’t allow to define this a noninferiority trial. Further larger randomized controlled studies are needed to reassure clinicians about the efficacy of this combined non-invasive approach.
Keywords
- Cervical insufficiency
- Cervical cerclage
- Arabin pessary
- Late abortion
- Preterm birth
- Shortened cervix
According to World Health Organization (WHO), preterm birth (PTB) still
represents the first cause of neonatal mortality and morbidity worldwide [1].
That’s the reason why all over the world government, institutions and scientific
societies are improving the efforts to face this public health problem, with all
due emotional and socio-economic implications [2]. Although enormous progress in
term of antenatal care have been made, global estimates report a rate of 10.6%
of PTB worldwide in 2014 [3], that means more than 1 case every 10 births and
around 15 million of premature newborns per year [4]. PTB is universally defined
as the delivery before 37 weeks or 259 days of gestation. It is stratified in
late PTB (weeks 34
The consequences of a premature delivery on newborns are numerous: although the increased mortality is obviously the most dramatic and evident effect, infants born preterm are more exposed than infants born full term to a wide range of short-term and long-term pathological conditions due to developmental immaturity [6]. Most of such complications carry lifelong consequences for the health, development and growth. A large percentage of babies born preterm will develop respiratory distress syndrome (RDS), associated to surfactant deficiency [7]. To reduce the risk, antenatal administration of glucocorticoids is recommended for women at risk for PTB [8]. Following the RDS, long-term condition such as spontaneous apnea, bronchopulmonary dysplasia and chronic lung disease can occur with higher likelihood of respiratory infections and neurodevelopmental impairing [9]. Due to intestinal fragility, preterm infants are exposed to high risk of developing necrotizing enterocolitis, that occurs in around 7% of infants with birth weights less than 1500 grams [10] and many times requires surgical intervention. Even sensory organs development is affected by PTB, in fact premature newborns suffer from hearing disorders [11] and various degrees of reduced vision that can be complete in some cases [12]. Central nervous system is also vulnerable to injury due to its incomplete formation and its high request for oxygen [13]. The most common form of neural injury is represented by intraventricular hemorrhage and periventricular leukomalacia [14], risk factor of development of cerebral palsy. PTB involve many other conditions affecting at various degrees cardiovascular, immune and hematologic systems. The results of these insults on central nervous system and other apparats is a neurocognitive impairment, with a potential loss of self-sufficiency even in adult life, and the need for intensive therapies and support to all the family unit.
PTB recognizes a multifactorial etiopathogenesis. The main conditions explaining PTB are: iatrogenic PTB (due to pathological conditions that impose medical staff to anticipate the birth as preeclampsia, severe fetal growth restriction or obstetrical emergencies) that occurs in about 25% of cases; preterm premature rupture of membranes (pPROM) in 25%; remaining 50% is referred as spontaneous, idiopathic PTB [15]. The role and the importance attributed to uterine cervix during pregnancy are widely accepted: its inability to contain and preserve the product of conception consequent to structural or functional, congenital or acquired defects, represents in fact one of the most important causes of preterm childbirth and/or late abortion. Cervical cerclage (CC) is a surgical procedure that has been employed in clinical practice as a therapy of cervical insufficiency since the mid-20th century, and that finds its rational in the increase of the mechanical resistance of the cervix. Different way to perform this kind of surgery have been described during the last decades. The most used cerclage techniques were described by Shirodkar and Mc Donald [16, 17]. The surgical intervention aims to close the insufficient or effaced cervix by a transvaginal purse-string suture. There is insufficient evidence to support any specific technique for cerclage insertion. In a secondary analysis of singleton pregnancy data from four randomized trials of cervical cerclage in women with a short cervix, there was no significant difference in the rate of delivery before 33 weeks’ gestation in those with Mc Donald cerclage when compared with those with a Shirodkar suture [18]. Abdominal cervical cerclage has been proposed [19] but its invasiveness seems to be the major concern.
A viable alternative to surgical treatment is represented by the application of an intra-vaginal non-invasive, easy to apply and non-operator dependent device, called Arabin® (Dr. Arabin GmbH & Co. Witten, Germany) pessary (AP). In 1979 the German gynecologist Hans Arabin developed a flexible silicon device with a circular central hole to allow the whole cervix to be included in. Due to the its shape, the device fit into the vaginal fornices and can be angulated following the evolution of uterus in pregnancy. Arabin assumed that he must not forcibly close the cervical canal, the principle on which is based the surgical cerclage, but just restore the cervix to the natural angle with the uterine body. In fact, AP was designed with a double intent: to hold and squeeze the cervix, but especially to tilt the cervix and rotate it slightly toward the sacrum. In this way the pessary can interrupt the possible evolution towards the onset of contractions that ultimately led to preterm delivery. In 1990 Quaas et al. [20] in an observational study of 107 patients undergoing AP application, both in case of prophylactic treatment or in case of emergency surgery, reported that in 92% of women pregnancy was maintained up to 36 weeks’ gestation and without complications. Further studies [21, 22] showed that AP, when applied in association with progesterone (PG), presented a lower rate of infections and uterine bleeding than cervical cerclage. AP reduced the costs of hospitalization and the economic resources employed, resulting more favorable in terms of cost-benefits. A comparison between different approaches (CC, AP, PG) to face preterm birth, published in 2013 by Alfirevic, showed no differences in the incidence of spontaneous preterm births, neonatal morbidity or perinatal mortality between the 3 groups [23]. However, the study is a retrospective cohort study affected by retrospective bias. The possibility of combining interventions to prevent PTB has been investigated: most of the studies compare CC plus PG versus CC alone, with no significative differences [24]. Less number of studies have evaluated the efficacy of exclusive AP versus AP plus vaginal PG. A study conducted by the same Arabin showed no differences among the two group in term of gestational age at birth, but the group of AP plus PG has been correlated with a better neonatal outcome in term of neonatal intensive care unit (NICU) admissions [25].
We are still waiting for further studies to confirm the validity of the pessary application in the prevention and treatment of cervical insufficiency. That is why the use of this device is yet not widely spread. The Italian Society of Obstetrics and Gynecology (SIGO) recommends that the use of AP should be included only in research protocols. The aim of our study is to increase the current knowledge about the prevention of the late abortion and/or the preterm birth in case of high risk, comparing the AP with the traditional surgical CC, in terms of gestational and neonatal outcomes and economic resources employed.
We report a retrospective observational cohort study on 26 pregnant women at
18–24 weeks of gestation admitted to the Obstetrics and Gynecology Department of
San Giovanni Calibita Fatebenefratelli Hospital “Isola Tiberina” of Rome, from
January 2015 to January 2017, with the diagnosis of threatened PTB defined as
shortened cervix (
| Inclusion criteria | Exclusion criteria |
| Singleton pregnancies between 18 and 24 weeks | Dilatated cervix and/or protruding amnio-chorial membranes |
| Anamnesis of 2 or more late abortions/preterm births | Women with severe abdominal pain or clinical evidence of sepsis |
| Cervical length less of 25 mm with or without funneling | Rupture of the membranes (or suspicious of rupture) at the moment of the admission |
| Other risk factors for cervical insufficiency (Mullerian anomalies, interventions on the cervix etc.) | Women already subjected to cervical cerclage |
| Fetuses with evidence of significant congenital, structural or chromosomal anomalies |
We evaluated the following anamnestic data: year of admission, age, ethnicity, parity, previous spontaneous abortions/intrauterine fetal death, previous uterine surgery, uterine anomalies. At the time of the admission and after the treatment, we observed: cervical length, presence of funneling, obstetrics pathological conditions, gestational age of CC/AP application, gestational age of cerclage/pessary removal, duration of treatment, days of hospitalization, use of tocolytics, maternal complications, gestational age at birth, mode of delivery (vaginal birth or C-section), indications for C-section, neonatal birth weight, 1 and 5-min Apgar score, neonatal complications.
After receiving procedure specific informed consent, all women were subjected to surgical CC or AP to prevent PTB, plus vaginal administration of 200 mg of PG according to current literature [27]. The choice of the treatment was based on the decision of the doctor who took charge of the patient or on the patient will after informed consent and exhaustive explanation of the two approaches.
Our Obstetrical Department is a tertiary center for Maternal-Fetal Medicine, and all the clinicians are well skilled to perform surgical CC and are trained in the placement of AP. All the CCs were performed according to the Shirodkar procedure [16].
The included population was divided into two groups depending on the type of treatment received: Group-1 included 18 pregnant women that were hospitalized and underwent emergency CC; Group-2 included 8 women treated with AP application in out-patient clinical service.
The approval for the processing of personal clinical data was obtained from the patients and from the local Research Ethics Committee.
Continuous data are presented in terms of mean (standard deviation) or, if they
have an asymmetric distribution, in terms of median (minimum–maximum).
Categorical data are presented in terms of absolute frequency (percentage). The
difference between the two groups concerning continuous variables was evaluated
through the Student T-test or through the non-parametric Mann-Whitney
test. The association between categorical variables was evaluated with the Chi
square test or when appropriate with the Fisher exact test. A p value
Demographic data do not show relevant differences between two groups: maternal
age oscillates between a maximum of 45 years and a minimum of 21 years, with no
correlation to the treatment or the outcome (p
| Group 1 | Group 2 | p | ||
| Parity (%) | 0 | 9 (50%) | 5 (62.5%) | 0.999 |
| 1 | 7 (39%) | 3 (37.5%) | ||
| 2 | 2 (11%) | 0 | ||
| Previous miscarriages | Median (min–max) | 1 (0–3) | 0 (0–2) | 0.226 |
The most common indication to the treatment was a cervical length
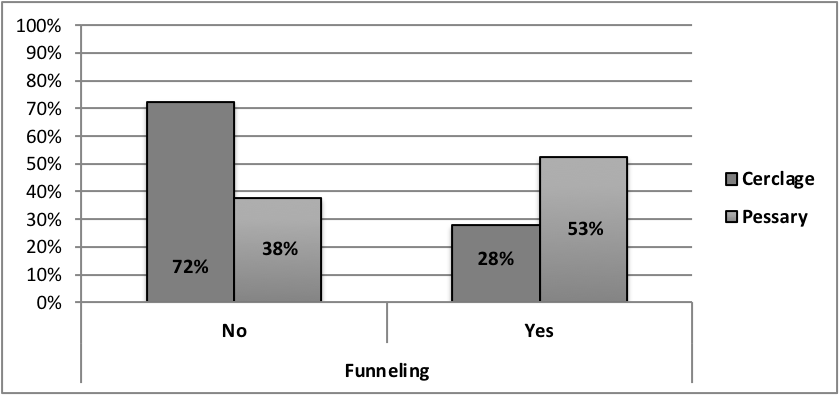 Fig. 1.
Fig. 1.Incidence of funneling.
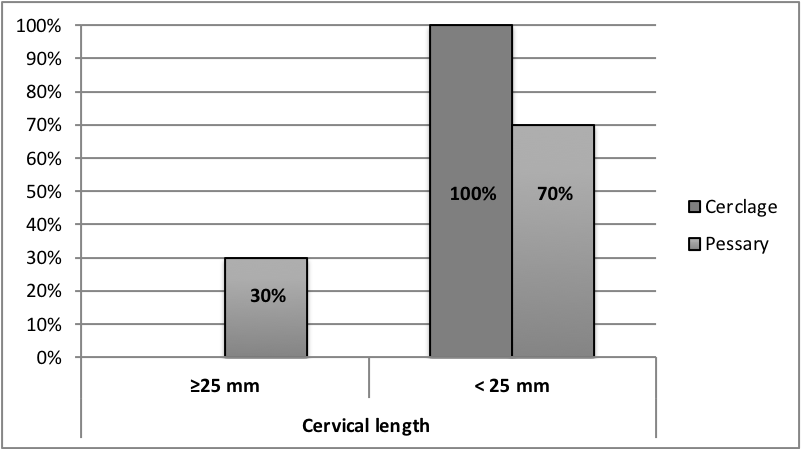 Fig. 2.
Fig. 2.
Incidence of cervical length
In Group-1 the average gestational age in which the CC was performed was 21.4 weeks, while in Group-2 the average gestational age in which the pessary was inserted was 22.8 weeks: in this case the p-value shows a statistically significant difference between the two groups as shown in Table 3.
| Group 1 | Group 2 | p-value | ||
| GA. application | Average | 21.4 | 22.8 | 0.038 |
| weeks (SD) | (1.60) | (1.13) | ||
| GA. removal | Average | 36.8 | 33.6 | 0.045 |
| weeks (SD) | (2.70) | (5.00) | ||
| Duration of treatment | Average | 15.3 | 10.7 | 0.013 |
| weeks (SD) | (3.55) | (5.13) |
Regarding Group-1, in 17/18 cases the cerclage was removed between 36 and 39 weeks with 11 spontaneous delivery (one at 36 weeks, one at 37 weeks, four at 38 weeks, two at 39 weeks, two at 40 weeks, one at 41 weeks) and 6 caesarean deliveries (4 of these were urgent: one at 36 weeks due to the onset of labor in a woman with a fetus in breech presentation, one at 36 weeks for pPROM and previous C-section, one at 38 weeks due to the onset of labor in a woman with a previous myomectomy and PROM, one at 39 weeks due to a failed induction of labor; and two elective caesarean deliveries between 38 and 39 weeks). In one case the cerclage was removed at 27 weeks because of the need to perform an urgent caesarean delivery due to the onset of labor in a woman with severe vaginal bleeding.
Regarding Group-2, in 6/8 cases the pessary was removed between 36 and 38 weeks
of gestation with 5 spontaneous delivery (two at 38 weeks, one at 39 weeks, one
at 40 weeks and one at 41 weeks) and one caesarean delivery at 39 weeks due to
fetal breech presentation. In one case the pessary was removed at 35
Statistically significant difference (p-value = 0.045) was found about the average gestational age at the moment of the removal of the treatment applied. The average duration of treatment too showed a statistically significant difference: in Group-1 it was 15.3 weeks; in Group-2 it was 10.7 weeks (p = 0.013).
Analyzing the data related to childbirth, in both study groups there were no abortion deliveries. The percentage of preterm deliveries was found to be 17% in Group-1 and 25% in Group-2 (Fig. 3) without statistically significant difference (p-value = 0.628).
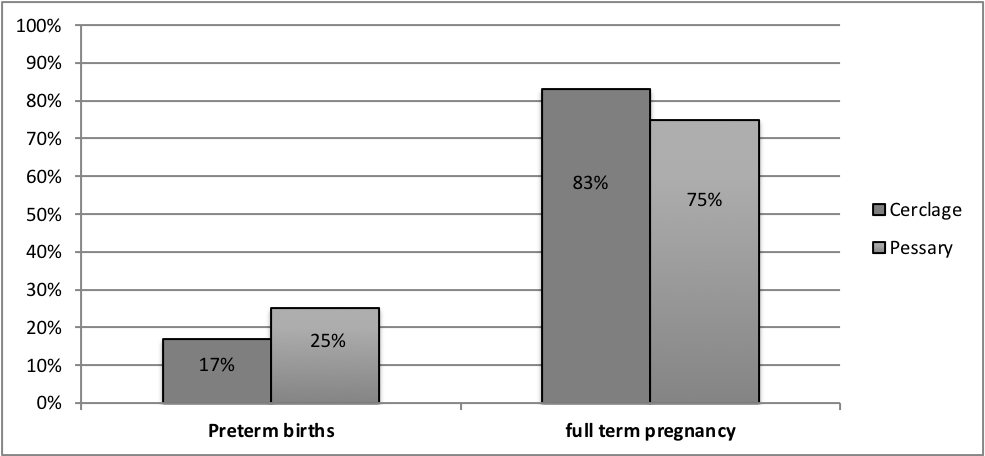 Fig. 3.
Fig. 3.Incidence of preterm births and full-term pregnancy.
Considering the way of delivery (spontaneous births, operative vaginal deliveries and C-sections) in the two groups (Fig. 4) there was no statistically significant difference (p = 0.999).
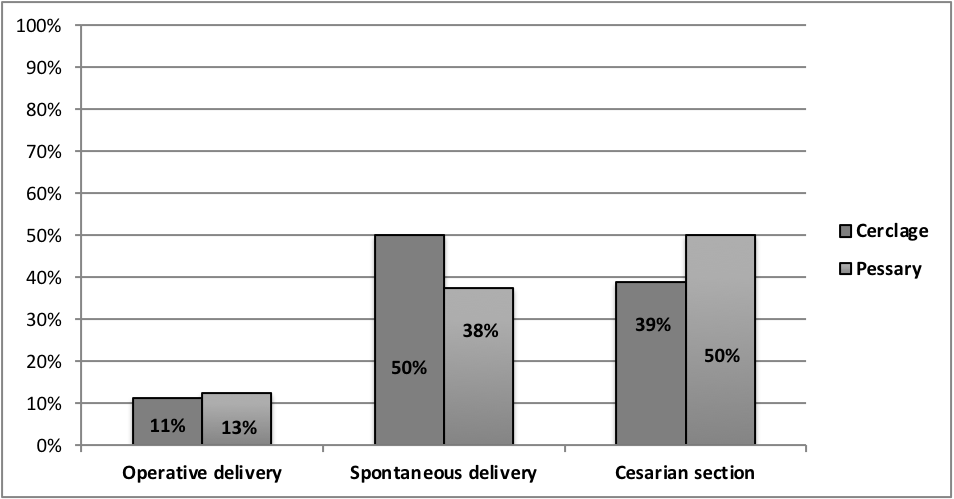 Fig. 4.
Fig. 4.Delivery mode.
There was also no statistically significant difference about the average gestational age at birth: in Group-1 it was 37.7 (sd = 3.12) weeks; in Group-2 it was 36.8 (sd = 5.17) weeks (p = 0.588). Finally, the weight of the new-born at birth, the 1 and 5-min Apgar score and neonatal complications were analyzed. In none of the variables in question a statistically significant difference has been found between the two groups (Table 4).
| Group 1 | Group 2 | p-value | ||
| Neonatal weight (gr) | Average (SD) | 3160.4 (710.22) | 2901.2 (968.97) | 0.450 a |
| Median | 3220 | 3040 | ||
| (Min–Max) | (900–4190) | (810–3920) | ||
| 1 min-Apgar score | Median | 9 | 9 | 0.534 a |
| (Min–Max) | (7–9) | (3–9) | ||
| 5 min-Apgar score | Median | 10 | 10 | 0.615 a |
| (Min–Max) | (8–10) | (7–10) | ||
| Neonatal complications (intubation, giving OX…) | % | 1/18 | 1/8 | 0.529 b |
| (n) | (n:1) | (n:1) | ||
| (a) All p values were from non-parametric Mann-Whitney test; (b) p value from Fisher exact test. | ||||
Regarding hospitalization, blood loss and pain, Group-2 women were followed up
in outpatient clinic after the placing of the device during a simple non-painful
obstetric examination, with no need of hospitalization and with no blood loss.
The women underwent CC were hospitalized (average number of days 2.6
The results obtained do not show a statistically significant difference between the two groups in terms of gestational and neonatal outcomes. The majority of patients gave birth at the end of pregnancy, regardless of the treatment executed and there were no adverse neonatal outcomes if the cases of extremely low gestational age birth are excluded (one per group).
Obviously, this study is only a description of the different approaches’ outcomes, suffering the bias of the observational retrospective studies. The decision of the treatment was made based on the experience of the clinicians or on the patient decision, with no accurate selection of the cases. Anyway, the demographic data of the populations do not show any difference on obstetric history or clinical conditions at time of admission, excepting for the higher percentage of patients with short cervix in the group of CC.
Because of 100% of patient in Group-1 presented with cervical length
Further studies are necessary, however the preliminary information obtained are satisfactory and let us look at the application of AP as a valid alternative to cerclage, as a feasible way to decrease the incidence and prevalence of late abortions and/or PTBs. Moreover, the AP reduces hospitalization costs and the economic resources used, resulting in more favorable cost-benefits relation. In fact, women to whom a pessary must be applied because of cervical shortening, without contractions or another comorbidity, are usually not hospitalized.
This observational retrospective study, with limitations due to the size of the population, show once again no superiority of one of the available approaches for the prevention of PTB. The results obtained do not show a statistically significant difference between the two groups in terms of gestational and neonatal outcomes. If these results will be confirmed by larger o randomized controlled trials, it will be possible to affirm that the CC and AP and PG vaginal administration are interchangeable treatment for threatened PTB. Considering surgical risks (anesthesia, blood loss), recovery-time and economic costs of CC, AP shows very interesting advantages resulting in more favorable cost-benefits relation. Treatment with a pessary can additionally reassure patients and encourage them to stay at home instead of being hospitalized. With early cervical shortening and/or additional risk factors such as sludge, severe funneling, membrane dissociation or even some degree of external dilatation, it is prudent to admit the patient initially and follow the course of clinical symptoms and the cervical appearance: in these cases, the hospitalization is necessary and it can last even weeks.
We confirmed that out-patient combination of AP and vaginal PG is a safe, non-invasive choice as treatment of PTB.
Unfortunately, the small population don’t allow to define this a noninferiority trial, and so further studies are definitely needed, however the preliminary information obtained are satisfactory and let us look at the application of AP as a valid alternative to CC, as a feasible way to decrease the incidence and prevalence of PTBs in a non-invasive, cost-effective way.
GL, as the principal investigator, ideated the study. MMS and VA followed the patients during the pregnancy. Two authors (CP, DS) revised the medical records; IS made the statistical study. ST and NC elaborated the manuscript, revised by GL. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The study was retrospective, based on the medical data of women that previously gave the consent. That’s why the Ethical Committee gave us the permission without ethic committee number. In our institution, every patient gives the consent to use proper medical data to research purposes.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. GL is our Editor Board, given his role as Editor Board, had no involvement in the peer-review of this article and has no access to information regarding its peer-review.